
Abstract
Background
Constipation and faecal incontinence are not so uncommon in patients with multiple sclerosis, impairing quality of life. The gut microbiota is altered in multiple sclerosis patients and likely contributes to disease pathogenesis. Trans-anal irrigation has been proven to allow treatment of neurogenic bowel dysfunction and may affect gut microbiota.
Objectives
The primary outcome was trans-anal irrigation effectiveness on constipation and faecal incontinence. The secondary outcome was gut microbiota profiling compared to healthy subjects and during trans-anal irrigation adoption.
Methods
We conducted a prospective cohort study on multiple sclerosis patients, screened with Patient Assessment of Constipation Quality of Life questionnaire before undergoing constipation and faecal incontinence scoring, abdomen X-ray for intestinal transit time, compilation of food and evacuation diaries and faecal sample collection for gut microbiota analysis before and after 4 weeks of trans-anal irrigation.
Results and Conclusions
Eighty patients were screened of which nearly half had intestinal symptoms. The included population (n = 37) was predominantly composed of women with significantly longer disease duration, higher mean age and disability than the excluded one (p < 0.05). Twelve patients completed the trans-anal irrigation phase, which led to significant improvement of bowel dysfunction symptom-related quality of life, increase in gut microbiota diversity and reduction of the proportions of pro-inflammatory taxa (p < 0.05). Trans-anal irrigation was safe, satisfactory and could help counteract multiple sclerosis-related dysbiosis.
Keywords
Introduction
Constipation and faecal incontinence are not so uncommon in patients with multiple sclerosis (MS), often coexisting and alternating especially in patients with higher disability and longer illness, reducing the quality of life (QoL) due to limitations in social, occupational and emotional life.1,2 Among the various treatments directed towards neurogenic bowel dysfunctions, trans-anal irrigation (TAI) is an emerging option that allows for mechanical bowel emptying. TAI of the rectum and colon is an irrigation method designed to assist the evacuation of faeces by introducing water from the anus with a purpose-made device. TAI consents to restore the bowel function in case of both constipation and faecal incontinence, by regularly emptying the bowel, obtaining a bowel routine with a possibility to choose the time and place of evacuation.3,4 Its efficacy and safety have been proven, but patient acceptability and degree of effectiveness on intestinal transit time (TT) have not been defined yet.
There is growing evidence demonstrating alterations in the gut microbiota (GM) of MS patients, its correlation with intestinal disorders and plausible immunological links with MS pathogenesis.5,8 In particular, the studies show an enrichment of pathobionts involved in increasing intestinal permeability and inducing the production of pro-inflammatory cytokines.9,10 On the other hand, as in most dysbiotic states, the GM of MS patients is depleted in typical health-associated taxa, such as short-chain fatty acid producers from the Lachnospiraceae and Ruminococcaceae families, and other anti-inflammatory commensals. 7
To our knowledge, the relationship between changes in GM composition and TAI adoption has never been explored in MS, as well as in other neurologic diseases, except for a recent study on paediatric patients with Spina bifida, who presented increased abundance in Roseburia after TAI treatment, associated with improved constipation and reduced urinary tract infections. 11 The objective of the presented study was to evaluate the efficacy of TAI on bowel dysfunction correlated to MS, and its impact on the GM structure.
Materials and methods
This was a monocentric, prospective, cohort, observational study conducted at the University Hospital of Ferrara. All consecutive patients referred to the MS Neurological Center of Ferrara University Hospital were screened from May 2018 to November 2019 by administering the Patient Assessment of Constipation QoL questionnaire (PAC-QoL), a self-filled instrument divided into two sections: B1–B6 section aims at documenting intestinal disorders on everyday life, while section B7 measures patient satisfaction with own's bowel management. 12 The inclusion criteria were MS patients, both relapsing-remitting (RR) and progressive (active and inactive) form, aged ≥18 years, residence in the Emilia Romagna Region (Italy) and PAC-QoL score ≥32, as an arbitrary inclusive score from previous epidemiological studies. 13 The exclusion criteria were Expanded Disability Status Scale (EDSS) ≥7, other neurological diseases, inflammatory bowel diseases (IBD), endocrine disorders, drugs affecting intestinal transit, intestinal bleeding in the last 3 months and ongoing infection.
The primary outcome was to evaluate the efficacy of TAI on MS-related constipation and faecal incontinence. The secondary outcome was the analysis of the baseline diversity and composition of GM compared to healthy Italians matched by GM-associated confounding factors (age, sex and geography), and of GM variation during TAI adoption.
Diverse questionnaires exploring different aspects of functional intestinal disorders were adopted as primary outcome measures to better focus and compare functional results before and after TAI treatment. In addition to PAC-QoL 12 and the Neurogenic Bowel Dysfunction Score (NBD), 14 we used the Agachan-Wexner (A-W) Constipation score 15 and the Obstructed Defecation Syndrome (ODS) questionnaire 16 to measure constipation-related outcome results; we adopted the Fecal Incontinence Cleveland Clinic Index (FI-CCI) 17 to measure faecal incontinence-related outcome results.
