
Abstract
Background
Sedentary behavior is a major concern in multiple sclerosis, as it may accelerate disease progression and physical disability. This is especially concerning in African Americans, who present with greater neurological disability than Caucasians.
Objective
We conducted a feasibility trial on an intervention targeting sedentary behavior in African Americans with multiple sclerosis.
Methods
We examined the feasibility of the Sit Less, Move More program, a 12-week behavioral intervention that used text messaging along with theory-driven newsletters and behavioral coaching for managing sedentary behavior. We recruited ambulatory, inactive, African Americans with multiple sclerosis, and assessed feasibility on process, resource, management, and scientific outcomes.
Results
Of the 64 people initially contacted, 45 were assessed for eligibility, 31 were sent the informed consent document, and 30 returned a signed document and were included in the study. Study costs were US$7242.38. Personnel time to complete the study was 130 h. There was a small effect on both device-measured (d = −0.19) and self-reported (d = −0.39) sedentary behavior.
Conclusions
The Sit Less, Move More intervention is safe and feasible for African Americans with multiple sclerosis, and yielded a small reduction in sedentary behavior. The intervention was low cost and well received. Our results suggest the Sit Less, Move More program should progress towards a Phase II trial to determine its efficacy.
Introduction
Sedentary behavior, defined as any waking activity performed in a seated or lying position with an energy expenditure ≤1.5 metabolic equivalents of task, is a major public health concern.1–3 This is especially relevant for people with chronic disabling diseases such as multiple sclerosis (MS) wherein sedentary behavior is two times higher than the general population, and increased sitting time is associated with a worsening of MS disability over time. 4 The negative effects of sedentary behavior may be particularly pertinent for African Americans with MS. Whereas it is unclear if the negative consequences of sedentary behavior are different in African Americans with MS than other races, it has consistently been reported that African Americans with MS have a more rapid clinical progression that is associated with greater disability and poorer recovery from relapses.5–7 Additional evidence of this accelerated disease course is provided by magnetic resonance imaging, which has demonstrated that African Americans with MS have greater lesion volume and brain atrophy compared with Caucasians with MS. 8 This is particularly troubling considering the incidence of MS is highest among African Americans compared with any other race, including Caucasians.9,10 Nevertheless, recent reviews have identified that only 1.7% of participants in studies of exercise and physical activity in people with MS were African American, and there is no research on reducing sedentary behavior for managing MS in this population.11,12 The limited amount of research underscores the importance of feasibility trials that provide information on the process, resource, management, and scientific outcomes of interventions targeting sedentary behavior in African Americans with MS as this is critical for informing the design of future large-scale studies that may affect a large number of African Americans with MS. 13
We recently proposed the Sit Less, Move More (SLMM) program as a feasibility study for managing sedentary behavior in African Americans with MS. 14 SLMM is a 12-week, home-based program that involves text messaging, print newsletters, and telephone-based coaching, all informed by social cognitive theory (SCT), for reducing sedentary behavior in African Americans with MS. Previous behavior change interventions guided by SCT have been efficacious in promoting change in sedentary behavior and physical activity among people with MS, as this theory identifies targets of behavior change, such as self-efficacy and goal setting, for designing the content of an intervention.15–18 These previously studied behavior change interventions19–23 served as the base of the SLMM program, but the various components of the intervention were tailored specifically to African Americans with MS based on stakeholder feedback from a focus group consisting of African Americans from a local MS support group. The current paper reports the results of the feasibility of SLMM based on recommendations and guidelines for feasibility trials, and includes process, resource, management, and scientific outcomes of the SLMM program.
Methods
The SLMM intervention protocol has been detailed in a recent publication. 14 The study used a single-group, pre-post intervention design to examine feasibility and initial efficacy of a 12-week, behavior change intervention for reducing sedentary behavior in African Americans with MS. The study was approved by the University Institutional Review Board and was registered on clinicaltrials.gov (NCT03671499).
