
Abstract
Background
Optical coherence tomography (OCT) provides quantitative measures of retinal layer thickness. Cigarette smoking is a risk factor for multiple sclerosis (MS) onset and disease severity: its effects on OCT metrics have not been assessed.
Objective
The objective of this study was to assess the effect of smoking history on retinal nerve fiber layer (RNFL) and ganglion cell-inner plexiform (GCIP) of MS patients by OCT.
Methods
112 MS patients were recruited from the Brigham and Women’s Hospital. Spectralis OCT scans were acquired to measure GCIP, peripapillary RNFL, and total macular volume. Multivariable linear mixed effects regression model assessed RNFL and GCIP change with fixed effects for smoking history while adjusting for optic neuritis eye status, age, disease duration, sex, baseline EDSS, and disease modifying therapies (DMTs).
Results
Smoking histories were available for 102 patients: 46 (45.10%) had a history of smoking cigarettes and 56 (54.90%) never smoked. No statistically significant differences were found between ever-smokers and never-smokers with respect to GCIP, RNFL, and macular volume.
Conclusion
Our study shows no significant difference in retinal thickness between ever-smokers and never-smokers. If confirmed, this result suggests mechanistic differences between the retina and other central nervous system (CNS) compartments in response to smoking and should be noted when considering OCT as a surrogate measure of CNS activity.
Keywords
Introduction
Among the recognized environmental risk factors for multiple sclerosis (MS), the most evidence has been acquired for low vitamin D levels, low of exposure to ultraviolet light, Epstein–Barr virus, and, importantly, cigarette smoking.1,2 As the incidence of MS rose consistently during the 20th century, cigarette smoking became a widespread habit in the general population in Europe and North America. Since the 1960s, epidemiological studies identified cigarette smoking as a risk factor for MS. Smoking has been associated with a dose dependent increased susceptibility to MS and, to a lesser extent, with the risk of conversion from clinically isolated syndrome (CIS) to clinically definite MS, and with an increased susceptibility to secondary progressive MS conversion.3–8 MS patients who smoke also seem to be predisposed to faster rates of disability accrual, as shown by higher Expanded Disability Status Scale (EDSS) scores.3,5,9–11
The impact of smoking in MS patients has also been assessed through imaging studies: on magnetic resonance imaging, smokers show greater lesion volumes, higher brain T2 lesion loads, and more severe brain atrophy than non-smokers.4,5 Spectral-domain optical coherence tomography (OCT) measurement of the retina yields high resolution imaging and quantification of the peripapillary retinal nerve fiber layer (RNFL) and segmented macular layers. RNFL and ganglion cell-inner plexiform layer (GCIP) have been used as outcome measures in a wide variety of studies: both appear to correlate with visual function and global disability (EDSS). In particular, GCIP appears to correlate with brain T2 lesion load, brain atrophy and EDSS-measured disability progression, rendering it a more robust measure than RNFL as it is less prone to artifacts and in the acute setting is less affected by post-optic neuritis associated swelling. The correlation between brain and retinal atrophy seems to result from a pathology of anterior visual pathway: while retrograde neurodegeneration results in GCIP thinning, anterograde neurodegeneration results in brain atrophy.12–16 Pathology studies have shown that anterior visual pathway damage is common among MS patients and therefore, it is a good hallmark of overall MS-related neurodegeneration. 17
We utilized OCT in an attempt to examine the impact of cigarette smoking on retinal measures in MS patients. To better characterize our population, we stratified out patients according to their smoking history (ever-smokers vs. never-smokers).
