
Abstract
Objectives
Healthcare chatbots have become essential tools for delivering health information and alleviating systemic pressures on medical resources. However, little research exists on how the AI attributes of healthcare chatbots affect users’ adoption intentions.
Methods
Drawing on the stimulus-organism-response framework and tri-dimensional trusting beliefs theory, this study considers two AI attributes—perceived intelligence and perceived anthropomorphism—as stimuli and explores their effects on users’ functional perceptions (perceived usefulness, perceived ease of use, perceived fairness, perceived performance risk) and relational perceptions (competence trust, benevolence trust, integrity trust), and subsequently users’ intention to adopt healthcare chatbots. The research model was assessed using partial least squares structural equation modeling, based on survey data from 416 respondents in China.
Results
The results demonstrate that both perceived intelligence and perceived anthropomorphism significantly influence users’ functional and relational perceptions. Perceived intelligence and perceived anthropomorphism enhance users’ intention to adopt healthcare chatbots through perceived usefulness, competence trust, and benevolence trust. Competence trust and benevolence trust mediate the effects of perceived intelligence and perceived anthropomorphism on users’ intention to adopt healthcare chatbots, while integrity trust did not significantly affect user adoption intention.
Conclusions
The findings enhance the theoretical understanding of healthcare chatbot adoption and provide practical insights for their design and implementation.
Keywords
Introduction
In recent years, the rapid development of artificial intelligence (AI) technologies has led to the widespread use of AI-enabled chatbots in healthcare to address people’s needs for health information and medical advice.1,2 These chatbots interact with users through natural language via text or voice, providing personalized health-related suggestions. 3 For example, Woebot offers mental health support based on cognitive behavioral therapy, while Ada Health utilizes predefined medical rules to help users identify symptoms and suggest potential conditions. 4 Such chatbot-based health consultation platforms can deliver timely, personalized, and professionally informed responses, 5 holding considerable potential to reduce the imbalance between increasing healthcare demand and limited medical resources.
Despite these potential benefits, individuals remain reluctant to rely on healthcare chatbots for medical advice and still prefer consulting human physicians.3,6 To address this skepticism, prior studies have made significant efforts to identify determinants of healthcare chatbot adoption.1,3,7,8 These factors include perceived usefulness, loneliness, subjective norms, and sense of uniqueness. For instance, research has shown that loneliness drives people to use conversational AI for emotional support, 7 while individuals with a high sense of uniqueness are less willing to accept medical AI for treatment. 8 However, these studies primarily focus on user-related factors and pay relatively limited attention to the role of chatbot-specific characteristics in shaping users’ experiences during human–chatbot interactions.
Compared with traditional approaches to seeking health information through search engines or online health communities, 9 healthcare chatbots possess distinctive AI-enabled features. These AI-enabled features, namely perceived intelligence and perceived anthropomorphism,10,11 are identified as two essential attributes of AI-based systems. Perceived anthropomorphism refers to the extent to which users perceive healthcare chatbots as human-like during consultations. 11 Perceived intelligence reflects users’ perceptions of a chatbot’s capability to understand requests, process information, and autonomously generate effective responses. 11 These two AI attributes may fundamentally shape users’ interaction experiences and influence how they perceive and evaluate healthcare chatbots. For instance, anthropomorphic characteristics can enhance users’ sense of social presence,3,12,13 making interactions feel similar to communicating with a real physician and thereby strengthening trust in healthcare chatbots. Existing evidence suggests that physicians are more likely to rely on AI advice when they believe in its capabilities. 14 Additionally, related constructs, such as personalization 1 and diagnostic affordances, 15 have been shown to influence usage intentions of AI-based healthcare systems. Although previous studies have examined user preferences for anthropomorphism and intelligence attributes in various AI applications,11,16,17 the mechanisms through which these two AI attributes affect users’ perceptions and adoption intentions of healthcare chatbots remain insufficiently understood.
Trust, as a key relational construct, is frequently recognized as playing a mediating role in human–chatbot interactions.11,18,19 However, most studies conceptualize trust as a unidimensional construct, overlooking the possibility that users evaluate AI systems across multiple trust dimensions. According to trusting beliefs theory, 20 trust in human-like AI systems comprises benevolence, integrity, and competence. Individuals evaluate not only system performance but also whether it understands their needs and provides reliable and honest recommendations. 21 These considerations reflect multiple dimensions of trust that shape users’ evaluations. Nevertheless, existing research has not adequately captured these complex perceptions in interactions with healthcare chatbots. Examining multidimensional trust can therefore provide a more nuanced understanding of how users evaluate healthcare chatbots and how these evaluations influence adoption decisions. Furthermore, it enables a deeper investigation of how perceived anthropomorphism and perceived intelligence shape different trust dimensions.
Beyond relational evaluations, users also form functional evaluations of AI systems. Prior research has identified perceived usefulness and perceived ease of use as key determinants of technology adoption. 22 However, in the context of healthcare and AI, concerns related to risk and fairness are also critical. Users’ concerns about potential errors made by medical AI systems may hinder adoption, 23 while perceptions of whether AI systems are unbiased play a crucial role in their successful implementation. 24 Despite their importance, limited research has examined how AI attributes shape perceptions of performance risk and fairness, or how these perceptions influence healthcare chatbot adoption.
Based on these gaps, this study addresses the following research question: How do perceived anthropomorphism and perceived intelligence influence users’ functional perceptions (i.e., perceived usefulness, perceived ease of use, perceived performance risk, and perceived fairness) and relational perceptions (i.e., benevolence trust, integrity trust, and competence trust), and subsequently shape the adoption intention of healthcare chatbots?
To address this question, we develop a theoretical model grounded in the stimulus–organism–response (S–O–R) framework. We conceptualize perceived anthropomorphism and perceived intelligence as stimuli and examine their effects on organism-level perceptions and behavioral responses (i.e., adoption intention). Drawing on the service robot acceptance model (sRAM), 22 we identify perceived usefulness, perceived ease of use, perceived fairness, and perceived performance risk as functional perceptions. For relational perceptions, we adopt the multidimensional trusting beliefs framework, operationalizing trust through benevolence, integrity, and competence. Data were collected from 416 respondents, and the proposed model was empirically tested using partial least squares structural equation modeling (PLS-SEM).
