
Abstract
Background
Both prolonged-release fampridine (PRF) and enabling active motor training (EAMT) are beneficial in multiple sclerosis (MS) patients. Their combined effect is, however, understudied.
Objective
The objective of this paper is to determine if PRF augments the beneficial effect of EAMT in MS patients as opposed to placebo.
Method
This is a pilot, randomized, placebo-controlled, double-blind 14-week study. Participants were randomly assigned to receive PRF 10 mg BID (n = 21) or placebo (n = 20). All patients underwent EAMT during the first six weeks. Patients were assessed at –4, 0, 6 and 14 weeks.
Results
Both groups remained stable between –4 to 0 weeks and showed statistically significant improvements for the six-minute walk and the five-times-sit-to-stand test at weeks 6 and 14. The PRF-treated group achieved a greater mean percentage improvement and a higher incidence of responders in all three tasks at both time points. The study was, however, underpowered to reach statistical significance.
Conclusion
Our results confirm previous studies demonstrating that MS patients, despite significant disability, do benefit from a rehabilitation program. Our study is the first to show a trend suggesting that PRF in MS patients appears to enhance the benefit of EAMT. Further studies are required to confirm this.
Clinical trial registration number with Clinicaltrial.gov: NCT02146534
Introduction
Multiple sclerosis (MS) is the most common cause of non-traumatic neurological disability affecting young adults in North America. The disorder is characterized by a chronic progressive demyelination and axonal degeneration within the central nervous system, leading to a wide variety of cognitive and physical symptoms. While these symptoms vary greatly among MS patients, walking impairment and fatigue have been identified as two of the most common symptoms in MS. Clinical research has shown that exercise in MS patients can improve muscle strength, aerobic capacity, and fatigue. Some research suggests, though this is still debated, that exercise may also slow MS disease progression through its effect on stress hormones, the immune system1 and/or growth hormones. Neuroscience studies investigating the role of exercise in the white matter (WM) of healthy individuals reported an increase of WM fiber pathways after active training. 2 Similar results were obtained in MS patients, where a group undergoing motor training preserved their WM integrity in the corpus callosum, as opposed to the control group, which experienced a significant worsening in microstructural integrity. 3 Not all MS patients, however, appear to benefit from rehabilitation and the benefit can be short lived. Which exercise or rehabilitative program is best remains also an unresolved question. A recent review of rehabilitation strategies in MS has highlighted the paucity of well-designed studies evaluating the different approaches used in MS rehabilitation.
Fampridine (4-aminopyridine) is a pre-synaptic potassium channel blocker found to improve axonal conduction in demyelinated nerve fibers, as well as synaptic transmission and neuronal excitability, resulting in an enhancement of neurological functions in people with MS.4–7 In the past several years, multiple clinical trials confirmed the beneficial effects of fampridine on walking speed and distance in MS patients, with improvement in walking abilities ranging from 31% to 46%.8–13 Fampridine was also found to have long-lasting improvement on the quality of life of MS patients (e.g. relationship difficulties, fatigue, time perspective).14,15 Prolonged-release fampridine (PRF) 10 mg twice a day (BID) is now considered a standard treatment for MS patients experiencing walking difficulties. 10 However, less than 40% of MS patients will show measurable benefit from PRF.
NeuroGym has developed a rehabilitation program for MS patients known as enabled active motor training (EAMT). This approach (see Appendix 1) focuses on improving motor control, biomechanics and strength of movement, in addition to the expected improvement in conditioning that is associated with exercise. The training program includes elements of strength training, mobility, balance and control training that address the major deficits identified in the initial individual evaluation of each patient with a focus on mobility. The approach maximizes brain-muscle interaction by manipulating both environmental and physical resources.
At the neurophysiological level, in MS patients acquiring motor skills implies learning to compensate for lost neural connections. Pharmaceutical intervention that enhances neural communication such as PRF could potentially facilitate such a process. We hypothesized that combining PRF with EAMT could lead to greater improvement in motor function and in a greater percentage of MS patients than with EAMT alone.
