
Abstract
Stigma associated with neurological disorders may contribute to a poor health-related quality of life. However, limited information is available in primary progressive multiple sclerosis. We investigated the presence and impact of stigma in patients with primary progressive multiple sclerosis. A non-interventional, cross-sectional study was conducted. A total of 55 primary progressive multiple sclerosis patients were studied (mean age 55.8±9.5 years, 56.4% male). The median Expanded Disability Status Scale score was 5.5 (4.0–6.5). Stigma prevalence was 78.2% (n=43). Twenty-four patients (43.6%) were classified as depressed. Scores on the eight-item Stigma Scale for Chronic Illness correlated with physical (rho=0.464, p<0.001) and psychological (rho=0.358, p=0.007) 29-item Multiple Sclerosis Impact Scale subscores. Stigma predicted concurrent depression (odds ratio=1.13; p=0.046). Stigma was highly prevalent with a detrimental effect on quality of life and mood in primary progressive multiple sclerosis.
Keywords
Introduction
Primary progressive multiple sclerosis (PPMS) accounts for 10–15% of the overall population with multiple sclerosis (MS). 1 Patients with PPMS usually become dependent on others, need assistance to carry out daily activities, and have high healthcare utilization. 2 Stigma refers to the disapproval and shame felt by people exhibiting characteristics that society considers wrong or unusual. 3 Stigma associated with chronic illnesses may contribute to lowered self-esteem, depression, anxiety and poor quality of life outcomes. 3 Patients with MS can feel stigmatised whereby the individual possesses characteristics that are either internally or externally perceived to be inferior, thus resulting in devaluation, rejection or exclusion.4–7 There is limited information available on the presence of stigma in patients with MS and no studies that have focused on patients with PPMS. The aim of this study was to assess the presence of stigma and its impact on health-related quality of life and mood in patients with PPMS.
Methods
A non-interventional, cross-sectional study in subjects with primary-progressive MS was conducted (the Understanding Primary Progressive Multiple Sclerosis (UPPMS) study).
Key eligibility criteria were age ≥18 years old, diagnosis of PPMS according to McDonald 2010 criteria, and duration of MS symptoms less than 10 years.8 Patients were recruited from 11 MS units in Spain between January–July 2017. The study was approved by the investigational review board of the Hospital Universitario 12 de Octubre (Madrid, Spain).
Outcome measures
The eight-item Stigma Scale for Chronic Illness (SSCI-8), the 29-item Multiple Sclerosis Impact Scale (MSIS-29) and the Beck Depression Inventory-Fast Screen (BDI-FS) were used to gather information from the patient´s perspective on stigma, health-related quality of life and depressive symptoms, respectively.3,9,10 The SSCI-8 includes eight items rated on a five-point Likert scale from ‘1’ (never) to ‘5’ (always). The total score ranges from 8–40, with higher scores indicating greater perception of stigma. 3 The SSCI-8 demonstrated validity and internally consistency across a sample of people with different neurological disorders, including MS.3,11 The MSIS-29 has two subscales: a 20-item physical impact scale and a nine-item psychological impact scale. 9 The BDI-FS is a seven-item questionnaire on a three-point scale. Scores can range from 0–21. 10 Cut-off scores ≥4 and ≥9 are used to define the presence of depression and moderate-to-severe depression, respectively.
Statistical analysis
Associations between patient-reported outcomes were analysed using Spearman’s rank correlation (SSCI-8 total score and the MSIS-29 physical and psychological impact subscales scores) and logistic regression (assessing the contribution of stigma to symptoms of depression (depressed, not depressed)).
Results
A total of 55 patients were included in the study. The main socio-demographic and clinical characteristics of the sample are shown in Table 1.
Socio-demographic and clinical characteristics of the sample.