This study makes three key contributions. First, it extends the literature on AI attributes10,11,17,19 by theorizing and empirically examining the distinct roles of perceived anthropomorphism and perceived intelligence in shaping user evaluations. By showing that these attributes jointly influence adoption through both relational and functional mechanisms, it provides a more nuanced understanding of how AI characteristics operate in healthcare contexts. Second, this study advances research on trust in human–AI interaction18,19 by unpacking its multidimensional nature, showing that competence trust and benevolence trust significantly influence adoption intention, whereas integrity trust does not. Additionally, we identify meaningful relationships between perceived fairness, perceived performance risk, and the three trust dimensions. Third, it offers an integrated model that elucidates the mechanisms through which AI attributes affect healthcare chatbot adoption, providing insights into the factors driving such adoption.
Theoretical background
AI attributes
With the advancement of AI-enabled information systems that provide users with personalized and intelligent experiences, increasing attention10,11,25 has been given to the unique attributes that distinguish such systems from traditional ones. Priya and Sharma 26 categorized the artificial intelligence attributes of intelligent virtual assistants into three types: perceived anthropomorphism, perceived intelligence, and perceived animacy. Similarly, Yang et al. 25 divided chatbots’ AI capabilities into two aspects: cognitive intelligence—the ability to analyze information—and emotional intelligence—the ability to recognize and express emotions. Moussawi et al. 10 summarized perceived anthropomorphism and perceived intelligence as two essential attributes of AI-enabled systems and developed reliable and valid scales to measure these two constructs. Since then, numerous scholars11,16,19 have adopted these measurement scales to investigate the roles of perceived anthropomorphism and perceived intelligence in shaping user behavior toward AI-powered technologies. Perceived intelligence 10 is defined as the extent to which a chatbot can autonomously generate effective outputs and process and produce natural language. This definition implies that an intelligent chatbot is characterized by autonomy, adaptability, learning capacity, and reasoning ability. Perceived anthropomorphism,10,11 on the other hand, refers to the extent to which a chatbot is viewed as human-like, based on traits like humor, friendliness, and care. Existing research has examined the effects of perceived anthropomorphism and perceived intelligence on adoption behavior in contexts such as hospitality and tourism,16,17 banking, 19 and personal intelligent agents. 11 However, studies focusing on healthcare chatbots remain limited. Some studies have explored how different anthropomorphic features2,3 influence users’ trust in health consultation services, yet little is known about how perceived anthropomorphism shapes users’ functional perceptions. Exploring how perceived anthropomorphism and perceived intelligence influence users’ functional, emotional and relational perceptions is crucial for maximizing the effectiveness of AI technologies in healthcare applications.
Functional and relational factors driving chatbot adoption
Existing studies based on the sRAM model22,23,27 have proposed that factors influencing users’ adoption intention toward chatbots can be captured from three dimensions, namely functional, social, and relational dimensions. This classification stems from the understanding that, in AI-based service contexts, individuals not only evaluate the technical effectiveness of a system but also develop social, emotional, and relational needs during interactions with it. 22 Within the functional dimension, perceived usefulness and perceived ease of use are two key elements that have been proven to positively influence the acceptance of chatbots.23,27 In addition, in healthcare contexts, users are often concerned about potential negative outcomes associated with intelligent technologies. Therefore, perceived performance risk 23 has been identified as a functional factor that negatively affects the adoption of healthcare chatbots. Moreover, because healthcare services often involve issues of resource allocation, users also evaluate the fairness of algorithms applied in this context. Prior studies 24 have found that users form trust perceptions based on their functional evaluations of algorithmic fairness. Regarding the relational dimension, trust is recognized as a critical relational variable,19,22,27 capturing the extent to which individuals feel comfortable and secure in relying on the trustee. Previous studies11,19,28 have demonstrated that trust serves as an important predictor of chatbot-based services adoption. Since the social dimension reflects users’ social needs in specific contexts,22,27 and the variable perceived humanness under this dimension overlaps conceptually with perceived anthropomorphism, the social dimension was not included in the study. While prior research has explored the effects of functional and relational perceptions on chatbot adoption,11,17,22,27 limited attention has been paid to identifying the factors that drive these perceptions and to examining the interactions between them.
Trusting beliefs
Scholars20,29 have posted that the dimensionality of trust in technology depends on the degree to which a technology is perceived as human-like. When a technology is perceived as less human-like, system-like trusting beliefs, including reliability, functionality, and helpfulness, are typically used. Conversely, when a technology is perceived as more human-like, trust is divided into three dimensions: integrity, competence, and benevolence. 20 Researchers 25 have adopted human-like trusting beliefs to measure trust in AI-based systems, as individuals often ascribe human qualities and attributes to such systems. In our study, we examine how the anthropomorphism and perceived intelligence of healthcare chatbots influence users’ perceptions. Thus, adopting human-like trusting beliefs is more appropriate for our context. Specifically, benevolence trust 20 reflects the trustor’s belief that the trustee (i.e., the healthcare chatbot) cares about the trustor’s interests, competence trust refers to the trustee’s ability to fulfill its commitments, and integrity trust represents the trustor’s perception that the trustee adheres to a set of principles acceptable to the trustor. Prior studies focusing on chatbot adoption have primarily treated trust as a unidimensional construct, examining its mediating role between AI features (e.g., perceived anthropomorphism, perceived intelligence)3,11,19 or technology features (e.g., perceived usefulness, perceived ease of use) 30 and user adoption behavior. However, little research has investigated the distinct roles of different trust dimensions, namely benevolence trust, competence trust, and integrity trust, in human–AI interactions. Investigating these aspects is crucial for gaining deeper insight into the mechanisms through which AI attributes influence user adoption intention of healthcare chatbots.
