
Abstract
Background
Risk factors for chronic disease include smoking, hazardous alcohol consumption, physical inactivity, unhealthy body mass index and poor diet (SNAP factors). In multiple sclerosis (MS) SNAP factors are associated with health outcomes such as disability in cross-sectional studies, but longitudinal data are lacking.
Objective
The objective of this study was to assess whether a combined SNAP risk score predicts disability worsening.
Methods
Longitudinal self-reported data from two time-points 2.5 years apart from an international survey of 1225 people with MS were used in linear regression models adjusted for potential confounding. Disability worsening was measured using the patient-derived Multiple Sclerosis Severity Score.
Results
The majority (62%) had two or more risk factors, with insufficient fruit and vegetable intake (83%), unhealthy body mass index (42%) and physical inactivity (33%) most common. Some SNAP factors at follow-up were associated with disability at follow-up (cross-sectionally), and in addition there was some evidence that increasing risk factors was associated with disability worsening over the 2.5 year study period. Baseline SNAP score was not predictive of disability worsening at follow-up, however.
Conclusion
Known risk factors for morbidity and mortality were common and associated with disability cross-sectionally, but not prospectively. Further studies using longer time frames, objective measures and interventions may elucidate potential benefits from changes in risk factors on MS outcomes.
Introduction
The majority of people with multiple sclerosis (MS) (around 90%) are initially diagnosed with the relapsing–remitting type of MS (RRMS).1,2 RRMS is characterised by relapses, onset of new neurological symptoms caused by lesions in the central nervous system (CNS), but often subsequent near-complete recovery. In most people with MS, however, such clinically evident relapses together with clinically silent lesion-causing relapses cause accumulating disability. Disability worsening is frequently seen as an important health outcome for patients and often used in studies assessing treatment outcomes in MS.
Although pharmacological treatments can be effective in delaying disability worsening and recent developments are promising, 3 they can have significant side effects, and treatment strategies for people with progressive MS are very limited.4,5 Identification of modifiable factors associated with disability worsening, which may be targeted through interventions, are a priority for people with MS. 6 Data from a North American study show that there is a high frequency of smoking, poor nutrition, alcohol consumption and low physical activity (the SNAP risk factors) in people with MS and that these modifiable risk factors commonly co-occur. 7 The SNAP risk factors, usually also including body mass index (BMI), are used as a framework to assess and modify risk factors for chronic disease in Australian general practice. 8 The recommendations as per the SNAP framework include smoking abstinence, non-hazardous alcohol consumption, regular physical activity, healthy BMI and sufficient fruit and vegetable intake. 8
While these risk factors are common in people with MS, and have been cross-sectionally associated with physical and mental health measures including level of disability, 9 it is unclear how they are associated with disease outcomes over time. A longitudinal imaging study showed that a lower healthy heart score, similar to SNAP, is associated with accelerated central brain atrophy in MS patients over time. 10 Our study aimed to assess whether the SNAP score, and change thereof, predicted disability and disability progression using longitudinal data from an international survey of people with MS.
Methods
Ethics
Ethics approval was granted by St Vincent’s Hospital Melbourne Human Research Ethics Committee (LRR055/12) and subsequently by The University of Melbourne’s Health Sciences Human Ethics Sub-Committee (HESC 1545102).
Participants and recruitment
The Health Outcomes and Lifestyle In a Sample of people with Multiple sclerosis (HOLISM) study recruited adults who self-reported a diagnosis of MS in 2012. 11 Recruitment advertisements were placed on online social media and forums and sent to email newsletters, MS organisations and societies worldwide to invite people to complete an online survey. After 2.5 years from the baseline HOLISM survey, all participants were invited by email to complete a similar follow-up survey online. Participants provided online consent and indicated they were aged 18 years or older. Participants were matched between waves based on participant IDs, name, date of birth and location of residence. More information regarding the methodology of the HOLISM study has been published previously. 12 Participants with a complete baseline SNAP score were included in this study.