Moreover, TAI effectiveness was determined by the variation of the TT, 18 the Bristol Stool Form Scale (BSFS) 19 and patient satisfaction, measured by the Visual Analogue Scale (VAS). 20 Figure 1 summarizes the study protocol.

Summary of the study protocol.
MS patients with PAC-QoL score ≥32 were offered a visit at the Colorectal Clinic where their dietary and evacuation habits were investigated in an interview and they filled out the above-mentioned questionnaires. Patients were given 7-day food and evacuation diaries, where recording also stool consistency according to BSFS, and a container for the faecal sample for GM analysis that was sent on ice to the Pharmacy and Biotechnology Department of the University of Bologna. Patients underwent radiologic TT study with radiopaque markers according to the Bouchoucha procedure revised by Abrahamsson. 18 Food diaries were analyzed by a dietician. Patients who completed the diagnostic phase were proposed to adopt TAI with the use of the Peristeen device (Coloplast A/S, Humblaebeck, Denmark), which consists of a disposable rectal probe and a water tank. 4 Water is instilled into the rectum by an insufflation system that can be adjusted by patients: the irrigation volume was 400 ml on alternate days. TAI training was carried out by the healthcare personnel. Afterwards, the patients continued TAI use independently for 4 weeks, scheduling the sessions to collect the faecal sample once a week but the day after the irrigation, and storing it in their home freezer. After 4 weeks of TAI use, patients filled in again the questionnaires mentioned above, brought back the food and evacuation diaries, and the four faecal samples were collected with the timing mentioned above; moreover, the TT study was repeated. Finally, overall satisfaction with TAI treatment by VAS and any adverse events (AEs) at 1 and 24 months after treatment were recorded. Patients underwent neurological and colorectal examinations every 6 months during the 24-month follow-up.
GM analysis by Illumina sequencing
Microbial DNA was extracted from faeces using the repeated bead-beating plus column method, as previously described. 21 The V3–V4 hypervariable regions of the 16S rRNA gene were amplified using 341F and 785R primers, and then sequenced on an Illumina MiSeq platform (Illumina, San Diego, CA, USA) at Wellmicro Srl (Bologna, Italy). Sequencing reads were deposited in the National Center for Biotechnology Information Sequence Read Archive (NCBI SRA; BioProject ID PRJNA825499).
Raw sequences were processed using QIIME with default parameters. 22 Length and quality-filtered sequences were clustered into Operational Taxonomic Units (OTUs) at 97% similarity using UCLUST, 23 and taxonomy was assigned using the RDP classifier and the Greengenes database (released May 2013). Publicly available GM sequences from healthy subjects as well as other MS patients without significant bowel symptoms were downloaded and processed as above. Specifically, for healthy controls, we recovered sequences from De Filippis et al. (23 subjects; NCBI SRA SRP042234), 24 Schnorr et al. (1 Italian; MG-RAST mgp12183) 25 and Biagi et al. (4 elderly and 2 young subjects; MG-RAST mgp17761) 26 (mean age, 50.1 years; female/male ratio, 26/4). For MS patients without significant bowel symptoms, we recovered sequences from Saresella et al. (18 subjects; NCBI SRA PRJNS633233) 7 (mean age, 51.1 years; female/male ratio, 12/6). Subjects were selected based on GM-associated confounding factors (i.e. age, sex, geographical location and even drug intake for MS patients) to minimize potential bias. Furthermore, all faecal samples had been processed in the same laboratory and then subjected to the same analysis steps. Alpha diversity was estimated using Chao1, the number of observed OTUs and the inverse Simpson index. For beta diversity, Principal Coordinates Analysis (PCoA) was performed on weighted and unweighted UniFrac distances, as well as Bray–Curtis dissimilarity calculated on genus-level relative abundances.
Statistical analysis
The calculation of the study size was based on the overall reported success rate of TAI of 50% on MS-related constipation and faecal incontinence. 3 Given that about 200 patients are visited each year at the MS centre, with an expectation of intestinal dysfunction in about 50% of patients visited and an assumed dropout rate of 20% at 12 months, the final sample size was determined to be 80 patients. The Shapiro–Wilk test was used to assess the normality of the distribution of continuous variables. In the presence of symmetry of the distributions, the variables were represented with mean and SD or, in case of non-normal distribution, with median and interquartile range [1Q–3Q]; categorical data were expressed as total numbers and percentages.
Statistical comparisons of continuous variables were assessed using the Mann–Whitney test for unpaired variables and the Wilcoxon signed-rank test for paired variables. The Spearman's rank correlation coefficient (ρ) was used to calculate the correlation between continuous variables. All analyses were performed using Stata 15.1 SE (Stata Corporation, College Station, TX, USA). As for GM, statistical analyses were carried out on R version 3.6.2 (https://www.r-project.org/) using the packages ‘made4’ and ‘vegan’. A permutation test with pseudo-F ratio was used to assess the significance of separation in PCoA. The Wilcoxon test (paired or unpaired as needed) was used to assess significant differences in alpha diversity and relative taxon abundance between groups, while the Kruskal–Wallis test was used for multiple comparisons. Kendall rank correlation test was used to assess associations between genus-level relative abundances and MS-related bowel dysfunction variables. When necessary, p-values were corrected for multiple comparisons using the Benjamini–Hochberg method. A p-value <0.05 was considered statistically significant, while a p-value <0.1 a tendency.