The stimulus-organism-response framework
The S-O-R model from environmental psychology was proposed to explain how the environment affects human behavior. 31 The theory proposes that environmental cues act as stimuli, influencing individuals’ internal experiences (organism), which then lead to behavioral responses. Stimuli refer to factors that, at a specific time and place, have a clear and systematic effect on behavior, independent of personal traits or choice alternatives. 32 By applying the S-O-R model to online commerce, Zheng et al. 32 conceptualized stimuli as the functional elements and design features of the online environment. Organisms refer to users’ internal states, involving cognitive and emotional states, such as perceptions, experiences, and evaluations. 31 Responses reflect the outcomes of user reactions to their assessments, such as purchase behavior, social commerce intentions, and product attachment32–34
Using the S-O-R model as the theoretical foundation for this study provides two important benefits. First, the S- O-R model is widely used to explain how users’ experiences and responses are shaped by external stimuli embedded in products or services. For example, Cho et al. 34 used the S-O-R model to explore how technological and fashion-related features of smartwatches influence users’ attachment to the product. Moreover, researchers have called for future studies to apply the S-O-R framework to investigate interactions between users and service robots.17,35 Therefore, this model offers a useful framework for understanding user’s perceptions and behavioral intentions towards healthcare chatbots. Second, healthcare chatbots differ significantly from traditional health consultation platforms, the S-O-R model helps identify the unique features of healthcare chatbots and develop an integrated model to explain how these features shaping user behavior.
In our study, perceived anthropomorphism and perceived intelligence are conceptualized as the stimuli (S). We examine the effects of these two AI attributes on users’ organismic experiences (O), which include both functional and relational perceptions. Specifically, perceived usefulness, perceived ease of use, perceived fairness, and perceived performance risk are classified as functional perceptions, while benevolence trust, integrity trust, and competence trust are identified as relational perceptions. Finally, users’ adoption intention of healthcare chatbots is regarded as the response (R) to these stimuli.
Hypothesis development
Using the S-O-R framework as a foundation, we developed our research model, which is presented in Figure 1. Our research model proposes that two AI attributes of healthcare chatbots (i.e., perceived anthropomorphism and perceived intelligence) act as stimuli that influence users’ internal experiences, including functional perceptions (i.e., perceived usefulness, perceived ease of use, perceived fairness, perceived performance risk) and relational perceptions (i.e., competence trust, benevolence trust, integrity trust). Subsequently, these perceptions influence the response (i.e., users’ intention to adopt healthcare chatbots). In addition, we derive hypotheses (H3(b), H4, H5(a), H5(b)) to investigate the relationship between functional perceptions and relational perceptions. Research model.
AI attributes and users’ functional and relational perceptions
Perceived intelligence refers to the extent to which a healthcare chatbot can process natural language and generate effective outputs.10,11 A healthcare chatbot that is perceived as intelligent is typically associated with characteristics such as autonomy, self-learning, adaptability, and efficiency.10,11,19 The perceived intelligence and competence characteristics of chatbots tend to foster users’ positive cognitive appraisals,17,36 such as increased hedonic value and satisfaction. Users often rely on healthcare chatbots to accomplish specific tasks, including symptom checking and medication inquiries. 23 The chatbot’s ability to process information and generate relevant content gives it the potential to assist users in completing these tasks effectively. Moreover, the intelligent attributes of healthcare chatbots enable them to better understand users’ needs. Since users can communicate with the chatbot using natural language, the required mental effort to operate the system is reduced. 11 When a chatbot is perceived as more intelligent, users are likely to perceive it as more useful and easier to use. In addition, during interactions with healthcare chatbots, users may implicitly ascribe human qualities to the system 22 and develop a relational bond with it. The chatbot’s ability to complete tasks efficiently, respond personally, and adapt to users’ needs can lead users to believe that the chatbot is capable of performing tasks as expected, thereby fostering competence trust. Hence, we hypothesize:
H1(a). Perceived intelligence positively affects perceived usefulness.
H1(b). Perceived intelligence positively affects perceived ease of use.
H1(c). Perceived intelligence positively affects competence trust.
Fairness in resource allocation 37 and performance risk 23 are critical concerns in healthcare services. Algorithmic fairness 24 is defined by an algorithm’s nondiscrimination, accuracy, and adherence to due process. Similarly, Colquitt 38 conceptualized justice as a four-factor construct encompassing distributive, procedural, interpersonal, and informational justice. Integrating these perspectives, this study defines perceived fairness as the extent to which a healthcare chatbot provides unbiased algorithmic decisions, ensures data accuracy, follows fair decision-making procedures, and ensures informational justice. Healthcare chatbots are supposed to perform tasks autonomously, which has generated optimism that they may reduce common human biases and errors in medical decision-making. 39 By relying on predefined rules, healthcare chatbots can standardize decision procedures. 40 Moreover, their advanced text and voice communication capabilities allow users with varying levels of information literacy to access the information they need. Therefore, a healthcare chatbot perceived as highly intelligent may be positively associated with perceived fairness.
Perceived performance risk 41 refers to the degree of uncertainty regarding the potential negative outcomes that a healthcare chatbot may produce. Users are particularly concerned about the performance risk of healthcare chatbots because such risks directly affect their health and safety. When AI systems can deliver accurate diagnostic results and demonstrate strong adaptability to users’ needs, individuals are more likely to believe that these systems can produce positive outcomes in other medical tasks and avoid potential risks or errors. Prior research has found that the use of AI in mobile banking significantly reduces users’ perceived financial risk. 19 Hence, we hypothesize:
H1(d). Perceived intelligence positively affects perceived fairness.
H1(e). Perceived intelligence negatively affects perceived performance risk.