Survey
HOLISM surveys included validated questionnaires where possible, and all data were self-reported. Demographic variables collected included age, sex and level of education. Clinical characteristics collected included current type of MS as diagnosed by a medical doctor, duration of MS since onset of symptoms, duration of MS since diagnosis by a medical doctor and, in addition, whether a participant was experiencing symptoms of a recent relapse at the time of the survey. Perceived relative socio-economic status (SES) was assessed by a nine-step ladder item where participants could indicate to what degree they perceived themselves to be poorer or richer compared with others in their country of residence. For analysis purposes, this nine-item scale was consolidated into three categories: Lower, Same, and Higher.
To assess level of disability, the Patient-Determined Disease Steps (PDDS), a self-reported equivalent of the Expanded Disability Status Scale commonly used to assess gait disability, 13 was included. The PDDS score in combination with disease duration informed the patient-derived Multiple Sclerosis Severity Score (P-MSSS), which estimates the disease duration-adjusted level of disability, where a higher score indicates greater disease severity. 14
SNAP (smoking, nutrition, alcohol, physical activity) was initially designed as a policy framework by the Australian government, and since adopted by The Royal Australian College of General Practitioners to include BMI. 8 SNAP risk factors were recorded in the HOLISM surveys.
Smoking status (never, former, current smoker) was assessed and categorised into current non-smoker (score of 1) or current smoker (score of 0) as per the SNAP recommendations. Fruit and vegetable intake was assessed using the modified Diet Habits Questionnaire; 15 consuming ≥5 serves of vegetables/day and ≥2 serves of fruit at least six days/week was scored as 1, as per the Australian Dietary Guidelines. 16 Alcohol consumption frequency (never drink to drink daily) and volume (ranging from ‘not applicable’ to 10+ standard drinks per day) were assessed and converted to standard drinks per week. Those consuming ≤2 standard alcoholic drinks/day, the Australian recommendation, 17 were assigned a score of 1 or 0 otherwise. Physical activity was assessed using the International Physical Activity Questionnaire-Short Form and participants were categorised as reporting either no/low physical activity (score of 0) or moderate/high levels of physical activity (score of 1). 18 BMI was computed from self-reported weight and height and classified using the World Health Organization classification system. 19 Healthy BMI was scored as 1, while underweight, overweight or obese BMI were scored as 0.
These individual scores were summated, resulting in a SNAP score ranging from 0 (all SNAP risk factors) to 5 (no SNAP risk factors), treated as a categorical variable. Given the relative infrequency of those with SNAP scores of 0, these were aggregated with 1.
Change in SNAP score between reviews was calculated as the difference between baseline and 2.5-year follow-up. Given the infrequency of marked change, those with increases of 2 and 3, or decreases of 2 and 3, were consolidated, and estimates of associations evaluated relative to 0 change.
Data analysis
Annualised disability change was estimated as the difference in P-MSSS between baseline and 2.5-year review, divided by the duration between waves in years. This variable was sufficiently homoscedastic that transformation was not required. Linear regression models were used for all analyses. Cross-sectional analyses examining the associations of individual SNAP factors, and SNAP score, with P-MSSS were adjusted for age, sex, MS type, perceived relative SES and whether participants were having ongoing symptoms from a recent relapse in the 30 days preceding review, based on a directed acyclic graph informed by the literature. Predictors of change in P-MSSS were also adjusted for these factors as well as baseline P-MSSS and baseline ongoing symptoms from a recent relapse.
Results
Cohort characteristics
Of 2466 people with MS at baseline, 1225 provided necessary information at 2.5-year follow-up for analyses in this study. Participants were from countries all over the world, with the majority from North America, the United Kingdom, Australia and New Zealand. Completion of the 2.5-year wave was associated with better health and healthier BMI as reported previously, 12 but not with any of the other SNAP factors. Most (82.2%) participants were female, were an average 45.9 (SD = 10.5) years of age at baseline, of median P-MSSS at baseline of 4.4 (interquartile range = 2.4–7.3), and the majority (63.3%) had RRMS (Table 1). About one-half of participants had a higher perceived SES compared with others in their country of residence at follow-up (not collected at baseline).
Cohort characteristics at baseline and 2.5-year review.

