
Abstract
Introduction
Epilepsy is a common neurological disorder that affects 50–70 million people worldwide. In India, it is estimated that there are nearly 7.5 million people with epilepsy. 1
The term idiopathic generalized epilepsies (IGE) may be imprecise as many monogenic or complex inheritance patterns are being recognized in their causation. 2 Over the years, it has been increasingly recognized that epilepsy can be associated with cognitive dysfunction, poor academic performance, and deranged social function. These have been collectively considered to be the neurobehavioral comorbidities of epilepsy. Executive function encompasses the cognitive skills necessary for goal-directed and intricate tasks, which include all domains involving forward thinking, formulating plans, recollecting short-term memory, initiating/inhibiting, monitoring and organizing everyday life. 3 Executive functions are essentially high-level cognitive functions, mediated primarily by the dorso-lateral prefrontal cortex (DLPFC). Patients with structural abnormalities of the neuraxis could be logically expected to have executive dysfunction. Surprisingly, these dysfunctions have also been reported among patients of epilepsy with normal neuroimaging studies and premorbid intelligence.
It has been recognized that cognitive problems often coexist from the onset of epilepsy in 40%–60% of patients. There are many factors that can lead to cognitive impairment in epilepsy, such as (a) seizures occurring during sprouts of cognitive development, (b) frequent epileptiform discharges in a interictal EEG, and (c) pharmacological treatment for epilepsy (especially polypharmacy). 4 It is postulated that cognitive impairment in epilepsy results from a stable irreversible structural changes, symptomatic epilepsy, and treatment-related dysfunction.
Systematic studies on the neuropsychological effects of IGE on executive functioning are lacking in an Indian context. Hence, this study was performed to know the impact of IGE on executive functions in adults using a validated Indian battery. Abnormalities if any help us in holistic management of patients of IGE.
Materials and Methods
Subjects
This was an observational cross-sectional Hospital-based study. All patients of IGE syndrome of generalized tonic clonic type and who were willing to participate in the study were recruited after an informed consent.
Inclusion criteria
Age >18 years. Normal MRI on epilepsy protocol. Baseline standard progressive matrices (SPM) score more than or equal to 25th percentile.
Exclusion criteria
Significant structural lesions detected in imaging. History of dementia/psychosis. History of alcohol and drug abuse.
Detailed history about the epilepsy, medications used, and other details were collected and recorded in a structured pro forma. For the purpose of analysis, we empirically considered patients who were seizure-free for 6 months prior to the study as having controlled seizures and those with recurrence as suffering from uncontrolled seizures. All patients were subjected to MRI brain (epilepsy protocol) and an interictal EEG recording. The tests used to assess executive functions were color trial (focused attention), digit vigilance test (sustained attention), verbal fluency and category fluency test (for word and idea generation), verbal n-back test (for working memory), Tower of London test (for planning and organization), and Stroop test (for inhibition). All the above-mentioned tests were taken from the NIMHANS neuropsychology battery, which was based on Indian population. We used the normative data of this battery for comparison in our subjects during statistical analysis. 5
Statistical Analysis
All the statistical methods were done using SPSS 21.0 version for windows. Statistics was done by means of proportions for categorical/binary variables and mean, median, standard deviation, and interquartile range (IQR) for continuous variables. Inferential statistics was done by using the chi-square test/Fisher’s exact test, y, and z. P < .05 was considered statistically significant. Chi-square test and Fisher’s exact test are used to compare two or more independent proportions. Fisher’s exact test is used when the number of expected numbers in >25% cells is <5.