Anthropomorphism refers to the attribution of human-like characteristics to non-human entities, such as chatbots and computers. 42 Research has shown that perceived anthropomorphism is positively associated with both users’ utilitarian values, which are task-oriented and rational, and hedonic values, which encompass emotional and social aspects.17,26 Specifically, anthropomorphism makes a chatbot appear more familiar, which facilitates easier and more natural interactions. 43 Furthermore, anthropomorphism can help build and enhance trust. The social and emotional cues presented by an anthropomorphic chatbot provide users with the necessary information to make trust inferences. Perceived anthropomorphism encourages users to experience social proximity 3 during their interactions with the chatbot, which fosters trust development. Users may feel that the healthcare chatbot is warm, that it cares about their interests, and that it adheres to principles they expect it to follow. Previous studies have demonstrated that perceived anthropomorphism is closely related to overall trust.2,11,44 When examining the sub-dimensions of trust, the stimulus of perceived anthropomorphism may have a significant impact on benevolence trust and integrity trust. Hence, we hypothesize:
H2(a). Perceived anthropomorphism positively affects perceived ease of use.
H2(b). Perceived anthropomorphism positively affects benevolence trust.
H2(c). Perceived anthropomorphism positively affects integrity trust.
User perceptions and adoption intentions of healthcare chatbots
Perceived usefulness refers to the extent to which an individual believes that using the information system improves their performance. 45 When chatbots deliver useful information and support task efficiency, they capture users’ interest in utilizing the service. 46 Huang 47 found that perceived accuracy and completeness enhanced pet owners’ satisfaction with veterinary chatbots. Studies across various fields have identified a positive connection between perceived ease of use and perceived usefulness, such as e-commerce, 30 intelligent agents, 11 and service robots. 22 Perceived ease of use reflects the cognitive effort involved in learning and using new technology. As perceived ease of use increases, cognitive load and effort decrease, leading users to perceive more benefits from technology. In the context of service robots, Moussawi 22 identified perceived ease of use and perceived usefulness as functional elements in the service robot acceptance model, with perceived ease of use positively affecting perceived usefulness. Hence, we hypothesize:
H3(a). Perceived usefulness positively affects users’ intention to adopt healthcare chatbots.
H3(b). Perceived ease of use positively affects perceived usefulness.
Fairness in algorithms refers to ensuring that algorithmic decisions do not result in discriminatory or inequitable outcomes. 24 In our study, perceived fairness in healthcare chatbots is derived from elements like unbiased algorithms, accurate data, due process, and informational fairness. Based on psychological contract violation theory, 23 biased algorithms challenge users’ fundamental beliefs about behavioral norms in trusting relationships, leading to greater integrity distrust in algorithms. Existing research has found that biased information increases users’ integrity distrust in AI-based customer service. 25 When services demonstrate accuracy, users are more likely to perceive the outcomes as reliable and trustworthy, believing that the algorithm will honor its commitment. 48 The perception of fairness plays a significant role in shaping trust in algorithm services. 24 , 49 When examining the sub-dimensions of trust, perceived fairness may have a significant impact on integrity trust. Hence, we hypothesize:
H4. Perceived fairness positively affects integrity trust.
Perceived performance risk is often regarded as a functional feature 23 that is closed linked to perceptions of competence and integrity, both of which are valued for utilitarian reasons. 29 While prior studies have examined the relationship between perceived risk and trust, findings remain inconclusive as to whether risk is an antecedent to trust or an outcome of trust.50,51 This study proposes a negative relationship where trust is considered the outcome of perceived performance risk; that is, when users feel safe with a healthcare chatbot, they are more likely to view it as trustworthy. 29 Hence, we hypothesize:
H5(a). Perceived performance risk negatively affects competence trust.
H5(b). Perceived performance risk negatively affects integrity trust.
According to McKnight’s web trust model, trusting beliefs, such as competence, benevolence, integrity, are positively related to trust intentions. 29 When users consider a technology trustworthy, they feel a secure willingness to depend on it. Research across various fields has confirmed the significant role of trust in predicting chatbot adoption intentions, such as hospitality and tourism,16,52 personal intelligent agents. 11 When customers feel a sense of trust in technology, they are less likely to be skeptical and more inclined to accept it. 53 In healthcare specifically, trust is a critical factor in influencing patients’ intention to adopt conversational agents. 5 If users perceive competence distrust or benevolence distrust in AI-based customer service, they may not use it and show resistance to it. 25 Hence, we hypothesize:
H6(a). Competence trust positively affects users’ intention to adopt healthcare chatbots.
H6(b). Benevolence trust positively affects users’ intention to adopt healthcare chatbots.
H6(c). Integrity trust positively affects users’ intention to adopt healthcare chatbots.
Research methodology
Research design and measurement
IFlytek Xiaoyi was chosen for this study, an advanced AI health assistant built on a medical large-model technology. As one of China’s pioneering and leading healthcare chatbots, iFlytek Xiaoyi was officially launched on October 24, 2023, and has exceeded 12 million downloads as of June 28, 2024. 54 IFlytek Xiaoyi provides users with various functions, including symptom self-examination, drug inquiries, report interpretation, and diet recommendations. Another reason for selecting iFlytek Xiaoyi as the research context is its ability to intelligently respond to health consultations and communicate in a human-like manner, distinguishing it from traditional health consultation platforms. The iFlytek Xiaoyi app supports multi-round, multi-modal interaction and can respond to health consultations across all ages and stages of the health cycle. In conclusion, the emerging and unique characteristics of iFlytek Xiaoyi, driven by a medical large model, indicate that it is a suitable research object for this study.