Results
The total duration of the study was 3 years. Of the 80 MS patients recruited, 37 (46.25%) had a PAC-QoL value
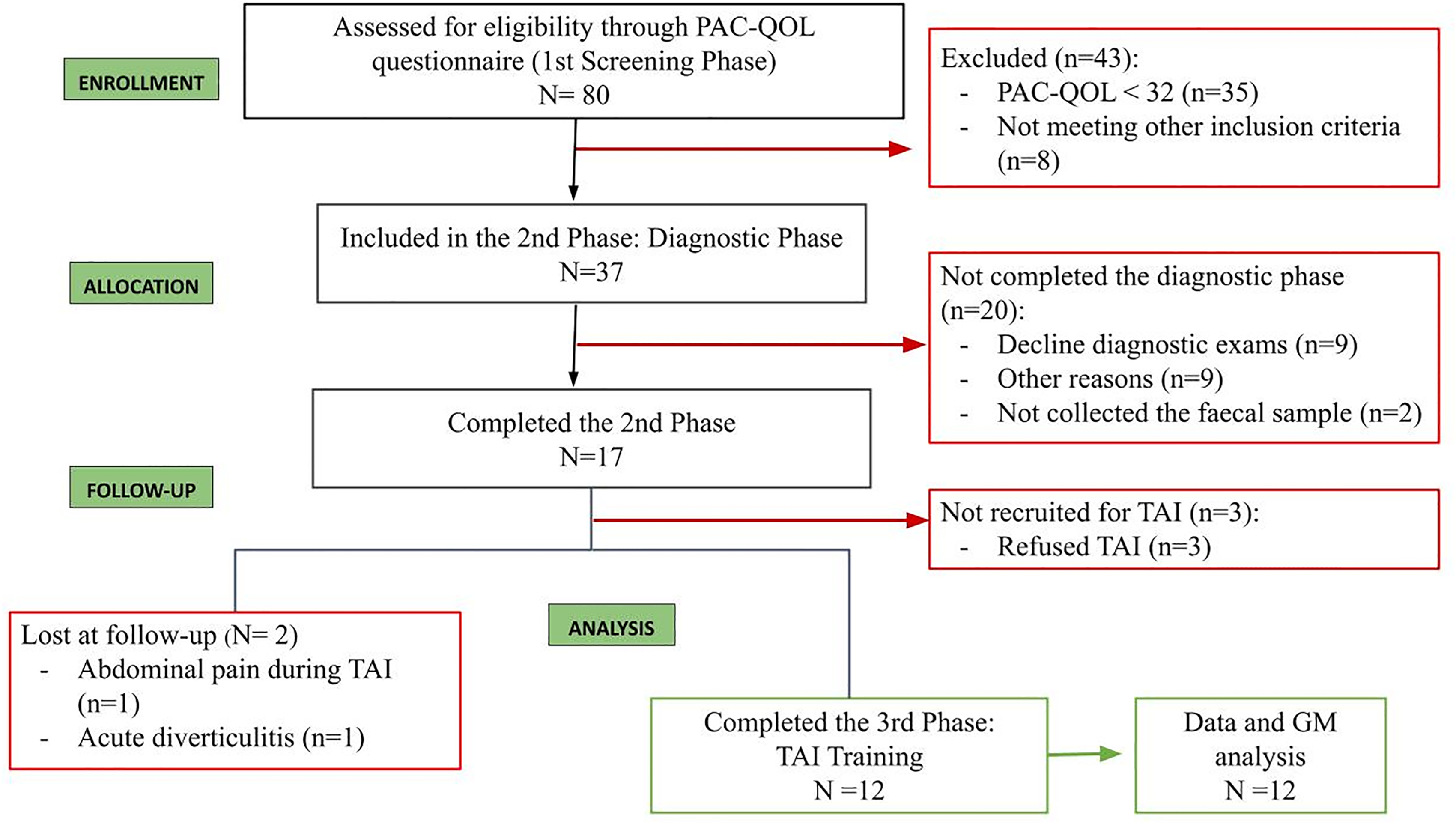
Flow diagram summarizing the phases of patient enrolment according to STROBE statement.
Demographic (a) and questionnaire (b) baseline characteristics of the study population (*for statistical significance).