The aim of the present study is to investigate in MS patients of all types with moderate disability the effect of a rehabilitation program as per the EAMT approach combined with PRF 10 mg BID or placebo.
Method
Study Design and Participants
The present study was reviewed and authorized by the Canadian Shield institutional review board. Consent was obtained from each patient. A sample of 41 patients diagnosed with MacDonald criteria (2010) MS were recruited for this pilot, single-center, double-blind, placebo-controlled, 14-week study. Patients were evaluated four weeks prior to randomization then at 0, 6, and 14 weeks post-randomization. The patients were randomized so half received PRF 10 mg BID, while the other half received a placebo. All patients met the prescribed criteria for PRF use as per product monograph, were clinically stable at entry and had an Expanded Disability Status Scale (EDSS) score between 3.5 and 7.0 with a pyramidal system functional assessment score of 2 or greater and the ability to complete all the assessments at baseline with or without aids. All the EDSS were performed by a single Neurostatus-trained neurologist. All patients underwent rehabilitation as per the NeuroGym EAMT approach, consisting of three sessions of one hour per week for a period of six weeks. The NeuroGym protocol (see Appendix 1) consists of a safe, physiotherapist-supervised training environment with an emphasis on repetition of enabled movement using biofeedback combined with a significant element of strengthening and biomechanics optimization. Movements necessary for walking are enabled despite significant disability with the help of specialized equipment such as the Bunger Mobility Trainer or the sit-to-stand (STS) apparatus. Biofeedback is attained using electromyography (EMG)-triggered video games. Walking balance is regained through controlled repetition of relearning exercises. This was followed by an eight-week observational period, during which patients kept taking their medication (PRF or placebo) and were encouraged to continue a training program at home.
Responders to treatment were defined as patients who displayed a 20% improvement from baseline in a specific task at a specific time point. Mean percentage improvement was measured for all patients within each of the two groups (placebo or PRF treated). Randomization was stratified according to EDSS to ensure a similar number of patients with EDSS of six or more in each group.
Outcome Measures
Timed 8-meter walk (T8MW)
The T8MW measures the time needed by a patient to walk eight meters, from the initiation of the instruction to reaching the eight-meter mark. Patients walked along a path clear of obstructions. Patients were instructed to walk as fast and safely as possible. The T8MW was performed twice and the average of the two trials was included in the analyses. A shorter time corresponds to a faster walking speed.
Six-minute walk (6MW)
The 6MW measures endurance during walking by assessing the number of meters a patient can walk during six minutes. Participants were instructed to walk as fast and safely as possible in a single 25-meter long corridor. A longer distance traveled reflects better walking endurance.
Five-times-sit-to-stand test (FTSTS)
The FTSTS measures lower body strength by assessing the time needed for a patient to stand up and sit five times from a chair. Patients start while sitting on a chair with armrests as they are allowed to use upper extremities to assist in raising themselves and the time needed to completely stand up and sit five times in a row is recorded. A shorter time corresponds to better lower limb muscle strength.
Statistical Analysis
In order to examine the scores of responders, a logistic regression was computed on the three outcome measures at six and 14 weeks. T-tests between groups were computed to examine group improvement over time per group and per task. Examination of the within- and between-group effect of active motor training was examined through a repeated multivariate analysis of variance (MANOVA) test.
Results
A summary of patients’ demographic information can be found in Table 1. Overall, no statistical difference was found between the two groups.
Descriptive.

EDSS: Expanded Disability Status Scale; MS: multiple sclerosis; SPMS: secondary progressive MS; PFR: prolonged-release fampridine; PPMS: primary progressive MS; RRMS: relapsing–remitting MS.