The constructs in the research model were measured using items adapted from prior research with minor adjustments for this study’s context. Specifically, perceived intelligence, perceived usefulness were measured using items adapted from Pillai and Sivathanu. 16 Perceived anthropomorphism was measured with items adapted from Fernandes and Oliveira. 53 Perceived ease of use, perceived performance risk, and users’ intention to adopt healthcare chatbots were measured with items adapted from Wang et al. 23 Perceived fairness was measured using items based on Colquitt 38 and Shin. 24 Competence trust, benevolence trust and integrity trust were all measured using items adapted from McKnight et al. 29 Back-translation between English and Chinese was conducted to ensure the measurement instrument’s original meaning was retained in the final survey. All the items were rated using a seven-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). A pre-test was conducted to ensure content validity, clarity, and readability of the questionnaire. Two academic experts assessed the content validity of each scale item, while ten postgraduate students with experience using AI-based health consultation services evaluated the clarity and readability of the survey questions. Based on their feedback, we reworded several items to improve comprehensibility and refined the survey instructions and response format. The final measurement items for the ten constructs are presented in Appendix A. Gender, age, education, frequency of healthcare chatbot usage, and timing of first use are included as control variables. A pilot study was conducted with the first 100 respondents. Reliability and validity were assessed, and two measurement items with low loadings (<0.70) were removed. After refinement, all constructs met the recommended thresholds. Based on these results, the survey was finally distributed on a larger scale.
Data collection
In our study, an online survey was designed and conducted to measure participants’ perceptions. Partial least squares structural equation modeling was then employed to analyze the proposed model. Our data collection procedure consisted of two stages. To ensure that participants had a concrete understanding of what healthcare. Chatbots are and their key features, all participants were required to engage in a real interaction with a healthcare chatbot before completing the questionnaire. Specifically, participants were directed to experience a healthcare chatbot, namely iFlytek Xiaoyi. They were instructed to complete at least three tasks, such as drug inquiries, self-diagnosis, and hospital searches. To ensure task completion, participants were required to upload their interaction records as verification. After completing the interaction, participants proceeded to the main survey. The questionnaire measured 10 constructs, along with demographic information and prior experience with healthcare chatbots. The process is shown in Appendix B.
Before the formal data collection, we assessed the minimum sample size required for PLS analysis of the proposed model using G*Power. A power analysis conducted with G*Power version 3.1.9.6, following previous studies,55,56 employed the linear multiple regression option with a medium effect size (f2 = 0.15), error probability (α =.05), statistical power (1 − β = .95), and nine predictors, yielding a minimum required sample size of 166.
This study employed a purposive sampling strategy to target current users and potential users of healthcare chatbots. Prior research has shown that individuals under the age of 3023 constitute the primary user group for healthcare chatbots. Accordingly, we adopted an online multi-platform recruitment strategy to reach this group. Participants were recruited through popular Chinese social media platforms, including WeChat, QQ, Weibo, and Xiaohongshu, which are widely used by the target population. To ensure sample relevance, participants were also asked to report their prior experience with healthcare chatbots and to complete an interaction task with a healthcare chatbot. The questionnaire was distributed via Wenjuanxing (https://www.wjx.cn/), a leading online survey platform in China. Data were collected in two rounds. The first round took place from December 18, 2023, to January 10, 2024, yielding 234 initial responses. The second round was conducted between March 15 and March 22, 2026, yielding 200 responses. To ensure data quality, the following screening criteria were applied: (1) participants had to complete at least three interaction tasks with the healthcare chatbot; (2) participants had to correctly answer two attention-check questions; (3) responses with unusually short completion times or exhibiting identical answers across all items were removed. After data cleaning, a total of 416 valid responses were retained for analysis, which satisfies the minimum sample size requirement.
This study was conducted in accordance with established ethical principles. All participants were informed of the study’s purpose, procedures, potential risks, and benefits. Written informed consent was obtained from all participants before study initiation. The survey data collected were processed anonymously and kept strictly confidential. The study protocol was reviewed and approved by the Ethics Review Board of Wuhan University.
Demographic information of respondents (N=416).

Results
Using the two-step approach suggested by Anderson and Gerbing, 57 we first evaluated the measurement model for reliability and validity of the instrument, then assessed the structural model. Given its robustness for both large and small sample sizes,30,58 we employed partial least squares structural equation model with SmartPLS (4.1.0.8) to analyze the research model.
Measurement model
VIF, loadings, reliability and convergent validity.

Discriminant validity.

Note. (1) The square root of the AVE for each construct is presented in bold; (2) Off-diagonal elements are correlations among latent constructs.
Common method bias
Since the data for this study was gathered using a questionnaire, it is essential to consider the potential issue of common method bias (CMB). We applied Harman’s single-factor test to detect the severity of common method bias. The test results indicated that the first factor explained 40.3% of the total variance, which did not exceed the 50% threshold, 60 proving that CMB is not a serious problem. This study also assessed the potential for multicollinearity by evaluating the variance inflation factors (VIF). As shown in Table 2, all VIF values were below the recommended threshold of 3.3, 61 suggesting that multicollinearity is not a concern. 62 Therefore, CMB was not an issue in this study.
