
Abstract
Background
In the Middle East and North Africa (MENA) region, few studies explored the quality of life of multiple sclerosis patients and the factors affecting it.
Objective
The objective of this study was to explore studies on multiple sclerosis quality of life in the MENA area through a comprehensive literature review. To validate the Multiple sclerosis international Quality of Life (MusiQoL) and Modified Fatigue Impact Scale (MFIS) in Arabic, and investigate the impact of sociodemographic and clinical variables of Lebanese multiple sclerosis patients on quality of life.
Methods
As part of an ongoing observational prospective research study, data from 663 stable multiple sclerosis patients were analysed.
Results
In Lebanese multiple sclerosis patients, the Arabic MusiQoL and MFIS seem to be accurate and valid tools with high reliability coefficients and confirmatory factor analytic indices. Variables such as age and disease type predicted multiple sclerosis quality of life, yet were significantly affected by psychosocial fatigue. The influence of sociodemographic and clinical variables on quality of life dimensions varied. Being a woman with multiple sclerosis, receiving medications and experiencing physical fatigue worsens the psychological wellbeing quality of life dimension.
Conclusion
Several sociodemographic and clinical variables predicted the health-related quality of life dimensions of multiple sclerosis patients in MENA. Further in-depth investigation to guide more targeted clinical management is recommended. We encourage using validated multidimensional tools to measure quality of life in MENA such as the Arabic MusiQoL.
Introduction
Multiple sclerosis (MS) affects the patients’ health-related Quality of Life (QoL) at all disease stages.1,2 Eckhart and colleagues theoretically defined health-related QoL as ‘physical and mental health perceptions of positive and negative aspects of life’. 3 The construct ‘health-related QoL’ is subjective and multidimensional. It includes physical and occupational functions, as well as psychological and social interactions. 4 These discrete QoL components can be affected by several factors including sociodemographic and clinical ones. 5 The most significant predictors include age and sex,5,6 disability (Expanded Disability Status Scale; EDSS) and depression.5,7–11 Often, a discrepancy between clinician and patient-perceived importance of different health-related QoL domains exists. 12 Some clinicians tend to place more importance on physical domains and less importance on mental and emotional domains when compared to patients. 12 Therefore, measuring the different patients’ perceived health-related QoL components accurately is essential, especially during clinical assessment and therapy planning. It is as essential to use cross-culturally valid measures to capture variances between sociocultural groups to ensure adequate treatment plans. 13
Several QoL measures have been used with MS patients. Some are generic or MS specific, while others combine both. 2 Disease-specific MS QoL measures were developed such as the Multiple sclerosis international Quality of Life (MusiQoL) questionnaire, 14 and the Multiple Sclerosis Impact Scale-29 (MSIS-29). 15 Both have good internal consistency and test–retest reliability. While the MSIS-29 assesses the disease physical and psychological aspects, 15 the multidimensional MusiQOL assesses different MS-related domains: activities of daily living, psychological wellbeing, symptoms, relationships, sentimental and sexual life, coping and rejection. 14
Fatigue is another incapacitating MS symptom;16,17 it hinders the patients’ physical functions and employment.17,18 As fatigue is a multidimensional phenomenon affecting various dimensions, the two most commonly used multifactorial questionnaires are the fatigue severity scale (FSS) and the modified fatigue impact scale (MFIS). 19 While the FSS focuses primarily on the physical aspects, the MFIS reports the physical, psychosocial and cognitive aspects of fatigue symptoms. 18
MS prevalence in the Middle East and North Africa (MENA) regions is estimated to be 51.52/100,000 and is expected to increase over time. 20 The Middle East MS Advisory Group recommended in 2011 that routine QoL assessments be performed using the MusiQoL, supplemented by the short form 36 health survey (SF-36) if needed, during yearly clinical visits. 21
This study aimed to: (a) explore the MS QoL literature and appraise the different methods used to measure it in the MENA region; (b) investigate the psychometric properties of the Arabic version of the MusiQOL and MFIS for the first time in Lebanon; and (c) examine the different sociodemographic and clinical variables (including fatigue) impact on health-related QoL of Lebanese MS patients.
Methods
Literature search
We searched Cochrane, Embase, Medline, Pubmed and Scopus databases for the MENA MS-related QoL literature. Figure 1 represents the search process and criteria followed at different stages.

