
Abstract
Background
In secondary progressive multiple sclerosis (SPMS) significance of enlarged perivascular spaces (ePVS) is unknown.
Introduction
Perivascular spaces are fluid filled spaces surrounding blood vessels that run from the subarachnoid space to the brain parenchyma. These spaces are thought to enlarge due to blood-brain barrier dysfunction, perivascular inflammation and impaired waste clearance, thus reflecting pathogenically significant processes for multiple sclerosis (MS). 1
When compared to healthy subjects, MS patients have higher numbers and volumes of enlarged perivascular spaces (ePVS). In relapsing MS, increased ePVS burden correlates with advanced age and male gender. 2 The relationship between ePVS burden and T2-lesion volume, brain volumetric measures, disease duration, and disability is less clear as many of these study cohorts include both relapsing and progressive phenotypes.3–6 No prior studies have evaluated these associations in a purely secondary progressive MS (SPMS) cohort to understand ePVS in this stage of the disease.
This study describes the associations between ePVS burden and demographic variables, MS duration, disability, cognition and radiologic outcomes in people with SPMS. We also explore the relationship between ePVS burden and presence of vascular co-morbidities, as high ePVS burden has been associated with small vessel disease. 1
Methods
Subjects
Post-hoc analysis was performed on baseline clinical and radiologic data from a clinical trial of people with SPMS conducted from 2011-2015 at the Veterans Administration Portland Health Care System (Portland, Oregon). 7 Study approval was obtained by local Institutional Review Boards and patients provided written informed consent.
Imaging outcomes
A 3.0 Tesla Philips MRI obtained: 1) 3 D high resolution magnetization prepared rapid acquisition gradient echo (MPRAGE) with 1 mm3 voxels, 2) orthogonal 3 D Fluid attenuated inversion recovery (FLAIR) series with 1 mm3 voxels, and 3) conventional 3 mm (0.3 gap) axial 2 D proton density/T2-weighted sequences with in-plane resolution of 1 mm2. A single rater blind to clinical data (LW) scored ePVS in the midbrain (MB), basal ganglia (BG), and centrum semiovale (CSO) using an established method which rated MB scores from 0–1, and CSO and BG scores from 0–4. 8 Rating was performed on T2-weighted sequences with reference to other sequences, as needed. Intra-rater reliability was calculated for a subset of 10 scans. Intraclass correlation (ICC) estimates were tested separately based on a single-rater, (LW), using absolute-agreement, two-way mixed-effects models. ICC for ratings in CSO and BG was good, (ICC= 0.91 and 0.80, respectively). The MB ICC model did not converge due to near-zero variance with agreement on 9 of 10 scans. SIENAX volumetrics and cross-sectional whole-brain volumes were performed by a single neuro-radiologist as described previously. 7
Clinical outcomes
Expanded Disability Status Scale (EDSS) measured disability, and Symbol Digit Modalities Test (SDMT) measured cognition. 7 Vascular co-morbidities are noted in Table 1.
Demographic table.
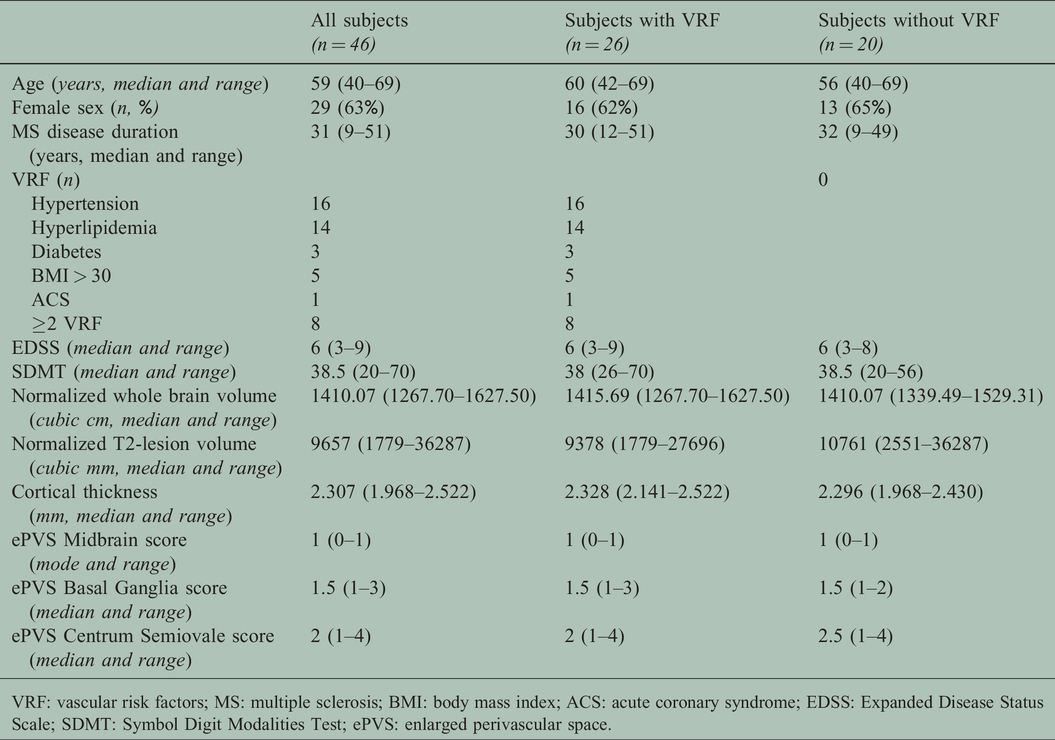
VRF: vascular risk factors; MS: multiple sclerosis; BMI: body mass index; ACS: acute coronary syndrome; EDSS: Expanded Disease Status Scale; SDMT: Symbol Digit Modalities Test; ePVS: enlarged perivascular space.