Results
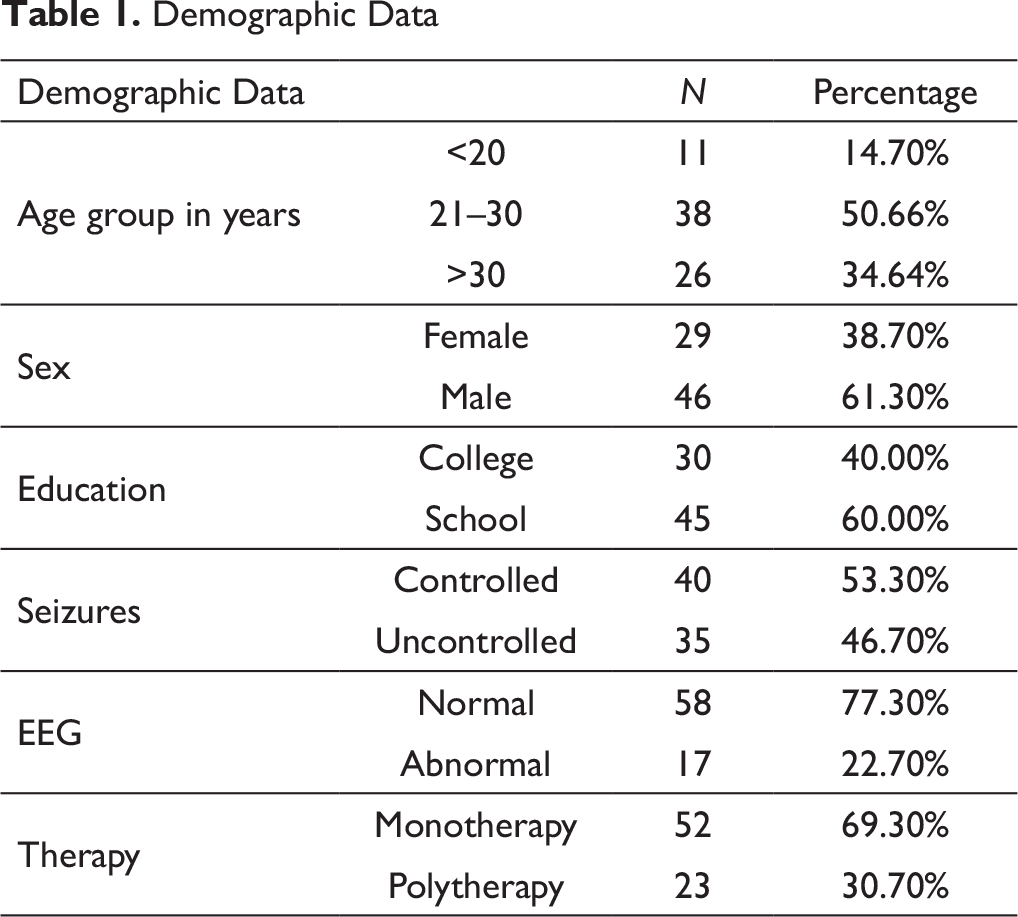
We recruited a total of 75 patients, out of which 46 (61.3%) were males and 29 (38.7%) were females. The mean age of study population was 28 ± 7.2 years. The mean age at seizure onset was 22 ± 7 years. Approximately 50% of the population were between 21 and 30 years of age. Demographic profile is depicted in Table 1.
Family history of seizures was seen in 8 (10.7%) of the study population. Approximately 53.3% of the patients had controlled seizures compared to 46.7% of uncontrolled seizure. EEG was abnormal in 17 (22.7%) subjects (e/o generalized spike/spike wave discharges—suggestive of primary generalized epilepsy) and normal in 58 (77.3%). A total of 52 (69.3%) patients were on monotherapy compared to 23 (30.7%) on polytherapy.