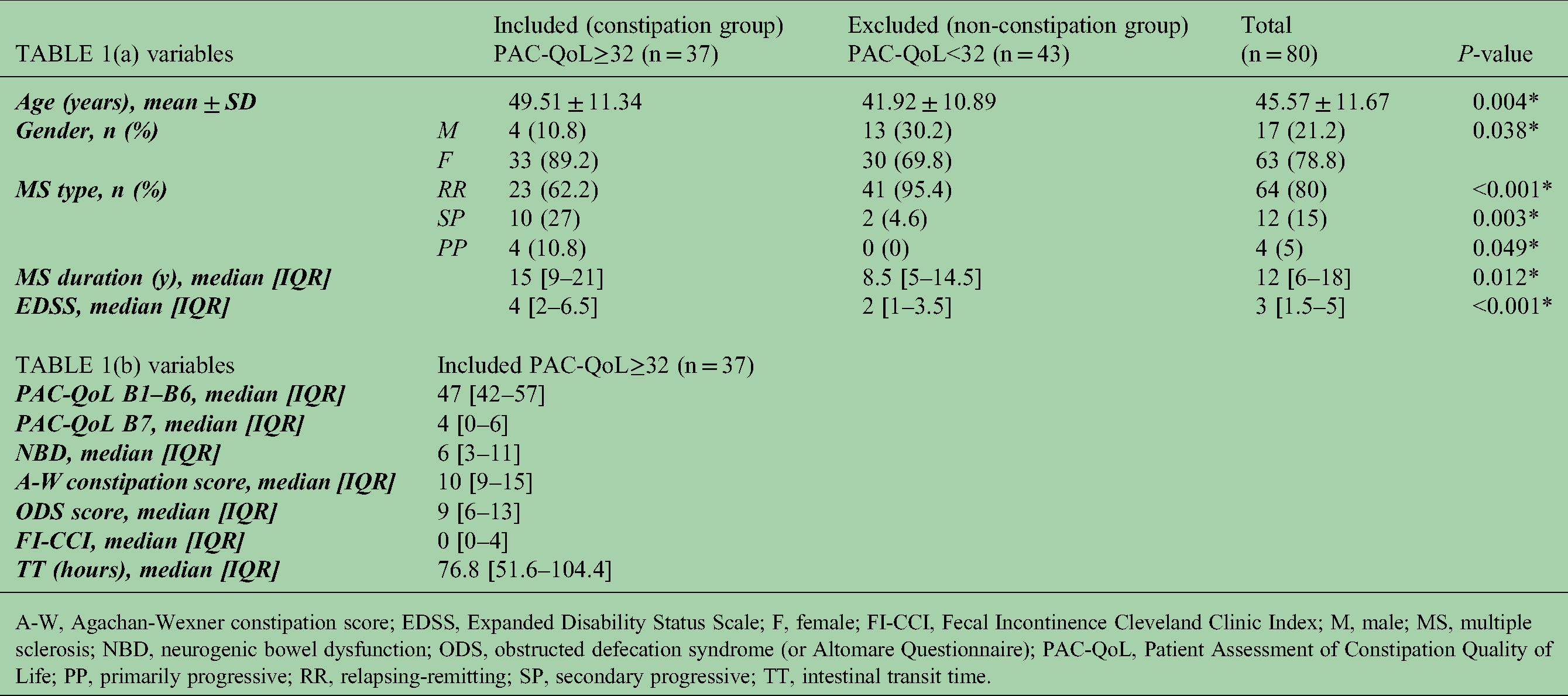
A-W, Agachan-Wexner constipation score; EDSS, Expanded Disability Status Scale; F, female; FI-CCI, Fecal Incontinence Cleveland Clinic Index; M, male; MS, multiple sclerosis; NBD, neurogenic bowel dysfunction; ODS, obstructed defecation syndrome (or Altomare Questionnaire); PAC-QoL, Patient Assessment of Constipation Quality of Life; PP, primarily progressive; RR, relapsing-remitting; SP, secondary progressive; TT, intestinal transit time.
Differences between pre and post-trans-anal irrigation (TAI) adoption in the 12 patients who completed the study.

A-W, Agachan-Wexner constipation score; FI-CCI, Fecal Incontinence Cleveland Clinic Index; NBD, neurogenic bowel dysfunction; ODS, obstructed defecation syndrome (or Altomare Questionnaire); PAC-QoL, Patient Assessment of Constipation Quality of Life; TT, intestinal transit time.
Median follow-up was 28 months [IQR: 18−33]: 83.3% of patients were still using TAI after 24 months and no relapse of disease-related symptoms occurred.
We observed two adverse effects (AEs): a woman who had a history of diverticulosis discontinued TAI for diverticulitis. After conservative medical therapy she was immediately well, but we preferred not to resume TAI treatment. Another woman who had a history of endometriosis interrupted TAI treatment at the beginning because of non-specific abdominal pain probably related to adhesion syndrome. Even after stopping TAI treatment, the patient had further episodes of abdominal pain and underwent surgical lysis of adhesions successively.