Structural model
The structural model results are shown in Figure 2 and Table 4, including path coefficients and explained variances. The bootstrapping approach was applied to estimate the statistical significance of the path coefficients. As shown in Figure 2 and Table 4, the paths from perceived intelligence to perceived usefulness, perceived ease of use, competence trust, perceived fairness, perceived performance risk were confirmed, supporting H1(a), H1(b), H1(c), H1(d), H1(e). The paths from perceived anthropomorphism to perceived ease of use (H2(a)), benevolence trust (H2(b)), integrity trust (H2(c)) were also supported. Perceived ease of use significantly positively affects perceived usefulness, supporting H3(b). The impact of perceived fairness on integrity trust was positive and significant, supporting H4; Perceived performance risk was found to have a negative effect on competence trust and integrity trust, supporting H5(a), H5(b). Perceived usefulness, competence trust, and benevolence trust were found to have a significant positive effect on users’ intention to adopt healthcare chatbots, while the effect of integrity trust on users’ intention to adopt healthcare chatbots was not significant. Thus, H3(a), H6(a), H6(b) were supported, while H6(c) was not supported. The results reveal that none of the control variables significantly influence users’ intention to adopt healthcare chatbots. PLS results (Note: * p< .05, ** p< .01, *** p< .001, N.S.=not significant). Hypothesis testing results.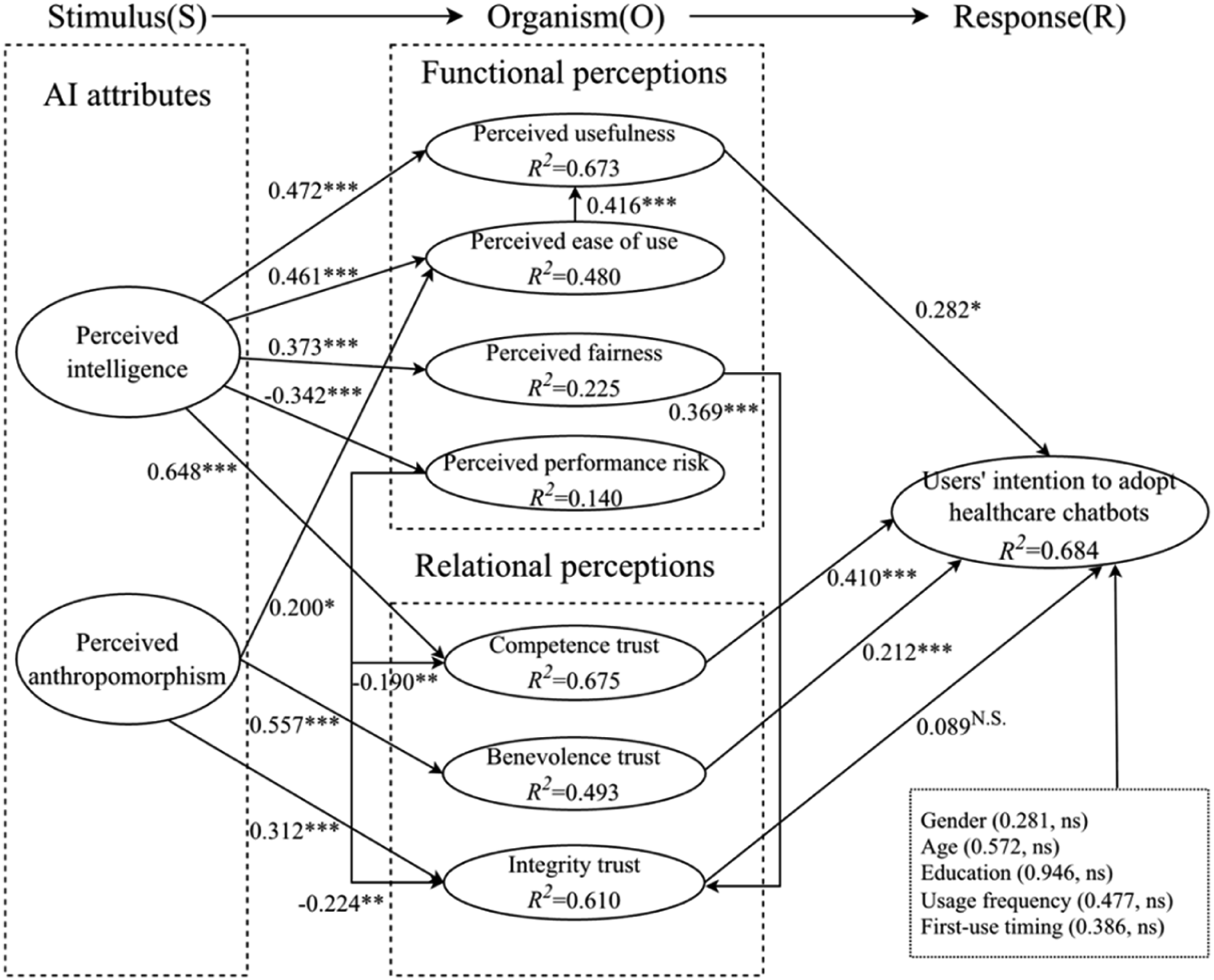

Furthermore, the R2 values were used to evaluate the model’s in-sample explanatory power. 58 The R2 values ranged from 14% to 68.4%, indicating that most variables explained moderate (>0.20) to substantial (>0.50) variance in the model (Figure 2).
Mediation test
Mediation effects.

Note: * p< .05, ** p< .01, *** p< .001.
Discussion and implications
Key findings
With the rapid rise of generative artificial intelligence and large language models,64,65 AI-powered chatbots have been increasingly applied in the healthcare sector to address users’ health information needs. However, how people perceive the unique intelligent and anthropomorphic attributes of AI-based health consultations, and how these perceptions influence their intention to adopt such services, remains underexplored. Drawing on the stimulus– organism–response framework, this study investigates how the unique AI attributes of healthcare chatbots influence users’ adoption intentions. Extending the S-O-R model with tri-dimensional trusting beliefs and the service robot acceptance model, we develop a theoretical model to examine the effects of perceived intelligence and perceived anthropomorphism on users’ functional and relational perceptions, which in turn affect their intention to adopt healthcare chatbots. A survey of 416 respondents was conducted to test the proposed hypotheses. The main findings are summarized as follows:
First, both perceived intelligence and perceived anthropomorphism significantly influence users’ functional and relational perceptions. Specifically, perceived intelligence positively affects perceived usefulness, perceived ease of use, and competence trust, consistent with Moussawi et al. 11 Moreover, perceived intelligence enhances users’ perception of fairness and reduces perceived performance risk. Perceived anthropomorphism has a significant impact on perceived ease of use, benevolence trust, and integrity trust, supporting previous findings that anthropomorphism strengthens user trust. 17 , 11 These results demonstrate that AI attributes shape both the functional and relational dimensions of users’ experiences with healthcare chatbots.