Participants and recruitment
Study inclusion criteria were: (a) African American; (b) 18–64 years of age; (c) self-reported MS diagnosis; (d) relapse-free in the last 30 days; (e) ambulatory with or without assistance based on a Patient-Determined Disease Steps (PDDS) score of 0–5; (f) self-reported daily engagement in sedentary behavior ≥480 minutes per day; (g) health contribution score (HCS) of <14 calculated from the Godin Leisure-Time Exercise Questionnaire; 24 (h) absence of major musculoskeletal problems and/or cardiovascular, cardiopulmonary, and/or metabolic diseases that are contraindications for changing physical activity and sedentary behavior levels (e.g. uncontrolled cardiac arrhythmias, asthma, or diabetes; musculoskeletal or rheumatoid disorders exacerbated by exercise); (i) living in the United States; and (j) ownership of a mobile phone capable of receiving text messages. We first recruited participants who met the inclusion criteria for race and age from those who had previously taken part in research studies in our laboratory. Participants were further recruited from local MS events sponsored by the National MS Society and through a mass email distributed via the iConquerMS network. Those who were interested in participating contacted laboratory personnel for more information about the study and determine eligibility. As the main purpose of the study was to assess the feasibility of the SLMM program, we did not perform a power analysis for calculating sample size, and instead based our sample size of 30 participants on previous feasibility studies in people with MS.21,25
Procedure
Figure 1 provides a timeline of the study and an overview of the intervention components. Eligible participants received the informed consent document and baseline assessment packet (questionnaires and accelerometers) via the United States Postal Service (USPS) and returned the completed materials in a pre-stamped, pre-addressed envelope. After receipt of the signed informed consent document and baseline assessment materials (T1), participants completed a 12-week intervention. There was a midpoint assessment (T2) that included the same testing materials as the baseline assessment mailed to each participant halfway through the intervention (i.e. during week 6). After the intervention (i.e. immediately after week 12), a post-intervention assessment (T3) was mailed to each participant. The post-intervention assessment included the same materials as the previous assessments (T1 and T2), but also included an additional survey to assess participant satisfaction of the SLMM program. The survey consisted of Likert scale questions (scored 1, “strongly disagree” to 5, “strongly agree”) and open-ended questions asking participants which aspects of the program they liked the most and which they liked the least. Participants received $25 remuneration for completing each of the three outcome assessments.
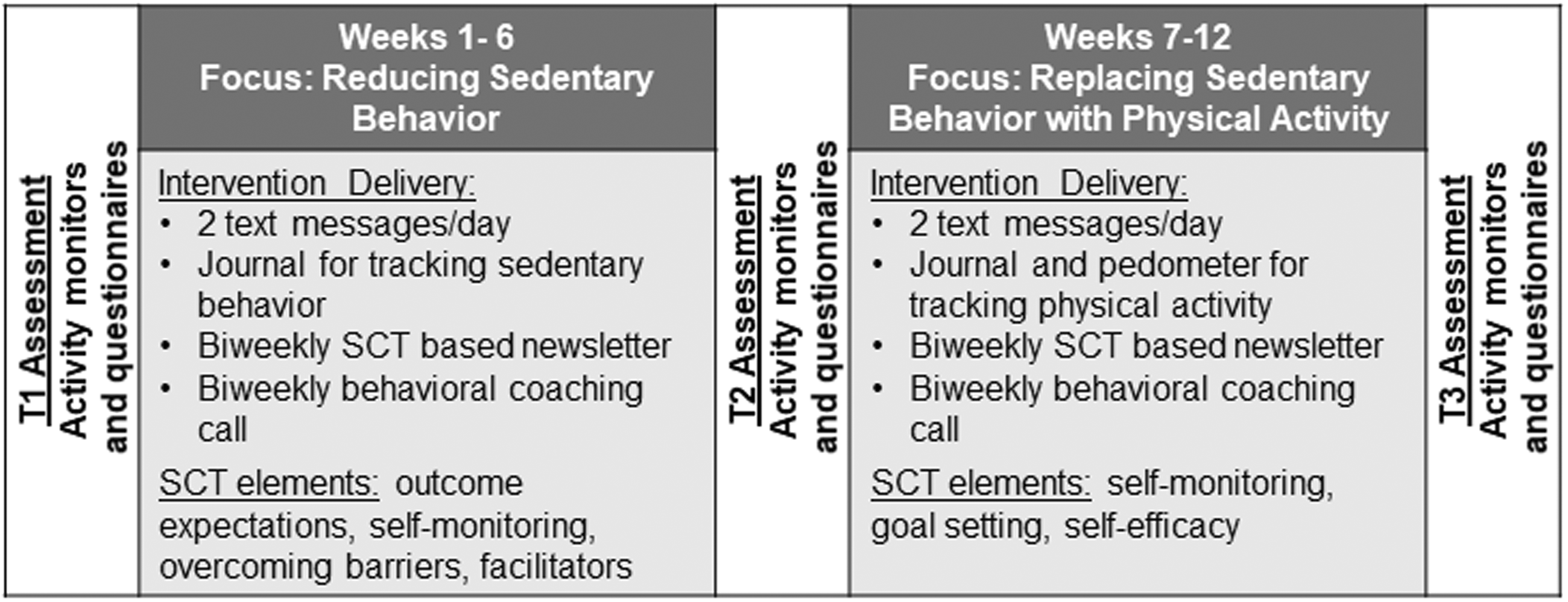
Overview of the intervention components and timeline.