GM analysis
GM was profiled for 17 MS patients at baseline and for 12 of these during TAI adoption. The 16S rRNA gene sequencing was performed on a total of 66 faecal samples, yielding 1,573,181 reads (mean ± SD; 23,836 ± 8163) that were clustered into 12,107 OTUs. The GM of MS patients at baseline (T0) was compared with that of age- and sex-matched healthy Italians living in the same geographical area, from publicly available databases.24,26 According to the inverse Simpson index, MS patients tended to show greater alpha diversity (p = 0.08) (Figure 3a). PCoA of inter-individual variation, based on Bray–Curtis dissimilarity between the genus-level profiles, showed significant separation between groups (p = 0.001) (Figure 3b). The GM profile of MS patients was characterized by profound deconstruction even at high taxonomic levels. In particular, we found significantly increased proportions of the phylum Verrucomicrobia, Actinobacteria and Proteobacteria, and reduced amounts of Bacteroidetes (p < 0.05) (Supplementary Figure 4A).

The gut microbiota of multiple sclerosis (MS) patients compared to healthy controls. (a) Alpha diversity estimated according to the inverse Simpson index for MS patients at baseline (T0) and age- and sex-matched healthy controls from the same geographical area. A trend towards greater diversity was observed for MS patients (p = 0.08; Wilcoxon test). (b) Principal Coordinates Analysis (PCoA) based on Bray–Curtis dissimilarity between the genus-level profiles of MS patients and healthy controls. Significant separation between groups was found (p = 0.001; permutation test with pseudo-F ratio). Ellipses include a 95% confidence area based on the standard error of the weighted average of sample coordinates. (c) Boxplots showing the relative abundance distribution of genera differentially represented between study groups (p < 0.05; Wilcoxon test).
At family level, the GM of MS patients was enriched in generally subdominant taxa, such as Actinomycetaceae, Methanobacteriaceae, Verrucomicrobiaceae, Peptostreptococcaceae, Turicibacteraceae, Coriobacteriaceae, Enterococcaceae, Enterobacteriaceae and Streptococcaceae, while depleted of the health-associated family Ruminococcaceae (p < 0.05) (Supplementary Figure 4B). The main discriminating genera included Akkermansia, Methanobrevibacter and several pro-inflammatory and pathobiont taxa, such as Collinsella, Eggerthella and Adlercreutzia (all belonging to Coriobacteriaceae), Enterococcus, Streptococcus, [Ruminococcus] and [Eubacterium], whose proportions were greater in MS patients than in healthy controls (p < 0.05) (Figure 3c). On the other hand, the GM of MS patients was depleted in health-associated short-chain fatty acid-producers, such as Coprococcus, Roseburia and Lachnospira (p < 0.05). As for MS type, we found that Streptococcus and [Ruminococcus] tended to be enriched in the SP form (p ≤ 0.07), while Clostridiales in the RR form (p = 0.03). Notably, all the differences reported above (except for the increase in alpha diversity and Blautia proportions) were also observed when considering only the 12 MS patients who subsequently adopted and completed TAI treatment (Supplementary Figures 5 and 6). Furthermore, when comparing the patients’ GM with that of other MS patients without significant bowel symptoms from a previous study 7 (Supplementary Figure 7), we found that the former exhibited reduced alpha diversity (p = 0.01) and significantly segregated from the latter in a Bray–Curtis dissimilarity-based PCoA between genus-level profiles (p = 0.01). Taxonomically, the patients in the present study showed reduced proportions of Lachnospira, Coprococcus and Ruminococcus, and increased proportions of Actinomyces and Turicibacte, compared to patients without significant bowel symptoms (p < 0.05).
GM dynamics were then assessed over time during TAI adoption, from baseline (T0), once a week up to 1 month. The alpha diversity metrics used (Chao1 index and the number of observed OTUs) showed a significant increase in diversity over time (p < 0.05) (Figure 4a), while no difference was observed in beta diversity, based on weighted and unweighted UniFrac distances (p = 1) (Figure 5).

The gut microbiota dynamics in multiple sclerosis (MS) patients undergoing trans-anal irrigation (TAI). (a) Alpha diversity estimated according to the number of observed Operational Taxonomic Units (OTUs) and the Chao1 index. A significant increase was observed over time with both metrics (*, p < 0.05; Wilcoxon test). (b) Bar plots showing the phylum (left) and family (right)-level composition of the gut microbiota (GM) of MS patients during TAI adoption. Only taxa with relative abundance >0.1% in at least 1 sample are shown. (c) Boxplots showing the relative abundance distribution of genera differentially represented over time (*, p < 0.05; #, 0.05<p < 0.1; Wilcoxon test). T0, baseline; T1–T4, samples collected once a week during TAI adoption for up to one month.

Beta diversity of the gut microbiota of multiple sclerosis (MS) patients during trans-anal irrigation (TAI) adoption. Principal Coordinates Analysis (PCoA) based on unweighted (left) and weighted (right) UniFrac distances between faecal samples from MS patients during TAI adoption. No significant separation was found over time (p = 1; permutation test with pseudo-F ratio). Ellipses include a 95% confidence area based on the standard error of the weighted average of sample coordinates. T0, baseline; T1–T4, samples collected once a week during TAI adoption for up to 1 month.
