
Abstract
Background
The purpose of this study was to assess family planning (FP) among women with multiple sclerosis (WwMS).
Methods
We invited 604 WwMS to answer a survey focused on FP: a) Temporal relationship between pregnancy and the diagnosis of multiple sclerosis; b) History of FP; c) Childbearing desire; d) Information on family planning. Comparisons between pregnancy and not pregnancy after MS, as well as, planned and unplanned pregnancy were analyzed. Multivariate and univariate analyses were used to assess the impact of independent variables and FP
Result
428 (71.7%) WwMS completed the survey. A 19.1% got pregnant after MS diagnosis and we evaluated FP in the last pregnancy, 56.1% patients had a planned pregnancy. Professional addressing FP (OR = 0.27, 95%-CI 0.08-0.92, p = 0.03) and non-injection drug treatment before pregnancy (OR = 2.88, 95%-CI 1.01-8.21, p = 0.047) were independent predictors of unplanned pregnancy in our multivariate model. Among WwMS ≤ 40 years, 48.7% had future childbearing desire. Young age (p < 0.001), PDDS <3 (p = 0.018), disease duration <5 years (p = 0.02), not childbearing before MS diagnosis (p < 0.001) and neurologist addressing family planning (p = 0.01) were significantly associated with childbearing desire.
Conclusions
This research highlights that pregnancy remains an important concern among WwMS.
Introduction
Multiple sclerosis (MS) is a chronic autoimmune disease of the central nervous system that predominantly affects women three times more frequently than men. MS is usually diagnosed between the ages of 20 and 40 years: a time in life when many people have the desire to start a family and, therefore, consider becoming pregnant. 1 For many years it has been thought that pregnancy could have a negative impact on the disease outcome but several studies have demonstrated that most women with MS (WwMS) can have normal pregnancies and deliver healthy children.2–4 Additionally, an increasing number of disease-modifying therapies (DMTs) have become available during the last years with some concern about the potential negative consequences of their use during pregnancy. 5 However, recent studies have shown that certain DMTs can be used with caution during part of pregnancy or, at least, until the moment of conception,6–9 while other DMTs may have negative effects on the fetus and newborn.10–12 This emphasizes the importance of providing adequate counseling to WwMS regarding family planning during the reproductive age.
There are several reports in the literature on the use of simple self-report measures or surveys that assess how MS patients plan their pregnancy.13–15 This study highlights that pregnancy remains an important yet unresolved concern in the treatment of MS patients.
While conclusions based on results of simple self-report measures or surveys have limitations, they may be the optimal method to understand which steps should be taken to improve family planning. Most of the studies on family planning in WwMS are carried out on Anglo-Saxon populations where the cultural and idiosyncratic differences with Latin American people is quite extensive. 16 Being able to learn about local data on this subject is of great value, since it would allow us to implement different strategies to improve family planning in clinical practice. The purpose of this study is to evaluate family planning in WwMS, factors associated with pregnancy after MS diagnosis and planned or unplanned pregnancy. Potential effect on treatment decisions in an Argentinean population was also analyzed.
Methods
Patients
We performed a cross-sectional study between March and April 2020. Six hundred and four WwMS were invited to participate in an anonymous, voluntary, self-administered web-based survey. In order to participate, WwMS had to be ≥18 years old and be followed up by a neurologist from the MS centers included in the study. Four hundred thirty-three (71.7%) WwMS completed the survey. Demographic data were collected using a database from each of the MS centers included in the study. These data were used to select the patients who were subsequently invited to the study. Each institutional review board approved the study protocols. All patients provided electronic informed consent.
Questionnaire
The questionnaire was developed to focus on four outcomes of interest and factors related to family planning in WwMS: a) Temporal relationship between pregnancy and the diagnosis of MS b) History of family planning: c) Childbearing desire; d) Information on family planning (see variables and definitions). It was designed by two MS experts (RA and NFL) and reviewed by LP for online data collection in Spanish language. A pilot study consisting of 25 patients with a diagnosis of MS was carried out prior to the main survey. Only minor changes to the wording were made based on the pilot testing. The changes were related to improve some expressions of Spanish grammatically and adapt the medical language to an appropriate language for the patients. No questions were canceled or added at this stage and the free text option was not included. The final questionnaire consisted of 22 questions (see the final version in Supplementary Material). Clinical and demographic information such as age, sex, time since diagnosis, disease subtype and DMTs (current and prior treatment to the last pregnancy) was registered. To provide a valid and comprehensive assessment of MS-related disability we used the patient-assessed Patient Determined Disease Steps (PDDS). 17 The PDDS has nine ordinal levels ranging between 0 (normal) and 8 (Bedridden). 17 This PDDS is strongly correlated to EDSS, and especially to pyramidal, cerebellar, sensory, visual, bowel/bladder, and ambulatory functional systems. 18 In addition, the PDDS was categorized into < 3 (mild disability) and ≥ 3 (range of disability from moderate to severe).