Behavioral intervention
The behavioral intervention was 12 weeks in duration and consisted of two 6-week phases. Phase 1 (weeks 1–6) focused on reducing sedentary behavior (Sit Less), and Phase 2 (weeks 7–12) focused on replacing sedentary behavior with light physical activity (LPA; Move More). The intervention involved two daily text messages, and biweekly newsletters and telephone calls with a behavioral coach (JFB). The behavioral coach was involved in the design of the behavioral intervention and selection of materials, and further received initial and ongoing training in the delivery of behavior change materials within the behavior coaching sessions. The content of the text messages, newsletters, and coaching calls were based on an SCT framework for guiding changes in health behavior and were culturally tailored based on feedback from a focus group of African Americans with MS within a local support group. The SCT framework identifies self-efficacy, outcome expectations, overcoming barriers, and goal setting as determinants of behavior change, and therefore strategies targeting these determinants of behavior change were incorporated into the content of the intervention materials. Participants were provided a journal to record daily sedentary behavior (during weeks 1–6) and physical activity (during weeks 7–12), and a pedometer for tracking daily step counts.
Feasibility metrics
Data were collected to assess feasibility on four domains: process, resource, management, and scientific outcomes. 13 Process feasibility measures included participant recruitment and eligibility rate. Resource feasibility was assessed by examining participant adherence (i.e. participation in the coaching calls) and retention rates. Additionally, time spent communicating with participants and the monetary costs of the study were considered as part of resource feasibility. Management feasibility was assessed based on time spent for material preparation and data entry, as well as missing data items. Measures of scientific feasibility included safety (e.g. adverse events), participant experience and burden, and the treatment effect on the behavioral outcomes.
Scientific outcomes
Participant demographic and clinical characteristics were collected during the baseline (T1) assessment. The primary scientific outcome of interest was a change in sedentary behavior. Secondary outcomes of interest included a change in physical activity and health-related quality of life.
Sedentary behavior and physical activity were assessed using accelerometry. At all assessment time points (T1, T2, and T3) participants wore an activPAL activity monitor (PAL Technologies) and an ActiGraph model GT3X+ activity monitor (ActiGraph LLC) for a 7-day period, removing the monitors for sleeping or during water-based activities. Data from the activPAL were classified as time spent sitting or lying down, standing, or during movement using a proprietary algorithm. The ActiGraph data were processed as 60-second epochs and classified as sedentary behavior, LPA, or moderate-to-vigorous physical activity (MVPA) based on established cut points in people with MS. 26 A minimum of 600 min of wear time was required to be considered a valid day of data for inclusion in the analysis for both accelerometer devices.
Sedentary behavior and physical activity were further measured subjectively with the Godin Leisure-Time Exercise Questionnaire (GLTEQ)27,28 and the short form of the International Physical Activity Questionnaire (IPAQ).29,30 Total leisure time physical activity was calculated from the GLTEQ by multiplying the recorded number of 15-min bouts of mild, moderate, and strenuous physical activity by weights of 3, 5, and 9, respectively, then summing the weighted values for a score that ranges from 0–119. The HCS representing health promoting physical activity was calculated by summing the weighted values for moderate and strenuous physical activity only, for a score that ranges from 0–98. Scores for walking, moderate, and vigorous activities were calculated from the IPAQ by multiplying the frequency scores of each activity type by 3.3, 4, and 8 metabolic equivalents, respectively. Scores were summed to form a measure of total physical activity ranging from 0–107. The duration component of the IPAQ was not included based on previous research that identified problems with accurate recall of activity duration in people with MS. 31 The IPAQ sitting question asks participants to report how much time (min) was spent sitting on average on a weekday.