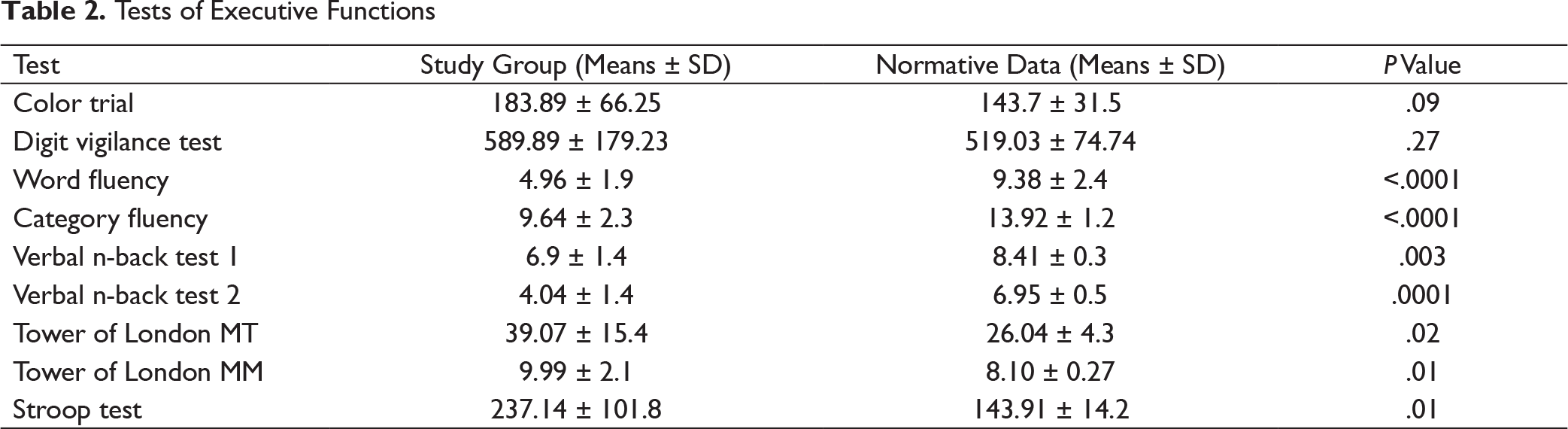
The mean of the values for the executive tests obtained from our study data was compared with the normative data published for NIMHANS executive tests battery. The results of the battery of various executive tests are summarized in Table 2.
Demographic Data
Tests of Executive Functions
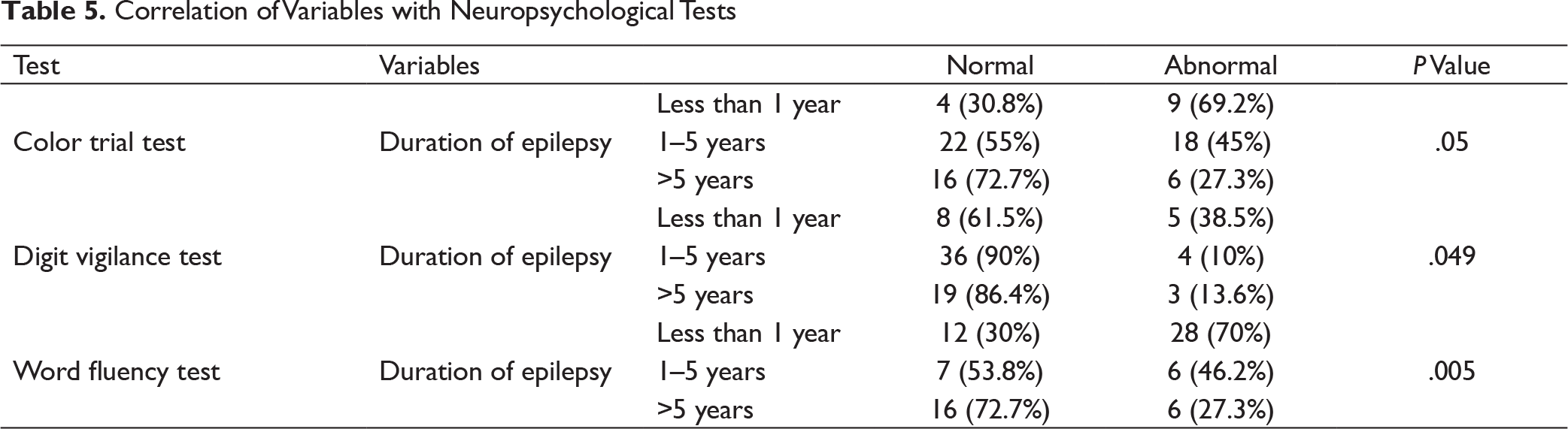
Correlation of Variables with Neuropsychological Tests

It showed statistically significant impairment in word fluency, category fluency, verbal n-back, Tower of London, and Stroop test among our subjects.