Overall, the phylum- and family-level compositional structure of GM was maintained over time (Figure 4b), except for an increase in the proportions of Methanobacteriaceae and Peptostreptococcaceae, and a decrease in Prevotellaceae (p < 0.05). At genus level, the main changes were the increase over time in Methanobrevibacter, Adlercreutzia, Dorea, Acinetobacter and Ruminococcus, and the decrease in Prevotella, Dialister and Phascolarctobacterium (p < 0.05) (Figure 4c). Proportions of Enterococcus also tended to decrease over time (p < 0.1). After a significant reduction at T1, both Faecalibacterium and Veillonella recovered the same relative abundances as at baseline.
Correlations between the relative abundances of bacterial taxa and MS-related bowel dysfunction variables pre and post-TAI adoption were specifically sought (Figure 6). Health-associated taxa such as Bifidobacterium and Faecalibacterium were negatively correlated with FI-CCI (p = 0.03, tau = −0.562 and p = 0.01, tau = −0.665, respectively). Other short-chain fatty acid producers from the Lachnospiraceae family showed expected correlations with PAC-QoL B7 (Anaerostipes, p = 0.06, tau = 0.488), ODS (Anaerostipes, p = 0.07, tau = -0.482; Blautia, p = 0.03, tau = −0.548), A-W constipation score (Anaerostipes, p = 0.07, tau = −0.482) and TT (Blautia, p = 0.09, tau = −0.432).

Associations between genus-level relative abundances and ms-related bowel dysfunction variables before and after the adoption of trans-anal irrigation (TAI). Statistically significant correlations (p < 0.05) or trends (p < 0.1) with an absolute Kendall rank correlation coefficient >0.4 are shown. Black dots, T0 (baseline); blue dots, T4 (after 1 month of TAI adoption).
On the other hand, we found a positive correlation between genera whose proportions decreased after TAI adoption and NBD (Prevotella, p = 0.03, tau = 0.565), ODS (Enterococcus, p = 0.05, tau = 0.575) and FI-CCI (Phascolarctobacterium, p = 0.07, tau = 0.525).
Discussion
In the present study, nearly half of non-preselected MS patients had bowel dysfunction symptoms, as was reported by Preziosi et al., 1 but in contrast to Bisecco et al. 2 who found 22% of MS patients with bowel dysfunction. Only partly, the incidence of bowel dysfunction is related to the high disability with EDSS values up to 6.5 and reduced mobility, so this disagreement could be also explained by the different diagnostic tools used: while Bisecco et al. 2 utilized the NBD score, in the current study we adopted the PAC-QoL that investigates not only the severity of constipation but all the symptoms deriving from bowel dysfunction, such as abdominal pain or bloating. Moreover, we adopted multiple scores to investigate the QoL (PAC-QoL and NBD) exploring different aspects of bowel disorders with the A-W Constipation score, ODS score and FI-CCI, evaluating TT, BSFS, diet and GM changes too, before and after TAI treatment. Our results demonstrated that the adoption of TAI with the Peristeen device resulted in a significant clinical improvement in bowel symptoms, with PAC-QoL scores and all other assessment tools being significantly reduced after 4 weeks of treatment, as confirmed by previous studies that have established the efficacy and tolerability of Peristeen device on defecation disorders in patients with various neurological, dysfunctional and post-surgical diseases.4,27 The regular use of Peristeen in standardized times and volumes obtained the emptying of the intestinal contents in few weeks, with successful results also in terms of patient satisfaction and adherence to treatment; in fact, over 80% of patients continued to use Peristeen at 24 months, and patient satisfaction remained high over time. The AEs observed at the beginning of treatment with TAI in two patients do not represent a safety concern related to the procedure itself but to patient selection: diverticulosis and endometriosis are relative contraindications to the use of TAI.