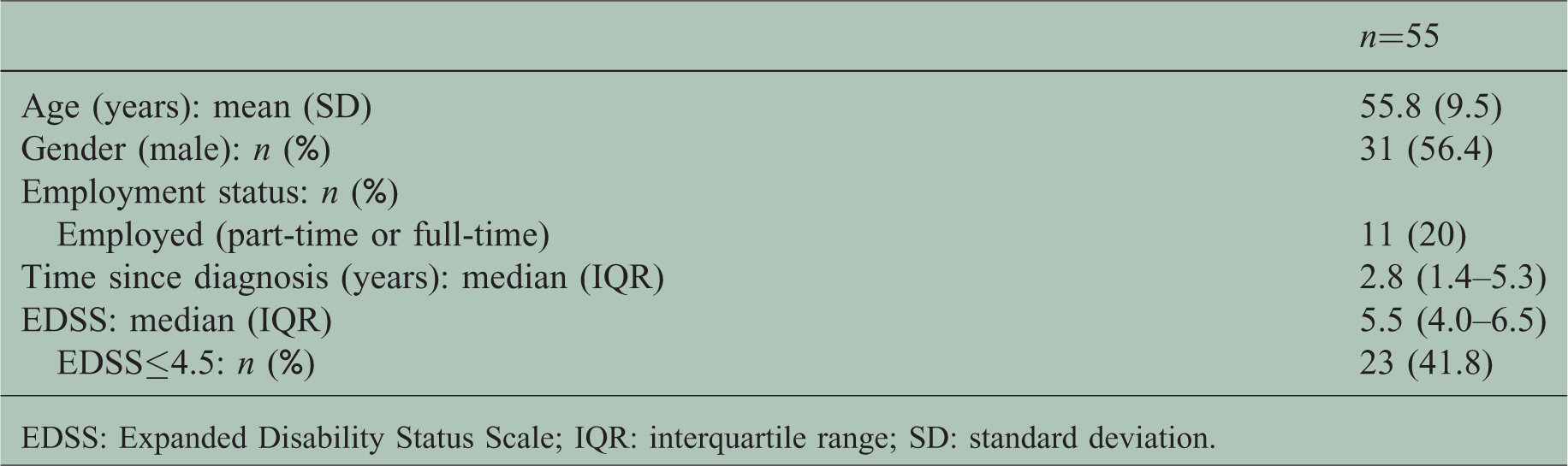
EDSS: Expanded Disability Status Scale; IQR: interquartile range; SD: standard deviation.
Stigma prevalence was 78.2% (95% confidence interval (CI) 64.6–87.8 (n = 43)) using a SSCI-8 cut-off score >8 (Table 2). Scoring for individual items showed the most strongly perceived stigmatization was the feeling of being left out of things and embarrassment about physical limitations, followed by embarrassment about the illness. Twenty-four patients (43.6%) were classified as depressed and six (11%) had moderate-to-severe depression.
Stigma, health-related quality of life and depression.
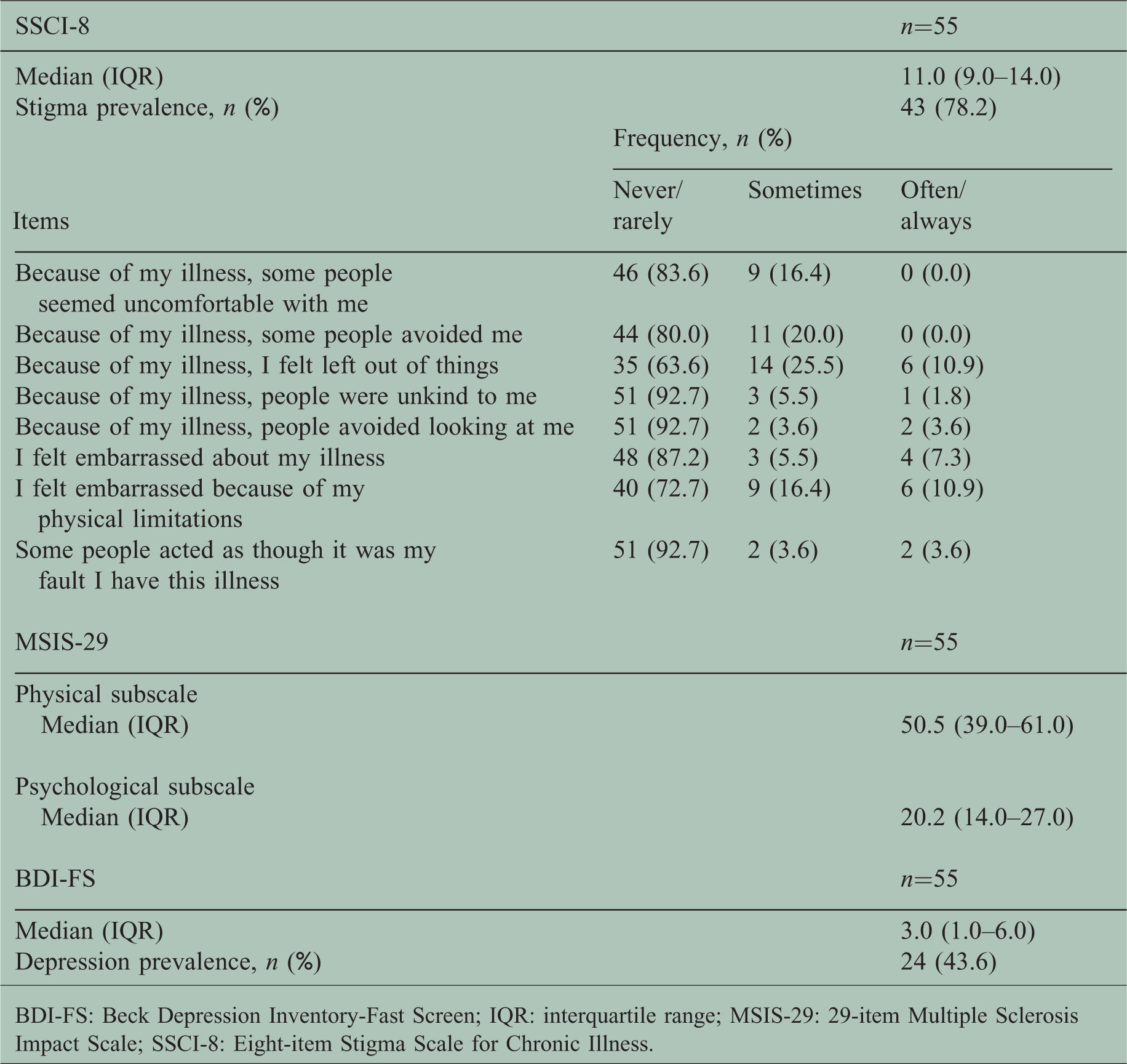
BDI-FS: Beck Depression Inventory-Fast Screen; IQR: interquartile range; MSIS-29: 29-item Multiple Sclerosis Impact Scale; SSCI-8: Eight-item Stigma Scale for Chronic Illness.
The SSCI-8 score showed a significant correlation with both physical (rho=0.464, p<0.001) and psychological (rho=0.358, p=0.007) MSIS-29 subscale scores. A correlation between Expanded Disability Status Scale (EDSS) and SSCI-8 scores was found (rho=0.248, p=0.06). Stigma was found to positively predict concurrent depression with an odds ratio (OR) of 1.13 (95% CI: 1.00–1.28; p=0.046).
Discussion
PPMS is characterised by insidious progression of disability over years with no remission and low magnetic resonance activity. 1 Stigma associated with neurological disorders may contribute to a poor health-related quality of life. 3 In our study, most patients with PPMS reported some degree of stigmatization and most responses were of low-to-moderate severity. Stigmatization was found to have a strong negative correlation with physical and psychological quality of life, and was able to positively predict depression.
The impact of stigmatisation on patients with MS has only recently begun to be explored. An online survey conducted in the USA using a combination of seven stigma measures found that perceptions of stigma were relatively low in patients with MS. 7 However, stigma was highly prevalent but low in severity in a Dutch study with 185 patients. 4 Individuals with a higher level of disability experienced more stigma (enacted stigma B=0.044, p<0.05; self-stigma B=0.063, p<0.01). In a sample of 342 patients from Greece, stigma showed statistically significant negative correlations with both physical and mental health dimensions of the Multiple Sclerosis Quality of Life-54 questionnaire. 