Abnormalities in the various domains of executive functions were analyzed among variables such as age of onset, education, duration of epilepsy, and in patients with controlled and uncontrolled epilepsy. As shown in the charts below that some of the variables were abnormal and statistically significant in these subgroups.
Statistically significant abnormality was observed in verbal n-back test 2 and Tower of London test among subjects less than 30 years of age as compared to patients more than 30 years of age with P value of .05 and .02, respectively (Table 3).
Color trial test was abnormal in 18 of college-qualified population (n = 30) vs 15 of school-qualified population (n = 45) which was significant (P = .02). Stroop test was more likely to be abnormal among school-qualified patients (n = 33, P = .04) (Table 4).
Correlation of Variables with Neuropsychological Tests

Correlation of Variables with Neuropsychological Tests
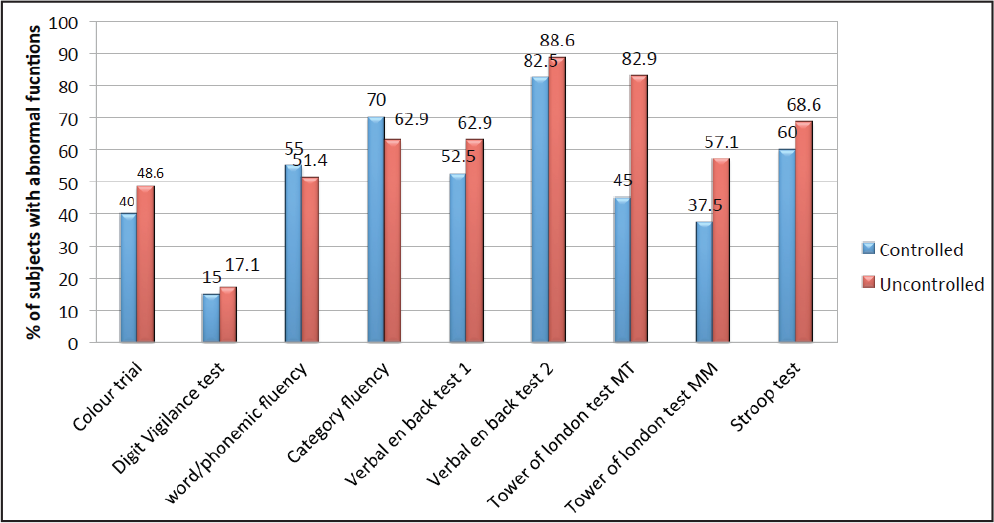
Comparison of Neuropsychological Tests Between Controlled and Uncontrolled Groups
Among patients of seizures of less than 1-year duration, color trial test was significantly abnormal (P = .05). Similar observations were made in digit vigilance test (P = .04) and word fluency test (P = .005) (Table 5).
Tower of London test was abnormal in 29 (83%) subjects with uncontrolled seizures compared to 18 (45%) subjects with controlled seizures that was statistically significant (P < .001). However, there were no statistically significant differences in color trial test, digit vigilance test, word fluency, category fluency, verbal n-back, and Stroop test (Figure 1).
Discussion
Executive functions of brain include cognitive activities that help in decision making, planning, awareness, and insight, which are especially useful in daily routine for full functioning of a person. Possible insult to the brain during seizures may cause dysfunction of brain activities including executive functions and may lead to a poor quality of life.
In our study, an extensive neuropsychological executive function evaluation was done using Indian standard battery (NIMHANS battery of tests).
