
Abstract
Background
It has been suggested that switching ability might not be affected in multiple sclerosis (MS) as previously thought; however, whether this is true under more ‘real-world’ conditions when asymmetry in task difficulty is present has not been ascertained.
Objective
The objective of this paper is to examine the impact of task difficulty asymmetry on task switching ability in MS.
Method
An ocular motor (OM) paradigm that interleaves the simple task of looking towards a target (prosaccade, PS) with the cognitively more difficult task of looking away from a target (antisaccade, PS) was used. Two switching conditions: (1) PS switch cost, switching to a simple task from a difficult task (PS switch), relative to performing two simple tasks concurrently (PS repeat); (2) AS switch cost, switching to a difficult task from a simple task (AS switch) relative to performing two difficult tasks concurrently (AS repeat). Forty-five relapsing–remitting MS patients and 30 control individuals were compared.
Results
Controls and patients produced a similar magnitude PS switch cost, suggesting that task difficulty asymmetry does not detrimentally impact MS patients when transitioning from a more difficult task to a simpler task. However, MS patients alone found switching from the simpler PS trial to the more difficult AS trial easier (shorter latency and reduced error) than performing two AS trials consecutively (AS switch benefit). Further, MS patients performed significantly more errors than controls when required to repeat the same trial consecutively.
Conclusion
MS patients appear to find the maintenance of task-relevant processes difficult not switching per se, with deficits exacerbated under increased attentional demands.
Introduction
Multiple sclerosis (MS) is a chronic inflammatory disease of the central nervous system characterised by recurrent, episodic neurological attacks and progressive degeneration. Patients may present with a plethora of symptoms consequential of the disseminated nature of the disease, with cognitive deficits now widely recognised as a primary symptom, affecting 45%–65% of patients. Although a range of cognitive deficits may occur, impairments of executive functions, information processing speed, attention, working memory and inhibitory control are commonly reported.1,2
Although cognitive deficits in MS may be reminiscent of variable and distributed damage to the networks underpinning these functions, evidence has highlighted the central role of networks involved with the prefrontal cortex (PFC) in executive deficits.3–6 The PFC is considered a key association area that helps mediate the integration and coordination of endogenous and exogenous processes, to allow the facilitation of context-appropriate and adaptive behaviour.7,8 Changes within the networks associated with these functions have been demonstrated in MS,3–6 leading to the suggestion that the specific assessment of PFC function may provide a useful way to assess cognitive changes in executive function in MS patients. 9
Experimentally, the assessment of processes associated with flexible and adaptive behaviour may occur through task-switching paradigms. 10 Fundamentally, these paradigms require a participant to respond in one of two ways depending on the type of stimulus presented, creating two different types of tasks. Trials prompting these different tasks are typically interleaved pseudo-randomly, with successive trials either requiring the repetition of the same task (repeat trials), or requiring a change from one task to another (switch trials). Generally, performance is poorer for switch trials compared to repeat trials (switch cost), with a larger switch cost considered indicative of poorer task-switching ability.10,11
Until quite recently, there has been a paucity of research investigating these important processes in MS, with deficits largely inferred from neuropsychological measures that implicate multiple cognitive domains; this necessarily confounds the measurement of task-switching deficits. However, a recently published paper by Migliore et al. 9 investigated task switching in MS using a specifically designed cued-switching paradigm, a classic methodology that allows the explicit measurement of switch cost. This study demonstrated that, when switching between two tasks of relatively equal difficulty, MS patients demonstrated poorer switching than controls when preparation time (cue-target interval) and inter-trial duration was short (150 ms respectively); when intervals where elongated to 1800 ms no significant differences in switch cost were evident. This suggests that processes involved in task switching might not be affected in MS as previously reported, instead poorer performance by MS patients are merely a consequence of changes in processing speed, a common finding for other executive tasks.12,13 Although this research represents an important first step in understanding the nature of task switching in MS, the homogeneity in the difficulty of the tasks used does not reflect the conditions experienced in the real world, with tasks usually varying in terms of their cognitive demands. Task-difficulty asymmetry is known to alter the switch-cost relationship, by placing different constraints on processes underlying task switching depending on whether the switch is made from a more difficult task to a simpler task or vice versa.11,14,15 As such it would be of interest to determine whether imposing a difference in task difficulty will differentially affect MS patients relative to controls.