Materials and methods
Subjects
Subjects enrolled in the Comprehensive Longitudinal Investigation of Multiple Sclerosis at the Brigham and Women’s Hospital (CLIMB) who also met the further inclusion criteria for this cross-sectional analysis: (1) enrolled in the longitudinal OCT subgroup, (2) were over the age of 18, and (3) met the 2010 McDonald diagnostic criteria for MS or CIS. As part of the demographic survey, patients provided both basic personal data such as gender, date of birth, optic neuritis (ON) history, and smoking history categorized as being never-smokers or ever-smokers. When providing ON history, each patient was asked to include the dates of past ON event and the laterality of each ON episode (bilateral, left, right). Healthy control (HC) subjects were also included and provided basic demographic data. All the data was then stored on the internal relational database of the CLIMB study. Exclusion criteria for MS and HC subjects included previous history of ophthalmological disorders, e.g., clinically-significant cataracts, glaucoma, diabetes and/or diabetic retinopathy, macular degeneration, and retinal detachment; refractive errors exceeding ±6 diopters; history of immunological and/or neurological disorders such as neuromyelitis optica, systemic lupus erythematosus, asthma, autoimmune thyroiditis, and rheumatoid arthritis. Additionally, we excluded from the study all MS patients with an acute use of steroids or acute ON within three months of OCT scans. Ten MS patients were excluded from the primary analysis due to their unknown status for smoking history.
All MS patients underwent standardized clinical exams performed by a neurologist, and OCT scanning. HCs also underwent visual acuity testing, and OCT scanning. Visual acuity was assessed for one eye at a time while the non-tested fellow eye was covered by the patient. The score of each chart was based on the number of letters correctly identified, which ranged from 0 to 60. Each patient was examined under reproducible conditions: the distance from the chart, the lighting of the room, and the test instructions were standardized. Also, all study participants provided written informed consent for their participation and the Partners Human Research Committee provided Institutional Review Board (IRB) approval.
Optical coherence tomography
Retinal imaging was performed by trained examiners using Spectralis OCT (software version 6.0.9.0, Heidelberg Engineering, Heidelberg, Germany). Peripapillary RNFL and macular volume scans were obtained from both eyes of each participant (without dilation), with automated segmentation providing measures of the GCIP. Scans were obtained using high resolution and automatic real-time tracking for B-scan averaging to enhance quality and were subsequently manually inspected to corroborate accurate fixation and centering.
Statistical analysis
We compared the demographic and clinical characteristics between ever-smoker and never-smoker MS patients at the baseline OCT exam. The continuous variables were described by mean and standard deviation (SD), while the categorical variables were described by counts and percentages. Means were compared with either a two-sample t-test or a Mann–Whitney U test for non-normal data, while proportions were compared with either a chi-square test or Fisher’s exact test for contingency tables.
We then compared RNFL and GCIP measurements between MS patients and HC. Since both eyes of each subject were included in this analysis, linear mixed models with unstructured correlation structures were used to adjust for the within-subject correlation. Multivariable linear mixed effects regression model assessed differences in RNFL and GCIP measurements with fixed effects for MS versus HC while adjusting for ON eye status, age, and sex.
We assessed the relationship of RNFL and GCIP measurements between ever-smokers and never-smokers using mixed linear regression models. Multivariable linear mixed effects regression model with unstructured correlation structures assessed differences in RNFL and GCIP measurements with fixed effects for smoking history while adjusting for ON eye status, age, disease duration, sex, baseline EDSS, and disease modifying therapies (DMTs). All statistical analyses were performed using SAS version 9.4 (Statistical Analytical System, SAS Institute).
Results
Demographics
Out of 112 MS patients, 102 had information available on cigarette smoking. 46 (45.10%) were ever-smokers and 56 (54.90%) were never-smokers. Table 1 displays demographic and baseline clinical characteristics of MS patients grouped according to their smoking status. Ever-smoker patients had longer disease duration at visit (17 vs. 12 years, p = 0.0038) and higher EDSS at visit (3 vs. 2, p = 0.0017) than never-smokers. There was no statistically significant difference in terms of their age at the baseline visit (48 vs. 45, p = 0.1540) or in their history of ON (54% vs. 43%, p = 0.2478).