All randomized patients completed the study. All patients in both groups attended and completed the 18 sessions of EAMT. PRF adherence was excellent. One patient was considered non-compliant. Four patients were 80% to 90% compliant and the rest were more than 90% compliant. There was no serious adverse event. As shown in Tables 2 and 3, repeated MANOVAs were performed for each motor task at the four time points by groups. There was no significant change between time points –4 and 0, demonstrating the absence of a learning effect. As shown in Figure 1(a), results of the 6MW support a linear function within participants between time points (F(1, 39) = 19.272, p < 0.001). Examination of pairwise comparisons support a statistically significant constant improvement in 6MW mean time between all time points, with the exception of between weeks 6 and 14 (p = 0.86). Between-group effect was nonsignificant (F(1, 39) = 1.833, p = 0.184). As observed in Figure 1(b), a similar pattern was observed in FTSTS, with a significant cubic function within participants between time points (F(1, 39) = 14.175, p = 0.001). Examination of pairwise comparisons identified statistically significant differences between baseline and week 6 (p < 0.001) and week 14 (p < 0.001). These results were not significant between groups (F(1, 39) = 2.497, p = 0.122). No statistically significant effects of time points or groups were observed in the 8MW.
Repeated MANOVA.

6MW: Six-minute walk; FTSTS: Five time sit to stand; MANOVA: multivariate analysis of variance.

(a) Change in performance over the four time points on the six-minute walk (6MW) within the prolonged-release fampridine and control groups, with error bars at 95% confidence interval. (b) Change in performance over the four time points on the five-time-sit-to-stand test (FTSTS) within the prolonged-release fampridine and control group, with error bars at 95% confidence interval. (c) Change in performance over the four time points on the eight-meter walk (8MW) within the prolonged-release fampridine and control groups, with error bars at 95% confidence interval.
Mean and SD by time points.

6MW: Six-minute walk; FTSTS: five-times- sit-to-stand; PFR: prolonged-release fampridine; SD: standard deviation.