Usually, when a large asymmetry in task difficulty is imposed the classic switching relationship (switch trial > repeat trials) is altered, with a reliable switch cost evident only when transitioning from a cognitively more demanding task (non-dominant) to a more well-learned, simpler task (dominant).11,16,17 Although several different theories attempt to explain this phenomenon, the influential task set inertia theory contends that the execution of a non-dominant response requires the inhibition of the dominant task set, with this inhibition proposed to persist inertially into the next trial. Therefore, when a switch is made from a more difficult, non-dominant response to a simpler dominant response, a behavioural cost is incurred (switch cost). Conversely, there is less need to inhibit a non-dominant response during the performance of a dominant response, producing little or no behavioural cost when switching from dominant to a non-dominant response.11,18
To investigate the impact of task difficulty asymmetry on task switching in MS, an ocular motor (OM) task-switching paradigm was used that interleaved the simpler, dominant response of looking towards a suddenly appearing peripheral stimulus (prosaccade: PS) and the more cognitively difficult, non-dominant response of looking away from a peripheral stimulus (antisaccade: AS). Two switching conditions were investigated: (1) switching to a simple task from a difficult task (AS-PS: PS switch), relative to performing two simple tasks concurrently (PS-PS: PS repeat); (2) switching to a difficult task from a simple task (PS-AS: AS switch) relative to performing two difficult tasks concurrently (AS-AS: AS repeat). An OM design was chosen for two reasons: (1) the prosaccade/antisaccade dichotomy represents an extreme example of task asymmetry, with a PS considered easier because of the relative automaticity of its occurrence, and (2) OM assessments have been shown to provide refined elucidation of deficits in MS, compared to more conventional assessment techniques.19,20 Further, given the findings of the study by Migliore et al., 9 preparation time and inter-trial periods were protracted to minimize the potential impact of processing speed on MS performance. It was expected that, because of the increased requirements introduced by the task asymmetry, MS patients would be more profoundly impacted by this task than controls.
Method
Participants
Forty-five patients with relapsing–remitting multiple sclerosis (RRMS) were recruited through the outpatient clinic at the Royal Melbourne Hospital, or private practice. At the time of testing, no patient was experiencing exacerbated symptomology, as determined by clinical assessment. All patients maintained their prescribed medication regimen throughout the study.
Thirty healthy control participants, without a history of neurological or psychiatric illness, were recruited from the community. One control participant was excluded from the study due to insufficient analysable eye movement data, a consequence of excessive blinking (86% of trials excluded).
Participant groups were comparable for age and estimated intelligence as determined by the National Adult Reading Test (NART). 21 MS patients reported significantly higher depressive symptomology as determined by the Beck Depression Inventory (BDI: F(1, 73) = 8.95, p = 0.004); 22 however, no patient was identified as suffering from clinically relevant depressive symptoms according to the cut-off score of 18.5, as previously determined for MS populations. 23 MS patients also completed the Modified Fatigue Impact Scale (MFIS). 24 No patient was found to be experiencing significant fatigue (>38 total score).24,25 BDI score and MFIS score were not found to be related to performance on the OM task-switching paradigm. Consequently, neither was not used as a covariates (Table 1).
Descriptive information for healthy controls and multiple sclerosis (MS) patients.