Literature search flow chart.
Research design
This study is part of a larger ongoing prospective research project conducted at the Nehme and Therese Tohme Multiple Sclerosis Center at the American University of Beirut Medical Center. The study was approved by the institutional review board of the American University of Beirut. All participants gave written informed consent before participation. Enrollment includes all age groups. A neurologist has diagnosed all patients following the revised McDonald MS diagnostic criteria 22 with Clinically Isolated Syndrome (CIS), Relapsing–Remitting Multiple Sclerosis (RRMS), Primary Progressive Multiple Sclerosis (PPMS), and Secondary Progressive Multiple Sclerosis (SPMS). Individuals with neurological diseases other than MS were excluded.
Sample characteristics
Sociodemographic and clinical information were extracted from 663 MS patients’ medical records. The former included age, sex, marital status, and education level. The latter included MS subtype, disease duration, and EDSS. Because there is an association between QoL and disease-modifying therapies (DMTs), 23 detailed information on this matter was also collected.
Quality of life
The Arabic MusiQoL version (5.4) was used 24 with permission from the publisher. The following nine dimensions are explored: activities of daily living, eight items; psychological wellbeing, four items; symptoms, four items; relationships with friends, three items; relationships with family, three items; sentimental and sexual life, two items; coping, two items; rejection, two items; and relationship with healthcare system, three items. Ten standardised scores can be derived which can range from 0 to 100; one score for each dimension and a total composite score (global index). Higher scores indicate better health-related QoL. The English version of the MusiQoL is known to have good reliability, with Cronbach’s alpha coefficients (α) ranging from 0.68 to 0.92. 24
Fatigue
The Arabic MFIS-21 version was used in this study. The MFIS is a modified form of the fatigue impact scale, 25 comprised of items derived from interviews with MS patients about how fatigue affects their lives. It includes physical, cognitive and psychosocial subscales ( 9, 10 and 2 items, respectively), and assesses the impact of fatigue impact on various daily activities. A total MFIS score is computed by adding the subscale scores, and can range from 0 to 84. The scale translation from English into Arabic followed the World Health Organization recommended process of instruments translation and adaptation. 26 The MFIS was translated and back-translated by a professional translator and the corresponding author. To assess face and content validity, a panel of five bilingual experts evaluated the 21 items in Arabic, and the items were modified according to the experts’ ratings and suggestions, then back-translated. The experts included two neurologists, two nurses and one family medicine specialist. This MFIS Arabic version can be obtained from the corresponding author. The English version of the MFIS is also known to have good reliability, with Cronbach α values for the total, physical, cognitive and psychosocial scores equal to 0.92, 0.88, 0.92 and 0.65, respectively. 27
Statistical analysis
Statistical analysis was performed using SAS System’s PROC CALIS (SAS Institute, 1990) and SPSS statistical software (version 24; SPSS Inc., Chicago, IL, USA). Descriptive statistical analysis was conducted on complete data (the mean and standard deviations for continuous variables, and frequency and percentages for the categorical variables). Group comparisons using independent t-tests and one-way analysis of variance (ANOVA) followed. Partial eta-squared (η2) was used as an effect size estimate. Pearson’s correlations were used to assess associations. Significant variables on these three sets of tests were then entered into multiple regression models as predictors. Unstandardised beta coefficients (β) are reported. P < 0.05 (two-tailed) was considered significant. Cronbach’s α values were calculated. Confirmatory Factor Analyses (CFA) were performed to assess a nine-factor structure of the MusiQoL and the MFIS 3-factor structure. To examine fit, χ2 values and four measures of goodness of fit were used to assess the CFA models: (a) the Root Mean Square Error of Approximation (RMSEA); (b) the Standardised Root Mean Squared Residual (SRMR); (c) the Non-Normed Fit Index (NNFI); and (d) the Comparative Fit Index (CFI). For the measures of fit, RMSEA should not be higher than 0.10, the SRMR value should be less than 0.08, and the values of NNFI and the CFI should be above 0.90.28,29
Results
Literature search findings
The most studied domains related to QoL in MS previously studied in the MENA region were depression,9,10,30–33 fatigue,10,32,34,35 and disability.3,8,31,32,35,36 The findings suggest that these factors are associated with poorer MS health-related QoL. The impact of a few therapies on QoL was investigated to some extent.37–47 Drawing firm conclusions on the findings of therapeutic approaches is difficult, due to the treatment choices and methods heterogeneity, and insufficient replication studies (see Supplementary Table 1).
