
Abstract
Background
Pediatric-onset multiple sclerosis (POMS) is considered a complex disease entity with many genetic and environmental factors implicated in its pathogenesis. Linkage studies in Caucasian adult populations consistently demonstrate the major histocompatibility complex and its HLA (human leukocyte antigen) polymorphisms as the genetic locus most strongly linked to MS.
Objective
To investigate the frequencies and possible clinical and imaging correlations of HLA-DRB1 alleles in a Hellenic POMS sample.
Methods
Fifty POMS patients fulfilling the IPMSSG (International Pediatric Multiple Sclerosis Study Group) criteria were enrolled using 144 adult-onset MS (AOMS) patients and 246 healthy controls for comparisons. HLA genotyping was performed with standard low-resolution sequence-specific oligonucleotide (SSO) techniques. Clinical and imaging correlations with specific HLA-DRB1 alleles were also examined.
Results
The HLA-DRB1*03 genotype was significantly higher in POMS patients compared to both the AOMS population (26% vs. 12.5%, p = 0.042) and the general population (26% vs. 12.6%, p = 0.004). HLA-DRB1*03-positive POMS patients had significantly more relapses (6.9 ± 4.9 vs. 4.2 ± 4.4, p = 0.005) and more thoracic spinal cord lesions than HLA-DRB1*03-negative patients (61.5% vs. 27%, p = 0.043).
Conclusion
In our Hellenic population, HLA-DRB1*03 allele confers increased risk for POMS and it is also correlated with possibly increased disease activity, expanding the existing knowledge on HLA associations and POMS.
Keywords
Introduction
Early-onset (pediatric and adolescent) multiple sclerosis (MS) accounts for approximately 3–5% of all MS cases, with the term pediatric-onset MS (POMS) being used largely interchangeably in the international literature for both age groups. 1 In parallel with adult-onset MS (AOMS), 2 POMS is considered a complex multi-factorial disease entity with many genetic, epigenetic, and environmental factors implicated in its pathogenesis.
Since the 1970s, it has been well established that the major histocompatibility complex (MHC) and its polymorphisms have a strong genetic effect on the risk of AOMS. 3 Carrying the HLA-DRB1*15:01 allele is associated with a threefold greater risk of developing MS, while HLA-A*02:01 confers protection against the disease. 4 A series of studies have confirmed the predisposing role of also HLA-DRB1*15 in POMS, although its effect is lower than that for AOMS, suggesting a fundamental genetic similarity between different age groups.5–7 However, whether the HLA-DRB1*15:01 allele is associated with lower age at MS onset by itself still remains controversial, 8 with one study indicating significance of epistatic interactions at the HLA-DRB1 locus, specifically between the HLA-DRB1*04:01 and HLA- DRB1*15:01 alleles. 9 In 2014, a putative predisposing role of HLA-DRB1*03 in POMS was proposed in the Hellenic population. 5 This allele has been correlated with a presumably better MS prognosis in Caucasian populations, but also with neuromyelitis optica (NMO), a mainly humoral demyelinating disease entity,3,5 A protective role of the HLA-DRB1*16 allele also emerged, expanding our knowledge in the field. 5
Previous studies in AOMS correlated HLA genotype with a series of clinical and paraclinical characteristics. Besides age of disease onset, proposed correlations suggested sex predominance,10,11 specific phenotype and disease course,12–14 as well as magnetic resonance imaging (MRI) findings and response to treatment.15,16 Similar studies are largely missing in POMS,17–19 creating space for further research toward a more personalized prognosis and therapeutic decision-making.
This study investigated the influence of HLA-DRB1 alleles on disease risk and/or protection in a Hellenic sample of 50 POMS patients, using 144 AOMS patients and 246 healthy controls (HCs) for comparisons. Clinical and imaging correlations with specific HLA genotypes were also examined in the Hellenic population for the first time.