To achieve the outcomes proposed for this study, the operational definitions of the variables of interest are listed below. Childbearing desire after MS diagnosis: WwMS with childbearing desire after the MS diagnosis or who maintained a previous desire despite the MS diagnosis. It does not refer to whether or not the woman tried to become pregnant. The response was dichotomized into “yes” or “no”. Frequency of neurologist addressing family planning: How often the neurologist had started the discussion on family planning during consultations. The response was categorized into: “never”, “occasionally” (in less than half of the consultations), “only at the patient’s request and on every consultation”. Information source related to family planning: The types of information sources were defined as “informal source”: when the information was not provided by health workers (e.g. relatives or friends, internet, other MS patients); “uncertain source”: when the patient did not remember the source of the information and “formal source” when the information was provided by health workers (physicians or patients’ organizations). Furthermore, information about the occurrence of planned or unplanned pregnancies was recorded. To avoid response and recall biases, in women with two or more pregnancies, information related only to the last pregnancy was requested. Planned pregnancy: when the patient decides to get pregnant considering the recommendations made by the neurologist related with the MS. Unplanned pregnancy: when the patient becomes pregnant without considering family planning strategies in MS patients. Childbearing desire and family planning strategy were only analyzed in the subgroup of patients ≤ 40 years. The analysis was limited to this age group, since the probability of maternity in Argentina over 40 years of age is very low (less than 5%). 19
Statistical analysis
Descriptive analyses of all variables were carried out. Results are presented as frequencies, percentages, mean, and standard deviation (SD) values. Comparisons between pregnancy and not pregnancy after MS, as well as, planned and unplanned pregnancy were analyzed using Chi-square or Fisher’s exact tests for categorical variables and t-test or Mann–Whitney U test for continuous variables, when appropriate. Unplanned pregnancy was dichotomized as follows: yes, or not. Thus, a binary logistic regression was built to identify predictors of unplanned pregnancy. The independent variables (potential predictors) such as age at last pregnancy (continuous variable), MS duration at last pregnancy (continuous variable), Motherhood before MS diagnosis (categorical variable), Information from health workers regarding family planning before the last pregnancy (categorical variable) and Non-injection drug treatment before pregnancy (categorical variable) were introduced one-by-one using the forward election approach (stepwise selection). Those variables with p < 0.20 in the univariate analysis (OR 95%CI) were considered as potential predictors and they were tested in the multivariate model all together (multivariate model). Due to the retrospective and exploratory nature of the study no adjustment for multiple comparisons was made. For all analyses, p-values < 0.05 were considered statistically significant. Data analysis was conducted using SPSS Statistics v22.
Results
General information
A total of 428 WwMS from the most representative Argentinian Provinces (Buenos Aires, Córdoba, Santa Fé and Mendoza), completed the survey. Population demographics and main characteristics are presented in Table 1. The mean age at survey was 40.5 (SD 10.94) years, almost half of the patients had had diagnosed MS for less than 5 years (49.3%) and median PDDS was 1 (IQR 3). A total of 180 (42.1%) got pregnant before MS diagnosis. Conversely, a total of 82 (19.1%) patients became pregnant after being diagnosed with MS: 78 (18.2%) became pregnant after MS diagnosis and 4 (0.9%) were pregnant at the time of the survey. Interferon was the most frequently used DMT prior to the last pregnancy; 34 out of 82 patients (41.4%). We analyzed different factors associated with pregnancy after MS diagnosis. Unchanged childbearing desire after MS diagnosis (p < 0.001), the frequency of neurologists addressing family planning (p = 0.009), neurologist explaining about risks related to DMTs and pregnancy (p < 0.001) and formal information source (information from the physicians or patient associations) on MS treatments and pregnancy (p < 0.001) were significantly associated with childbearing after MS diagnosis (Table 2).
General characteristics of the studied Argentinean cohort (n = 428).

SD: standard deviation; MS: multiple sclerosis; PDDS: Patient Determined Disease Steps scale.
Differences between women with MS who became pregnant or not after MS diagnosis.

aInformal: relatives or friends, internet, other MS patients. Formal: physicians or patients’ organizations. DMTs: Drugs modified treatment.Bold numbers mark the degree of significance.