Health-related quality of life was assessed with the 36-item Short Form Health Survey (SF36). 32 The SF36 provides a measure of quality of life in eight domains: physical functioning (limitations in physical functioning due to health problems), role-physical (limitations in usual activities because of physical health problems), role-emotional (limitations in usual activities due to emotional problems), vitality (energy and fatigue), emotional wellbeing (psychological distress and wellbeing), social functioning (limitations in social functioning due to physical or emotional problems), pain, and general health. Combining scales from the SF36 provides two summary scores: a physical component and a mental component. On all scales, a higher score indicates a higher quality of life.
Data analysis
Data were analyzed in SPSS Statistics, Version 25 (IBM Corporation, Armonk, NY). Descriptive statistics are reported for clinical and demographic characteristics and all behavioral outcomes. Feasibility metrics for process, resource, and management are reported descriptively as frequencies and percentages. Estimates of effect size (Cohen’s d) were calculated to describe the treatment effect of the SLMM intervention on all behavioral outcome measures. The effect sizes were interpreted as small, moderate, or large based on values of 0.2, 0.5, and 0.8, respectively. 33
Results
Participants
Participant demographic characteristics are presented in Table 1. Participants were mainly female (86.7%) and had relapsing-remitting MS (93.3%). The mean age was 44.3 years (±9.4 years) and the mean disease duration was 10.7 years (±7.3 years). Participants had a median PDDS score of 3.0 (range 0–5, interquartile range 2.0) indicative of moderate ambulatory disability.
Participant demographic information (n=30).

IQR: interquartile rating; MS: multiple sclerosis; PDDS: Patient Determined Disease Steps scale; PPMS: primary progressive multiple sclerosis; RRMS: relapsing remitting multiple sclerosis.
Process feasibility
Recruitment. The CONSORT diagram presented in Figure 2 details the participant flow through the study. There were 64 people with MS who were contacted to participate in the study. Of those individuals initially contacted, 45 (70%) were assessed for eligibility. Those not assessed for eligibility were either not interested in participating (n = 4, 6%), or we were unable to contact them for screening (n = 15, 23%). Of the 45 potential participants assessed for study eligibility, 14 (22%) were excluded during telephone screening based on not meeting inclusion criteria; nine were too active, four reported a PDDS score >5, and one did not self-identify as African American. In total, 31 (69%) of the interested participants were eligible to participate and were sent T1 baseline materials including a consent document. One person who qualified did not return a signed consent form and therefore was not included in the study. Overall, 30 participants signed and returned the consent document and baseline materials and were included in the study, yielding a final sample of 30.

CONSORT diagram outlining participant flow from recruitment through data analysis.
Resource feasibility
Retention, adherence, and attrition. Of the 30 participants who were enrolled in the study, 30 (100%) returned the midpoint (T2) testing materials, and 29 (97%) returned the post-intervention (T3) testing materials. Adherence was assessed based on participation in the biweekly telephone coaching calls. In total, 25 (83%) participated in all seven coaching calls, four (13%) participated in six of the seven calls, and one (3%) participated in five of the seven calls. Regarding attrition, one participant did not return the post-intervention packet and therefore did not fully complete the study. This participant completed all seven coaching calls and never expressed an interest in dropping out of the study. We were unable to contact this participant and ascertain why the post-intervention packet was not returned. This participant’s data are included in our analysis of intervention outcomes from T1 to T2 and our analysis of missing data, but not in our analyses of intervention outcomes from T2 to T3 and T1 to T3.
Communication. The initial recruitment phone call that included screening for eligibility lasted 15 min (±3 min, range 8–22 min). The mean turnaround time for assessment packets to leave our laboratory, be completed by participants, and received by our laboratory was 27 days (±16 days, range 12–58 days) for T1, 22 days (±8 days, range 13–42 days) for T2, and 26 days (±10 days, range 13–54 days) for T3.