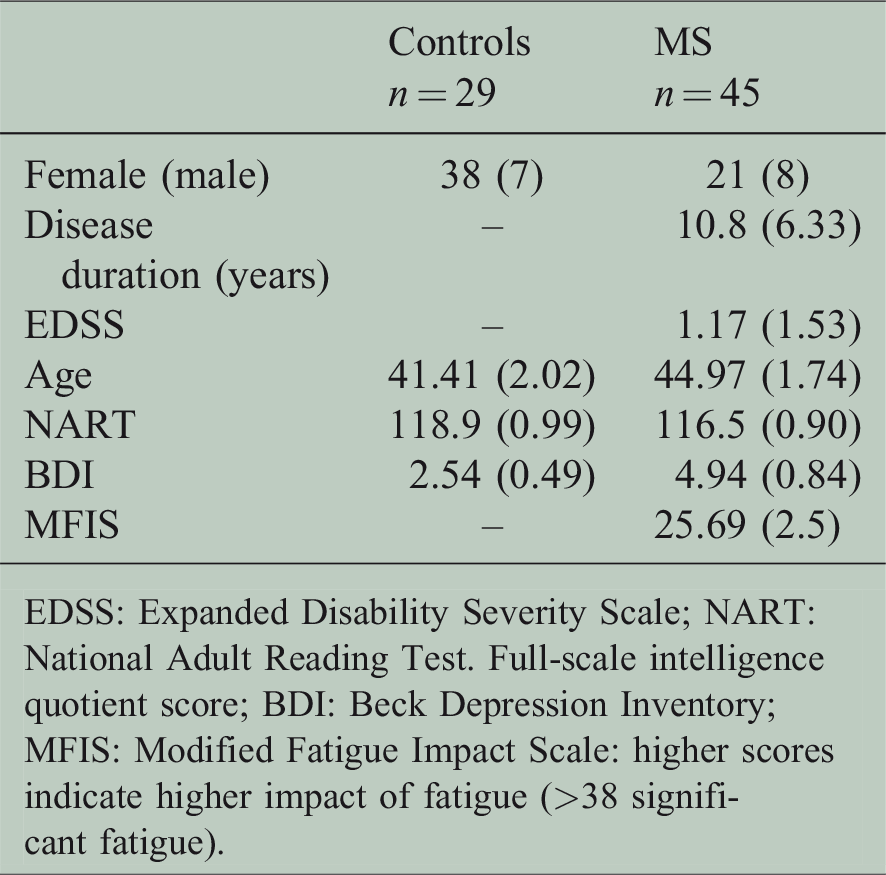
EDSS: Expanded Disability Severity Scale; NART: National Adult Reading Test. Full-scale intelligence quotient score; BDI: Beck Depression Inventory; MFIS: Modified Fatigue Impact Scale: higher scores indicate higher impact of fatigue (>38 significant fatigue).
All participants were screened to exclude substance abuse/dependence, and gave their informed consent prior to inclusion in the study in accordance with the Declaration of Helsinki. Testing occurred at the Royal Melbourne Hospital and ethics approval was granted by the Melbourne Health Human Research Ethics Committee (2007.094).
OM apparatus and protocol
Horizontal displacement of both eyes (saccades) was recorded using an Eyelink II dark pupil, video-oculography system. This system has high resolution (noise limited at <0.01 degrees) and an acquisition rate of 500 Hz.
Participants were seated in a darkened room, 840 mm in front of a 75 Hz cathode ray tube monitor (resolution: 1024 × 768). Task stimuli were presented on a black background and comprised green, blue and purple crosses (1.5-degree visual angle). Blue and purple crosses appeared centrally, whilst green crosses appeared either 5 degrees or 10 degrees right or left of centre.
At the start of every trial, all participants fixated on a central cross for 1000, 1250 or 1500 ms (presentation randomised to reduce anticipatory responding). A green cross then appeared in one of the four peripheral locations for 1500 ms, concomitant with the disappearance of the central cross.
The colour of the central cross (blue or purple) indicated how a participant was to respond to the appearance of the peripheral green cross. A blue cross indicated that the participant should look at the green target cross (PS trial), whilst a purple cross indicated that the participant should look to the mirror opposite position to the green target cross (AS trial). A central fixation square was used to reorient gaze centrally in preparation for the next trial (Figure 1).