Demographics characteristics between ever-smokers versus never-smokers MS patients.

MS = multiple sclerosis; OCT = optic coherence tomography; EDSS = Expanded Disability Status Scale; CIS = clinically isolated syndrome; SD = standard deviation.
Means were compared with a two-sample t-test.
Proportions were compared via a chi-square test for contingency tables.
Proportions were compared via a Fisher’s exact test for contingency tables.
Rank scores were compared via the Mann–Whitney U test.
MS and healthy controls
57 HC and 112 MS patients were included in our preliminary analysis which focused on comparing the two groups in RNFL and GCIP measures. Supplementary table 1 shows their baseline demographic and clinical characteristics. HC were younger (38 y.o. vs. 46 y.o., p < 0.0001) and more racially diverse (p < 0.0001) compared to MS patients.
As expected, MS patients had lower retinal thickness compared to HC. MS patients had lower total macular volume compared to HC (HC: 1.94 mm3 vs. MS: 1.77 mm3, β = 0.11, p = 0.0106), lower GCIP inner ring thickness (HC: 93.36 µm vs. MS: .26 µm, β = 11.81, p < 0.0001), and thinner GCIP outcomes across all individual quadrants (Table 2). HC had greater mean global RNFL (99.62 µm vs. 85.99 µm, β = 12.14, p < 0.0001) and greater RNFL papillomacular bundle (PMB) thickness (58.16 µm vs. 48.19 µm, β = 8.40, p = 0.0015) compared to MS patients (Table 3).
Association of GCIP measurements between MS patients versus healthy controls.
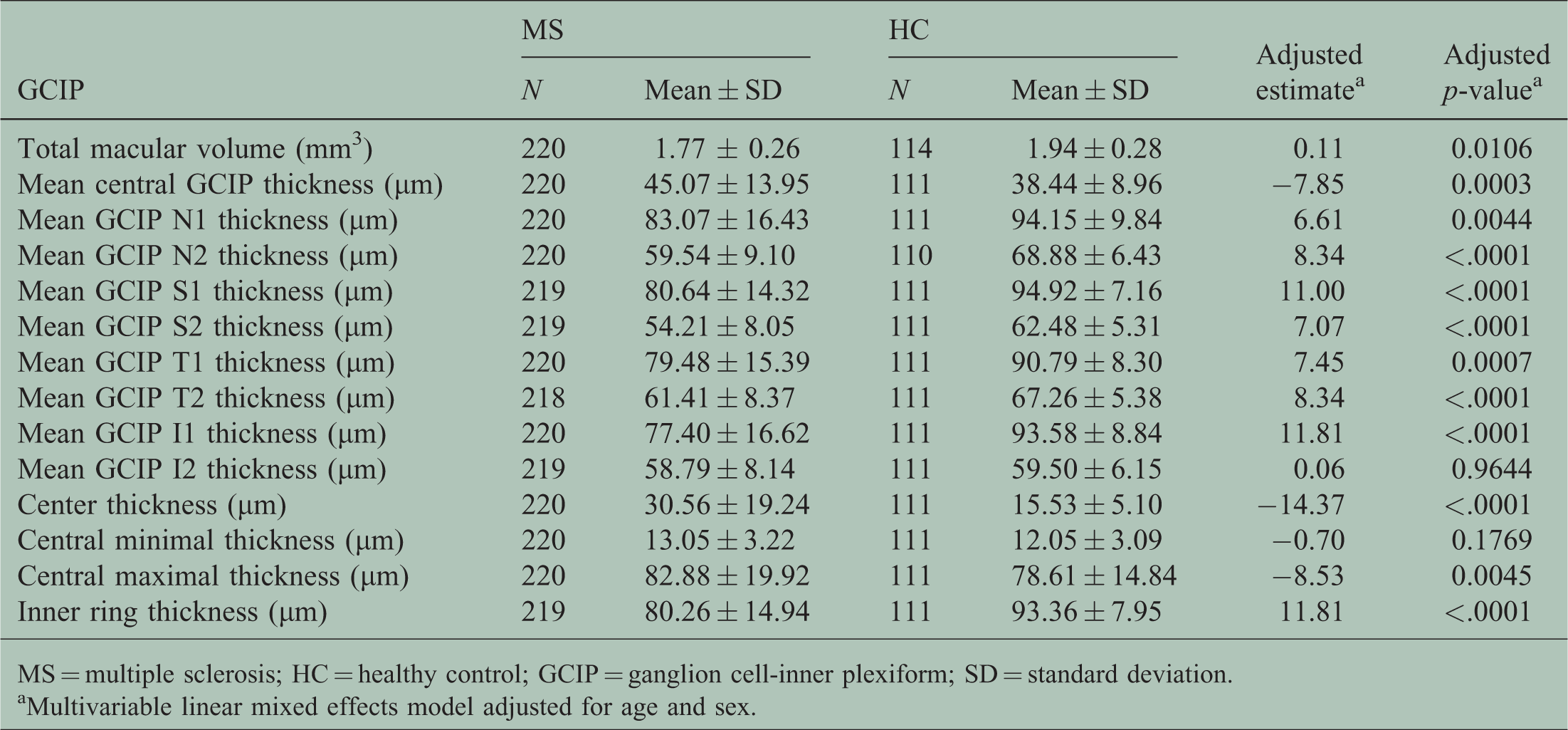
MS = multiple sclerosis; HC = healthy control; GCIP = ganglion cell-inner plexiform; SD = standard deviation.