Second, perceived usefulness, competence trust, and benevolence trust directly drive users’ intentions to adopt healthcare chatbots. Specifically, perceived usefulness and competence trust mediate the relationship between perceived intelligence and user adoption intention, while benevolence trust mediates the relationship between perceived anthropomorphism and users’ intention to adopt healthcare chatbots. In contrast, integrity trust does not significantly affect user adoption intention, echoing findings by Yang et al., 25 who reported no significant link between integrity distrust and chatbot resistance. A possible explanation is that users tend to hold lower moral expectations for algorithms. 66 Thus, integrity may not serve as a primary determinant of adoption. Overall, these findings suggest that users have dual expectations of healthcare chatbots, as functional technologies that must be useful and as social entities that must be trustworthy.
Third, the results reveal differentiated roles of competence trust, integrity trust, and benevolence trust in human– chatbot interactions. Competence trust and benevolence trust mediate the effects of AI attributes on users’ intention to adopt healthcare chatbots. Furthermore, perceived fairness enhances integrity trust, consistent with Shin et al., 24 indicating that users are more likely to trust and accept healthcare chatbots when they perceive the underlying algorithms as fair. Conversely, perceived performance risk reduces both competence trust and integrity trust, indirectly influencing adoption intention through competence trust. These findings illuminate the interplay between users’ functional and relational perceptions and underscore the pivotal role of multidimensional trust in shaping user acceptance of healthcare chatbots.
Theoretical implications
This research makes several theoretical contributions. First, this study advances research on health information behavior and human–AI interaction by proposing a novel theoretical framework to explain users’ adoption of healthcare chatbots. Drawing on the S-O-R framework, we conceptualize perceived anthropomorphism and perceived intelligence as two distinct stimuli, and demonstrate that these AI attributes jointly influence adoption through both functional and relational mechanisms. Specifically, perceived intelligence affects adoption intention via perceived usefulness and competence trust, whereas perceived anthropomorphism operates through benevolence trust. Unlike prior studies that primarily focus on users’ emotional responses to anthropomorphic design,3,7,8 this study highlights the role of AI attributes and systematically examines the functional and relational pathways through which they influence adoption. This nuanced framework offers a more comprehensive understanding of how users process AI attributes when seeking health information and making adoption decisions.
Second, this study contributes to the theory of human-like trusting beliefs theory 20 by empirically demonstrating its applicability in human–AI interaction, particularly in explaining users’ complex perceptions of healthcare chatbots. While prior research has mainly applied this theory in the context of mobile application adoption,20,67 we extend it by disentangling the distinct roles of the tri-dimensional trust construct in chatbot adoption. The results show that benevolence trust and competence trust act as key mediators between AI attributes and adoption intention, exhibiting complementary and indirect-only mediation patterns, respectively, whereas integrity trust does not significantly influence adoption intention. Furthermore, we identify important links between functional perceptions and trust dimensions: perceived fairness positively affects integrity trust, while perceived performance risk negatively influences both competence and integrity trust. These findings deepen our understanding of the antecedents and consequences of tri-dimensional trusting beliefs in human–AI interaction.
Third, this research refines and extends service robot acceptance theory 22 by incorporating AI attributes as upstream stimuli, and by introducing perceived fairness and perceived performance risk as additional functional perceptions that are particularly salient in healthcare contexts. While existing models largely emphasize perceived usefulness and ease of use,11,19,27 our findings show that adoption decisions for healthcare chatbots are also shaped by concerns about risk and fairness, given the sensitive nature of health information. Specifically, perceived performance risk influences adoption indirectly through competence trust, while perceived fairness shapes users’ perceptions of integrity. By integrating these new constructs and extending the model to include upstream AI attributes, this study not only enriches service robot acceptance theory but also broadens its theoretical scope.
Practical implications
This study provides several important practical implications. First, to enhance user adoption, healthcare chatbots should be deliberately designed to balance intelligent capabilities and anthropomorphic features. Developers should prioritize improving the accuracy, source transparency, and explainability of responses 48 —such as clearly citing reliable medical sources and providing confidence levels—to strengthen users’ perceived intelligence and reduce performance risk. Simultaneously, subtle anthropomorphic elements, including empathetic language, voice tone variation, and contextual emotional recognition, 1 can effectively enhance benevolence trust, particularly in emotionally sensitive interactions such as mental health support or chronic disease management.
Second, given that competence trust and benevolence trust are the dominant drivers of adoption while integrity trust plays a limited role, designers should focus on building functional reliability and relational warmth. However, the relatively weak effect of integrity trust also signals a potential vulnerability: users may currently hold lower moral expectations toward AI. 66 To address this, healthcare institutions and regulators should develop clear ethical guidelines and accountability frameworks for healthcare chatbots. For instance, implementing auditable decision logs, transparent data usage policies, and human oversight mechanisms can gradually elevate users’ integrity perceptions and foster long-term trust in AI-assisted health information services.
Limitations and future research
This study provides contributions to human-AI interaction research, yet some limitations still exist, offering opportunities for future research. First, while we explore the effect of AI attributes on user adoption behavior through their perceptions of healthcare chatbots, we did not consider the role of users’ health state in healthcare chatbot adoption. Previous research has found that factors such as the severity and type of a health condition can impact the adoption of conversational agents in healthcare. 5 Perceived health information needs and health anxiety can drive users to engage with chatbots for health assistance. 23 In this regard, further research could explore the role of users’ health state in the relationship between AI attributes and users’ intention to adopt healthcare chatbots.
Second, the data in this study were collected through questionnaires and were based solely on China. Further research could replicate this study in different countries or regions to obtain more generalizable findings. Besides, we collected data through surveys to measure variables such as perceived intelligence, perceived anthropomorphism, functional perceptions, and relational perceptions after user interactions with healthcare chatbots. Future research could leverage actual interaction data between users and healthcare chatbots, such as analyzing anthropomorphic features exhibited in chatbot dialogue, as well as users’ emotional and cognitive states reflected in the interaction texts.