The mean age of study population with seizures was 28 years with standard deviation of 7.2 years. The mean age at seizure onset was 22 years with standard deviation of 7 years. These findings were in line with a study done by Shehata and Bateh 6 in which mean age of patients with IGE was 28.92 ± 8.70 years, while mean age at seizure onset was 20.19 ± 9.82 years.
Approximately 50% of the population were between 21 and 30 years of age and slightly male predominant (61% male) similar to other studies like Tian et al. (55% male) 7 and Kumar et al. (62% ). 8 Family history of seizures was seen in only 8 (10.7%) of the study population similar to other studies like Davidson et al. 9
EEG was abnormal in only 17 (22.7%) subjects. Most of our patients were on monotherapy (69.3%). In a study conducted by Kumar et al. 8 , 74% of patients were on monotherapy and 62% were on monotherapy in a study done by Turaga et al. 10
Category fluency (dominant temporal lobe), word fluency (left prefrontal cortex), verbal n-back test (left supplementary motor and premotor areas), Tower of London test (bilateral dorsal prefrontal cortex), and Stroop test (bilateral superior medial prefrontal regions) were impaired predominantly in our study population. Gelziniene et al. 11 in his study found executive dysfunction in verbal fluency, Stroop test, and trail making test in IGE patients, similar to our findings.
Color trial test was affected in college-qualified population when compared to school-qualified population, whereas executive dysfunction in Stroop test was affected in school-qualified population compared to college-qualified population.
Tower of London test and verbal n-back test were predominantly affected in patients with seizure onset at a younger age.
Color trial test, digit vigilance test, and word fluency tests were paradoxically affected in uncontrolled seizure population with seizure duration of less than 1 year compared to a seizure population with seizure duration of more than 1 year. This could be attributed to increased frequency of seizure attacks in population with seizure duration of less than 1 year, which was in line with a study conducted by Hoie et al., 12 who noted that poor executive functions were related to early epilepsy onset, high seizure frequency, and polytherapy.
Similar to our study, tests of executive function were impaired in studies by Turaga et al., Black et al., and Kim et al.10,13,14 However, these studies are not comparable with our study as they included different set of patients (Turaga et al. 10 —chronic mesial temporal lobe epilepsy, Black et al. 13 —temporal lobe epilepsy patients, and Kim et al. 14 —cognitive effects of certain antiepileptic medications).
Conclusion
Executive dysfunction was noted in IGE patients. Young age of seizure onset and increased frequency of seizures were found to have effect on attention, cognitive speed, fluency, and planning. Patients with uncontrolled epilepsy were more likely to have executive dysfunction. Executive dysfunction was noted predominantly in dominant frontal lobe, superior medial prefrontal, temporal lobe, and orbitofrontal areas. Hence, all patients with IGE should be screened for executive dysfunction, the presence of which should prompt the clinician to initiate cognitive retraining.
Author Contributions
Contributor 1: Conception and design of the work, data acquisition, analysis, and interpretation of data, manuscript preparation and editing.
Contributor 2: Conception and design of the work, data acquisition, analysis, and interpretation of data, manuscript preparation, editing and review
Contributor 3: Conception and design of the work, analysis, interpretation of data, manuscript preparation, editing and review.
Contributor 4: Conception and design of the work, data analysis, and interpretation of data, manuscript preparation, editing and review.
Contributor 5: Data acquisition, data analysis, and interpretation of data and manuscript preparation.
Contributor 6: Data acquisition, analysis, and interpretation of data, manuscript preparation.
Contributor 7: Data acquisition, analysis, and interpretation of data, manuscript preparation.
Footnotes
Declaration of Conflicting Interests
Ethical Statement
The authors state that subjects have given their written informed consent and that the study protocol was approved by the institute’s ethical committee ([JSSMC/2308/11 NCT /2019-20 (03/09/20)].
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ICMJE Statement
This manuscript has been edited in accordance to the guidelines of the International Committee of the Medical Journal Editors.