Multivariable linear mixed effects model adjusted for age and sex.
Association of RNFL measurements between MS patients versus healthy control.

MS = multiple sclerosis; HC = healthy control; RNFL = retinal nerve fiber layer; PMB = papillomacular bundle thickness; SD = standard deviation.
Multivariable linear mixed effects model adjusted for age and sex.
Relationship of smoking history to GCIP and RNFL
We tested the association of GCIP and RNFL measurements between ever-smokers versus never-smokers MS patients, including nine RNFL and fourteen GCIP sectors (Tables 4 and 5). We failed to find any significant effect on GCIP metrics or RNFL measurements between ever-smokers versus never-smokers MS patients after adjusting for ON eye status, age, disease duration, sex, baseline EDSS and DMTs. The distribution in GCIP total macular volume, GCIP inner ring thickness, RNFL mean global, and RNFL PMB between ever-smokers and never-smokers are shown in Figure 1.

Comparing RNFL and GCIP distributions between the ever-smokers versus never-smokers showing the median, mean (unfilled diamond shape), and interquartile range. (a) Comparing GCIP total macular volume between ever-smokers (N = 45) vs. never-smokers (N = 60). (b) Comparing GCIP inner ring thickness between ever-smokers (N = 44) vs. never-smokers (N = 60). (c) Comparing RNFL mean global thickness between ever-smokers (N = 40) vs. never-smokers (N = 49). (d) Comparing RNFL mean thickness PMB between ever-smokers (N = 41) vs. never-smokers (N = 53).
Association of GCIP measurements between ever-smokers versus never-smokers MS patients.
