
Abstract
Objective
To systematically evaluate the effects of mobile health (mHealth) interventions on bowel symptoms, self-care ability, and quality of life (QoL) in colorectal cancer patients after anus-preserving surgery.
Design
a systematic review and meta-analysis.
Methods
We comprehensively searched PubMed, Web of Science, Embase, Cochrane Library, Sinomed, CNKI, and Wanfang databases for randomized controlled trials (RCTs) from inception to September 2024. Study quality was assessed using the Cochrane risk-of-bias tool, and data were synthesized with RevMan 5.4. Sensitivity and subgroup analyses were performed to explore heterogeneity.
Results
Twelve RCTs involving 1,888 participants were included. The meta-analysis demonstrated that while mHealth interventions did not significantly improve bowel symptoms overall (SMD = -0.40, 95% CI [-1.22, 0.41]), they yielded significant enhancements in patients’ self-care ability (SMD=1.38, 95% CI [0.49, 2.27]) and QoL (SMD=0.96, 95% CI [0.51, 1.41]). Crucially, subgroup analyses revealed that: 1) a 6-month intervention duration was associated with a significant improvement in bowel symptoms, and 2) social-platform-based mHealth interventions were substantially more effective in boosting self-care ability and QoL compared to other formats (e.g., apps, websites). Sensitivity analysis confirmed the robustness of these findings.
Conclusion
mHealth interventions may be effective in enhancing self-care ability and QoL for colorectal cancer survivors after sphincter-preserving surgery, with particularly significant outcomes when interventions delivered via social media platforms or sustained for at least six months. These findings provide evidence-based guidance for clinical practice, but should be interpreted cautiously due to low-certainty evidence. High-quality randomized controlled trials are needed to confirm the results.
1. Introduction
Colorectal cancer (CRC) ranks as the third most common malignancy and the second leading cause of cancer-related mortality worldwide.1,2 Updated global cancer statistics for 2022 reported approximately 1.932 million new cases and 935,000 deaths, underscoring its substantial disease burden. 3 Advances in screening and treatment have improved the five-year relative survival rate to 65%. 4 However, sphincter-preserving surgery, while avoiding a permanent stoma, frequently leads to impaired anal function. Consequently, a significant proportion (48% to 82.6%)5,6 of patients develop long-term bowel dysfunction, often referred to as Low Anterior Resection Syndrome (LARS), which includes symptoms such as diarrhea, increased stool frequency, urgency, and fecal incontinence.7,8 These symptoms can persist for one year or longer, with 46.4% to 80% of patients still affected 4 to 7.5 years postoperatively.9,10 The persistent bowel symptoms severely impact patients’ quality of life (QoL). Frequent bowel movements and fecal incontinence can cause perianal skin breakdown, pain, and bleeding.11–13 Furthermore, patients often experience psychological distress, anxiety, depression, and social isolation, leading to significant declines in social, emotional, and role functioning.14–16 Therefore, patients with CRC after anus-preserving surgery are a group that needs to be highly concerned.
Current management of bowel dysfunction after anus-preserving surgery mainly relies on long-term self-care behaviors, including dietary regulation, pelvic floor muscle training, bowel habit training, and symptom monitoring. 17 Therefore, sustained behavioral support and continuous follow-up are essential.Traditionally, post-discharge self-management support relies on outpatient follow-ups and printed materials. However, this model is often hampered by missed appointments, lack of timely professional guidance, and poor patient adherence, ultimately failing to adequately improve bowel symptoms and QoL, particularly in areas requiring consistent practice like functional exercise and perianal skin care. 18 Mobile health (mHealth) management has emerged as a promising solution to these shortcomings. Utilizing technologies like text messages, mobile apps, social media, and wearable devices, mHealth delivers services such as health education, remote monitoring, and professional consultation. 19 Through the synergistic effects of diverse mechanisms—including behavioral change techniques, self-efficacy enhancement, patient activation, real-time monitoring with timely feedback, and social support with peer connections,20–23 mHealth interventions can systematically enhance patients’ postoperative health behavior adherence and self-care capabilities.This promotes early symptom recognition and management, alleviates psychological burdens in disease management, and ultimately translates into substantial improvements in quality of life and optimized clinical outcomes. Compared with other diseases, CRC survivorship care is especially dependent on patient engagement and adherence to complex self-management strategies, making it a highly relevant target for mHealth interventions.
The application of mHealth in the care of postoperative CRC patients is growing, with studies reporting benefits for QoL, psychological symptoms, and self-efficacy. 24 Nevertheless, the existing evidence is inconsistent. For instance, while some trials found no significant effect of mHealth on QoL, 25 others reported positive outcomes. 26 This inconsistency may be attributed to variations in intervention characteristics, such as duration and delivery platform. 27 Moreover, current systematic reviews and meta-analyses possess notable limitations. Some only narratively summarize mHealth forms and effects.28,29 while others are restricted by their scope—focusing only on physical activity and QoL without adequately addressing bowel symptoms and self-care ability 30 or including non-randomized studies and multiple cancer types, thereby diluting CRC-specific insights. 24 Consequently, a comprehensive and rigorous synthesis focusing specifically on the impact of mHealth on the critical outcomes of bowel symptoms and self-care ability in CRC patients after sphincter-preserving surgery is lacking.
To address these gaps, this study aims to: (1) systematically review the characteristics of mHealth interventions (e.g., duration, delivery platform) for CRC patients after sphincter-preserving surgery; and (2) conduct a meta-analysis to determine the effects of these interventions on bowel symptoms, self-care ability, and QoL. By synthesizing evidence from randomized controlled trials (RCTs), this research seeks to provide a robust evidence base for optimizing mHealth strategies in this patient population.