The most frequently used instruments were the MSQoL-54 in its different versions (Arabic, Persian), followed by the SF-36 and its shortened versions (SF-12, SF-6), MSIS-29, and MusiQoL. Only three validation studies were published about MS-related QoL scales in MENA; they were all validation of the Persian QoL scales.48–50
In addition, although the three previously mentioned Persian validation studies reported good psychometric properties,48–50 these validated measures either cover one QoL dimension or are specific to particular MS-related events or symptoms.48–50 Another identified gap is related to the psychometric properties of these measures. When examining the validated tools’ internal structure, we found that two of the previous validation studies relied solely on calculating Cronbach’s alpha only as an indicator of internal consistency;48,49 while the third study did not address this matter. 50 In addition to reliability, measuring validity is fundamental; providing CFA evidence of validity was missing for most of the QoL tools previously used in the MENA. 51
Sample descriptives
The mean age of MS patients was 37.6 ± 12.3 years, and 65.2% were women. The majority were diagnosed with RRMS (82.7%), with a mean disease duration of 92.4 ± 9.6 months, and EDSS 2.15 ± 1.98. The majority were married (58.2%) at the time of data collection and attained university education (45.4%) (Table 1). MusiQoL and MFIS scores are summarised in Table 2.
Sociodemographic and clinical characteristics.
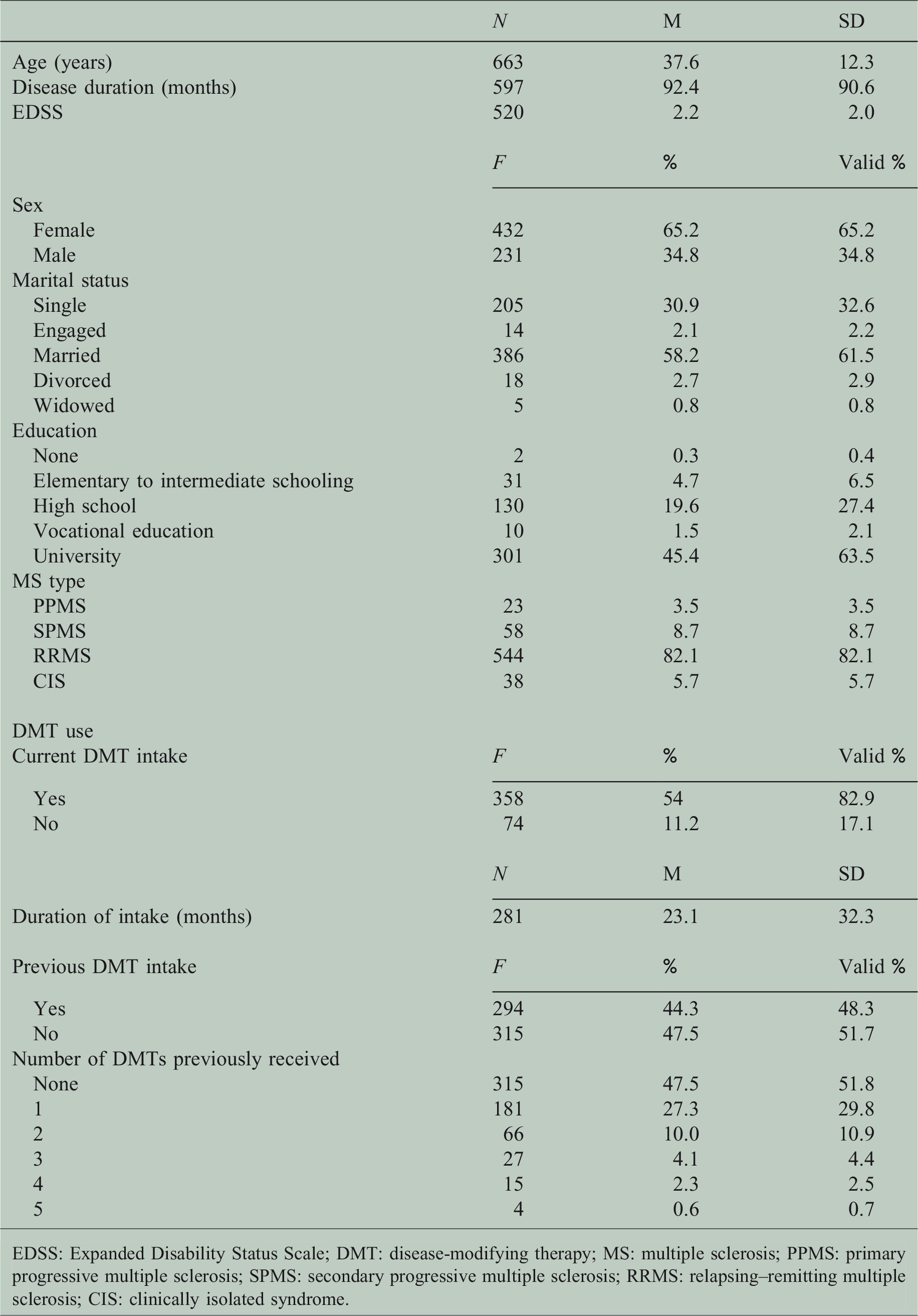
EDSS: Expanded Disability Status Scale; DMT: disease-modifying therapy; MS: multiple sclerosis; PPMS: primary progressive multiple sclerosis; SPMS: secondary progressive multiple sclerosis; RRMS: relapsing–remitting multiple sclerosis; CIS: clinically isolated syndrome.
MusiQoL and MFIS scores.

MusiQoL: multiple sclerosis international quality of life; MFIS: modified fatigue impact scale.
Sociodemographic and clinical variables associated with MusiQoL