Family planning
Among the 82 patients with childbearing after MS diagnosis, we evaluate family planning in the last pregnancy. In this context, 56.1% had a planned pregnancy and 43.9% of patients had an unplanned pregnancy. We did not find significant differences between both groups in relation to age at last pregnancy (p = 0.37), childbearing before MS diagnosis (p = 0.90) and year of the last pregnancy (p = 0.70). On the other hand, having information form health workers regarding family planning in the last pregnancy (p = 0.01)) was significantly associated with planned pregnancy. We found a trend towards the use of injectable treatments in the group of WwMS who planned their pregnancy (p = 0.07) (Table 3). As shown in Table 4, family planning addressed by the neurologist (OR = 0.27, 95%-CI 0.08-0.92, p = 0.03) and non-injection drug treatment before pregnancy (OR = 2.88, 95%-CI 1.01-8.21, p = 0.047) were independent predictors of unplanned pregnancy in our multivariate model.
Factors associated with pregnancy planning.

Note: Patients that became pregnant after being diagnosed with Multiple Sclerosis: Information related to the last pregnancy.
SD: standard deviation; Injectable drugs: Interferon or glatiramer acetate, DMT: Drug modified treatment. CM: contraception method.
a7 Injectable drugs, 3 natalizumab and 3 dimethyl fumarate.
bOther treatment: Fingolimod, dimethyl fumarate, cladribine; natalizumab, ocrelizumab.
c1 ocrelizumab, 2 fingolimod, 2 cladribine.
d19 Injectable drugs, 1 natalizumab, 2 dimethyl fumarate.Bold numbers mark the degree of significance.
Multivariate logistic regression analysis: Variables independently associated with unplanned pregnancy (n = 428).
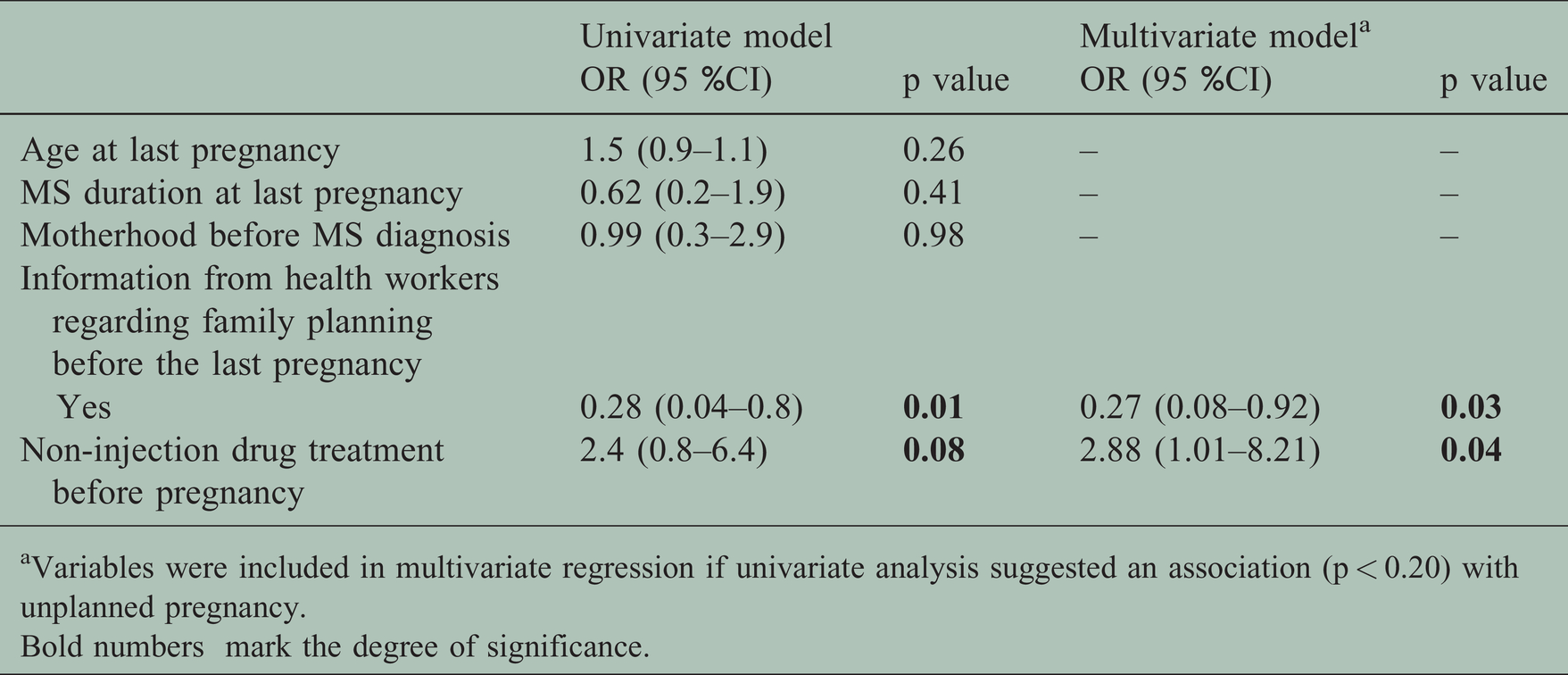
aVariables were included in multivariate regression if univariate analysis suggested an association (p < 0.20) with unplanned pregnancy.Bold numbers mark the degree of significance.