2. Methods
The systematic review and meta-analysis was registered in the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY) (registration number: INPLASY202490104), and it was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement. Ethical approval and informed consent were deemed unnecessary, as all data used in this study were sourced from previously published articles.
2.1 Search strategy
The search strategy was developed according to the principles of PICOS (Participants, Interventions, Controls, Outcomes, and Study Design), and the search was conducted using a combination of subject terms and free words, encompassing seven databases: PubMed, Web of Science, Embase, Cochrane Library, Sinomed, China Knowledge, and Wanfang. The search period extended from the establishment of the database to September 2024; the search language was limited to either Chinese or English, and the search expressions are shown in the supplementary material table S1. References from literature and reviews were also traced, and grey literature, such as dissertations and conference papers, was included to ensure a comprehensive search.
2.2 Study eligibility criteria
Studies were included in this review if they met the following criteria: (1) Study participants: patients diagnosed with colorectal cancer who have undergone anus-preserving surgery; (2) Interventions: studies in which mHealth interventions were implemented in the experimental group, including the application of wireless devices such as phone calls, text messaging, emails, mobile handsets, WeChat platforms, websites, apps, and wearable devices for health management of patients; (3) Control: usual care was provided in the control group; (4) Outcome indicators: studies that included at least one of the outcome indicators of bowel symptoms, self-care ability,and quality of life; (5) Study design: randomised controlled trials; (6) Literature: in Chinese or English. Studies were excluded if they met the following criteria: (1) patients with colostomy after colorectal cancer; (2) duplicate publications; (3) literature lacking full text or containing incomplete data; (4) literature with a methodological quality grade of C.
2.3 Study selection and data extraction
All identified records were imported into NoteExpress 4.1 software for duplicate removal. Subsequently, two reviewers independently performed an initial screening of the titles and abstracts of the studies according to the inclusion and exclusion criteria, and then reviewed the full text for further screening. The included studies were reviewed and compared; if there was ambiguity, two researchers determined whether the study was included by discussing each other or consulting a third researcher.
Two reviewers independently extracted data using a standardized, pilot-tested data extraction form, which was developed based on the Cochrane Handbook recommendations. Information extracted included the first author, year of publication, country where the study took place, sample size, sample characteristics (e.g., age, gender), form of intervention, duration and content of the intervention, outcome indicators and measurement tools. Disagreements, if any, were resolved through discussion with a third researcher.
2.4 Quality assessment
The risk of bias for each outcome was assessed by two independent reviewers using the Cochrane Risk-of-Bias Tool. If the evaluation results were inconsistent, a third researcher was consulted to assist in the decision. The assessment criteria were as follows: (1) generation of randomized sequences; (2) allocation concealment; (3) blinding of study participants and intervention implementers; (4) blinding of outcome measures; (5) completeness of data on outcome indicators; (6) possibility of selective reporting; and (7) other sources of bias.Each criterion was evaluated as either ‘low risk of bias’, ‘high risk of bias’, or ‘unclear’. If the above criteria were fully met, the likelihood of all types of bias would be considered minimal and graded as A. Partial fulfillment of the above criteria indicated that the likelihood of bias should be regarded as moderate and graded as B. Complete failure to meet the above criteria indicated a high likelihood of bias and was classified as C.
The overall quality of evidence for each outcome was assessed by two independent reviewers using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) approach, which classifies the evidence into four grades: ‘high, moderate, low, and very low’. The GRADEpro GDT software developed by the GRADE Working Group was used to grade the quality of evidence.
2.5 Data synthesis and analysis
Descriptive analyses were used to characterize the studies included. Data were analyzed and assessed for heterogeneity using Review Manager 5.4. The effect of the intervention was estimated by calculating the mean difference (MD) or standardized mean difference (SMD) and 95% confidence intervals (CIs)., For continuous data measured by the same instrument, the mean difference (MD) with 95% CI was employed to determine the effect of the intervention. In contrast, for continuous data measured by different instruments, the standardized mean difference (SMD) with 95% CI was calculated using the general inverse variance method.The overall effect was determined by utilizing a Z statistic with P < 0.05; if P < 0.05, the difference in overall effect was deemed statistically significant 31 ; Heterogeneity was quantified using the I2 statistic, with values of 0%–40%, 30%–60%, 50%–90%, and 75%–100% indicating negligible, moderate, substantial, and considerable heterogeneity, respectively. A fixed-effects model was used if heterogeneity was negligible (I2 < 50%); otherwise, a random-effects model was employed. 32 Subgroup analyses were conducted to explore the source of heterogeneity according to the duration and form of intervention; Sensitivity analyses were conducted by excluding one study at a time to evaluate the stability and reliability of the results of meta-analyses; And publication bias was assessed by funnel plot analyses.