6 Perception of stigma was also associated with greater informal caregiver’s burden (OR=3.83, 95% CI 1.84–7.96) in a survey of 530 patients from Canada. 12 In addition, results from the semi-annual survey administered by the North American Research Committee on Multiple Sclerosis (NARCOMS) showed that higher levels of stigma were significantly associated with more depressive symptoms. 5 Stigma continued to predict significantly higher levels of depression one year later, even after controlling for covariates. Ballesteros et al. recently reported the presence of stigma ‘often’ or ‘always’ in almost 20% of a sample of 201 patients from Spain (median SSCI-8 score of 10.0, interquartile range: 8.0–14.0). 11 Most patients in all of these studies had relapsing–remitting or secondary progressive MS. Additional differences regarding our findings could be based on the administration of different instruments to assess stigma and selection processes to recruit patients.
Our study has several limitations. Socio-demographic and clinical characteristics such as patients’ economic status, current disease-modifying treatment, and number of hospital admissions were not collected. The relatively small sample size and the cross-sectional analysis could be additional limiting factors. Despite limitations, the study also has several strengths. The sample was managed in 11 different MS units on a national level, which allows results to be generalised to community practice.
Conclusions
Stigma was highly prevalent and detrimental to health-related quality of life and mood in patients with PPMS. Identifying stigma may be crucial to implement specific educational intervention strategies and as a screening tool to identify individuals with or at risk of depression. Further studies with a larger sample size and longitudinal follow-up are needed to confirm these results.
Footnotes
Acknowledgements
The authors wish to thank the patients and their families for making the UPPMS study possible. The abstract of this article was presented at the 34th Congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS) as an ePoster presentation with interim findings (October 10, 2018).
Conflict of Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DP and JM are employees of Roche Farma Spain. None of the other authors report any conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Medical Department of Roche Farma, Spain.