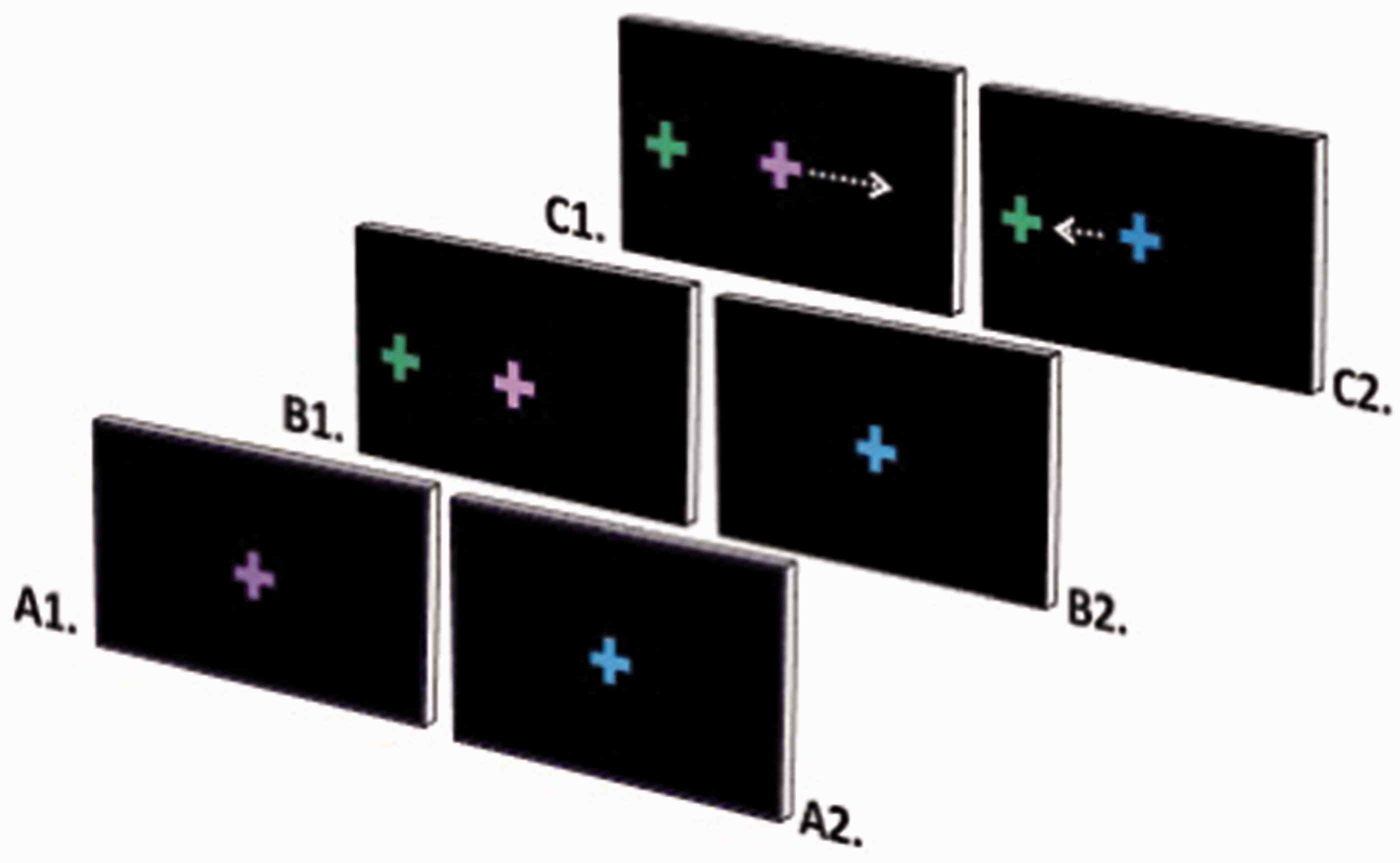
Ocular motor switch task. (a) Participants fixate on a central cross which is either a (A1) purple cross, which indicates an antisaccade trial, or a (A2) blue cross, which indicates a prosaccade trial. (B1 and 2) A peripheral green target cross appears. (C1) Participants perform an eye movement to the mirror opposite position to the green cross (antisaccade). (C2) Participants perform an eye movement to the green cross (prosaccade).
