
Abstract
After an initial meeting in 2013 that reviewed adherence to disease modifying therapy, the AD@MS group conducted a follow-up meeting in 2014 that examined adherence to behavioural interventions in MS (e.g. physical activity, diet, psychosocial interventions). Very few studies have studied adherence to behavioural interventions in MS. Outcomes beyond six months are lacking, as well as implementation work in the community. Psychological interventions need to overcome stigma and other barriers to facilitate initiation and maintenance of behaviour change. A focus group concentrated on physical activity and exercise as one major behavioural intervention domain in MS. The discussion revealed that patients are confronted with multiple challenges when attempting to regularly engage in physical activity. Highlighted needs for future research included an improved understanding of patients’ and health experts’ knowledge and attitudes towards physical activity as well as a need for longitudinal research that investigates exercise persistence.
Introduction
Adherence to medical interventions is a global problem, particularly in chronic diseases such as multiple sclerosis (MS). Participants of a first international meeting on Adherence in MS (AD@MS) in 2013 under the auspices of the European Rehabilitation in MS (RIMS) Network concluded that there is a lack of rigorous and robust research examining adherence to medication regimens in MS. 1 The group further highlighted the importance of research examining the preferences, attitudes and needs of patients regarding behaviour change decisions, and the importance of investigating the provision of high quality patient information as a prerequisite for optimal decision making.
The goal of the second AD@MS meeting (5 June 2014) was to summarize the current knowledge of adherence to behavioural interventions in MS and to identify core areas for future research. In the 2013 consensus we defined adherence as active agreement, consent and involvement of patients in their medical treatment. This definition of adherence can include drug treatments and medically oriented diagnostic tests, but also substantial and subtle lifestyle changes. We now operationally define behavioural interventions as educational and interactive treatments designed to induce healthy non-pharmacologic behaviour change. Behavioural interventions that successfully promote a healthy lifestyle can reduce the risk and/or severity of many chronic conditions, including cardiovascular disease, cancer, depression, dementia and sexually transmitted disease. 2
Rehabilitation may be the most complex behavioural intervention. It is a problem-solving educational process designed to change behaviour and adherence to these changes via enhanced activity and health participation. 3 Understanding rehabilitation adherence requires the examination of multiple distinct treatment approaches and processes that are commonly oriented by a set of overlapping goals. Whereas adherence to single components of a rehabilitation process (e.g. exercise, diet or use of specific self-management skills) can be studied, examining adherence to the whole approach presents significant methodological challenges.
Although adherence is a multi-dimensional construct, it is often conceptualized as unitary in drug treatment and behavioural intervention studies. Multimodal measurement of adherence may be especially important in behavioural interventions to obtain a detailed estimate of patient engagement. 4 Moreover, the effectiveness of behavioural interventions frequently depends upon the continued application of newly acquired skills. As such, adherence research is at the core of all behavioural interventions.
The first part of the second AD@MS meeting consisted of a series of short presentations by participants detailing behavioural adherence to psychosocial interventions, diet and exercise. Next, a structured focus group (n = 20) was used to compile future research prospects for physical activity adherence in MS (for detailed group information see the participant list below). A list of core questions was devised by the facilitator (PB) and the focus group lasted for 90 minutes.
Summary of major topics
Diet change and adherence
As evidenced by rising rates of obesity in the western world, adherence to healthy diets requires substantial behavioural control. While there is some scientific agreement surrounding what constitutes optimal nutrition in the general population, 5 there is no specific consensus in MS. Obesity causes fatigue and mobility problems in the general population and worsens mobility symptoms in MS. Moreover, new data suggest that obesity is associated with disease onset and symptoms expression. As such, dietary counselling in MS is highly relevant, but rarely discussed in the scientific literature. MS patients commonly seek an array of dietary interventions and supplements. Although many different diets such as vitamin D supplementation, low salt, and ketogenic diets have been touted for their possible therapeutic effects, current evidence may only justify supplementation with polyunsaturated fatty acids.6,7 Given the emerging importance of obesity as a risk factor for developing MS and the value placed on nutritional supplementation by MS patients, the paucity of valid studies in this area is possibly one the most unmet needs in MS lifestyle research. Studies promoting diets in MS beyond supplementary interventions are largely absent. With improved life expectancy, addressing co-morbidities like obesity becomes increasingly relevant to patients with MS.