3. Results
3.1 Search results and selection
A total of 1,189 related studies were retrieved in this study. After removing 345 duplicate studies and 509 unrelated studies, a total of 335 articles were left. According to the inclusion and exclusion criteria, a total of 12 studies were finally included. The literature screening process is shown in Figure 1. The flowchart of literature screening process.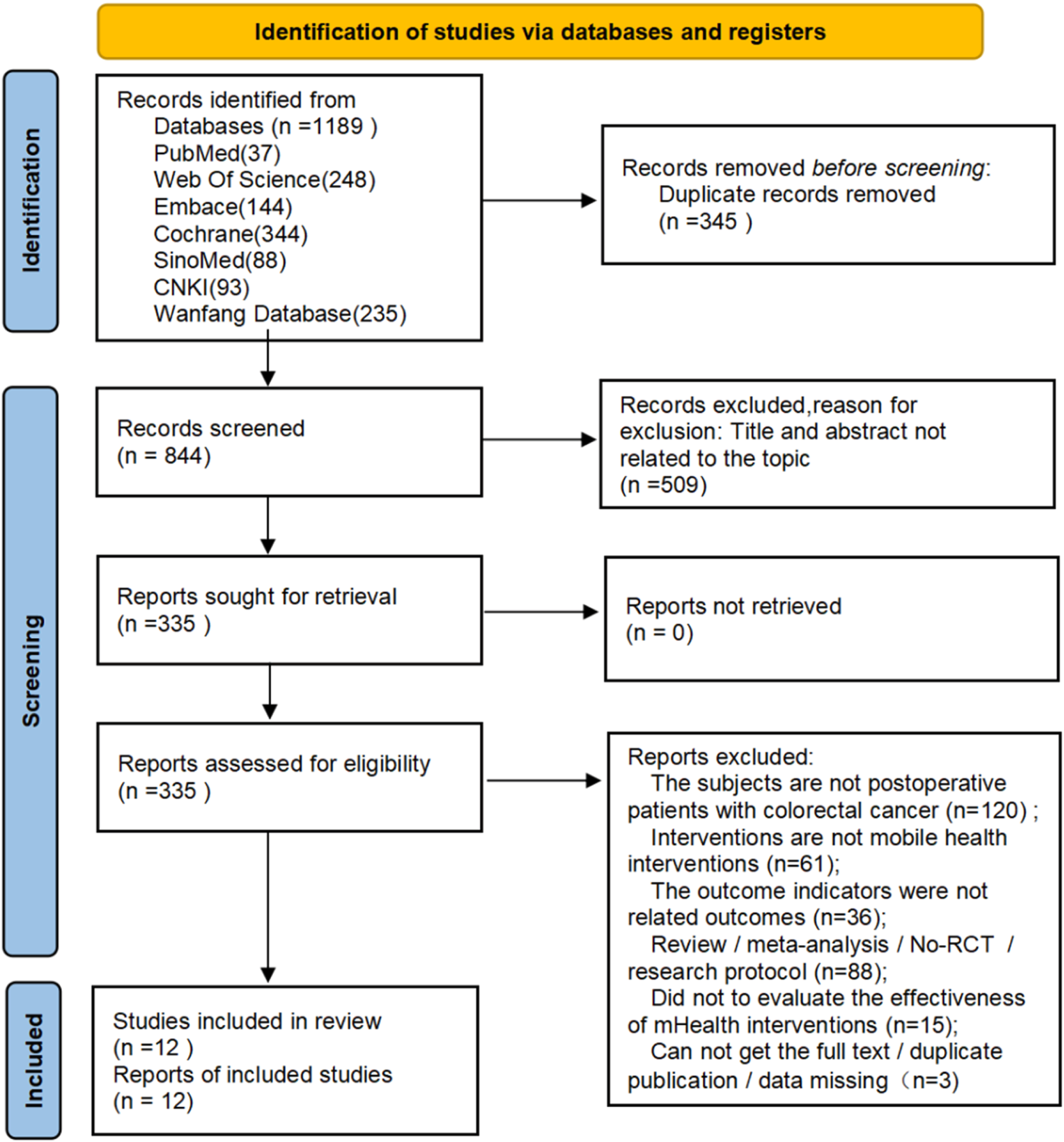
3.2 Description of included studies
3.2.1 Study characteristics
Basic characteristics of included studies.

ESCA: the exercise of self-care ability scale.
MSKCC-BFI: Memorial Sloan Kettering Bowel Function Instrument.
EORTC-QLQ-C30: the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Scale.
FACT-C: the Functional Assessment of Cancer Therapy Common Scale.
FIQL: the self-administered Fecal Incontinence Quality of Life Questionnaire.
Hart and Dobb Scale: Hart and Dobb Scale of Diarrhoea Severity.
WHO- QOLBREF: the Modified World Health Organisation Quality of Survival Measurement Scale.
EORTC: the European Organisation for Research and Treatment of Cancer.
SF-36: Medical Outcomes Study 36-Item Short Form Health Survey.
SQUASH questionnaire: Short Questionnaire to Assess Health-Enhancing Physical Activity.
SDS and SAS: Self-Rating Depression Scale and Self-Rating Anxiety Scale.
CIS + HADS: Checklist Individual Strength (CIS), Hospital Anxiety and Depression Scale (HADS).
FACIT-F: Functional Assessment of Chronic Illness Therapy Fatigue Scale.
3.2.2 Participants characteristics
A total of 1,888 participants were included in this research, including 932 in the intervention group and 956 in the control group. The number of participants in each study ranged from 41 to 625; the average age of patients after colorectal surgery ranged from 46.01 to 66.55 years; and most of the patients were male (1,337, 70.8%). 8 studies focused on colorectal cancer patients after surgery, 4 studies focused on rectal cancer patients after surgery, and two studies examined low and ultra-low rectal cancer patients after surgery. See Table 1.
3.2.3 The form and duration of mHealth intervention
Characteristics of intervention measures included in the study.
