
Abstract
Background
Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) has various similarities with AQP4-IgG-seropositive Neuromyelitis Optica Spectrum Disorder (AQP4-IgG + NMOSD) in terms of clinical presentations, magnetic resonance imaging (MRI) findings, and response to treatment. But unlike AQP4-IgG + NMOSD, which is known to coexist with various autoimmune diseases and cancers, an association of MOGAD with these conditions is less clear.
Methods
We conducted a systematic search in PubMed, Scopus, Web of Science, and Embase based on the preferred reporting items for systematic reviews and meta-analysis (PRISMA). Duplicates were removed using Mendeley 1.19.8 (USA production) and the citations were uploaded into Covidence systematic review platform for screening.
Results
The most common autoimmune disease overlapping with MOGAD was anti-N-Methyl-D-Aspartate receptor encephalitis (anti-NMDAR-EN), followed by autoimmune thyroid disorders, and the most common autoantibody was antinuclear antibody (ANA), followed by AQP4-IgG (double-positive MOG-IgG and AQP4-IgG). A few sporadic cases of cancers and MOG-IgG-associated paraneoplastic encephalomyelitis were found.
Conclusion
Unlike AQP4-IgG + NMOSD, MOGAD lacks clustering of autoimmune diseases and autoantibodies associated with systemic and organ-specific autoimmunity. Other than anti-NMDAR-EN and perhaps AQP4-IgG + NMOSD, the evidence thus far does not support the need for routine screening of overlapping autoimmunity and neoplasms in patients with MOGAD.
Keywords
Introduction
Myelin oligodendrocyte glycoprotein antibody disease (MOGAD) refers to a range of central nervous system (CNS) inflammatory conditions associated with the presence of autoantibodies against MOG. These conditions include acute disseminated encephalomyelitis (ADEM), optic neuritis (ON), or transverse myelitis (TM), as well as some cases of aquaporin-4 (AQP4)-IgG seronegative Neuromyelitis Optica Spectrum Disorder (NMOSD). 1 Despite the diversity of clinical and pathologic manifestations and disease outcomes, seropositive MOGAD is now regarded as a distinct entity among CNS inflammatory disorders linked together by immunity to MOG. Preliminary studies indicate that MOGAD has a more benign course and relatively better recovery from relapses in most patients compared to AQP4-IgG + NMOSD. 2
Identifying associations among autoimmune diseases is important in patients with CNS demyelinating disorders because it may change the therapeutic strategies, monitoring approaches and intervals, and prognosis of both CNS inflammatory diseases and the co-existing autoimmune entity. 3 The underlying mechanisms of autoimmunity and autoantibody production in autoantibody-associated neurological syndromes are still unclear. One may postulate that a common immunologic defect may drive autoimmunity or autoantibody production in various organs, or that an existing autoimmune condition or malignancy may trigger additional defects in the immune system resulting in the development of new autoantibody or autoimmunity. 4
One of the recognizable features of AQP4-IgG + NMOSD is the large overlap with other autoimmune conditions such as systemic lupus erythematosus (SLE), Sjogren's disease, autoimmune thyroid disorders (ATDs), and myasthenia gravis (MG).5,6 In contrast, there is less known about the association of immunological comorbidities with MOGAD.
Published reports of co-existing autoimmunity in a large cohort of pediatric and adult patients with MOGAD and AQP4-IgG + NMOSD highlight the point that concomitant autoimmunity is less common in MOGAD when compared to AQP4-IgG + NMOSD. 3 Other comparative studies showed that antinuclear antibody (ANA) was positive in 43% of AQP4 + IgG NMOSD but only 7% of MOGAD patients. 7 Similarly, concomitant autoimmune disorders were observed in 45% and 11% of AQP4-IgG + NMOSD, and MOGAD patients, respectively. 8
Herein, we systematically reviewed the literature for cases of autoimmune diseases, autoantibodies, neoplasms, and paraneoplastic syndromes that have been reported to overlap with MOGAD.
Methods
We conducted this systematic review to investigate any overlapping of MOGAD/positive MOG-IgG and other autoimmune diseases, autoantibodies, neoplasms, and paraneoplastic syndromes, based on the preferred reporting items for systematic reviews and meta-analysis (PRISMA).