Age was negatively associated with the MusiQoL index, along with the following MusiQoL dimensions, ‘activities of daily living’ and ‘rejection’. Getting older, being less able to engage in activities of daily living, and a greater sense of rejection was associated with worse QoL (see Supplementary Table 2). Interestingly, some scores differed based on sex. Men scored higher on the MusiQoL index 69.2 ± 15.8; (t (536) –2.1, P = 0.034)), ‘psychological wellbeing’ (60.3 ± 28.1; (t (654) –3.5, P < 0.001)), and ‘coping’ (67.3 ± 31.2; (t (626) –2, P = 0.044)) when compared to women (66.3 ± 15.2, 52.6 ± 25.7 and 61.9 ± 32, respectively). We did not find any statistically significant difference between men and women regarding disease duration, EDSS level, or any other sociodemographic and clinical variable.
Significant differences in the MusiQoL index (F (3,534) 11.6, η2 = 0.06, P < 0.001), and the following dimensions; ‘activities of daily living’ (F (3,648) 42.9, η2 = 0.17, P < 0.001), ‘psychological wellbeing’ (F (3,652) 5, η2 = 0.02, P = 0.002), and ‘rejection’ (F (3,627) 18, η2 = 0.09, P < 0.001) were found between MS subtypes. As expected, CIS patients had significantly better MusiQoL index than PPMS and SPMS. RRMS patients reported better total MusiQoL than SPMS (P < 0.001) (see Supplementary Table 3). Both variables, ‘MS disease duration’ and ‘EDSS’ , were negatively associated with the MusiQoL index and several dimensions including ‘activities of daily living’ and ‘sentimental and sexual life’. For these two independent variables, bivariate correlation analysis results refer to Supplementary Table 2.
When examining the MusiQoL association with current DMT use, only the ‘relationship with healthcare system’ differed for medication intake (t (403) –3.1, P = 0.002). Patients who at the time of data collection were on DMT reported higher scores (79.8 ± 23.5) than those who were off therapy (69.8 ± 27.2). However, the current DMT intake duration was not associated with any MusiQoL index or dimension scores (P > 0.05).