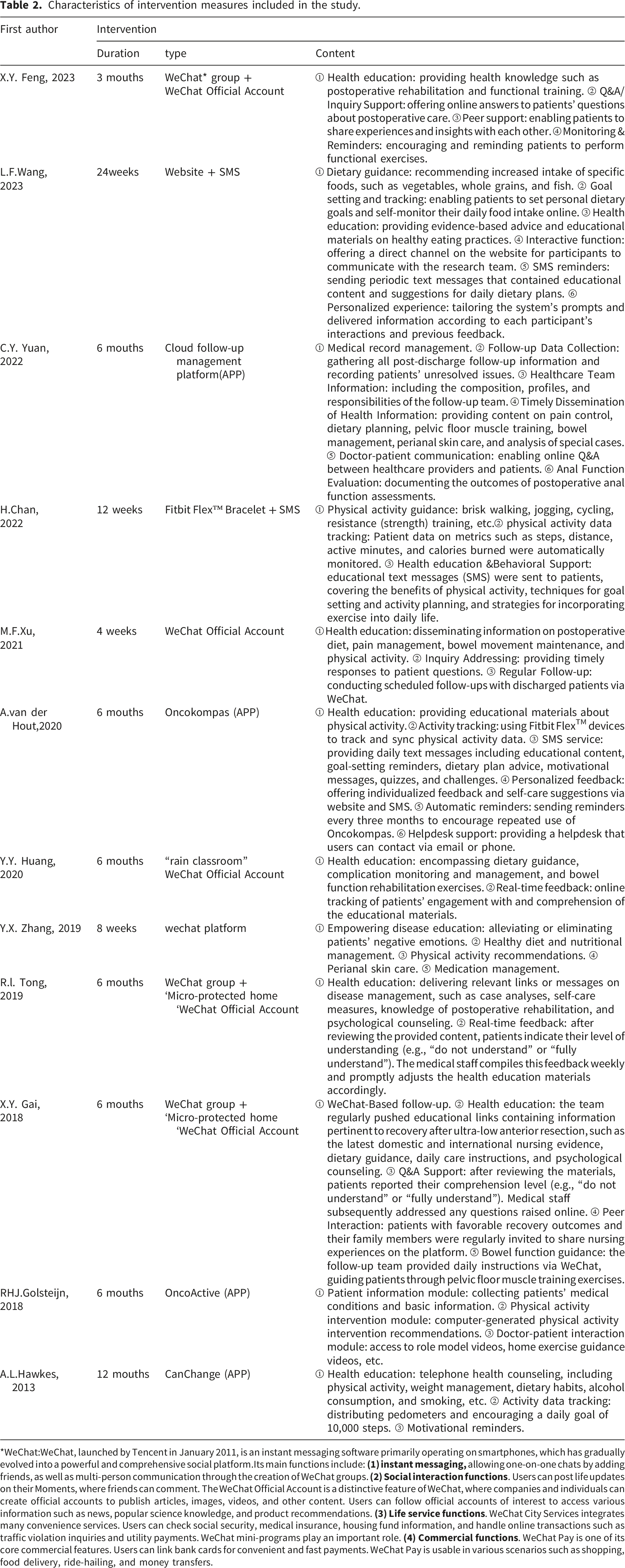
*WeChat:WeChat, launched by Tencent in January 2011, is an instant messaging software primarily operating on smartphones, which has gradually evolved into a powerful and comprehensive social platform.Its main functions include:
3.2.4 The content of mHealth interventions
(1) (2) (3) (4) (5) (6) (7) (8)
3.2.5 Characteristics of controls
All the patients in the control group received usual care. The responsible nurses carried out oral health education before discharge, including postoperative diet management, physical activity, defecation training, psychological counseling, etc., and issued a paper-based health education manual for follow-up by telephone or outpatient service. See Table 1.
3.2.6 Outcome measures