Search strategy
We designed our systematic search syntax based on PRISMA from inception to July 2022, which included all mesh terms of “MOGAD,” all autoimmune diseases, autoantibodies, neoplasms, and paraneoplastic syndromes (Supp. 1.) Our syntax was customized to match the four main systematic review databases including PubMed, Scopus, Web of Science, and Embase. The following results were imported to the desktop version of Mendeley 1.19.8 (USA production) to merge duplications and prepare for the screening. Two independent investigators (N.M. and G.B.) screened all publications to find probable appropriate studies by title and abstracts through Covidence systematic review software. 9 Disagreements in screening were resolved by debating. In addition, the gray literature and reference lists of all articles included in the search were reviewed to ensure no information was left out.
Study selection and data extraction
The data extraction table advanced by the variables including author, year, the number of cases, sex, age, clinical presentation, antibody testing assay and source, and notable clinical features and MRI findings. The inclusion criteria consisted of all studies (case reports, case series, observational studies, etc.) which reported at least one autoimmune disease, positive autoantibody (with or without disease presentation), neoplasm, or paraneoplastic syndrome, overlapping with MOGAD or positive MOG-IgG serostatus (either simultaneously or with an interval between them). On the other hand, exclusion criteria comprised papers without English abstracts, and all types of reviews, letters, and commentaries. N.M and G.B. separately extracted the included articles and disagreements resolved by the expert opinion (M.L).