Materials and methods
Patients
The First Department of Neurology of National and Kapodistrian University of Athens (NKUA) is the reference center for a wide spectrum of neurological disorders, including MS and other demyelinating diseases. MS patients are admitted in our Demyelinating Diseases Unit and are frequently followed up in the outpatient clinic. POMS patients were enrolled in our inpatient/outpatient Demyelinating Diseases Unit, as well as in other pediatric neurology reference centers. Fifty POMS patients (32 females, 18 males, mean age 26.7 ±10.4 years old) fulfilling the IPMSSG (International Pediatric Multiple Sclerosis Study Group) criteria for POMS diagnosis were selected. 20 All patients and legal guardians provided written informed consent. The study received ethical approval by the Hospital Ethics Committees, consistent with the Declaration of Helsinki.
At this time, no patients were identified with primary progressive MS (PPMS), while 11 (22%) patients had the secondary progressive type (SPMS). The mean age of disease onset was 15.3 ± 2.8 years old; the mean disease duration was 138.6 ± 114.1 months and the median Expanded Disability Status Scale (EDSS) was 2.8 ± 1.5. 21 We used two different control groups of Hellenic origin; an AOMS group with 144 AOMS patients from our center and a general population group of 246 HCs who were genotyped in the past, from centers all over the country, in the biggest genotyping research study in the Hellenic population, contacted by the reference Immunogenetics and Histocompatibility Center in Greece. 22 AOMS patients fulfilled the McDonald criteria of 2010. 23 Valid MRI results of the brain, cervical and spinal cord were available for all patients, while cerebrospinal fluid (CSF) (i.e. presence of oligoclonal bands, OCBs) assessments were available in 36 (72%) of the patients, with 31 (86.1%) being positive for OCBs. With regards to the presence of OCBs in the CSF, only some patients had been subjected to CSF analysis, as this was not a prerequisite for the MS diagnosis according to the revised 2010 McDonald criteria for AOMS and the IPMSSG 2013 criteria for POMS (Table 1). The time point of HLA sampling was the time point of all disease characteristics and MRI performance. None of our patients was on relapse.
Clinical characteristics in POMS and AOMS.

MS = multiple sclerosis, POMS = pediatric-onset MS, AOMS = adult-onset MS, EDSS = Expanded Disability Status Scale, CIS = clinically isolated syndrome, CDMS = clinically definite MS.*p ≤ 0.05.
HLA-DRB1 genotyping
HLA genotyping was performed at the Immunogenetics Laboratory of the First Department of Neurology at Aeginition Hospital. High molecular weight DNA was extracted from peripheral blood samples (8 mL peripheral blood in sodium citrate, ACD Vacutainer® tube) using the DNA extraction, Maxi Kit (QIAGEN, Germany) as per manufacturer’s guidelines. HLA class II (HLA-DRB1) frequencies were determined by molecular techniques for all the specificities included in the HLA nomenclature of 2012 (we present only the first two digits of each allele, for low resolution respectively). 24 The HLA-DRB1 genotyping was performed using a PCR-SSO (polymerase chain reaction, sequence-specific oligonucleotide) technique, based on a method that depends on reverse hybridization (HLA-DRB1 Plus, INNO-LiPA, low resolution, Innogenetics, Fujirebio, Europe) according to the manufacturer’s protocol. Quality control has been secured. First, our HCs are already genotyped individuals from the large histocompatibility study of Papassavas et al. in 2000. 22 Second, we have used external controls for our laboratory; thus we have typed random MS samples in different HLA-genotyping laboratories in Athens and found no discrepancies in our results. Finally, our laboratory has participated in EFI (European Federation of Immunogenetics) quality control in 2001.