When we explored the MusiQoL based on previous DMT use, we found different results. Patients who did not receive DMTs in the past had higher MusiQoL index (69.5 ± 14.8) than those who did (64.7 ± 15.7) (t (495) 3.5, P = 0.001). Similar findings were present concerning other dimensions: ‘activities of daily living’, ‘symptoms’, ‘sentimental and sexual life’, and ‘rejection’ (Table 3). In addition, we found an effect of the numbers of DMTs (i.e. count of DMTs previously received, from 0 to 5) previously taken on the scores of the MusiQoL index (F (5,490) 3.8, η2 = 0.04, P = 0.002) and ‘activities of daily living’ (F (5,593) 10.7, η2 = 0.08, P < 0.001), ‘psychological wellbeing’ (F (5,597) 2.4, η2 = 0.01, P = 0.033), ‘sentimental and sexual life’ (F (5,548) 4.2, η2 = 0.05, P = 0.001), and ‘rejection’ (F (5,576) 2.8, η2 = 0.02, P = 0.017). We found a trend towards a decrease in MusiQoL scores as the numbers of DMTs previously received increased. For instance, patients who did not have a history of past DMT intake at the time of data collection reported better scores on ‘activities of daily living’ dimension (69 ± 26) than those who received two medications (53.3 ± 29.1, P < 0.001), three medications (44.1 ± 26.2, P < 0.001), and four medications (44.9 ± 31, P = 0.013). Receiving more than one DMT often indicates more aggressive disease, disease progression, or non-response to treatment, necessitating a change of treatment hence lowering the health-related QoL scores. Results of the Tukey post-hoc test analysis are shown in Supplementary Table 4.
The MusiQoL scores and previous DMT intake (yes/no).
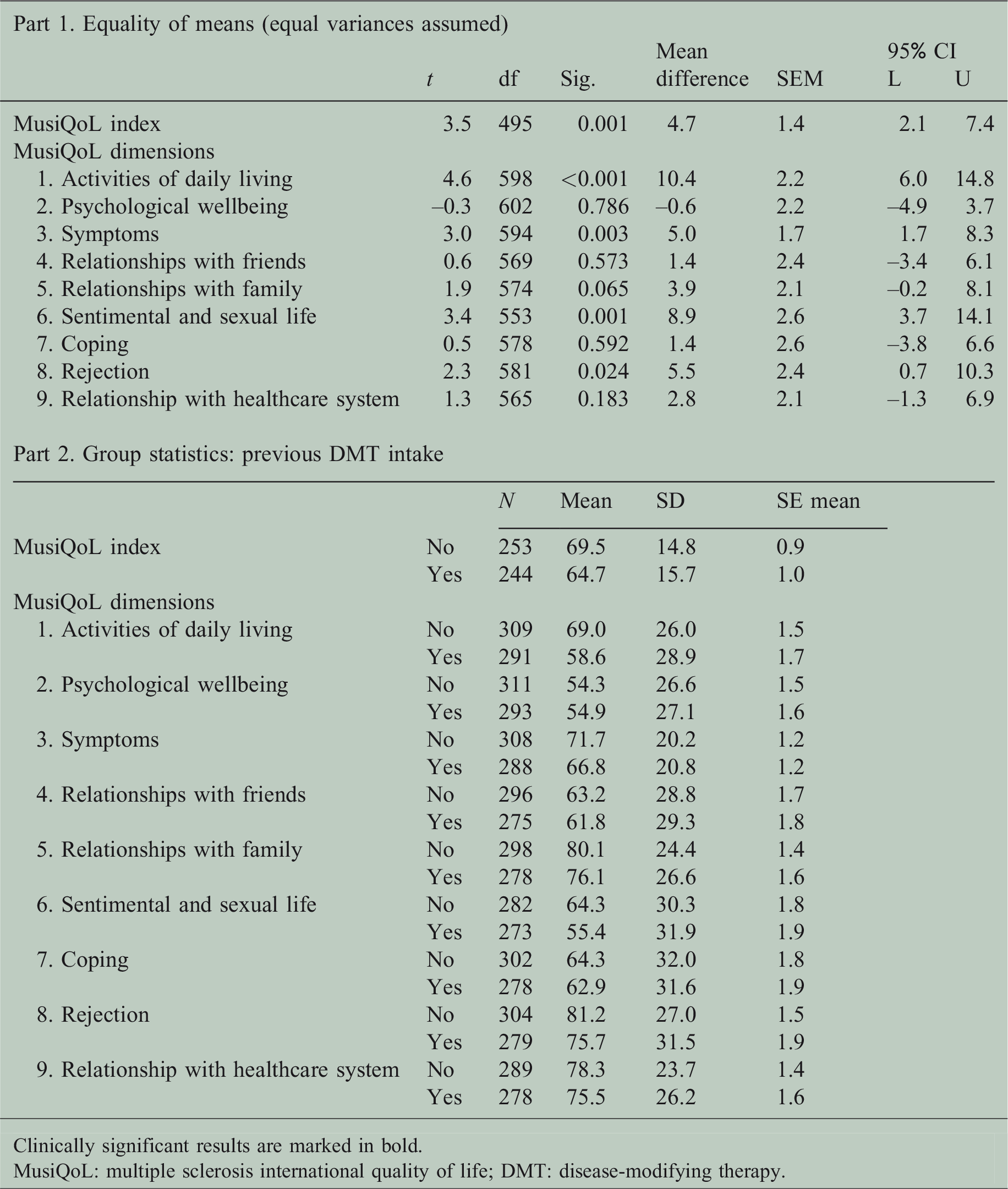
Clinically significant results are marked in bold.