All participants were familiarised with the task by way of a guided example of each trial type, followed by a practice block of 12 trials (six AS trials, six PS trials). Three test blocks were completed each consisting of 32 PS trials and 32 AS trials presented in a pseudo-random order (APAAPAPP). Trials were classified as a repeat trial in which two consecutive trials required the same response (i.e. PP: PS repeat; AA: AS repeat), and a switch trial in which a different response was required on two consecutive trials (AP: PS switch; PA: AS switch). Across the three test blocks 48 PS and 48 AS trials were presented with approximately even numbers of switch and repeat trials. The first trial of every block was excluded from switch/repeat trial analyses since they represented neither a switch nor repeat trial.
Neuropsychological tests
The Paced Auditory Serial Addition Test (PASAT: three-second interval) 26 and Symbol Digit Modalities Test (SDMT verbal) 27 were administered to all participants according to standardised instructions.
Data analysis
Eye movement analysis was performed offline using a custom, in-house Matlab program. Saccade latency (ms) was calculated from a monocular eye trace, as the temporal difference between target (blue or purple cross) onset and saccade onset. Saccade onset/offset was determined using a velocity criterion of 30 degrees per second. For switch trials, only trials not preceded by an error were included, with evidence suggesting that an effect of switching occurs only when the previous trial is correct. 28
Errors were calculated as a proportion of total trials and defined as a PS performed during an AS trial or vice versa. Trials were removed from the analysis of latency during which (1) an error was performed, (2) fixation was not maintained within two degrees of the central target, (3) a blink occurred around trial onset that was thought to interfere with saccade onset, or (4) no response was made within the trial period. Independent of task-relevant errors, approximately 1.7% of trials were removed from analysis for MS patients, and approximately 0.43% trials were removed for control participants.
To investigate the effect of task-difficulty asymmetry, two switching conditions were investigated: (1) PS switch cost, switching to a simple task from a difficult task (AS-PS: PS switch), relative to performing two simple tasks concurrently (PS-PS: PS repeat), and (2) AS switch cost, switching to a difficult task from a simple task (PS-AS: AS switch) relative to performing two difficult tasks concurrently (AS-AS: AS repeat). To achieve this, error rate and latency for each condition were submitted to a two (group: controls, MS) by two (trial type: PS, AS) by two (transition type: repeat trials, switch trials) repeated-measures analysis of variance (ANOVA). Post hoc analyses were performed using paired-samples t test or Wilcoxon signed rank tests where violations to normality were found. Pearson’s correlations were performed to investigate relationships between neuropsychological test performance and task-switching variables, with Spearman’s used where violations to normality were found. Group differences in neuropsychological test performance were assessed by one-way ANOVAs.
Results
Descriptive results for the OM switch task and neuropsychological tests can be found in Table 2.
Mean and standard error for ocular motor switch task variables and neuropsychological test performance.