Statistical analyses
Univariate comparisons were made using Mann–Whitney U and chi-square tests (with Yates correction for 2 × 2 tables) for interval and categorical variables, respectively. The Hardy–Weinberg proportions (HWPs) for HLA-DRB1 haplotypes were ascertained by using PyPoP software. Ewens–Watterson (EW) homozygosity test for neutrality was also performed. Calculation of the normalized deviate of the homozygosity (i.e. Fnd) was done, with positive and negative values implying directional and balancing selection, respectively. HLA-DRB1 genotypic frequency in the subgroups of MS patients was compared with that reported in a previous study of Hellenic HCs using chi-square tests. 22 Significance was set at 0.05. In HLA-DRB1 genotype -related tests (except those for clinical parameters), p value correction was made according to the Benjamini–Yekutieli method (or B-Y) based on the following formula: p(B-Y) = a/(Σ1/i), where i denotes the number of comparisons and a = 0.05. 25 Statistical analyses were performed using SPSS 22 (SPSS Inc, Chicago, IL, USA).
Results
Non-genetic comparisons between POMS and AOMS
POMS patients had a significantly younger age, which primarily reflected the time of blood sampling. Compared to AOMS, POMS patients also presented with significantly lower EDSS (POMS 2.8 ± 1.5, AOMS 3.4 ± 1.7, p = 0.011) and clinically isolated syndrome onset (POMS 33/50 (66%), AOMS 60/144 (41.7%), p = 0.005). We did not find any POMS patients with PPMS (Table 1).
HLA genotypic comparisons between POMS/AOMS and POMS/general population
Twelve distinct HLA-DRB1 alleles were identified (total alleles: 388) in all MS patients. There were 23 homozygotes and 179 heterozygotes. The most common genotypes were HLA-DRB1*15/DRB1*11 (6.2%) and HLA-DRB1*16/DRB1*11 (6.2%). There were no deviations from the HWP (F(8) = 8.74, p = 0.364). The EW homozygosity test of neutrality was significantly negative (i.e. Fnd = −1.509, p = 0.0013), denoting a balanced selection. In summary, the most common HLA genotypes in POMS were HLA-DRB1*11 (38%), and HLA-DRB1*15 (28%), followed by HLA-DRB1*03 (26%), HLA-DRB1*04 (26%), and HLA-DRB1*16 (26%).
As shown in Table 2, the frequency of the HLA-DRB1*03-positive MS patients was significantly higher in the POMS than the AOMS population (26% vs. 12.5%, p = 0.042), but not reaching statistical significance after B-Y correction (i.e. p ≤ 0.017). The presence of the HLA-DRB1*03 genotype was also significantly higher in POMS than in the general population (26% vs. 12.6%, p = 0.004; Table 3), while HLA-DRB1*11 was significantly lower in these patients (38% vs. 52%, p = 0.033), suggesting a protective trend.
HLA genotypic comparisons between POMS and AOMS.
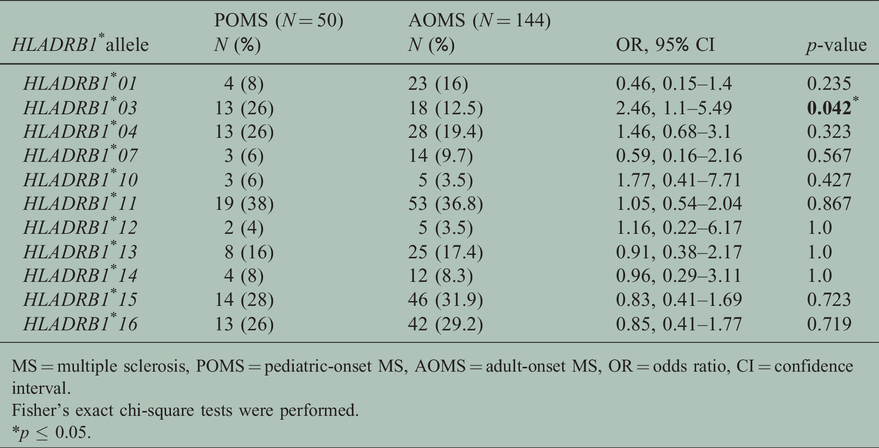
MS = multiple sclerosis, POMS = pediatric-onset MS, AOMS = adult-onset MS, OR = odds ratio, CI = confidence interval.