Results
The PRISMA flow chart of this study is shown in Figure 1. Using the search strategy, 10,601 studies were identified however, 5664 studies remained after duplicate removes. After eliminating these duplicates, 296 and 343 studies assessed for full text eligibility by N.M. and I.L. independent screening. Our literature review showed that the most common autoimmune disease reported to overlap with MOGAD or positive MOG-IgG serostatus, is anti-NMDAR encephalitis (Anti-NMDAR-EN) (200 cases) (Table 1), followed by ATD (38cases), and SLE (35 cases) (Table 3). The most frequently reported autoantibodies overlapping with MOGAD were ANA (96 cases) (Table 3), and AQP4-IgG (70 cases of double-positive MOG-IgG and AQP4-IgG) (Table 2) respectively.
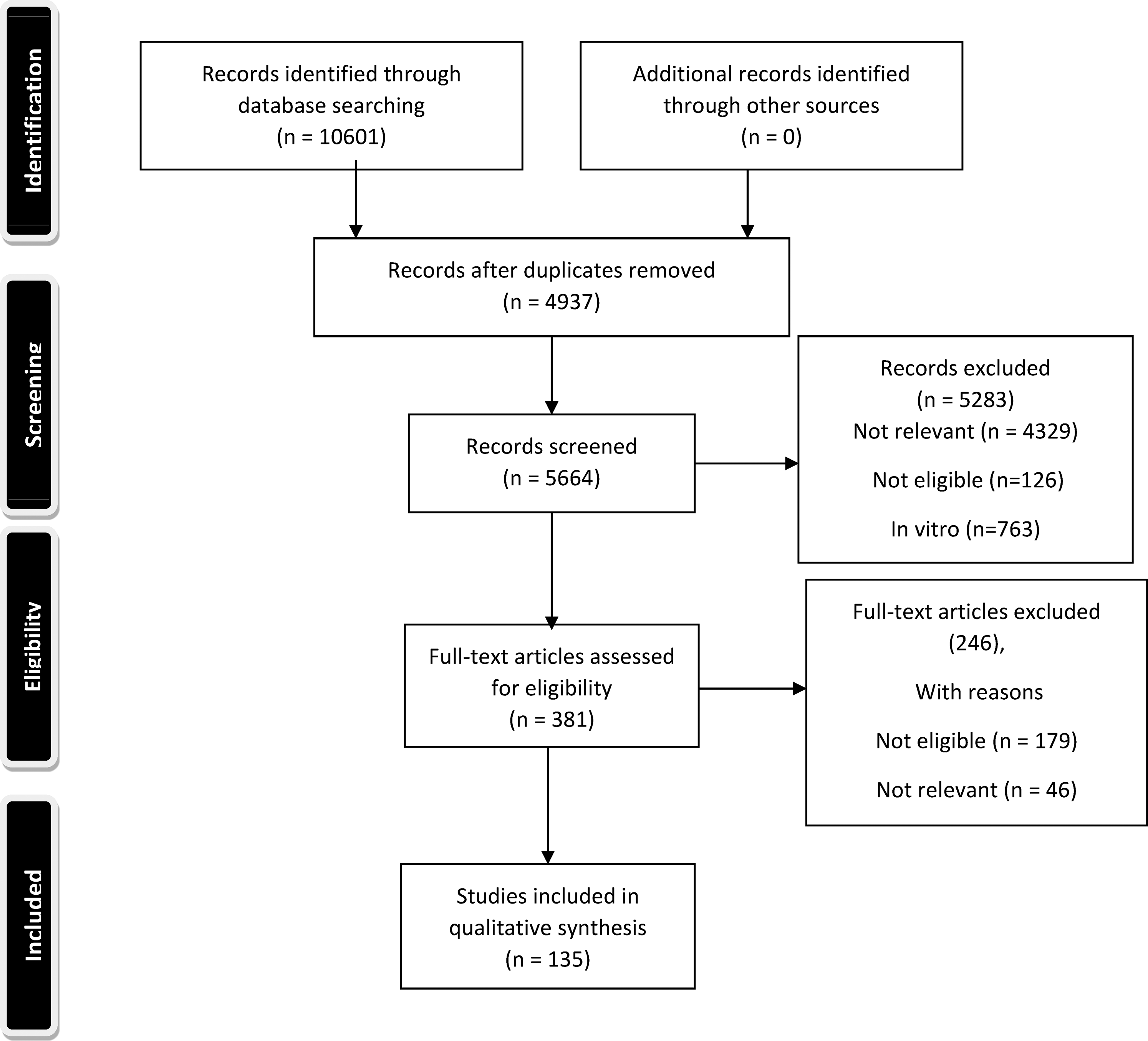
PRISMA flow chart of the study.
Overlapping MOGAD/positive MOG-IgG and anti-NMDAR-encephalitis/positive anti-NMDAR-IgG.
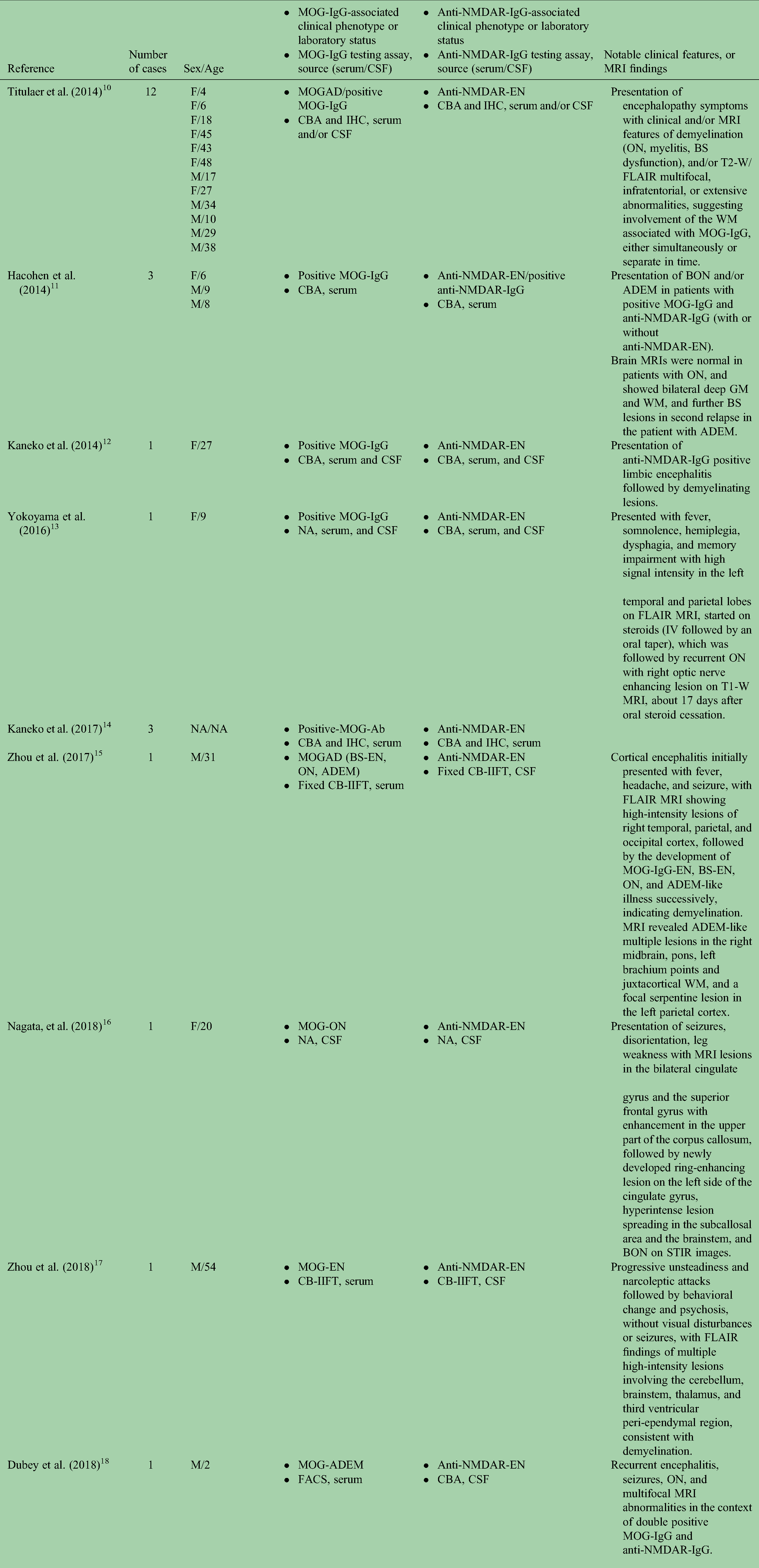
Abbreviations: MOGAD: myelin oligodendrocyte antibody associated disease; NMDAR: N-methyl-D-aspartate; MRI: magnetic resonance imaging; EN: encephalitis; CBA: cell-based-assay; IHC: immunohistochemistry; CSF: cerebrospinal fluid; ON: optic neuritis; BS: brainstem; T2-W: T2 weighted image; FLAIR: fluid-attenuated inversion recovery; WM: white matter; NA: not available, DS: demyelinating syndrome; BON: bilateral optic neuritis; ADEM: acute disseminated encephalomyelitis; GM: gray matter; T1-W: T1 weighted image; IIFT: indirect immunofluorescence test; STIR: short tau inversion recovery; FACS: fluorescence-activated cell sorting; EM: encephalomyelitis; IF: immunofluorescence; CASPR2: contactin-associated protein-like 2