Monetary requirements. Total costs to conduct the study were US$7242.38 or US$241.41 per person. This included costs for materials (i.e. paper and envelopes; US$842.21), postage (US$1111.76), equipment (pedometers; US$705.49), participant remuneration (US$2250), and indirect costs (US$2332.92). The total does not include personnel costs as these would vary based on the specific circumstances of each institution. However, by providing an indication of the personnel time required for such a study (below), the cost for personnel can be estimated accordingly. Costs for reusable study materials such as the ActiGraph (US$250 per unit) or activPAL (US$290 per unit) activity monitors were not included in the total costs as laboratories may already have these items available for use, but the cost per unit is provided and total costs can be estimated accordingly.
Management feasibility
Personnel time requirement. Total personnel time to complete the study was 129.5 h and included time spent on recruitment and screening telephone calls (8 h), behavioral coaching calls (34.5 h; mean duration = 10 min ±3 min, range 4–22 min), preparing and delivering text messages (15 h), material preparation and mailing (49 h), and data entry (23 h).
Missing data. Missing data are detailed in Table 2. At baseline (T1), 10 participants (33%) had no valid days (wear time <600 min) for the activPAL device and one participant (3%) had no valid days for the ActiGraph device. Questionnaire packets were completed and returned by all participants (100%) during baseline; however, seven participants (23%) answered “Don’t know/Not sure” for time spent sitting on the IPAQ. At the midpoint assessment (T2), six participants (20%) had no valid days for the activPAL device and three participants (10%) had no valid days for the ActiGraph device. Questionnaire packets were completed and returned by all participants (100%) during the midpoint assessment; however, six participants (20%) answered “Don’t know/Not sure” for time spent sitting on the IPAQ and 1 participant (3%) did not answer all questions on the IPAQ. At the post-intervention assessment (T3), eight participants (27%) had no valid days for the activPAL device and four participants (13%) had no valid days for the ActiGraph device. Questionnaire packets were completed and returned by 26 participants (87%). Of the 26 returned questionnaire packets, 10 participants (33%) answered “Don’t know/Not sure” for time spent sitting on the IPAQ and one participant (3%) did not answer all questions on the IPAQ.
Number of valid data items.
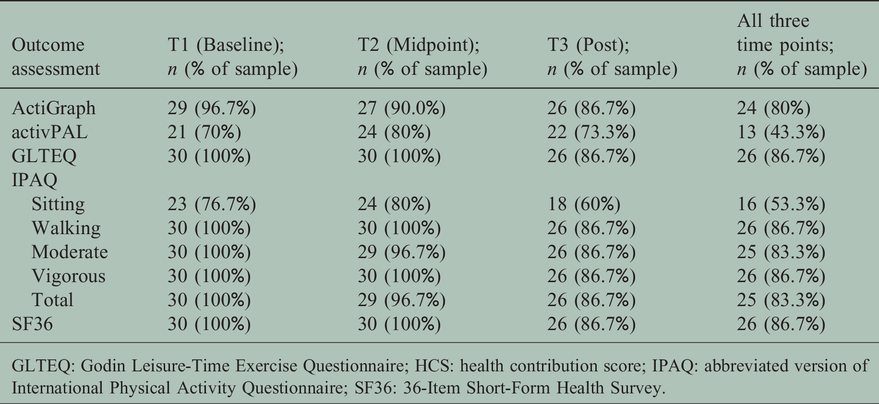
GLTEQ: Godin Leisure-Time Exercise Questionnaire; HCS: health contribution score; IPAQ: abbreviated version of International Physical Activity Questionnaire; SF36: 36-Item Short-Form Health Survey.
Overall, for the activPAL device, only 13 participants (43%) had at least 1 valid day at all three assessment time points, 12 participants (40%) had at least 1 valid day at two assessment time points, four participants (13%) had at least 1 valid day at one assessment time point, and one participant (3%) had no valid days across all time points. For the ActiGraph device, 24 participants (80%) had at least 1 valid day at all three assessment time points, four participants (13%) had at least 1 valid day at two assessment time points, and two participants (7%) had at least 1 valid day at one assessment time point. For both the activPAL and AcitGraph devices, participants were more likely to have a valid day during the week (average number of participants obtaining a valid day during the week: activPAL = 15; ActiGraph = 20) than the weekend (average number of participants obtaining a valid day during the weekend: activPAL = 9; ActiGraph = 13). All participants that returned a questionnaire packet during the post-intervention assessment (n = 26, 87%) also completed the feedback survey.
Scientific outcomes
Safety. There were no instances of health problems or adverse events reported during the intervention period.