SNAP: smoking, nutrition, alcohol, physical activity; IQR: interquartile range; MS: multiple sclerosis; P-MSSS: patient-determined Multiple Sclerosis Severity Score
SNAP score
The sample had a mean baseline SNAP score of 3.2 (SD = 1.0) and only 4.7% having scores ≤1 (Table 2). The majority had two or more risk factors at baseline, most commonly insufficient fruit and vegetable intake (82.9%), unhealthy weight (41.9%) and insufficient physical activity (32.9%). Mean SNAP score at follow-up was 3.2 (SD = 1.0). While there was no overall material change in SNAP scores (mean = 0.0, SD = 0.9), 24.0% decreased and 27.1% increased their SNAP score between reviews, SNAP scores were significantly higher (healthier) among those with higher education (ptrend<0.001). Neither age nor sex was significantly associated with SNAP score.
SNAP risk factors at baseline and 2.5-year review.
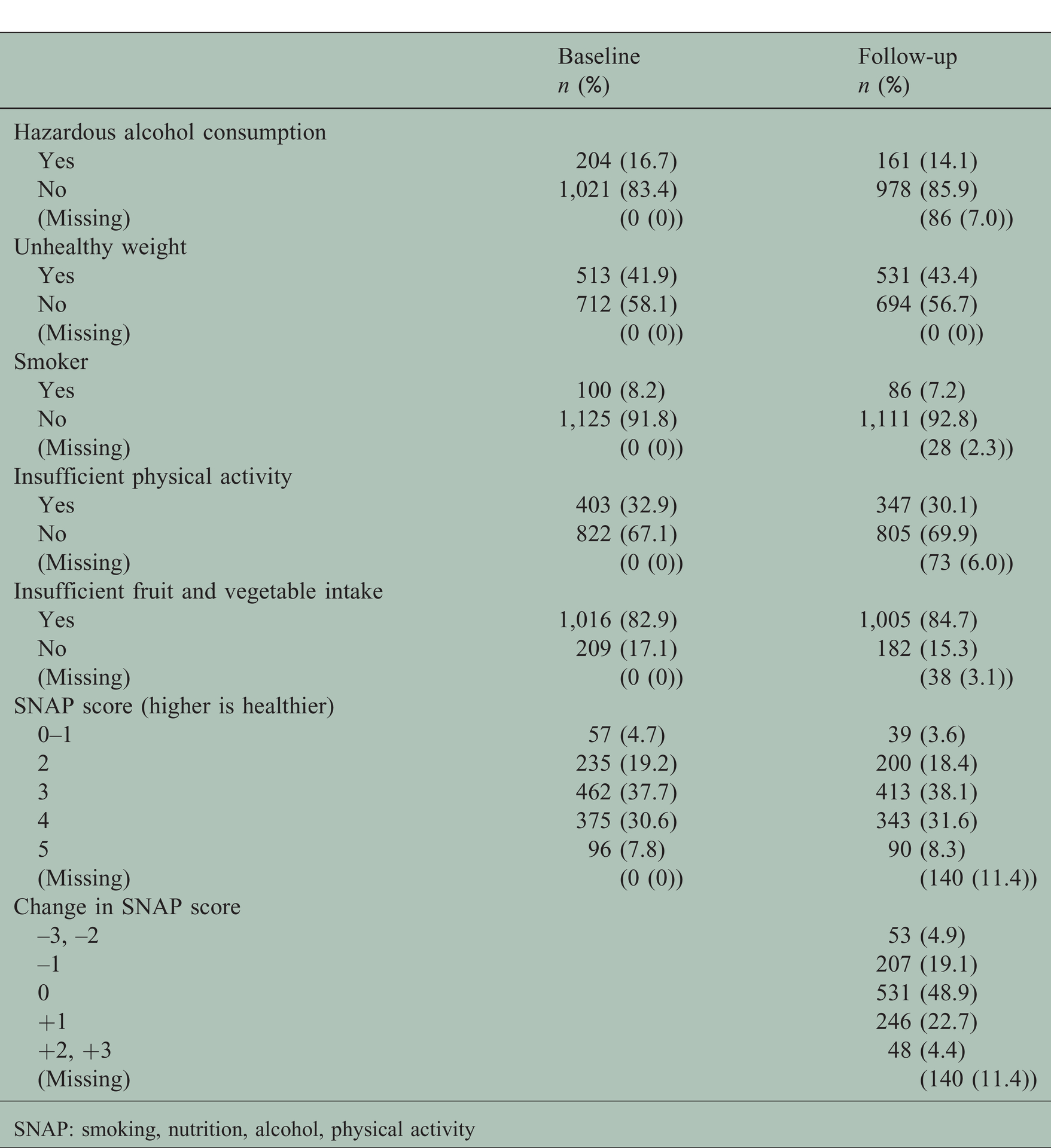
SNAP: smoking, nutrition, alcohol, physical activity
SNAP score at follow-up was associated with lower disability, such that those with a score of ≥4 had 1.0-points lower P-MSSS and those with a score of 5 had 1.1-points lower P-MSSS (Supplementary Material Table 1 online). Individual SNAP factors associated with significantly lower disability included healthy weight (–0.4 points) and healthy physical activity (–1.3 points), while there was some evidence that non-smoking could be associated with lower disability (–0.5, p = 0.07).