MusiQoL: multiple sclerosis international quality of life; DMT: disease-modifying therapy.
All MFIS subscales were negatively associated with the MusiQoL index. Physical fatigue showed the most robust relationship when compared to cognitive and psychosocial fatigue. ‘Activities of daily living’ was significantly correlated with physical, cognitive, and psychosocial fatigue. Other dimensions showing similar results include ‘psychological wellbeing’, ‘symptoms’, and ‘rejection’. The ‘coping’ dimension was associated only with physical and psychosocial fatigue (Supplementary Table 2).
Predictors of health-related QoL in MS
Multiple regression analysis was run for each dependent variable, the MusiQoL index and seven of its dimensions, yielding eight models in total. The analysis was not performed on the dimensions ‘relationships with friends’ and ‘relationships with family’ because these were not significantly associated with any variable. The models’ summaries (including entered variables and results) are shown in Table 4. All tested regression models were found to be statistically significant.
Summary of the multiple variables’ regression models.

β coefficients of each variable within the regression models are reported. Only variables with reported β have been entered into the concerned model.
*Significance at 0.05 level (two-tailed).
**Significance at 0.01 level (two-tailed).
Clinically significant results are marked in bold.
MusiQoL: Multiple sclerosis international Quality of Life; DMT: Disease-Modifying Therapy; MFIS: Modified Fatigue Impact Scale; IV: Independent Variable; DV: Dependent Variable
When examining the MusiQoL index, the variables entered into the model predicted 41.9% of the variance. However, only psychosocial fatigue was a significant predictor (β = –3.4, P = 0.007). A decrease in psychosocial fatigue was associated with an improvement in the MusiQoL index.
The dimension ‘activities of daily living’ varied by 52.2% with the predictors entered in the model. For every one unit decrease in the EDSS score and physical fatigue, this QoL dimension improved by 4.6 (P = 0.04) and 1.1 (P = 0.02) units respectively. The ‘psychological wellbeing’ dimension had 45.3% of its' variance explained by the variables entered. This dimension seems to be negatively affected by physical fatigue, but positively affected by male sex, as opposed to women, and with the ‘increase of previous DMT count’. The ‘symptoms’ dimension was largely associated with cognitive fatigue. For every one unit decrease in cognitive fatigue, there was a 1.4 improvement in MS symptom-related QoL (P < 0.001). Within the ‘coping’ dimension, higher EDSS and less psychosocial fatigue were found to be significant predictors of more coping. Finally, when exploring the ‘relationship with the healthcare system’ dimension, current DMT intake was associated with a 12.3 (P < 0.001) increase in this QoL dimension as opposed to no intake. Although the models about ‘sentimental and sexual life’ and ‘rejection’ were significant, none had significant predictor coefficients.
MusiQoL and MFIS psychometric properties
The reliability coefficients of the MusiQoL index score and MFIS were 0.9 and 0.96 and ranged between 0.71 and 0.94, and between 0.89 and 0.95 for its' dimensions respectively. The two instruments showed excellent internal consistency properties (Supplementary Table 5).
The CFA results and chi-square values were statistically significant for both questionnaires. RMSEA values were 0.06 (MusiQoL) and 0.09 (MFIS). SRMR values were 0.06 (MusiQoL) and 0.07 (MFIS). The CFI was above 0.9 in both models, and the NNFI was above 0.9 for the MusiQoL and borderline (0.8986) for the MFIS. The CFAs showed data fitting the hypothesised measurement models which suggest good psychometric validity (Supplementary Table 5).