Participant experience and burden. In total, 26 participants completed the feedback questionnaire. Overall, participants were satisfied with all aspects of the intervention (Figure 3(a)) and rated all aspects of the intervention as useful and suitable for reducing sedentary behavior (Figure 3(b)). Participants rated the amount of texts, newsletters, and coaching calls as appropriate (Figure 3(c)). Participants strongly agreed that the intervention would be effective in a large group of people and would recommend the program to others (Figure 3(d)). Examples of comments provided in response to the open-ended questions on the feedback survey are presented in Table 3.
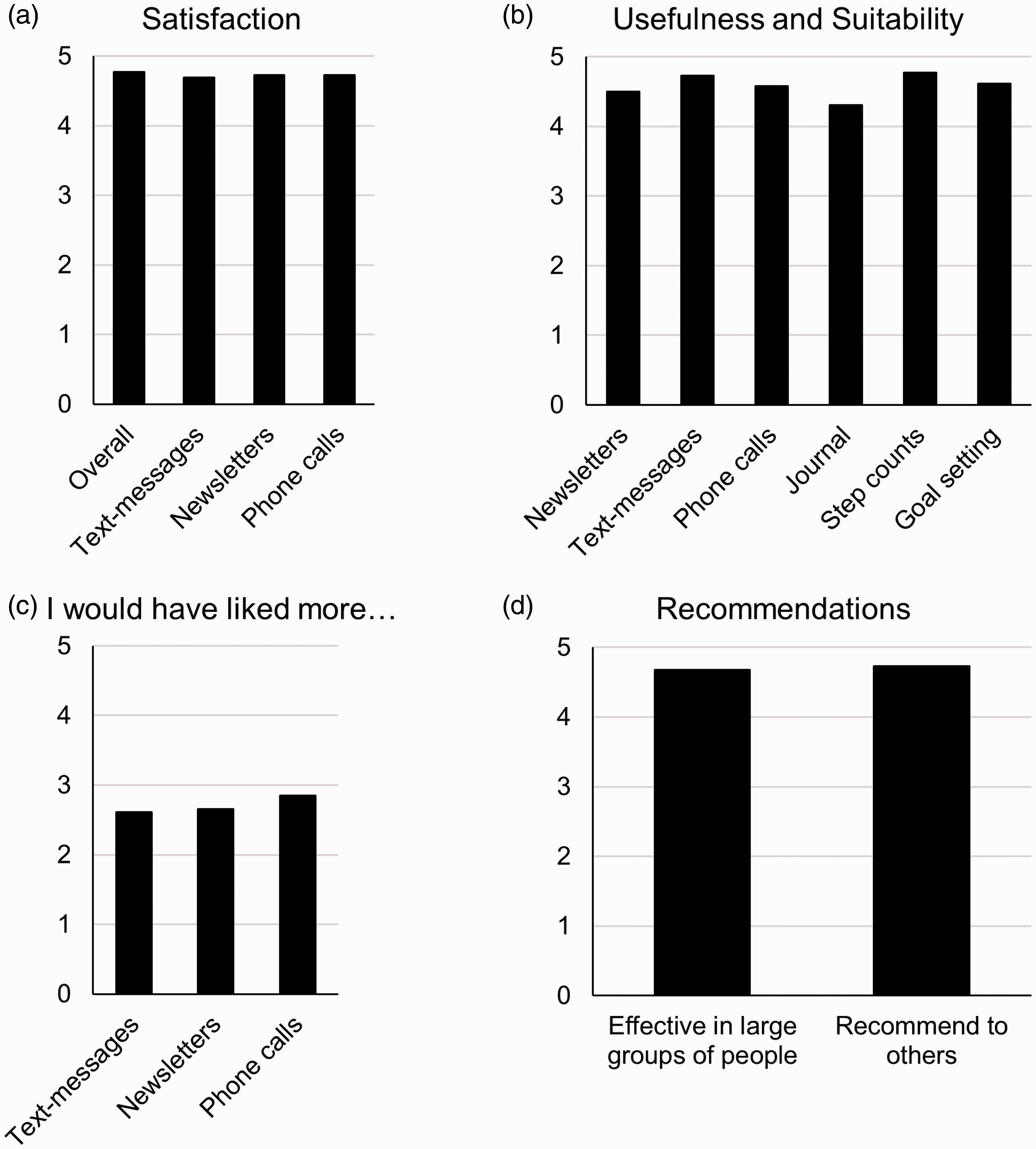
Participant feedback on the satisfaction and usefulness of different intervention components. A score of 0 indicates low agreement/satisfaction and a score of 5 indicates high agreement/satisfaction.