PRF responders’ information can be found in Table 5. The highest incidence of responders was at week 14 on the FTSTS, with half of the sample displaying a >20% improvement from baseline. One-third of the participants qualified as responders at week 6 on the FTSTS, and around one-quarter both at weeks 6 and 14 on the 6MW. Only a few participants responded to the T8MW at both time points. A higher incidence of responders was seen in the PRF-treated group for T8MW, 6MW, and FTSTS at six weeks (odds ratio (OR) of 1.059, 0.800, and 1.436, respectively) and at 14 weeks (OR of 2.222, 1.063, and 3.018, respectively).
Group improvement.
PFR: prolonged-release fampridine; SD: standard deviation.
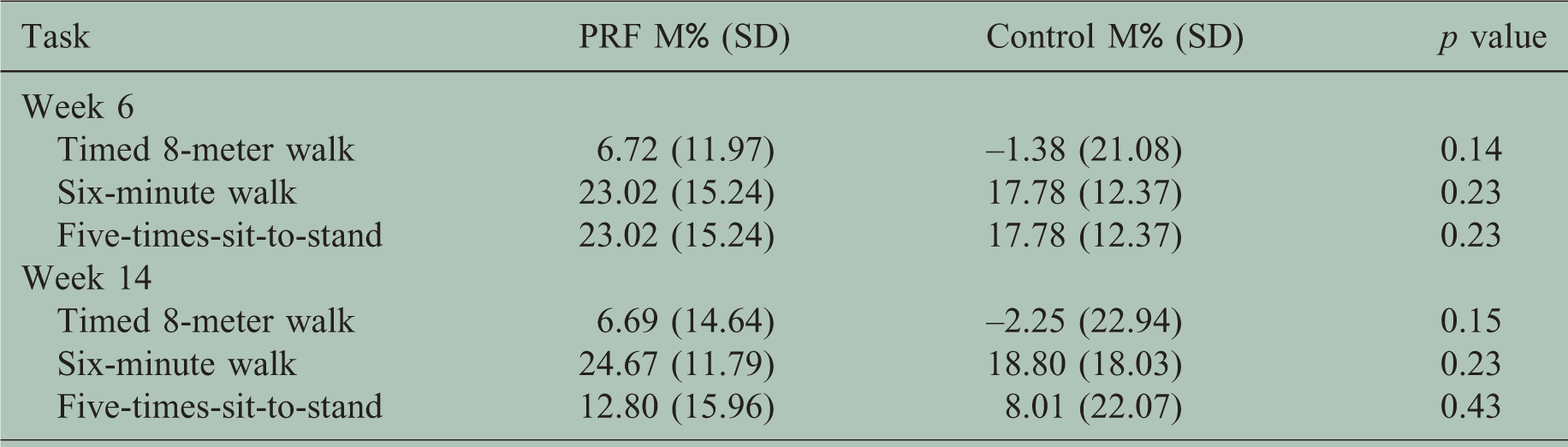
Group improvement from baseline measures can be found in Table 4. The PRF group displayed higher mean percentage improvement on all tasks at both time points (M% = 6.72 to 24.67). While the results of the control group are similar at both time points, albeit weaker, than the results of the PRF group on the 6MW and the FTSTS, controls performed worse over time on the T8MW. Despite a slight improvement at week 14, controls’ performances on the T8MW remained weaker than their initial performances at baseline.
Responders.
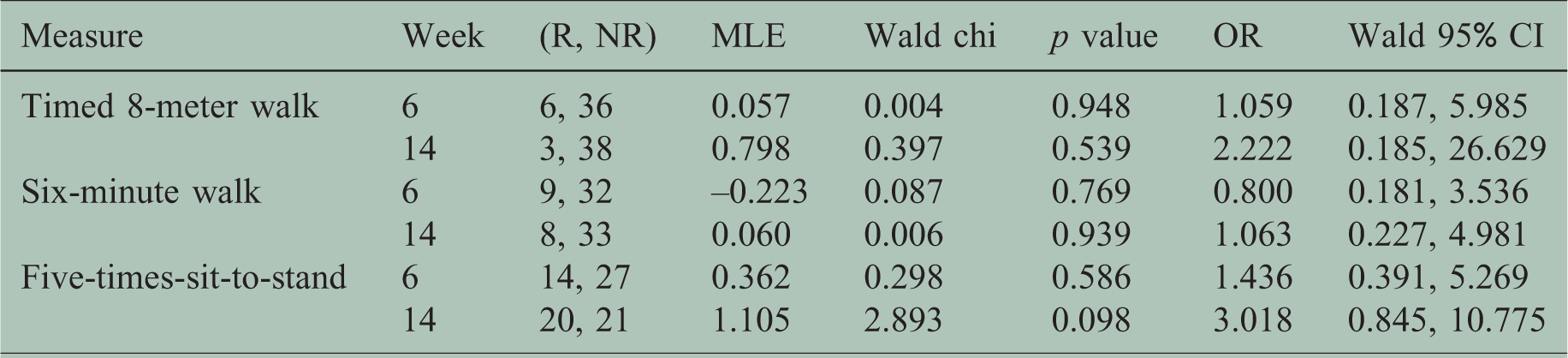
CI: confidence interval; MLE: maximum likelihood estimation; OR: odds ratio; R: response; NR: no-response.
Discussion
The beneficial effect of active motor training on its own has been shown in previous research. Our study similarly demonstrates the capacity of MS patients despite having significant preexisting disability (mean EDSS 4.7) to undergo a training program that resulted after only six weeks in significant motor improvement in the placebo group as shown by the 6MW (8% mean group improvement) and FTSTS (18.8% mean group improvement) but interestingly not for the T8MW. The NeuroGym EAMT program employed in our study provided training in many aspects of mobility but especially for standing (see Appendix 1), which we believe explains why the greatest improvement was noted in the FTSTS. The fact that the benefit was still present after an eight-week observational period testifies to the durability of the benefit.