The TT did not show significant variations after TAI treatment. 18 This is actually not surprising for two main reasons: (i) the 76.8 h pre-TAI average value was not much higher than normal and (ii) the complexity of the mechanisms underlying the neurogenic bowel dysfunction results from a combined deficit of colon peristalsis and rectal emptying with chronic faecal retention.28,29 Similarly, stool consistency recorded by BSFS, and patient's diet did not vary over time, confirming the dietary imbalances detected in MS patients. 30 TAI by itself cannot change them, unless being associated with a proper dietary regimen and/or supplementation with prebiotics and/or probiotics. 31
Regarding the analysis of GM, our results confirm that the composition of GM in MS patients is profoundly different compared to a healthy population of the same age and sex, coming from the same geographical area.5,6,8 The following dysbiotic features were in fact observed at baseline: i) lower relative abundance of health-associated taxa, mainly short-chain fatty acid producers from the Lachnospiraceae (i.e. Coprococcus, Roseburia and Lachnospira) and Ruminococcaceae families and (ii) larger proportions of the mucus lover Akkermansia and a range of generally subdominant taxa with pathogenic potential, including Coriobacteriaceae (i.e. Collinsella, Adlercreutzia and Eggerthella), Enterobacteriaceae, Enterococcus, Streptococcus, [Ruminococcus] and [Eubacterium]. It is worth noting that most of the latter have already been found to be overrepresented in MS patients and are known to degrade mucus and/or to be associated with loss of barrier integrity and pro-inflammatory responses,5,9 potentially contributing to exacerbating MS symptoms. This could also be one of the possible explanations for the earlier onset of intestinal than neurological symptoms in some individuals. With specific regard to bowel dysfunction, it should be noted that the dysbiosis of the patients in our study only partially overlapped that of other patients without significant bowel symptoms, which on the one hand supports the involvement of some microbes in MS in general (e.g. Akkermansia and Collinsella) and on the other hand suggests that other microorganisms may be specifically related to bowel dysfunction. In particular, MS patients with bowel symptoms showed even smaller relative abundances of beneficial microbes (i.e. Lachnospira, Coprococcus and Ruminococcus) and even higher proportions of Actinomyces and Turicibacter. Although not much information is available on these microorganisms, Turicibacter has recently been identified as a potential gut inflammation-related taxon, 32 as well as a possible marker of the chronic-progressive form of MS, 33 and it is known that Actinomyces could aggravate lesions caused by inflammatory states by inducing changes in the enteric environment and modulating immune responses. 34 As expected, MS-related GM alteration was more severe in patients with progressive form, who were particularly enriched in Streptococcus and [Ruminococcus]. On the other hand, it must be said that these dysbiotic features found in MS patients before TAI are different from those found in SCI patients (Spinal Cord Injury), reinforcing the hypothesis that MS dysbiosis is truly peculiar, potentially pathognomonic, so it may indeed have an etiopathogenetic role. 35
The adoption of TAI did not have a significant impact on the overall structure of GM, but it did lead to an increase in diversity (a hallmark of healthy gut), and a number of compositional changes, some of which may be favourable in the context of MS. In particular, we observed a reduction in the proportions of Prevotella, which has already been found enriched in MS patients as well as in subjects with other autoimmune disorders, where it may play a role in supporting an inflammatory tone.8,36 We also found a tendency towards reduced amounts of Enterococcus, a known pathobiont that was overrepresented at baseline, and significantly increased amounts of Ruminococcus, a short-chain fatty acid producer generally prevalent in healthy subjects, which was largely depleted prior to TAI adoption. Interestingly, Prevotella, Enterococcus and health-associated taxa (such as bifidobacteria, Lachnospiraceae and Ruminococcaceae members) showed expected correlations with MS-related bowel dysfunction variables. It is therefore tempting to speculate that, while not dramatically impacting the GM structure, the adoption of TAI could favour some microbial rearrangements associated with better overall intestinal health. However, it should be noted that after treatment, MS patients also showed increased levels of Peptostreptococcaceae, less characterized microorganisms but generally believed to be pro-inflammatory, 37 and Methanobrevibacter, an archaeon typically enriched in MS. 5
Some limitations of the current study were the single centre, the use of PAC-QoL to screen the population only for constipation, and the small sample. However, the study protocol required significant patient engagement and half of the included patients did not complete the diagnostic phase. It should be pointed out that the patients were screened from MS Neurological Centre to assess the presence of intestinal dysfunction even if they did not report intestinal symptoms as a priority over other symptoms. Moreover, once the diagnostic phase was completed, 82.3% of patients accepted TAI but two patients discontinued it due to clinical problems. If we had offered TAI directly to all included patients without the diagnostic phase, the adherence rate to TAI treatment would probably have been higher. Another confounding variable to consider is the fact that the increased engagement with clinicians monitoring patient diet/bowels over the study period could have influenced patient-reported symptoms and QoL, but not the objective scores obtained from the A-W Constipation, ODS and FI-CCI questionnaires. Based on these limitations, we are planning to build a multicentre study, with a larger number of patients screened with NBD score, focused on functional insights into the GM role in MS and related bowel dysfunction, possibly employing other omics techniques, such as shotgun metagenomics and metabolomics.
Conclusions
This prospective single-centre study in the MS population demonstrates that TAI with the Peristeen device is not only safe and satisfactory, but also improves symptoms and QoL related to neurological bowel dysfunction, which affects approximately half of the MS population. Furthermore, during TAI adoption, GM diversity increased, while the proportions of potential pathobionts decreased. These changes in GM composition are not consequences of dietary regimen improvements, so the healthier intestinal environment can be fully ascribed to the TAI effect on colonic dysfunction. Future studies with larger cohorts are needed to better understand the role of GM and its therapeutic implications which would lead to the development of gut-directed treatments.