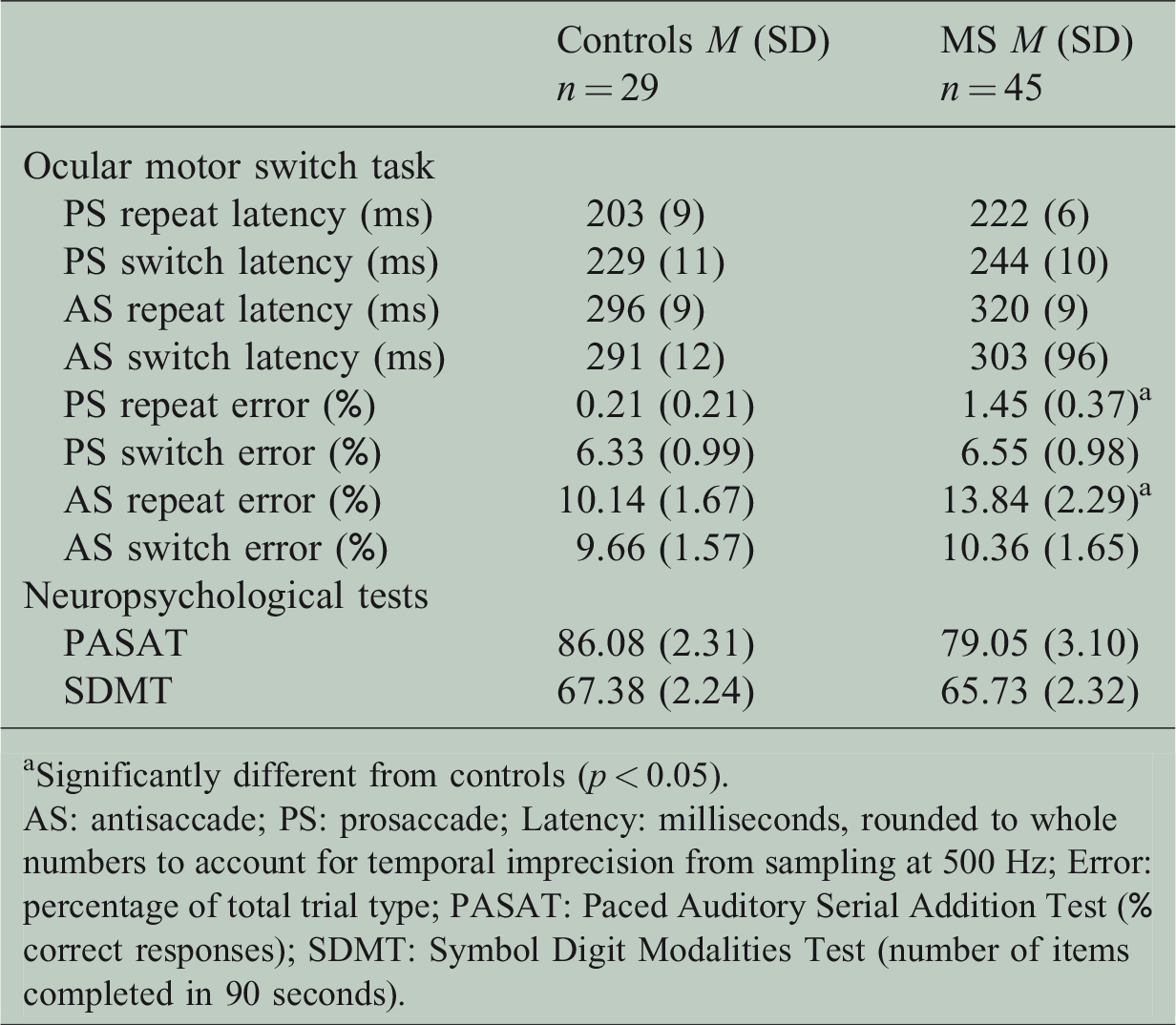
Significantly different from controls (p < 0.05).
AS: antisaccade; PS: prosaccade; Latency: milliseconds, rounded to whole numbers to account for temporal imprecision from sampling at 500 Hz; Error: percentage of total trial type; PASAT: Paced Auditory Serial Addition Test (% correct responses); SDMT: Symbol Digit Modalities Test (number of items completed in 90 seconds).
For PS trials, latencies were significantly shorter than AS trials (main effect: F(1, 71) = 251.32, p < 0.001, ηp2 = 0.78), and produced significantly fewer errors (main effect: F(1, 72) = 33.92, p < 0.001, ηp2 = 0.32); no effect of group by trial was found. Similarly, latencies for repeat trials were significantly shorter than switch trials (main effect: F(1, 71) = 7.23, p = 0.009, ηp2 = 0.092); no effect of group by transition was found.