Overlapping MOGAD/positive MOG-IgG and AQP4-IgG + NMOSD.

Abbreviations: NMOSD: neuromyelitis optica spectrum disorder; CBA: cell-based assay; ON: optic neuritis, TM: transverse myelitis; LETM: longitudinally extensive transverse myelitis; MRI: magnetic resonance imaging; ELISA: enzyme-linked immunosorbent assay; MS: multiple sclerosis; EDSS: expanded disability status scale; GlyR-Ab: glycine receptor antibody; FL-MOG: full-length human MOG-Ab; SL-MOG: short-length human MOG-Ab; BON: bilateral optic neuritis; EM: encephalomyelitis; FACS: fluorescence-activated cell sorting; IIF: indirect immunofluorescence; MG: myasthenia gravis.
Overlapping MOGAD/positive MOG-IgG and other autoimmune diseases and/or autoantibodies.

We found 9 cases of overlapping MOGAD and positive Glycine-Receptor (Gly-R)-antibody (Table 3), and one case of each of the following: double positive MOG-IgG and anti-NMDAR-EN with positive anti-contactin-associated protein-like 2 (CASPR2) antibody, glial fibrillary acidic protein (GFAP) astrocytopathy with double positive AQP4-IgG and MOG-IgG, MG with double positive AQP4-IgG and MOG-IgG, MOGAD with positive CASPR2-IgG and leucine-rich glioma-inactivated 1 (LGI1) IgG, MOGAD with atopic dermatitis and asthma bronchiole, and MOG-ON with Sjogren's syndrome with positive Sjogren's syndrome antigen A antibody (SSA), ANA, and rheumatoid factor (RF).
A review of neoplasms and paraneoplastic syndromes associated with MOGAD showed five sporadic cases of cancers (T-cell lymphoma, lung, and colon) and three cases of MOG-IgG-associated paraneoplastic encephalomyelitis in the setting of malignancies of the ovary, lungs, and breast. Results of overlap between MOGAD and cancers/paraneoplastic syndromes are summarized in Table 4.