Fisher’s exact chi-square tests were performed.
*p ≤ 0.05.
HLA genotypic comparisons between POMS and general population.

MS = multiple sclerosis, POMS = pediatric-onset MS, AOMS = adult-onset MS, OR = odds ratio, CI = confidence interval.
Fisher’s exact chi-square tests were performed.
*p ≤ 0.05.
¥p ≤ 0.017 according to the B-Y correction method.
A total of 14 out of 50 POMS patients (28%) were positive for HLA-DRB1*15 genotype, which is significantly higher than the 16.7% genotype frequency in the general population (p = 0.025), confirming the well-established role of this allele in MS pathogenesis. HLA- DRB1*15 genotype positivity was 31.9% (46/144) in AOMS similar to that of POMS patients (p = 0.723).
Clinical comparisons among most frequent HLA genotypes in POMS
POMS patients who were positive for the HLA-DRB1*03 had significantly more relapses since onset than HLA-DRB1*03-negative POMS patients (6.9 ± 4.9 vs. 4.2 ± 4.4, p = 0.005), while they also had more thoracic spinal cord lesions (61.5% vs. 27%, p = 0.043) (Table 4). It is noted that HLA-DRB1*03:01-positive patients had the same disease duration with HLA-DRB1*03-negative patients (161.6 ± 110.9 vs. 130.5 ± 115.6 respectively, p = 0.432).
Demographic and clinical comparisons between HLA-DRB1*03-positive and HLA-DRB1*03-negative POMS patients.

MS = multiple sclerosis, POMS = pediatric-onset MS, EDSS = Expanded Disability Status Scale, CIS = clinically isolated syndrome, CDMS = clinically definite MS, OR = odds ratio, CI = confidence interval.
aMann–Whitney U tests for numerical and Fisher’s chi-square exact test for categorical characteristics.
*p ≤ 0.05.
A sensitivity analysis was conducted for annual relapse rate (ARR) by using a negative binomial model with log(duration of disease in years) as an offset variable after adjusting for the HLA-DRB1*03, gender, and disease type predictors. The HLA-DRB1*03 allele remained a strong significant predictor of relapses (ARR for HLA-DRB1*03-positive patients 0.85 ± 0.25 and for HLA-DRB1*03-negative patients 0.43 ± 0.08, p = 0.037). Also, after adjusting for disease duration and type of MS in a logistic regression model, HLA-DRB1*03-positive patients were more likely to have thoracic spinal cord lesions than HLA-DRB1*03-negative patients (OR 5.66, 95% CI 1.17–27.35, p = 0.031).
No other significant association was found between HLA and any other demographic or clinical parameter.
Discussion
MHC represents a cluster of highly polymorphic genes, which encode cell-surface proteins on antigen-presenting cells of the peripheral (macrophages and dendritic cells) and central (astrocytes and microglia) immune system, assisting antigen presentation to T-lymphocytes and participating in the initiation of the inflammatory cascade. 26 POMS patients manifest increased activation of CD4+ T memory cells and increased proportions of Th17 central memory cells compared to HCs and AOMS patients, along with increased levels of pro-inflammatory and fewer regulatory B cells.27,28 Moreover, dozens of environmental factors and exposures increase the risk for developing AOMS or POMS through their interplay with the HLA locus, including and, probably not limited to, Epstein–Barr virus (EBV) remote infection, exposure to ultraviolet radiation and vitamin D status, obesity, puberty, and smoking.18,19,29–31
We report the results of low-resolution HLA-DRB1 genotyping, as done in other Caucasian populations, and its possible clinical and imaging impact on POMS in a representative Hellenic sample of 50 POMS patients, comparing them to 144 AOMS patients and 246 HCs. On a rough epidemiological basis, no major or meaningful differences were noticed regarding the clinical and imaging characteristics of our POMS patients compared to other pediatric populations. 1 More than 95% of POMS patients follow a relapsing–remitting course at onset, while PPMS is exceptionally rare, occurring in less than 2% of children.1,32 In our study, none of the POMS patients presented with primary progressive disease, which can be attributed to our sample size compared to that of large, multicenter series. 32 There are no sufficient data regarding the exact time interval for progression of our POMS to SPMS. Nevertheless, 11 patients (22%) progressed to secondary progressive disease, a percentage in accordance with other series. 32