A differential effect when switching from an AS to a PS (PS switch) compared to when switching from a PS to an AS (AS switch) was found for latency (main effect: F(1,71) = 37.68, p < 0.001, ηp2 = 0.35) and error (main effect: F(1, 72) = 36.12, p < 0.001, ηp2 = 0.33). Specifically, post hoc analyses revealed that controls and MS patients demonstrated a significant cost of switching for PS trials, with performance on PS switch trials significantly poorer than PS repeat trials: latency (controls: z = –4.64, p < 0.001, r = 0.61; MS: z = –3.16, p < 0.001, r = 0.33) and error (controls: z = –3.91, p < 0.001, r = 0.51; MS: z = –4.58, p < 0.001, r = 0.68). However, for controls, AS trials had comparable latencies irrespective of transition type (switch or repeat): unidirectional switch cost. In contrast, MS patients performed AS switch trials with significantly shorter latencies than AS repeat trials (AS latency switch benefit: t(44) = 2.97, p < 0.005, d = 0.21), and made significantly more errors on AS repeat trials than AS switch trials (AS error switch benefit: z = –2.533, p = 0.011, r = 0.38).
For controls, no relationships were evident between any OM task-switching variable and neuropsychological test performance. However, for MS patients, poorer SDMT performance was related to a larger AS switch benefit (error only: r = 0.35, p = 0.022), and poorer PASAT and SDMT performance was related to higher AS repeat trial error rate (PASAT: r = –0.43, p = 0.006; SDMT: r = –0.46, p = 0.002), AS switch latency (PASAT: r = –0.46, p = 0.003; SDMT: r = –0.59, p = 0.000) and repeat trial latency (PASAT: r = –0.42, p = 0.007; SDMT: r = –0.53, p = 0.000). Longer PS switch trial latency was related to poorer PASAT performance only (PASAT: r = –0.42, p = 0.006). No relationship between Expanded Disability Severity Scale score and any OM task-switching variable was found. Further, no group differences in neuropsychological performance were found.
Discussion
The ability to flexibly adapt behaviour to accommodate changes in situational demands is fundamental to successful interaction within an environment. In line with the impact of the extreme asymmetry between AS and PS trials on switching, control participants exhibited a unidirectional switch cost for PS; poorer performance (increased latencies and errors) when switching from a cognitively more difficult AS trial to a PS trial (PS switch), relative to performing two simpler PS trials concurrently (PS switch cost), whilst no difference in performance when switching from a PS to an AS (AS switch) relative to performing two AS trials concurrently (AS repeat). MS patients similarly demonstrated a significant PS switch cost (latency and errors), which was not found to be significantly larger than controls. Further, no significant group differences in latency for any trial type were found, suggesting that the timing of this task did not adversely affect MS patients. Overall, these results indicate that task asymmetry does not negatively impact switching in MS patients when transitioning from a more difficult task to a simpler task.
Unexpectedly, and in contrast to previous studies that have used a similar paradigm,16,17 MS patients alone demonstrated an AS switch benefit, whereby switching from the simpler PS trial to the more difficult AS trial was easier (shorter latency and reduced error) than performing two AS trials consecutively; a larger AS switch benefit was related to poorer SDMT performance (error only). Further, MS patients performed significantly more errors than controls when required to repeat the same trial consecutively (PS and AS repeat trials), with the performance of errors on AS repeat trials related to poorer SDMT and PASAT performance.
Although an AS switch benefit has been reported in previous studies that interleaved PS and AS responses,29–31 these studies included an atypical AS design whereby two static, equidistant, peripheral targets were used instead of the classic single, dynamic target, as was used in this study. Static targets remove the need to inhibit the prepotent response elicited by the appearance of a peripheral target, as well as reducing the requirement to approximate spatial location; this effectively reduces the difficulty of AS trials and the degree of asymmetry with PS trials. When these factors have been introduced, such as in this study, only a unidirectional cost of switching has been reported.16,17 Consequently, the theoretical explanation given in these studies do not explain the pattern of results found in this study, with the current results suggesting that MS patients may have deficits in task set maintenance rather than in switching per se.