Supplemental Material
sj-docx-1-mso-10.1177_20552173221109771 - Supplemental material for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study
Supplemental material, sj-docx-1-mso-10.1177_20552173221109771 for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study by Simona Ascanelli, Cristina Bombardini, Laura Chimisso, Paolo Carcoforo, Silvia Turroni, Federica D’Amico, Maria Luisa Caniati, Eleonora Baldi, Valeria Tugnoli, Chiara Morotti, Giorgia Valpiani and Gabriele Bazzocchi in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-tif-2-mso-10.1177_20552173221109771 - Supplemental material for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study
Supplemental material, sj-tif-2-mso-10.1177_20552173221109771 for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study by Simona Ascanelli, Cristina Bombardini, Laura Chimisso, Paolo Carcoforo, Silvia Turroni, Federica D’Amico, Maria Luisa Caniati, Eleonora Baldi, Valeria Tugnoli, Chiara Morotti, Giorgia Valpiani and Gabriele Bazzocchi in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-tif-3-mso-10.1177_20552173221109771 - Supplemental material for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study
Supplemental material, sj-tif-3-mso-10.1177_20552173221109771 for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study by Simona Ascanelli, Cristina Bombardini, Laura Chimisso, Paolo Carcoforo, Silvia Turroni, Federica D’Amico, Maria Luisa Caniati, Eleonora Baldi, Valeria Tugnoli, Chiara Morotti, Giorgia Valpiani and Gabriele Bazzocchi in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-tif-4-mso-10.1177_20552173221109771 - Supplemental material for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study
Supplemental material, sj-tif-4-mso-10.1177_20552173221109771 for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study by Simona Ascanelli, Cristina Bombardini, Laura Chimisso, Paolo Carcoforo, Silvia Turroni, Federica D’Amico, Maria Luisa Caniati, Eleonora Baldi, Valeria Tugnoli, Chiara Morotti, Giorgia Valpiani and Gabriele Bazzocchi in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-tif-5-mso-10.1177_20552173221109771 - Supplemental material for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study
Supplemental material, sj-tif-5-mso-10.1177_20552173221109771 for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study by Simona Ascanelli, Cristina Bombardini, Laura Chimisso, Paolo Carcoforo, Silvia Turroni, Federica D’Amico, Maria Luisa Caniati, Eleonora Baldi, Valeria Tugnoli, Chiara Morotti, Giorgia Valpiani and Gabriele Bazzocchi in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-tif-6-mso-10.1177_20552173221109771 - Supplemental material for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study
Supplemental material, sj-tif-6-mso-10.1177_20552173221109771 for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study by Simona Ascanelli, Cristina Bombardini, Laura Chimisso, Paolo Carcoforo, Silvia Turroni, Federica D’Amico, Maria Luisa Caniati, Eleonora Baldi, Valeria Tugnoli, Chiara Morotti, Giorgia Valpiani and Gabriele Bazzocchi in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-tif-7-mso-10.1177_20552173221109771 - Supplemental material for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study
Supplemental material, sj-tif-7-mso-10.1177_20552173221109771 for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study by Simona Ascanelli, Cristina Bombardini, Laura Chimisso, Paolo Carcoforo, Silvia Turroni, Federica D’Amico, Maria Luisa Caniati, Eleonora Baldi, Valeria Tugnoli, Chiara Morotti, Giorgia Valpiani and Gabriele Bazzocchi in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-tif-8-mso-10.1177_20552173221109771 - Supplemental material for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study
Supplemental material, sj-tif-8-mso-10.1177_20552173221109771 for Trans-anal irrigation in patients with multiple sclerosis: Efficacy in treating disease-related bowel dysfunctions and impact on the gut microbiota: A monocentric prospective study by Simona Ascanelli, Cristina Bombardini, Laura Chimisso, Paolo Carcoforo, Silvia Turroni, Federica D’Amico, Maria Luisa Caniati, Eleonora Baldi, Valeria Tugnoli, Chiara Morotti, Giorgia Valpiani and Gabriele Bazzocchi in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Acknowledgements
The authors would like to thank Coloplast, Italy for substantive contribution with use of the Peristeen device.
Author’s contribution
Simona Ascanelli: Conception and design, analysis and interpretation of data, drafting the article and final approval of the submitted version.
Cristina Bombardini: Drafting and revising critically the article and final approval of the submitted version.
Silvia Turroni, Federica D’Amico, Eleonora Baldi, Maria Luisa Caniatti and Laura Chimisso: Acquisition, analysis and interpretation of data, revising critically the article and final approval of the submitted version.
Giorgia Valpiani and Chiara Morotti: Analysis and interpretation of data, revising critically the article and final approval of the submitted version.
Paolo Carcoforo, Valeria Tugnoli and Gabriele Bazzocchi: Conception and design, revising critically the article and final approval of the submitted version.
The entire manuscript has been revised according to the STROBE statement checklist and guidelines.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the local Ethics Committee with registration number UHFerrara170485. All procedures performed in this study involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was also registered on ClinicalTrials.gov with identifier number NCT04599595.
Consent to participate and for publication
Informed consent to participate and for publication was obtained from all individual participants included in the study, legal guardians or parents where possible. All information was kept confidential at all times, and data were collected in a uniquely coded manner for each patient so that biographical data could not be traced.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.