Baseline SNAP score (Table 3) and individual SNAP risk factors (Supplementary Table 2) were not significantly associated with annualised change in P-MSSS. However, there was a significant trend in the association between change in SNAP score and P-MSSS score (p=0.039), such that those who decreased their SNAP score during follow-up (increasing risk factors) had greater disability worsening, while those who increased their score (decreasing risk factors) had lower disability worsening (Table 3; Figure 1 with geometric means). Stratifying by MS type did not change results (not shown).

Associations between change in SNAP score and annualised change in patient-derived Multiple Sclerosis Severity Score (P-MSSS). Adjusted for baseline P-MSSS, whether participants were having ongoing symptoms from a recent relapse at the time of disability measures, age, sex, baseline multiple sclerosis type and socioeconomic status.
SNAP score at baseline as predictor of annualised change in disability.

Models adjusted for baseline patient-determined Multiple Sclerosis Severity Score, whether participants were having ongoing symptoms from a recent relapse at the time of disability measures, age, sex, baseline multiple sclerosis type and socioeconomic status.
SNAP: smoking, nutrition, alcohol, physical activity; CI: confidence interval
Discussion
Most participants in our study did not meet health recommendations to prevent chronic disease; the majority had two or more SNAP risk factors at baseline, including insufficient fruit and vegetable intake (83%), unhealthy weight (42%), insufficient physical activity (33%), hazardous levels of alcohol consumption (17%) and smoking (8%). These findings are in line with data from a small North American study in people with MS which showed similar prevalence rates of risk factors poor diet (86%) and excess alcohol consumption (10%, more conservative cut-off for women in their study), although they reported prevalences of smoking and insufficient physical activity twice as high (16% and 62% respectively) compared with our study. 7 Similarly, a large study from the North American Research Committee on MS (NARCOMS) registry reported a smoking prevalence of 17% 20 in 2004. However, a later study on health behaviours reported a smoking prevalence of 9% and insufficient physical activity participation of 37%, 21 more in line with our results. An Australian study using a representative sample of people with MS also reported much higher occurrence of these same risk factors, with 90% not meeting dietary recommendations regarding fruit and vegetable intake, 47% insufficiently physically active and 61% with a BMI outside the healthy range. 22
We did not find strong evidence that individual SNAP risk factors, or a combined SNAP score at baseline, were prospectively associated with disease duration-adjusted level of disability at follow-up. However, we found that physical activity, healthy weight and potentially smoking at follow-up were cross-sectionally associated with lower levels of disability. These results were in line with findings from the aforementioned large cross-sectional study from the NARCOMS Registry, reporting that a composite lifestyle score including healthy diet (>median diet quality score), healthy weight (BMI <25), physical activity (participating in exercise in the past month) and smoking abstinence were associated with better health outcomes, including disability. 21 We found some evidence that a change in SNAP score was associated with disability, such that those who decreased their SNAP score during follow-up (increasing the number of risk factors) had greater disability worsening, while those who increased their score (decreasing the number of risk factors) had lower disability worsening (ptrend=0.039). However, because these changes in disability worsening and SNAP factors were measured over the same period, we cannot infer temporality or causality. Therefore, while these risk factors are associated with disability levels cross-sectionally, in line with the literature, we did not find a prospective link.