Statistical analysis
Descriptive statistics described the cohort. Kendall rank correlation coefficient (τC) for ePVS score between regions (MB v. BG: τC = −0.03; MB v. CSO: τC = 0.06; BG v. CSO: τC = 0.28) indicated that these regions could be analyzed independently. Ordinal logistic regression models examined associations between regional ePVS score and each variable, adjusted for age, gender, and T2-lesion volume (because ePVS detection was obscured with increased T2-lesion burden). Residual associations of ePVS score with age and gender were obtained using ordinal logistic regression models, adjusting for all other variables simultaneously. Analyses were performed using R v4.0.0 (R Core Team, 2020, Vienna, Austria) and Stata v15 (StataCorp. 2017, College Station, TX), particularly the package gologit2 (Williams, R. 2006).
Results
Data from 46 subjects were analyzed (Table 1). One subject was excluded from MB analysis and 3 subjects were excluded from CSO analysis because of white matter burden that obscured ePVS detection. In the BG, ePVS most scores clustered between 1 (n = 23) or 2 (n = 22). In the CSO, ePVS scores followed a normal distribution. There was no difference in T2-lesion volume in subjects with or without vascular co-morbidities (t44 = 1.38, p = 0.17).
In the MB, there were no statistically significant associations between ePVS score and any variable (Table 2). In the BG, there were statistically significant associations between decreasing EDSS and increasing ePVS score (Z = –2.04), and between advancing age and increasing ePVS score (Z = 2.68). In the CSO, there were statistically significant associations between advancing age and increasing ePVS score (Z = 2.66) and male gender (Z = 2.45). No statistically significant associations were found between MS duration, cognition, cortical thickness, whole brain volume, or the presence of vascular co-morbidities and ePVS scores in any region.
Z-scores representing the associations between each variable and ePVS score in each region.

Note: The sign of the Z-score indicates the direction of the association, with positive Z-scores indicating increased odds of higher ePVS score. A threshold of |1.96| was considered to be significant in this analysis (significant associations in bold). aAdjusted Z-scores controlled for age, gender, and T2 lesion volume.
MS: multiple sclerosis; EDSS: Expanded Disease Status Scale; SDMT: Symbol Digit Modalities Test.
Discussion
In this post-hoc analysis of people with SPMS, higher regional ePVS scores were associated with increasing age and male gender, consistent with previous studies in RRMS. 2 In our cohort, higher BG ePVS scores were associated with lower EDSS which has not been described. 9 Finally, ePVS scores were not associated with MS disease duration, cognition, whole brain volume, cortical thickness, or presence of vascular co-morbidities.
Our results suggest that ePVS may not be an informative disease marker of neurodegeneration for SPMS. Previously, Wuerfel et al. linked ePVS burden to neuro-inflammation, with increased ePVS volumes at time points with gadolinium enhancing lesions in RRMS patients. 4 Moreover, a study performed by Kilsdonk et al. with mixed MS subtypes demonstrated that ePVS count was also related to supratentorial brain atrophy and disease duration. 3 However, increased ePVS burden is also associated with non-inflammatory conditions like advancing age, possibly related to impaired fluid clearance. 1 It is possible that our study detected associations between ePVS and advancing age but not disease duration or brain atrophy because our group of SPMS subjects was older, but had less underlying neuro-inflammation than these cohorts. Additionally, these studies used different techniques and MRI field strengths to measure ePVS burden.
While our study utilized a validated technique to evaluate ePVS burden, the ordinal technique may not be sensitive enough to detect meaningful differences between groups. The narrow range of BG scores seen in this cohort was also a limitation and may have contributed to the association between low EDSS scores and higher ePVS burden in this region. Future studies including comparisons to age-matched healthy controls, using ultra-high field 7 T MRI, and incorporating more robust quantification may provide more information about ePVS in people with MS.
Conflict of Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
sj-pdf-1-mso-10.1177_2055217320964502 - Supplemental material for Enlarged perivascular spaces are not associated with vascular co-morbidities, clinical outcomes, and brain volumes in people with secondary progressive multiple sclerosis
Supplemental material, sj-pdf-1-mso-10.1177_2055217320964502 for Enlarged perivascular spaces are not associated with vascular co-morbidities, clinical outcomes, and brain volumes in people with secondary progressive multiple sclerosis by Lindsey Wooliscroft Dennis Bourdette and Rebecca Spain in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Department of Veterans Affairs (B7493-W, R. Spain), NIH (UL1TR000128). Dr. Wooliscroft is supported by K23HD101667 from the National Institutes of Health (NIH). Dr. Silbermann is supported by NMSS Sylvia Lawry Fellowship. Dr. Boespflug was supported by K01AG059842 and P30AG008017 from the NIH.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.