Behavioural interventions to manage neuropsychiatric symptoms and distress
An increasing number of studies show beneficial effects of psychosocial interventions to control and manage common mental health difficulties in MS, including fatigue, depression and cognitive dysfunction.8–10 Despite these successes, psychosocial interventions generally show drop-out rates from 25% to 75% and lack long-term follow-up data. 4 Measuring adherence to these interventions is a complex endeavour. In addition to missing appointments outright, patients fail to actively engage during, between or after sessions. In contrast to drug regimens for chronic disease that typically must be taken indefinitely, psychosocial interventions may be applied in a low frequency for a defined number of sessions, some with occasional follow-up or ‘booster’ sessions. While session attendance can easily be measured, intra- and inter-session involvement depends on surrogates such as questionnaires, interviews and audio/video ratings. These interventions commonly promote adherence by using reminder calls, motivational interviewing, SMS texting, email, motivational enhancement techniques, and concrete support (e.g. scheduling, transportation). Homework completion has been shown to contribute substantially to treatment effects in psychosocial interventions. 11 In addition, promoting a strong therapeutic alliance between patients and their providers based on trust may play a substantial role in fostering adherence.
Based on the cognitive problems in MS, specific neuropsychological interventions are increasingly studied. 10 They need to handle not only the stigma of psychiatric disease but also the stigma of cognitive dysfunction.
Finally, although seldom studied, acceptance-oriented psychological interventions might improve openness to behaviour change.
Physical activity
Among other benefits, regular physical activity and exercise improve functional mobility and overall quality of life in MS. 12 On the other hand, physical activity rates are reduced in MS leading to concerns about exercise adherence. Bodily limitations, difficulties with service access and limited transportation are substantial barriers. Exercise studies in MS have shown as high as 80% adherence rates in the core study phase 13 but data six months or more post intervention are scarce. Moreover, how adherence is defined in exercise studies is highly variable and no gold standard exists for the requisite percentage of training sessions completed or the amount of in-session effort required. Implementation of exercise programmes within the community is one major key to increasing physical activity among patients with MS. This can be addressed by identifying theoretically-based determinants of physical activity (e.g. self-efficacy or outcome expectations as facilitators and bodily limitations as impediments) that can then be targeted by behavioural interventions or integrated into exercise training programmes.
There is limited evidence regarding optimal approaches for initiating and then maintaining changes in physical activity and very little research has been conducted among MS patients with a progressive course. Various approaches to improving exercise adherence have been discussed, including group training, socializing via internet exchanges, and the application of gaming settings. Health education and financial incentives have also been proposed as possible means of improving exercise adherence. However, more research is needed to fully ascertain the efficacy of these approaches. Collectively, these voids in the literature served as a major impetus for the focus group to discuss exercise and physical activity.