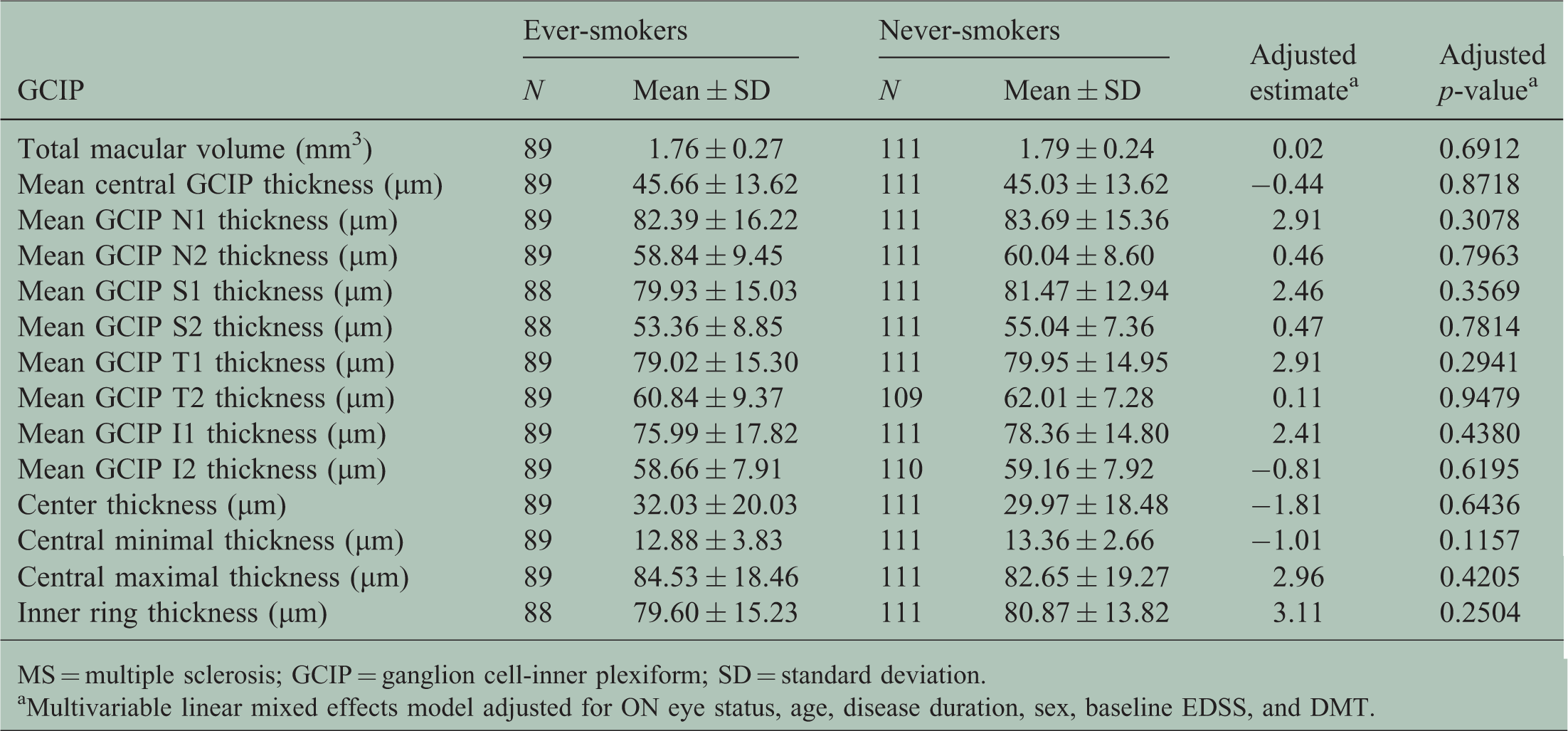
MS = multiple sclerosis; GCIP = ganglion cell-inner plexiform; SD = standard deviation.
Multivariable linear mixed effects model adjusted for ON eye status, age, disease duration, sex, baseline EDSS, and DMT.
Association of RNFL measurements between ever-smokers versus never-smokers MS patients.

MS = multiple sclerosis; RNFL = retinal nerve fiber layer; PMB = papillomacular bundle thickness; SD = standard deviation.
Multivariable linear mixed effects model adjusted for ON eye status, age, disease duration, sex, baseline EDSS, and DMT.