Subgroup of patients ≤ 40 years
A total of 230 WwMS ≤ 40 years were identified. The mean age at survey was 32.37 (SD 5.56) years, most of the respondents had had diagnosed MS for less than 5 yeras (43.6%) and PDDS <3 (85.6%). Most of them were under treatment with oral DMTs 118 (51.4%). A total of 169 (73.5%) were not pregnant before MS diagnosis, 15.7% WwMS became pregnant after being diagnosed with MS. Interestingly, in 47.8% of WwMS the desire to have children did not change after MS diagnosis and 38.3% answered that family planning is an important factor in relation to the choice of treatment. On the other hand, 204 (88.69%) had concerns regarding maternity and the MS diagnosis. The most frequent ones were the fear of having relapses after pregnancy (37.70%) and 7% of WwMS had concerns related to the possibility of their child inheriting the disease.
Among WwMS ≤ 40 years, 48.7% had childbearing desires at the moment of survey (future childbearing desire) and 3 patients were trying to conceive at the moment of survey. Young age (p < 0.001), PDDS <3 (p = 0.018), disease duration shorter than 5 years (p = 0.02), not having children before MS diagnosis (p < 0.001) and the family planning subject being address by the neurologist (p = 0.01) were significantly associated with the desire to have children. Family planning information was asked among WwMS with future childbearing desire. Although most patients, 86 (72.3%), received information from formal information sources (physicians or patient associations), 18 (15.1%) reported that their neurologist had never provided them with information about family planning and 38 (31.9%) said that that was only occasionally (Table 5). In this group we identified that the contraceptive methods most commonly used by the WwMS were contraceptive pills (36.2%), followed by condoms (31.9%). Only 2.5% used a combined method (Condom + pills). On the other hand, 14.3% had already discussed and understood the future family planning strategy with their neurologist, 69.2% had not yet discussed the future family planning strategy with their neurologist, while 16.5% reported not understanding the neurologist’s answer on family planning strategy.
Plans for future childbearing in women with MS.

Note: This analysis was carried out in WwMS ≤ 40 years.
SD: standard deviation; MS: multiple sclerosis; EDSS: Expanded disability status scale; MA: monoclonal antibodies; Others: azathioprine and rituximab; Injectable: glatiramer acetate, interferon. Oral drugs: fingolimod, dimethyl fumarate and teriflunomide; Monoclonal antibodies: ocrelizumab, alemtuzumab and natalizumab; PDDS: Patient Determined Disease Steps scale. NA: not applicable.Bold numbers mark the degree of significance.
Discussion
Despite a substantial amount of data on successful outcomes of pregnancy in WwMS, both newly-diagnosed and longer-term WwMS continue to express a number of concerns regarding reproductive issues. In this research, we found a high percentage of unplanned pregnancies compared to previous series.14,16,20 Similar to previous reports, 21 only less than one fifth of respondents became pregnant after MS diagnosis. In addition, we found that the frequency of neurologists addressing family planning (and explaining about risks related to DMTs) and formal information source related to family planning (defined for this study as information provided by health workers) were significantly associated with childbearing after MS diagnosis. Therefore, the lack of an active approach to the topic of family planning by the neurologist and non-injection drug treatment before pregnancy were independent predictors of unplanned pregnancy in our multivariate model. The frequency at which the topic of pregnancy was addressed by the neurologists was captured by our survey and in most cases family planning was discussed only at the patient’s request. Different studies highlighted and confirmed a gap in the doctor–WwMS communication on reproduction, pregnancy, and childbearing issues.22,23 In a previous Italian study only a minority of patients with MS had received doctor counseling to plan pregnancy or to avoid accidental maternity. 13 In a Swiss MS patients survey, only a few neurologists initiated the subject of pregnancy at each consultation, whereas a greater number did so sporadically, when the patient asked, or did not raise the topic of pregnancy at all. 14 Another study from Germany focused on investigating neurologists’ expertise in MS and pregnancy found that respondents answered about half of the questions correctly. 24 In this study, 13% of neurologists indicated not to counsel WwMS about pregnancy and send them to specialized outpatient centers, to a gynecologist, general practitioner or other neurologists. 25 In an anonymous survey, 28 healthcare providers in the United States, showed that family planning issues were brought up by only 57% of physicians when starting a DMT in women of child-bearing potential. 26
In agreement with previous studies,13,16,24,27 a small percentage of WwMS in our study reported changes in the desire to have children after MS diagnosis. Besides, we found that future childbearing desire between WwMS in reproductive age was associated with younger age, milder disability, shorter disease duration and no childbearing before MS diagnosis. An Italian study, showed that about 7% of MS patients declared that they had never wanted to become parents because of MS, this being representative of a dramatic impact of diagnosis on somebody’s life project. 13 On the other hand, a previous study, found that WwMS with high disease activity were less likely to want to start a family than respondents with lower disease activity. 16