Conclusions
With the rapid development of artificial intelligence technologies, such as the rise of large language models, AI- based chatbots have been widely used to provide health advice. This study advances understanding of how users adopt AI-powered healthcare chatbots by integrating the stimulus–organism–response framework with the theory of tri-dimensional trusting beliefs and service robot acceptance. Drawing on survey data from 416 respondents, the research demonstrates that users’ perceptions of intelligence and anthropomorphism are key stimuli influencing both their functional and relational perceptions, which in turn shape their intention to adopt healthcare chatbots.
The findings reveal that perceived intelligence enhances users’ perceptions of usefulness, ease of use, competence trust, and fairness, while reducing performance concerns. Perceived anthropomorphism strengthens ease of use, benevolence trust, and integrity trust. Moreover, competence trust and benevolence trust emerge as critical mediators between AI attributes and adoption intentions, underscoring the multidimensional nature of trust in human–AI interaction. Although integrity trust exerts limited influence on adoption, its relationship with perceived fairness and perceived performance risk provides important insight into the ethical dimensions of AI trust formation. By distinguishing functional and relational mechanisms, this study contributes to theoretical advancement in human–AI interaction, enriching the S-O-R framework and extending service robot acceptance theory to the healthcare domain. Practically, the results suggest that developers and healthcare institutions should focus on enhancing both the intelligence and anthropomorphic qualities of chatbots, improving their transparency, reliability, and empathetic communication to foster user trust and acceptance.
Footnotes
Acknowledgements
The authors would like to thank the editors and the anonymous reviewers for their insightful comments and constructive suggestions. We also sincerely thank all participants who took part in this study.
Ethical considerations
This study was approved by the Ethics Review Board of Wuhan University.
Consent to participate
All participants were informed of the study’s purpose, procedures, potential risks, and benefits. Written informed consent was obtained from all participants prior to participation.
Author contributions
LSS contributed to the conceptualization and methodology of the study, conducted data collection and analysis, and drafted and revised the manuscript. ZH contributed to the methodology, data collection and analysis, and manuscript revision. FH contributed to the conceptualization of the study, manuscript revision, and funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant number 72474160, no.72074171).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the first author upon reasonable request.
Data Guarantor
LSS.
Appendix
Constructs and items
Constructs
Items
Perceive usefulness
16
PU1: Healthcare chatbots are useful for my health consultation.
PU2: Healthcare chatbots improve the efficiency of my health consultation.
PU3: Healthcare chatbots save me time on health consultations.
PU4: Overall, I feel that healthcare chatbots are very useful for health consultation.
Perceived ease of use
23
PEOU1: I find healthcare chatbots easy to use.
PEOU2: Using healthcare chatbots to obtain disease and health information is convenient and efficient.
PEOU3: Interacting with healthcare chatbots does not require much effort.
PEOU4: My interactions with healthcare chatbots are clear and easy to understand.
Perceived fairness24,38
PF1: Healthcare chatbots are fair to all users when providing services, with no favoritism or discrimination.
PF2: The process used by the healthcare chatbot to provide services is unbiased.
PF3: The opportunity to obtain information using a healthcare chatbot is fair, everyone is given the same opportunity to obtain the desired information.
PF4: The source of data throughout a healthcare chatbot and its data sources should be identified, logged, and benchmarked. (deleted)
Perceived performance risk
23
PPR1: I am worried that the healthcare chatbot may not provide the benefits I anticipate.
PPR2: I am worried that the healthcare chatbot will provide incorrect medical diagnoses.
PPR3: I feel anxious about whether the healthcare chatbot's service will be reliable whenever I think about using it.
PPR4: I am worried whether the healthcare chatbot will perform as well as it should.
Perceived anthropomorphism
53
PA1: I enjoy interacting with the healthcare chatbot.
PA2: The healthcare chatbot understands my needs.
PA3: Using the healthcare chatbot makes me feel like I'm conversing with a doctor.
PA4: When interacting with the virtual healthcare chatbot, I feel that communicating with doctors has become easier.
Perceived intelligence
16
PI1: I think healthcare chatbots are competent in providing health consultations.
PI2: I think healthcare chatbots are knowledgeable in health consultations.
PI3: I consider healthcare chatbots to be intelligent.
PI4: I think healthcare chatbots are responsible. (deleted)
Competence trust25,29
CT1: I believe that healthcare chatbots are competent and effective in providing health consultation services.
CT2: I believe the healthcare chatbot can perform well in providing health advice.
CT3: Overall, I believe the healthcare chatbot is a capable and proficient platform for health consultations.
CT4: In general, I believe that healthcare chatbots are very knowledgeable about health.
Benevolence trust25,29
BT1: I believe that healthcare chatbots provide services based on my interests.
BT2: If I require help, the healthcare chatbot will do its best to assist me.
BT3: The healthcare chatbot is interested in my well-being during the interaction.
Integrity trust25,29
IT1: The healthcare chatbot is truthful in its dealings with me.
IT2: I believe the healthcare chatbot is honest.
IT3: The healthcare chatbot would keep its commitments.
IT4: The interactions with the healthcare chatbot are sincere.
Users’ intention to adopt healthcare chatbots
23
UIAHC1: I am satisfied with using healthcare chatbots to obtain health consultation services.
UIAHC2: I plan to use the healthcare chatbot in the future.
UIAHC3: Using a healthcare chatbot would be a good idea when I feel unwell.
UIAHC4: I am willing to accept the health consultation services provided by the healthcare chatbot.
The experimental process
Heterotrait–monotrait (HTMT)
BT
UIAHC
PF
PPR
PA
PEOU
PI
PU
IT
CT
BT
-
UIAHC
0.626
PF
0.458
0.457
PPR
0.315
0.432
0.272
PA
0.693
0.631
0.492
0.275
PEOU
0.634
0.650
0.646
0.279
0.589
PI
0.587
0.796
0.498
0.432
0.821
0.716
PU
0.594
0.808
0.487
0.312
0.659
0.780
0.828
IT
0.746
0.626
0.646
0.450
0.622
0.714
0.680
0.645
CT
0.356
0.816
0.460
0.463
0.626
0.616
0.838
0.819
0.483
-