Regarding HLA genotyping, we reconfirm HLA- DRB1*15 allele as more frequent in POMS patients than HCs, but do not observe any association between the presence of HLA-DRB1*15 and earlier age of MS onset. 5 In our research we had no information regarding the genotypes of the patients’ parents. As a result, a possible parent of origin effect which could correlate lower age of onset with the maternally or paternally transmitted genes could not be tested. A protective effect of HLA-DRB1*11 allele was also noticed, as MS patients show decreased frequencies of this allele, irrespectively of age at disease onset, a finding also confirmed in older studies.5,33
We have previously shown that the HLA-DRB1*03 allele is associated with disease risk. 5 This allele has been associated with MS susceptibility, 34 and with the presence of IgM OCBs. In older studies, the HLA-DRB1*03 allele did not affect clinical disease severity, cognition, or cerebral atrophy, although in one study it was associated with better MS prognosis.3,15 Interestingly, the HLA-DRB1*03 allele has been strongly associated with NMO, a mainly humoral, anti-AQP4 disease entity. 35 The higher frequency of HLA-DRB1*03 in POMS than AOMS patients (p = 0.042*) and especially HCs (p = 0.004, p ≤ 0.017 in B-Y correction method) was clearly demonstrated. This correlation, and at such a statistically significant degree, could indicate a probably enhanced role of humoral immunity in POMS, which, if confirmed, could shift our therapeutic strategies to B-cell-directed therapies in the future. To our knowledge, such a finding concerning the HLA-DRB1*03 allele risk in POMS has not been reported in other populations.
The clinical significance of HLA-DRB1*03 predominance is strengthened further by the comparative analysis of patients’ clinical characteristics on the basis of the most frequently observed HLA genotypes. HLA-DRB1*03-positive POMS patients present an increased number of clinical relapses and an enhanced lesion burden at the thoracic level, compared to HLA-DRB1*03-negative patients. It is noted that HLA-DRB1*03:01-positive patients had the same disease duration and the above effects remained significant in the sensitivity analysis that has been accomplished. On the basis of this finding, we suggest that the HLA-DRB1*03 allele not only predisposes to POMS, but is also correlated with increased disease activity. This finding needs further verification in larger samples, even in different ethnic groups, for safer conclusions. There is paucity of HLA genotypic/clinical correlation studies in POMS, with only a few exceptions. Specifically, there are some isolated correlations of HLA-DRB1*15 with a low vitamin D-dependent relapse rate,18,19 and possibly a later age at menarche. 19
Limitations in our study are the low-resolution technique performed for HLA genotyping and the relatively small sample size. Nevertheless, POMS accounts for approximately 3–5% of all MS cases and, thus, all studies in POMS have inherent difficulties. In this regard, our sample of 50 Hellenic POMS patients represents a proportionally satisfactory number. We would like to underline that all the participants of our POMS, AOMS, and HC groups come from reference centers from all over Greece. In the Hellenic population no allelic association of HLA-DRB1 has been found concerning the age and gender, and our POMS and HC groups studied here have the same age range (approximately 20–55 years old). Thus, the low-resolution HLA genotyping represents a satisfactory process, as a first step concerning the POMS sample in the Hellenic population and the HLA-DRB1*03 allele cannot be altered by high-resolution typing, but only to be enriched with more digits, corresponding each high-resolution level.
In conclusion, our study reports in a relatively large country-wide pediatric MS sample the HLA-DRB1 frequencies, as well as the correlations of specific HLA-DRB1 alleles with clinical and MRI characteristics in Hellenic POMS.
Footnotes
Conflict of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publicationof this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.