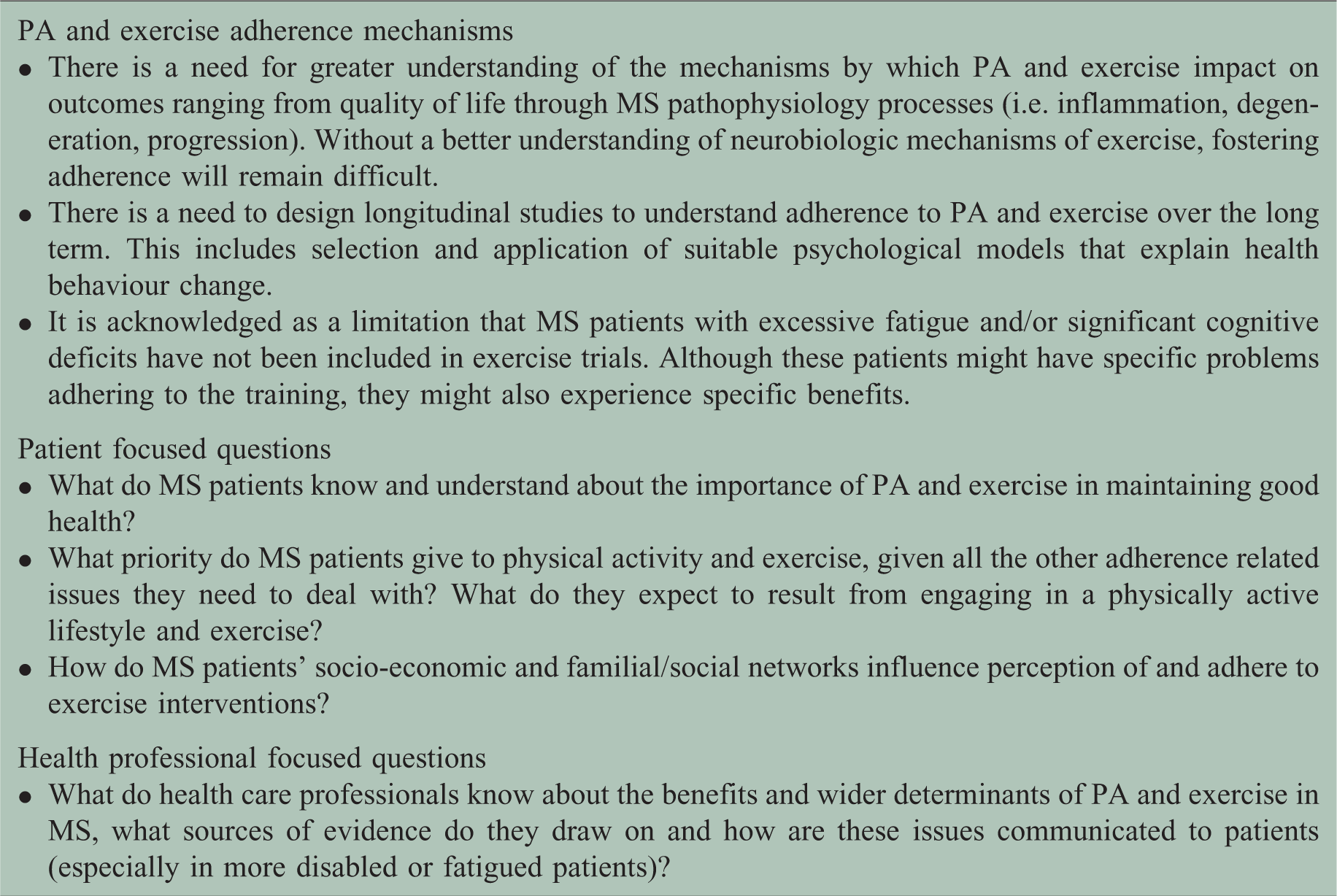
Focus group on adherence to physical activity in MS
Research issues derived from the focus group regarding physical activity (PA), exercise and adherence.
Conclusions
Drug and behavioural therapies both play a major role in the optimal management of MS. While a plethora of data suggest short-term effects on patient-reported outcomes, the long-term impact of behavioural interventions on psychological wellbeing, symptom management, illness-related impairment, activity and healthcare participation is not clear. The group agreed that any large behavioural intervention study should include maintenance data beyond month 6 post treatment. In addition, it was agreed that multiple levels of adherence data should be obtained and reported for all behavioural trials. Finally, there was consensus that there is a lack of information regarding how patients and health professionals perceive nonadherence to behavioural interventions.
Footnotes
Acknowledgements
Participants: neurologists: A Solari, C Heesen; psychologists: P Hamalainen, J Bruce, L Eliasson, P Weinmann, R Moss-Morris, A Bougoussian, K Liethmann, A Giordano, R Gearing; health scientist: S Köpke; physiotherapists: P Feys, P van Asch; occupational therapists: D Kos, M Finlayson; sport scientists: R Motl, U Dalgas; sociologist: P Bissell; MS nurse: V Mathews; nutrition researcher: F Visioli.
Funding
This work was supported by Novartis Pharma (unconditional grant).
Conflict of interest
The authors declare that there is no conflict of interest.