Discussion
The findings of this study suggest one more time that health-related QoL in MS patients is multifactorial. In addition, we showed for the first time in an Arab country that certain sociodemographic and clinical variables seem to affect particular QoL dimensions more than others. For instance, physical fatigue was associated with worse QoL, as well as several dimensions such as ‘rejection’. Moreover, this fatigue form affected ‘activities of daily living’ and ‘psychological wellbeing’ dimensions only. Our results from Lebanon are in line with the literature from developed countries and the MENA areas.52,53
The MusiQoL index was associated with various sociodemographic, clinical and fatigue factors. Taken together, these findings are comparable to those of several previous studies.5–8,10 However, psychosocial fatigue was the only significant predictor of how the overall health-related QoL varied in MS patients. The importance of psychosocial factors in MS was previously highlighted. 11 This is particularly relevant to Lebanon whereby its social structure is mainly collectivistic, 54 and social support is one of the primary ways by which individuals cope with stressful events. 55 One pilot study conducted on Lebanese MS patients showed that received social support had a positive association with the MusiQoL index, and with five of its' dimensions including ‘psychological wellbeing’ and ‘coping’. 56 Other studies in MENA also highlight the importance of social support in MS.10,57 The absence of associations between psychosocial fatigue and the MusiQoL dimensions ‘relationships with friends’ and ‘relationships with family’ could be due to the difference in the type of information captured by these two MusiQoL factors and the fatigue subscale. The MusiQoL asks about ‘talking, feeling understood, and feeling encouraged’, whereas the MFIS psychosocial fatigue dimension focuses on motivation to participate in social activities and limitation of ability to perform certain activities away from home.
Further research is needed to understand better the relationship between psychosocial fatigue and the QoL in MS. We recommend adding more items to the MusiQoL scale to encompass additional psychosocial aspects beyond the relationship with family and friends. These cumulative findings encourage examining these constructs in more detail to open new avenues within the therapeutic context of MS patients and ultimately improve their QoL.
Another finding worthy of further investigation is the significantly worse impact of MS on women’s ‘psychological wellbeing’ and ‘coping’ QoL dimensions albeit with similar disease duration and EDSS levels as male participants, This is not the first study to report such differences in QoL perception between the sexes. 58
The three fatigue forms evaluated in this study were associated with most QoL aspects and predicted variance in several dimensions. This is similar to findings on fatigue in MS reported in developed countries by Pittion-Vouyovitch et al. (2006), also concurrent with findings within the MENA region.10,32,34,35,59 Fatigue remains one of the most disabling MS symptom awaiting more effective therapeutic interventions.
Higher EDSS was associated with poorer MusiQoL index; it also predicted worse ‘activities of daily living’ and ‘coping’; similar to previous findings.8,31,32,35,36,60–62 Developing interventions to improve the QoL coping dimension in MS patients with higher EDSS is necessary, with particular relevance to women in our sample.
This study has several strengths including the large sample size utilised and the validity analyses performed. It is the first study in the MENA region which validated the MusiQoL and encourages the instrument’s adaptation into other countries. However, the literature search was limited to manuscripts in the English language, and some studies did not have full text available. Additional discriminant measures and test–retest reliability analysis should be performed to understand the questionnaires’ properties further. Although predictors were examined, causal inferences cannot be made given the study cross-sectional nature. Finally, the impact of modifiable lifestyle factors and depression on QoL was not explored.
Both measures explored in this study could enhance clinical practice outcomes when integrated into healthcare. Characterising MS health-related QoL and a better understanding of its different dimensions will facilitate the devise of targeted care plans.
Supplemental Material
MSO848467 Supplemental Material - Supplemental material for Factors affecting MS patients’ health-related quality of life and measurement challenges in Lebanon and the MENA region
Supplemental material, MSO848467 Supplemental Material for Factors affecting MS patients’ health-related quality of life and measurement challenges in Lebanon and the MENA region by Natali Farran, Batoul R Safieddine, Mariam Bayram, Tracy Abi Hanna, Joelle Massouh, Mona AlKhawaja, Hani Tamim and Hala Darwish in Multiple Sclerosis Journal—Experimental, Translational and Clinical
Footnotes
Conflict of Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from the Nehme and Therese Tohme MS Center at the American University of Beirut Medical Center.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.