Examples of written feedback following completion of the intervention.

MS: multiple sclerosis.
Treatment effect. Effect sizes for differences in all outcome variables are presented in Table 4. There was a small reduction in device-measured sedentary time (ActiGraph: d = −0.19; activPAL: d = −0.13) from T1 to T3. There was a moderate reduction in self-reported sedentary time (d = −0.39) from T1 to T3. Device measured LPA did not change from T1 to T3; however, there was a small effect on MVPA measured by the ActiGraph accelerometer (d = 0.22). Based on the GLTEQ, there was a moderate increase of total physical activity (d = 0.51) and MVPA (d = 0.42); yet, based on the IPAQ, there was no change in self-reported physical activity (d = −0.05). There was a small to moderate effect on health-related quality of life across all domains. The effect was greater on the mental component score (d = 0.48) than the physical component score (d = 0.21) and was greatest for the social functioning subscale (d = 0.67).
Outcomes at T1 (baseline), T2 (midpoint), and T3 (post-intervention).

Data presented as mean (SD). LPA: light physical activity; MVPA: moderate to vigorous physical activity; GLTEQ: Godin Leisure-Time Exercise Questionnaire; HCS: health contribution score; IPAQ: abbreviated version of International Physical Activity Questionnaire; SF36: 36-Item Short-Form Health Survey; Phys: physical component score; Mental: mental component score; PhysFunc: physical function subscale; RLphys: role limitations due to physical health problems subscale; Rlemot: role limitations due to emotional problems subscale; Vitality: vitality subscale; EmoWb: emotional wellbeing subscale; SocFunc: social functioning subscale; Pain: bodily pain subscale; GenHealth: general health perceptions subscale.
Discussion
This study determined the feasibility of the SLMM program, a 12-week home-based program that used text messaging, newsletters, and behavioral coaching based on SCT for reducing sedentary behavior in African Americans with MS. Feasibility was assessed on four domains: process, resource, management, and scientific outcomes. 13 Such feasibility trials are important for informing future, large-scale interventions and serve to strengthen the scientific foundation of exercise-related research in MS.
Process feasibility assessed the key processes associated with recruitment that are integral to the success of the study. 13 Our approach to recruitment that included contacting prospective participants via our laboratory database, word of mouth at local MS events, and a mass email distributed by iConquerMS yielded a higher overall recruitment rate (70%) than previous studies.21,34 This supports using a similar strategy as appropriate for a larger-scale study. Our eligibility rate (69%) assessed the number of interested individuals that qualified for the study indicates our inclusion criteria were appropriate for the target population and would be suitable for future studies. 21
Resource feasibility assessed time and monetary resources associated with participant retention and compliance with the study. 13 Our high retention rate (97%) demonstrates overall acceptability and tolerability of the SLMM program. Most participants (83%) completed all behavioral coaching sessions. Issues with scheduling were the most common reason for not completing a call. On average, it took 25 days for participants to receive, complete, and return testing materials, and this turnaround time needs to be accounted for when developing nationwide, home-based studies. We further provide an estimate of the cost of the research as this is important for informing future funding proposals and large-scale studies.
Management feasibility assesses problems with data management and includes personnel time required for data preparation and entry as well as an analysis of missing data. 13 There was a larger percentage of missing data for the activPAL accelerometer than for the ActiGraph accelerometer. Participants reported that the Tegaderm used to secure the activPAL device on the thigh was uncomfortable. Additionally, the activPAL device was visible when wearing certain types of clothing (e.g. shorts), and participants reported not wearing the device when it could not be adequately covered. It should also be noted that the data-collection period for the activPAL device is limited to a 2-week window, whereas the ActiGraph will continue to collect data as long as the battery lasts (∼30 days). At times, the data collection period of the activPAL device would end before participants had completed all 7 days of wear. In terms of self-report outcomes, the high percentage of missing data for the sitting question on the IPAQ is of concern. Many participants chose “I don’t know/Not sure” in response to this question instead of estimating the time spent sitting.