The studies assessed patients’ bowel symptoms, self-care abilities, and quality of life at the end of the intervention, and some of the studies measured patients’ postoperative complication rates, bowel training compliance, diarrhoea distress, psychological status, self-efficacy, and other outcome indicators. See Table 1. (1) (2) (3)
3.3 Risk of bias
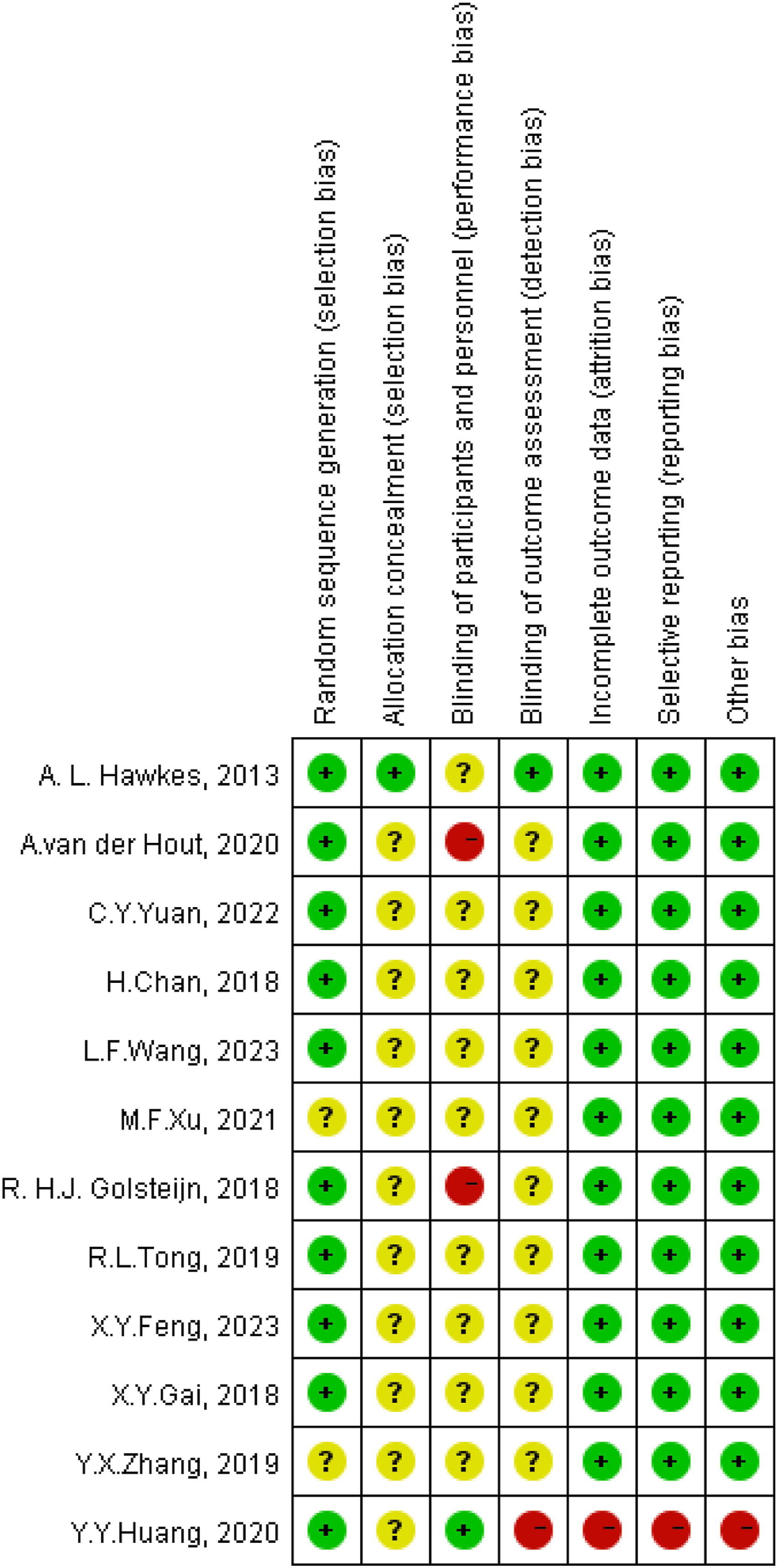
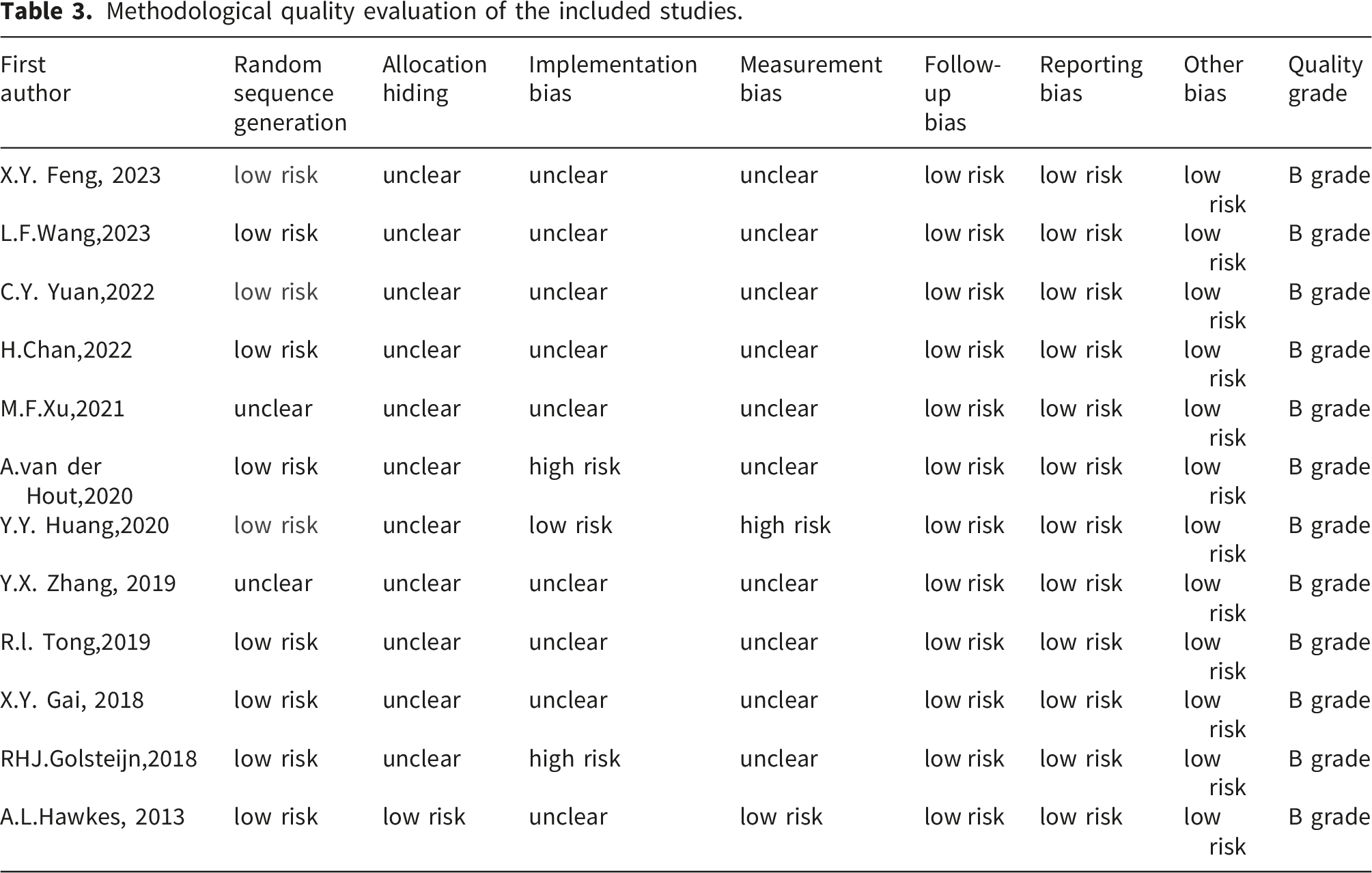
The risk of bias evaluation of the studies is shown in Figures 2 and 3 and table 3. 10 studies described the generation of random sequences in detail and were rated as low risk of bias, 2 studies did not describe the generation of random sequences were rated as unclear; only 1 study described allocation concealment, which was rated as low risk of bias; 3 studies described the implementation