A recent systematic review of observational studies by Hempel et al. concluded that smoking is a risk factor for disability worsening in people with MS. 23 Similarly, several studies suggest a role for physical activity, 24 higher BMI and an adverse lipid profile 25 in disability worsening, although Hempel et al. concluded that there is insufficient evidence to reach definite conclusions about these modifiable factors. 23 Studies assessing the role of alcohol consumption in disability worsening shows mixed results, 23 with one recent cross-sectional study showing associations of red wine or alcohol consumption with lower levels of disability but increased CNS lesions. 26 However, a systematic review of interventions of modifiable factors showed no evidence of benefit for disability worsening. 27
The foundations of secondary prevention of cardiovascular disease are modifying risk factors: promoting smoking cessation, healthy BMI, low saturated fat intake, regular physical activity and low alcohol consumption. 28 Similarly, these modifiable factors have been implicated in cancer. 29 It is likely that these factors play a role in health outcomes for people with MS also. In relation to MS-specific outcomes such as disability worsening and disease progression, observational studies and some small trials show similar links between modifiable factors and health outcomes; however, solid evidence for long-term benefits of behaviour changes or interventions is still lacking. 27
Strengths and limitations
This study, like many other surveys, is susceptible to participation bias. Only English-speaking volunteer participants were included in this study. Participants unable to use a device on which to complete the online survey, with severe vision, cognitive or dexterity impairment are unlikely to have participated. Attrition bias is another limitation, as attrition (not at random) between baseline to 2.5-year follow-up was 43.2% (n = 1063). 12 In light of these limitations, results presented in this study may have biased estimates and associations may be less representative of the general MS population. Further, measurement error may have resulted from self-reported data on which our study relied. It is possible that the prevalence of risk factors among people with MS is higher than what we have reported. While examining the association between change in SNAP score and P-MSSS score linearity was assumed, while future research may examine the shape in more detail. Finally, as disability progresses slowly in most people with MS, longer follow-up times would strengthen these analyses, and ongoing follow-up studies from this dataset are planned. Strengths of this study include a large, international sample, with a wealth of data on modifiable factors for which there was a substantial exposure gradient. This enabled us to look at a composite risk score, rather than associations with individual factors only.
Conclusion
Most people with MS in our sample, like the general population, do not meet dietary recommendations regarding fruit and vegetable intake, and many do not meet recommendations to have a BMI in the healthy range, or participate in regular physical activity. Our longitudinal self-reported data showed some evidence for an association between increasing SNAP risk factors and disability worsening, although causality could not be determined from this analysis. While our study confirmed cross-sectional associations between modifiable risk factors and health outcomes, our data collected at two time points, 2.5 years apart, did not show strong evidence for a prospective association between baseline SNAP score and disability worsening. Further prospective studies with longer follow-up, representative samples, and objective measures are needed to elucidate potential benefits from changes in modifiable risk factors on MS outcomes.
Supplemental Material
MSO881769 Supplemental Material - Supplemental material for Does a modifiable risk factor score predict disability worsening in people with multiple sclerosis?
Supplemental material, MSO881769 Supplemental Material for Does a modifiable risk factor score predict disability worsening in people with multiple sclerosis? by Claudia H Marck, Zoe Aitken, Steve Jr Tracey J Weiland and George A Jelinek in Multiple Sclerosis Journal—Experimental, Translational and Clinical
Footnotes
Author contribution
CHM, ZA, TJW and GAJ were involved in study conception. CHM was involved in data management, data collection and led the design of the study and drafting of the manuscript. SSJr was responsible for data analyses. All authors were involved in study design and editing of the draft and approve it for submission.
Conflicts of Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GJ has received remuneration for facilitating lifestyle courses for people with MS and royalties for the books Overcoming multiple sclerosis: The evidence based 7 step recovery program; Overcoming Multiple sclerosis: The evidence based guide to recovery and Taking control of multiple sclerosis. The other authors report no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bloom Foundation, Wal Pisciotta, anonymous donors and a National Health and Medical Research Council Early Career Fellowship (APP1120014).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.