Overlapping MOGAD/positive

EM: encephalomyelitis; ON: optic neuritis; LETM: longitudinally extensive transverse myelitis; MY: myelitis
Discussion
To our knowledge, this is the first literature review of coexisting autoimmune diseases and cancers with MOGAD. Unlike AQP4-IgG + NMOSD, MOGAD lacks clustering of autoimmune diseases and autoantibodies associated with systemic and organ-specific autoimmunity. 3 Kunchok et al. showed that the frequency of any autoimmune diseases was 33.5% in AQP4-IgG + NMOSD adult-onset patients, and 12.2% in MOGAD adult-onset patients. These frequencies were 14.3% and 3.6% in pediatric-onset AQP4-IgG + NMOSD, and MOGAD patients, respectively. 3 This finding implies a difference in the immunopathogenic mechanisms involved in the development of each entity, such that AQP4-IgG + NMOSD is more attributable to a defect in immune tolerance, while MOGAD is more likely to be an aberrant autoimmune response to certain triggers, such as infection, vaccination, or malignancy.3,146
The major finding of our study was that the most frequent autoimmune disorder that has been reported to co-exist with MOGAD is anti-NMDAR-EN, which is a similar finding to previous studies. 53 Some studies have referred to this co-occurrence as “overlapping syndrome of MOGAD and anti-NMDAR-EN, (MNOS).”19,51 In our literature review, we captured a total of 200 patients who either met the diagnostic criteria for autoimmune encephalitis and were simultaneously seropositive for both anti-NMDAR-IgG, and MOG-IgG or who met the diagnostic criteria for each of MOG-associated encephalitis (MOGAD-EN) or anti-NMDAR-EN and was seropositive for the antibody associated with the other one, at the same time. 10 Given the rarity of both MOGAD and anti-NMDAR-EN, the co-occurrence of these two entities may happen in the context of an association or could be just a coincidence. This overlap could be categorized as one of the following chronological phenotypes: (1) cases that start with a presentation of anti-NMDAR-EN who develop demyelinating events consistent with MOGAD later; (2) cases with a known diagnosis of MOGAD who later present with anti-NMDAR-EN; and (3) cases of autoimmune encephalitis with concurrent positive MOG-IgG and anti-NMDAR-IgG, demonstrating that antibodies against NMDAR and MOG can be simultaneously detected in one patient.10,54 One possible explanation could be an immunological activation (e.g. an infection) driving the production of different subclasses of neuronal autoantibodies (anti-MOG-IgG, anti-NMDAR-IgG), resulting in the development of two different diseases.13,53 Another hypothesis is that since both MOG and NMDAR are expressed on oligodendrocytes, an immune attack against one may provoke targeting the other one by antigen spreading.22,53
Considering the different disease courses and the outcomes of the two diseases, the management of the co-existing MOGAD and anti-NMDAR-EN could be challenging. MOGAD was perceived primarily as a monophasic CNS inflammatory disease, but further observations showed that a relapsing course occur in 28–60% of patients, and in up to 83% of cases with long-term observation, especially those with persistent positive MOG-IgG status.99,143 Some evidence of subclinical disease activity and progression has been shown to be present in some of the patients with MOGAD. 2 Patients with anti-NMDAR-EN tend to have more severe neurologic presentations, and poor long-term functional outcomes, and the mortality rate has been reported between 5% and 7%.144–146 In their study of 23 patients with overlapping demyelinating syndrome and anti-NMDAR-EN, Titaluer et al. demonstrate that the demyelinating episodes are more difficult to treat than anti-NMDAR-EN and often required more aggressive therapies, emphasizing the importance of its prompt diagnosis and treatment. 10
We found 70 patients reported to be double-positive for MOG-IgG and AQP4-IgG, suggesting the co-existence of these two antibodies in the same patient is not as rare as previously thought. 25 Patients with double positive AQP4-IgG and MOG-IgG have been reported to be more refractory to therapies, relapse frequently, and progress rapidly.68,75 Matsuda et al. reported one double seropositive case which had recurrent ON attacks with residual visual field deficit, resulting in no improvement in visual acuity despite courses of treatments. They concluded that regardless of the method of measurement, double-positive cases were found to have a significantly poorer visual outcome, suggesting that anti-AQP4 and anti-MOG antibodies may indicate the prognosis of visual function in ON. 75 Kezuka et al. noted that 50% of double-positive patients did not respond to corticosteroid pulse therapy and plasmapheresis, and show no post-treatment improvement in visual function, whereas the visual acuity improved significantly in the double negative group following the same treatment.68–75 Overall, these findings suggest that MOG-AQP4-IgG double seropositivity might be a marker of a poor outcome in NMO spectrum disorders, possibly because of the involvement of both astrocytes and oligodendrocytes.68,75 Given the overall rarity of double positive cases based on the results of the larger studies, and considering the superior specificity of the AQP4-IgG test compared to the MOG-IgG test, and that a reliable cell-based-assay (CBA) for detecting MOG-IgG has been available just recently (2017), there is a high possibility that most of the double positive cases may likely be AQP4-IgG + NMOSD with false positive MOG-IgG test results, especially in reports made before this time with using enzyme-linked immunosorbent assay (ELISA).68,75–147 False positive AQP4-IgG test results may occur rarely as well.