of blinding, of which 1 study was rated as low risk of bias, 2 studies were rated as high risk of bias, and the remaining 9 studies were not described were rated as unclear; 2 studies described the method of measurement, of which 1 study was rated as low risk of bias, 1 study was rated as high risk of bias, and the remaining 10 studies were not described were rated as unclear; 12 studies reported the rate of lost to follow-up, which was rated as low risk of bias; 12 studies reported the outcome metrics in full, which was rated as low risk of bias; and 12 studies did not have any other bias-shifting factors, which was rated as a low risk of bias, and ultimately all 12 studies were rated B on the methodological quality assessment.The final grades for bowel symptoms, self-care ability, and quality of life bodies of evidence were very low, low, and low, respectively, as shown in supplementary material table S3. Risk of bias graph. Risk of bias summary. Methodological quality evaluation of the included studies.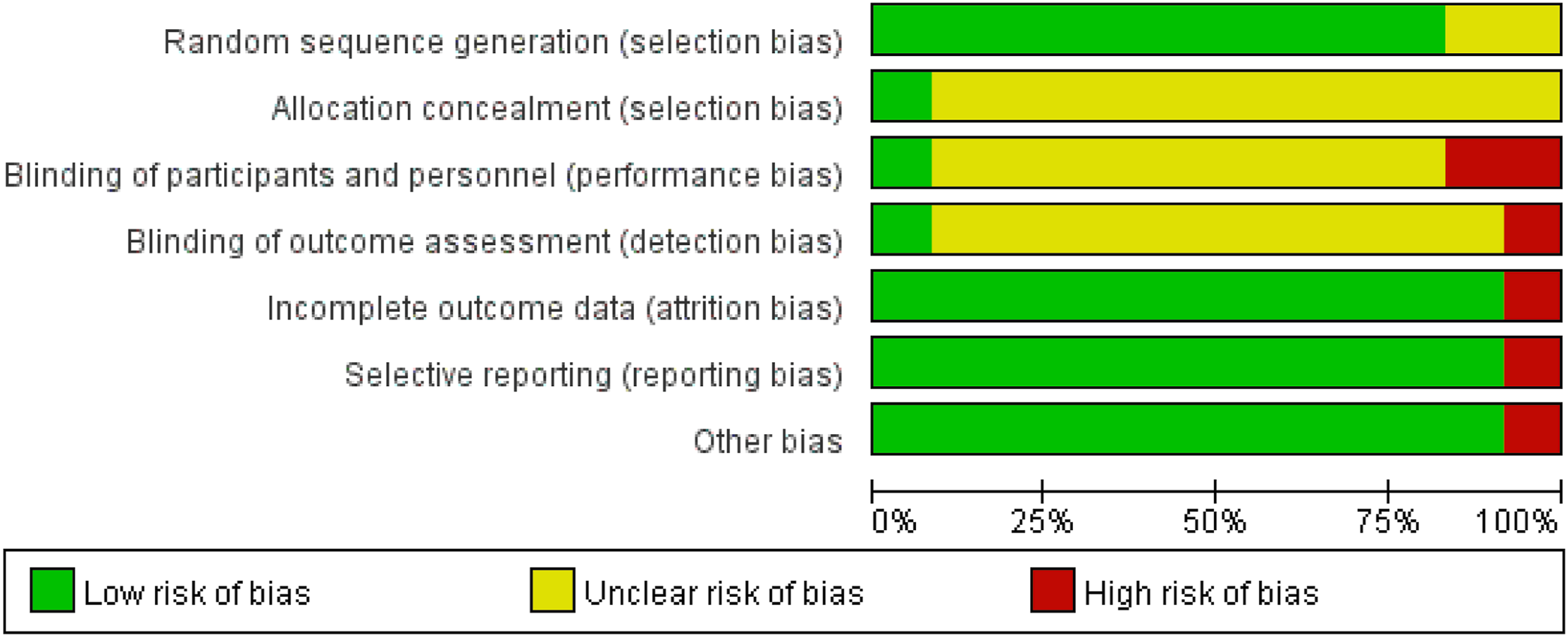
3.4. Meta-analysis results
3.4.1 Bowel symptoms
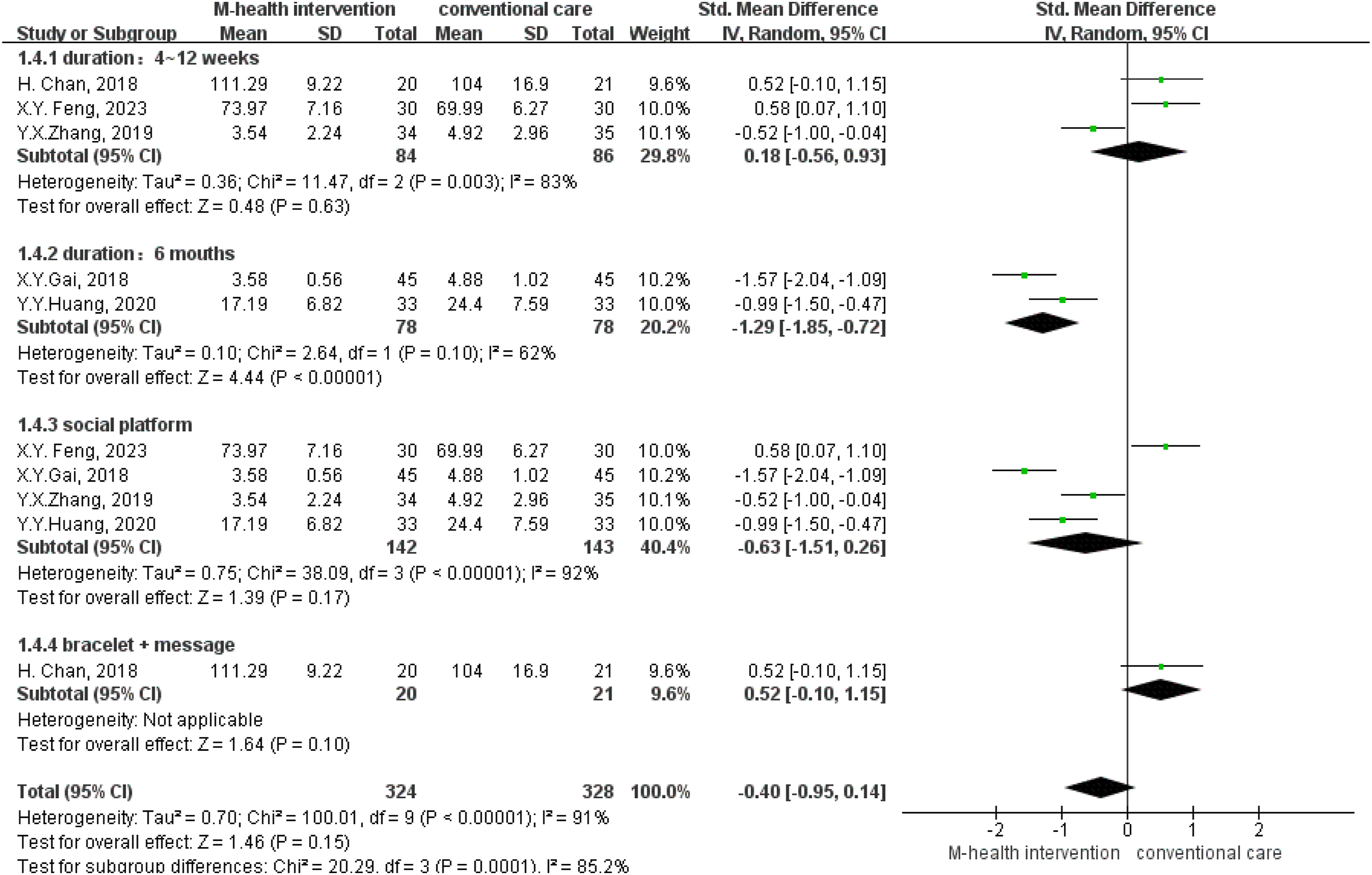
Five studies34,36,39,41,43 analyzed the effect of mHealth interventions on bowel symptoms in postoperative colorectal cancer patients. There was high heterogeneity among the studies (I2=92%, P<0.1); therefore, a random-effects model was used for data analysis. The results showed that mHealth interventions did not significantly improve bowel symptoms in postoperative colorectal cancer patients; the difference was not statistically significant (SMD = -0.40, 95% CI (-1.22, 0.41), Z=0.97, P=0.33), see Figure 4. Forest plot of bowel symptoms.