Comparison of the PRF group to the placebo group demonstrates the benefits of PRF in addition to motor training, noting both a greater number of responders and greater group mean improvement at both time points. The lack of statistical significance can be attributed to our study being underpowered. The benefit was more marked in regards to gait and standing speed as measured by the T8MW and FTSTS and less with regards to endurance as measured by the 6MW. This could be explained by the PRF mechanism of action and/or the greater impact of the EAMT on the 6MW.
While the PRF group displayed consistent improvement in walking speed over time, the placebo group when compared to baseline actually performed slightly worse over time. A potential explanation for the lack of “improvement” in the T8MW is the nature of motor training combined with the requirement of the task. The NeuroGym EAMT program encouraged and resulted in mechanical changes in gait (e.g. focus on bending at the knee during stance and avoiding hyperextension)—such changes, though functionally very effective, can result in a different focus and in a temporary decrease in short distance gait speed.
A large number of patients qualified as responders in one or more of the three tests at weeks 6 and 14. While the number of responders was as expected higher at week 6 than at week 14 for the T8MW and the 6MW, the opposite was true for the FTSTS, with more patients qualifying as responders at week 14 than at week 6. Though our confidence intervals were large, this could suggest a more sustained improvement in lower extremity strength from the PRF-enhanced motor training and/or the result of improving other tested components of the FTSTS such as balance.
Limitations
Our study had several limitations, including but not limited to small sample size and relatively short duration. The question would have been better addressed with a study design that included a group of PRF alone and a group without either motor training or PRF. Though we stratified randomization according to EDSS, the placebo group had consistently poorer performances on all three measures including at weeks –4 and 0. Randomization stratification according to performance at the week –4 evaluations could perhaps have resulted in more balanced groups when it came to motor performance. Our confidence intervals were quite large and overlapped significantly, indicative of significant heterogeneity within groups, which is to be expected with inclusion of EDSS ranging from 3.5 to 7.0 inclusively. Perhaps with a greater study population we could have further divided the groups into EDSS less than 4 and greater than 4, resulting in more homogenous groups and tighter confidence intervals. Our repeated use of the study measures could have induced a learning effect throughout the study. However, closer examination shows that there did not seem to be any significant “learning” of the study measures when we look at changes in the results between the evaluations at weeks –4 and 0.
Conclusions
Though none of our between-group study endpoints reached statistical significance, all of our results trended toward a beneficial effect of combining PRF treatment with active motor training. These performance increases were present in patients with all types of MS, and were more noticeable compared to placebo at week 14. We believe that with greater statistical power our study would have confirmed an additive benefit of using PRF as an adjunct to motor training in MS patients both in degree and sustainability of the improvement.
Our results confirm previous studies demonstrating that MS patients, despite significant disability, do benefit from a rehabilitation program. Such benefit was sustained eight weeks later. Our study is the first to show a trend suggesting that PRF in MS patients appears to enhance the benefit of EAMT. Further studies are required to confirm this.
Footnotes
Acknowledgement
This study was presented during a poster session at the conference of American Academy of Neurology, 2015.
Conflict of Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr F. Jacques received compensation from pharmaceuticals Merck Serono, Biogen, Sanofi Genzyme, Teva Marion and Novartis for giving presentations and his participation in ad boards. He has received unrestricted grants from Biogen, Merck Serono and Sanofi Genzyme for investigator-initiated trials. A. Schembri, PhD, has received personal compensation for activities with Cogstate as an employee. Dr Nativ has received personal compensation for activities with Clinique NeuroGym as owner and director. C. Paquette is an employee of Clinique Neuro-Outaouais. Dr Kalinowski has received personal compensation for activities with Cogstate as an employee.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported financially by Biogen Canada Inc, which also provided the experimental drug and the placebo.