We found 35 cases of coexisting MOGAD and SLE, or SLE patients harboring MOG-IgG, some of which had a presentation of neuropsychiatric SLE (NPSLE). It is worthy of mentioning that, since the denominator to get to 35 cases is unknown, therefore the causal connection between MOGAD and SLE is either unclear or not present.
The potential role of anti-tumor necrosis factor (TNF)-alpha inhibitors in the development of CNS demyelination has been postulated to explain the overlapping MOGAD and some cases of Crohn's disease, ankylosing spondylitis, and psoriasis.114–116 Other autoimmune disorders and autoantibodies that have been shown to overlap with MOGAD come from case reports and observational studies, which seem to be a coincidence and comparable with their frequency in the general population. Reports of MOGAD in patients with malignancies may represent the development of MOGAD as a paraneoplastic syndrome or could be an incidental co-occurrence, or false positive results of the MOG-IgG test.
Other than anti-NMDAR-EN and perhaps AQP4-IgG + NMOSD, the evidence thus far does not support the need for routine screening of overlapping autoimmunity and neoplasms in a patient with MOGAD. On the other hand, the antibody screening test for MOG-IgG may be helpful in cases of development of any atypical symptoms for encephalitis, or MRI findings attributable to demyelination, especially in patients with a diagnosis of anti-NMDAR-EN.
Most of our data come from case reports, case series, and observational studies, and only a few large studies looking at the association between MOGAD and autoimmune diseases are available, so we do not have a total denominator to report a fixed ratio or percentage of overlapping MOGAD and autoimmune disorders or cancers, and without the denominator, studies that found little or no association can make it appear like there is an association. The publication bias can inflate the potential connection between MOGAD and other autoimmune diseases or autoantibodies such as SLE or double AQP4-IgG and MOG-IgG positive cases, and this makes it hard to judge if there is a true connection between these two entities. As a result, we cannot draw a precise conclusion by only assessing and contrasting the total number of reported cases, which does not actually indicate the prevalence of concomitant autoimmune entities in MOGAD. In summary, our study suggests that the connection between autoimmune diseases and MOGAD is low or at least less than AQP4-IgG + NMOSD, and further studies are needed to establish the predisposing factors in the development of concurrent autoimmune diseases or autoantibodies in patients with MOGAD.
Supplemental Material
sj-docx-1-mso-10.1177_20552173221128170 - Supplemental material for Autoimmune diseases and cancers overlapping with myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD): A systematic review
Supplemental material, sj-docx-1-mso-10.1177_20552173221128170 for Autoimmune diseases and cancers overlapping with myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD): A systematic review by Negar Molazadeh, Gauruv Bose, Itay Lotan and Michael Levy in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Declaration of conflicting interests
The institution of Dr Molazadeh has received research support from Genentech, Inc. Dr Gauruv Bose has received an endMS Postdoctoral Fellowship award from the Multiple Sclerosis Society of Canada. Dr Lotan has nothing to disclose. Dr Levy received personal consulting fees from Genentech/Roche, Alexion, Horizon, Sanofi, and UCB. He has also received research support from Genentech/Roche, Alexion, Horizon, Sanofi, and UCB.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.