Discussion
In this cross-sectional study, our aim was to determine whether or not a history of cigarette smoking was associated with retinal damage quantified by RNFL, GCIP, and macular volume measures. We hypothesized that patients who had an ever-smoker history would have significantly thinned retina layers compared to patients who were never-smokers. Our results showed no significant differences in the thickness of retinal layers between ever-smoker and never-smoker MS patients.
While cigarette smoking has been consistently associated with MS, the exact mechanism of cigarette smoking toxicity has not been fully understood. The composition of cigarette smoke is complex, comprising more than 7000 chemicals, including nicotine and its derivatives along with a large number of compounds that form the cigarette smoke condensate. 18 According to both experimental and epidemiological studies, it is the smoke condensate rather than nicotine that is responsible for the major toxic effects on MS patients.19,20 Some of these toxic compounds can directly damage axons (e.g. nitric oxide) and compounds that trigger demyelination (e.g. cyanates). 21 Also, cigarette smoke has been implicated in the activation of lung macrophages, which may incite the proinflammatory cascade of MS.20,22,23 Further, microglial activation in the central nervous system (CNS) has also been suggested as an important hub in the process of demyelination. 19
We expected smoking to be detrimental to MS patients via either direct retinal toxicity or through proinflammatory activation of the immune system leading to a more active disease phenotype. In fact, smoking has been shown to have deleterious effects on both the retina and the optic nerve in the context of acute macular degeneration, tobacco–alcohol amblyopia, and Cuban epidemic optic neuropathy.24,25 Furthermore, retinal thinning in MS patients can be due to a direct damage of the optic nerve or to a more widespread process of brain atrophy resulting in trans-synaptic retinal thinning: both relapses and brain atrophy can be facilitated by cigarette smoking.4,15,26–30
To the best of our knowledge via review of available literature in PubMed, this study appears to be the first to address the association of cigarette ever-smokers versus never-smokers MS patients using OCT imaging. In previous studies of healthy individuals, the effects of cigarette smoking on retinal parameters have been inconsistent. While a few studies showed a decrease in RNFL and choroidal thickness in smokers, other studies have failed to replicate those findings.31–33 Cigarette smoking has been shown to play a role in increasing RNFL thinning in migraine patients. 34 In contrast, our study showed no effect of smoking on RNFL thinning in MS patients.
The strengths of our study were a large patient population, the presence of smokers and non-smokers, and controlling for history of ON. The main limitations of our study were the cross-sectional design, the lack of more quantitative data on smoking history (e.g. pack-year history), the absence of a control population of smokers and non-smokers, and the division between ever-smokers and never-smokers (i.e. not considering the distinction between past and active smokers). In regard to quantitative smoking data, previous studies showed that cigarette smoking becomes a relevant factor past a given dose threshold. By the same token, quitting can reverse at least some of the negative effects of smoking: the date of quitting is likely to be informative.11,35 Therefore, a precise smoking history and pack-year values may be integral to an optimal analysis of the impact of cigarette smoking.
In conclusion, this study suggests that cigarette smoking history may not have an impact on retinal deterioration in MS. The question is likely more complex than currently appreciated. Therefore, longitudinal studies will be crucial to identify how retinal structures and other sites in the CNS are selectively affected by cigarette smoking. Our study suggests that compartments within the CNS respond differentially to neurodegenerative stressors, and that this factor should be accounted for when considering interventional studies using surrogate markers such as retinal measures for neurodegeneration in MS.
Supplemental Material
Supplemental material for Cross-sectional study of smoking exposure: no differential effect on OCT metrics in a cohort of MS patients
Supplemental Material for Cross-sectional study of smoking exposure: no differential effect on OCT metrics in a cohort of MS patients by Mattia Rosso, Dorlan J Kimbrough, Cindy T Gonzalez, Bonnie I Glanz, Brian C Healy, Maria Assunta Rocca, Massimo Filippi, Howard Weiner and Tanuja Chitnis in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Conflict of Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The CLIMB study is supported in part by grants from the Nancy Davis Foundation without walls and Merck-Serono.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.