Scientific feasibility assesses the safety of the intervention, participant burden and acceptability, and the effect of the intervention on measured outcomes. 13 No adverse events or health problems were reported by participants, indicating the safety of the SLMM program in people with MS. Overall, feedback from the survey indicated a high level of satisfaction and acceptability of the SLMM program (Figure 3). Feedback from the open-ended questions on the survey (Table 3) indicated the most burdensome aspects of the study were issues with assessment materials (e.g. discomfort of the Tegaderm, amount of paperwork), and not the intervention itself.
There was a small treatment effect on our primary scientific outcome of sedentary behavior. This was indicated by a reduction in self-reported sitting time on the IPAQ and device-measured sedentary behavior. These results are consistent with those from a recent study that demonstrated the validity of the sitting item from the IPAQ in people with MS. 35 Our secondary outcomes examined change in physical activity. There was a moderate treatment effect on physical activity, indicated by an increase in exercise participation measured via the GLTEQ. These results are incongruous with results from the IPAQ whereby participants reported a small decrease in physical activity. It was recently reported that there is little agreement between the IPAQ and device measured physical activity, 36 suggesting other self-report measures such as the GLTEQ that have been validated in people with MS27,37 may be more appropriate for subjectively measuring physical activity. Additional secondary outcomes included a treatment effect on health-related quality of life. There were small to moderate effects across all domains measured by the SF36. The effect was greater on the mental component score than the physical component score, which was supported by moderate effects on the role limitations due to emotional problems, emotional wellbeing, and social functioning subscales.
The results from this study are of major importance as African Americans with MS have been a group that has not received proper attention in intervention studies aiming at behavior change. 11 In African Americans with MS, reducing sedentary behavior might represent an essential approach for slowing the development of neurological disabilities and comorbidities. This is especially important as African Americans with MS experience an accelerated, more disabling disease course compared to Caucasians with MS.6,38 Yet, despite a recent increase in the incidence of MS in African Americans, a limited number of studies have examined the feasibility of reducing such behavior in this population. The strategy adopted in the current study is of relevance from an epidemiological perspective as it may allow for reaching a large number of individuals in a cost-effective manner.
Suggestions for future research
Our feasibility study provides several lessons for informing future trials for yielding a larger change in sedentary behavior. Based on participant burden and the high level of missing data, researchers should consider eliminating the activPAL device and only use the ActiGraph as a method of device measured sedentary behavior. Additionally, the lack of agreement between the IPAQ and device-measured physical activity raises concerns on the validity of the questionnaire for measuring physical activity in people with MS. The usefulness of the IPAQ is further a concern based on the high percentage of participants that responded “I don’t know/Not sure” in response to the sitting time question on the IPAQ. Future studies should consider a different subjective measure of sitting time that does not include a “no response” option. Short questionnaires that inquire about a range of sedentary behaviors rather than a single question that asks the participant to recall all sedentary time may be a more appropriate and accurate estimate of sedentary behavior. 39 Additionally, future studies should consider providing the questionnaires in both a paper and online format, enabling the participant to choose their preferred method, thereby reducing participant burden.
Regarding the intervention, problems or concerns that should be addressed prior to implementation in large-scale studies include: (a) developing a more efficient approach for maintaining a consistent coaching schedule; (b) developing a minimum standard of training for behavioral coaches for consistent, broad-scale delivery of the intervention; (c) providing a shared space or forum for participants to interact and support one another; and (d) supplying the pedometer earlier in the program and providing a more sophisticated, interactive platform to monitor and track steps. After integrating the proposed adaptations, future research should consider utilizing the SLMM intervention in more specific populations, such as African Americans with MS with more severe disability, to more comprehensively determine the efficacy of the program.
Conclusion
The SLMM intervention is safe and feasible for people with MS and yielded a small positive change in sedentary behavior. The intervention was low cost and well received as an approach for reducing sedentary behavior. Overall, our results suggest that the SLMM program progress towards a Phase II trial to determine its efficacy for reducing sedentary behavior in African Americans with MS. 40
Footnotes
Conflict of Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a pilot grant from the Consortium of Multiple Sclerosis Centers. Jessica F. Baird was supported by a National Institutes of Health training grant (2T32HD071866-06). Jeffer E. Sasaki was supported by a mentor-based fellowship from NMSS (MB0011).