Generally, switching from one task to another relies upon accurate and persistent task-set representations of each of the required responses, as well as inhibitory control required to prevent the execution of an erroneous task set. The PFC has been proposed to be pivotal to task switching, facilitating the maintenance of task sets within persistent neural firing loops (task-set maintenance) and the generation of flexible stimulus-response (S-R) mappings that can direct processing within parietal and motor areas (e.g. superior colliculus, the premotor command centre for eye movements). 32 Consequently, the integrity of task-set maintenance directly mediates the effectiveness of the S-R maps to direct behaviour. 33 Attention is known to be pivotal to the maintenance of task set, with disruption to attentional processes shown to affect the integrity of maintained information and thus the resultant S-R maps. 34 This relationship is directly affected by the degree of asymmetry between the previous and current task set that is currently being maintained, producing distinct differences in the resultant response. 28
Specifically, engagement in attentionally demanding tasks can increase inhibition of responses to simpler, more dominant tasks, whilst facilitating responses to more cognitively demanding, non-dominant tasks, producing reduced latencies.34,35 In line with this, Cherkasova et al. 30 demonstrated that individuals with poorer sustained attention produce larger latency AS switch benefit. Potentially, for individuals with poorer attentional control, completion of a correct AS switch trial requires increased devotion of attentional resources due to the added cognitive demands, resulting in increased facilitation (reduced latency) of the response. MS patients frequently report poorer maintenance of attentional set and allocation of attentional resources, 2 potentially explaining why a significant AS latency switch benefit was produced for MS patients alone.
Similarly, the AS switch benefit for error in MS may also be consequential of changes in attentional control. Generally, an AS error is explained as a failure to inhibit the dominant PS response, a consequence of the integrity of task-set maintenance and the resultant ability to bias the competition between saccade and fixation neurons in the superior colliculus (the premotor command centre for saccade generation). 36 However, for task-switching paradigms, errors for each AS trial type (AS repeat, AS switch) are conceivably a consequence of a different balance of constraints, with an AS repeat error a failure to maintain the AS task set from the previous trial, and a AS switch error involving a failure to successfully switch to a new task set.
MS patients performed more errors on AS repeat trials than AS switch trials (switch benefit), suggesting that maintaining the AS task set was significantly more difficult than transitioning to the AS task set. This difficulty in task-set maintenance would also account for the higher proportion of errors performed by MS patients on both AS and PS repeat trials compared to controls (no group difference in switch trial error rate), demonstrating that irrespective of whether the task set represents a simpler or more difficult response, maintenance is affected in MS patients. Further support for this assertion comes from the finding that a larger AS error switch benefit and higher erroneous responding on AS repeat trials were related to poorer performance on the SDMT (switch benefit) and PASAT (repeat trial errors).
Overall, it appears that MS patients have difficulty maintaining task set generally, a potential consequence of attentional dysfunction, which is exacerbated under conditions during which increased recruitment of attentional resources is required. These results are particularly salient given the absence of significant group differences in latency across all task measures, suggesting that processing speed is not the factor underlying the results. This is in contradiction to the current notion that executive deficits in MS are simply the consequence of changes in basic information processing speed rather than deficits in distinct executive processes.12,13 Potentially, an underlying deficit in basic attentional processes may be central to executive dysfunction in MS, with attentional proficiency integral to cognitive processing generally. 8 Further investigation of this idea is required.
Footnotes
Acknowledgements
We would like to thank all participants who gave up their time to contribute to this study.
Conflicts of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Meaghan Clough, Paige Foletta, Dr Anne-Marie Tearnes, Ashley N. Frohman and Derek Sears have nothing to declare. Dr Owen B. White reports grants from Bayer, Australia, during the conduct of the study, personal fees from Bayer, Australia, grants from Biogen, grants and personal fees from Novartis, and personal fees from Genzyme, outside the submitted work. Dr Joanne Fielding reports grants from Bayer, Australia, during the conduct of the study, and grants from Biogen and Novartis, outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.