We found that almost half of WwMS in reproductive age answered that family planning is an important factor in relation to the choice of treatment. In addition, we found a trend towards injectable treatment in the WwMS group who planned their pregnancy. A recently published study, showed that therapy choice with respect to pregnancy was important or very important to the majority of WwMS with a short-term plan to conceive. For these patients, a numerically higher proportion used injectable DMTs compared with oral and infusion therapies. In addition, significantly more women with a short-term plan used injectables than those without a plan to conceive. Overall, injectable DMTs were the most commonly used therapies prior to almost half of all recorded planned pregnancies. 14 Although we did not ask patients about the knowledge of risks of DMTs in pregnancy, the Danish study showed that almost half of WwMS respondents answered that they did not know whether any DMT could affect the foetus. 16 This highlights the need for careful consideration of choice of DMT not only in women planning pregnancy, but in all fertile women.
Similar to others published studies, most of WwMS in this study had concerns regarding maternity and MS diagnosis.22,28 An observational study in Portuguese WwMS, showed that most of them reported that the number of intended pregnancies changed after MS diagnosis and the main reasons presented for having fewer pregnancies than previously were fear of future disability and the possibility of having relapses.15,16 A study using the North American Research Committee on Multiple Sclerosis (NARCOMS) database showed that WwMS’ concerns related to MS revolved around fear of inadequate parenting abilities, passing on MS to a child and possible risks associated with exposure to DMTs during pregnancy. 21
Several studies have addressed family planning in general populations in Latin America (LATAM). According to some of them, LATAM population has substantially improved access to family planning over the past years. However, modern contraceptive use and demand for family planning varied widely from country to country. Moreover, there is no single uniform policy approach amongst LATAM countries, as they are in very different situations regarding family planning, and there are still substantial disparities in healthcare access for marginalized groups. On the other hand, unplanned pregnancy rates in adolescent women continue to be a public health problem.29–32 We must consider these findings in the general population and interpret our results with caution. This study has several limitations that should be mentioned. Given that the questionnaire was not validated and a limited number of patients participated in the study, it is possible that a subset of patients with a special interest in the topic of family planning may have responded the questionnaire. Being an anonymized survey, it was not possible to compare the demographic data of the patients who answered the survey in relation to those who did not answer it. Furthermore, it is a limitation that the extent to which the sample is representative of the general MS population remains unknown. Patients with MS of different ages were included and this could affect findings, family planning advice has changed over the last years and in recent years different DMT have been approved. On the other hand, FP was only evaluated in women under 40 years of age and these results cannot be extrapolated to older women with a desire to have children. Finally, taking into account that this study is a cross-sectional study, it is not possible to establish “causality”. Factors associated with motherhood after MS diagnosis could reflect the reverse. In this sense, was having information on family planning the cause or consequence of more pregnancies after MS diagnosis? Could the patients who became pregnant have sought more information? The same analysis could be used for associations with unplanned pregnancy. Despite these limitations, the survey represents a large sample of WwMS patients and provides information about family planning. In order to examine a population that was representative of female Argentinian WwMS, this survey was distributed by 10 MS centers. On the other hand, very little information is currently available on this subject in our region, which is another strength of this study.
In conclusion, our results show similar findings to studies from North America and Europe. Considering the scarcity of data in our region, we were unable to compare our data with other LATAM countries. Research looking into reproductive health is a critical but sometimes neglected aspect of clinical research and practice of medicine in general. This study highlights the unmet needs of many WwMS regarding reproductive issues, as well as the fact that family planning is considered an important factor in relation to the choice of treatment. The high percentage of unplanned pregnancies reinforces the need not only for more comprehensive advice from neurologists specialized in MS, but also for shared decision-making processes when choosing treatment in women of reproductive age.
Conflict of Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.