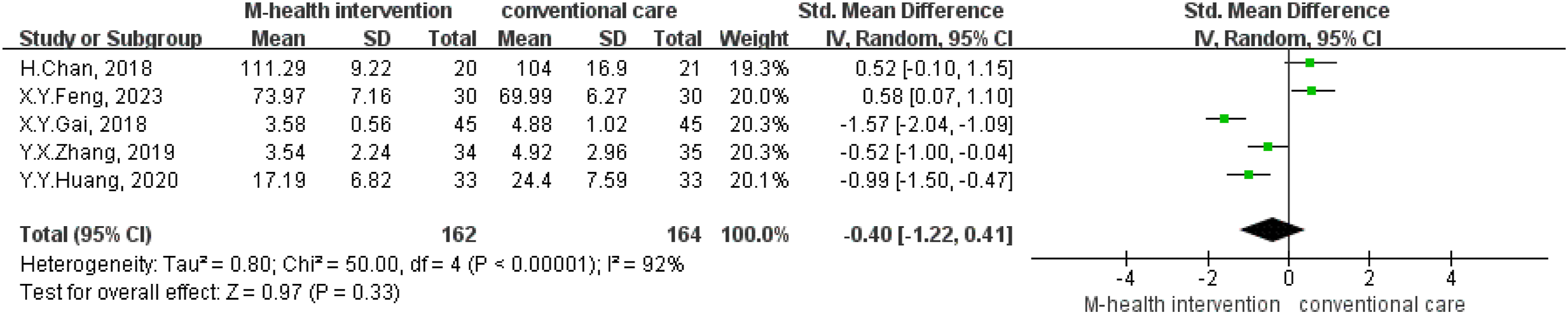
3.4.2. Self-care ability
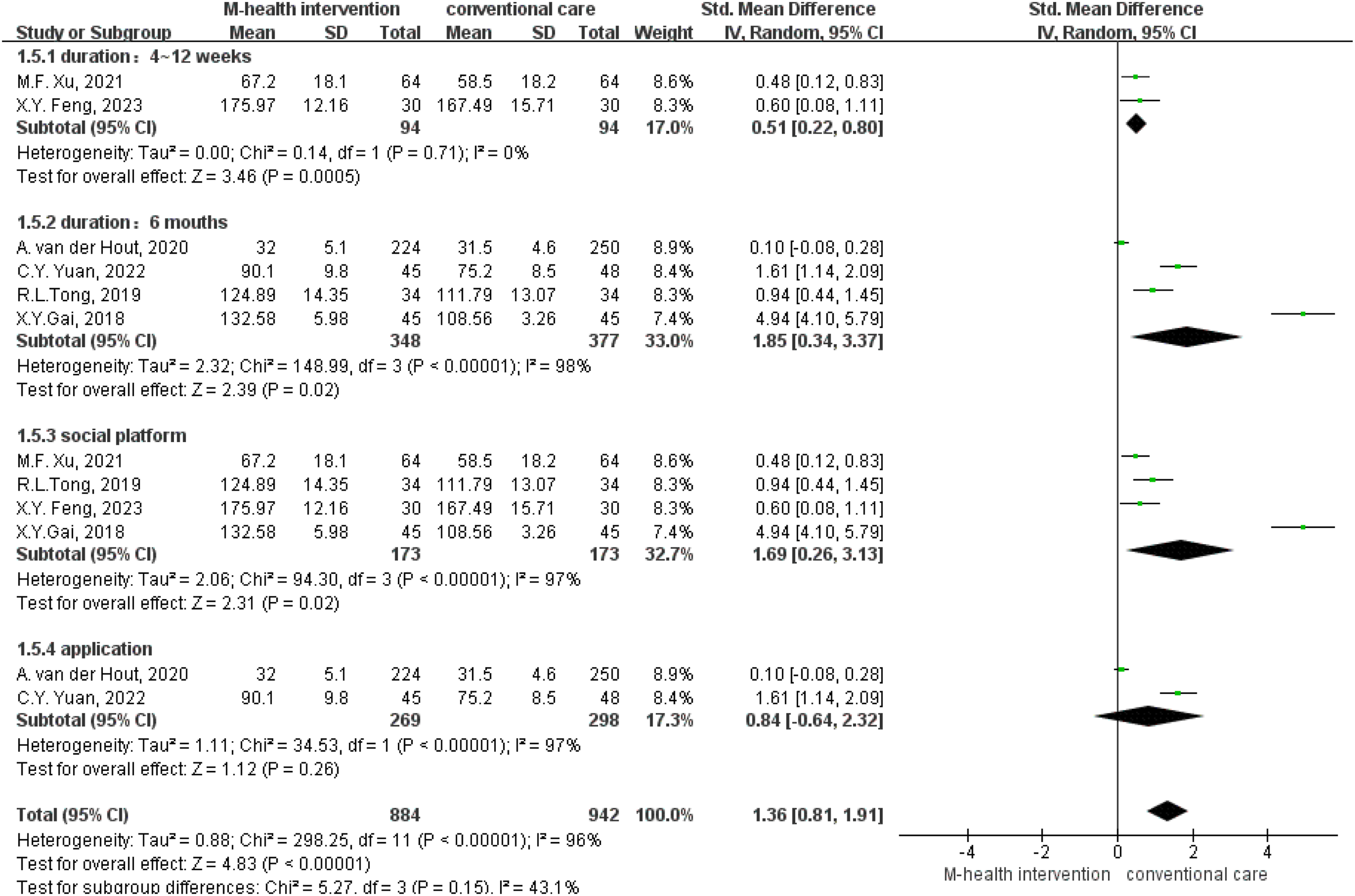
Six studies33,35–37,39,40 analyzed the effect of mHealth interventions on self-care ability in postoperative colorectal cancer patients. There was high heterogeneity among the studies (I2=97%, P<0.00001), therefore a random-effects model was used for data analysis. Results showed that mHealth intervention significantly enhanced the self-care abilities of patients, with statistically significant differences (SMD=1.38, 95% CI (0.49, 2.27), Z=3.04, P=0.002), see Figure 5. Forest plot of self-care ability.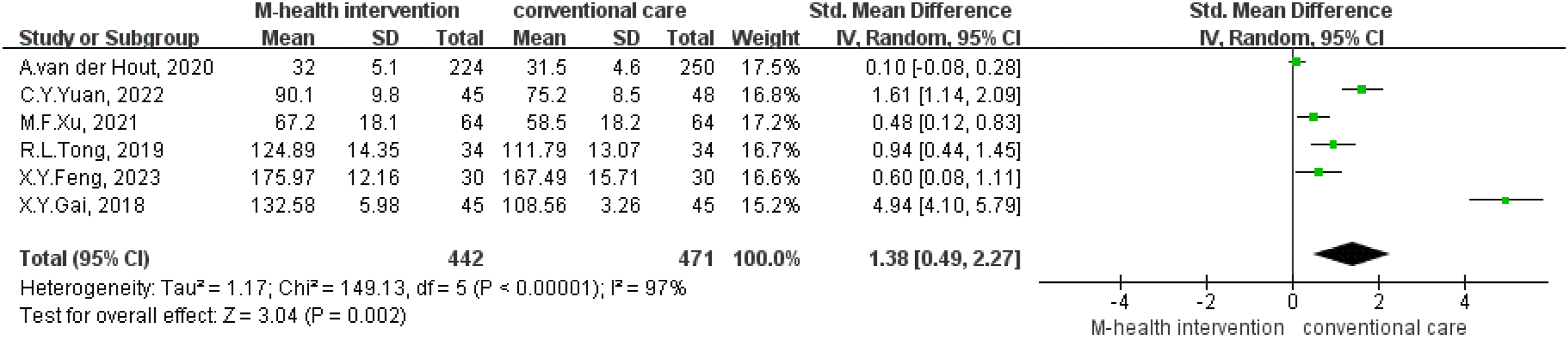
3.4.3. Quality of life
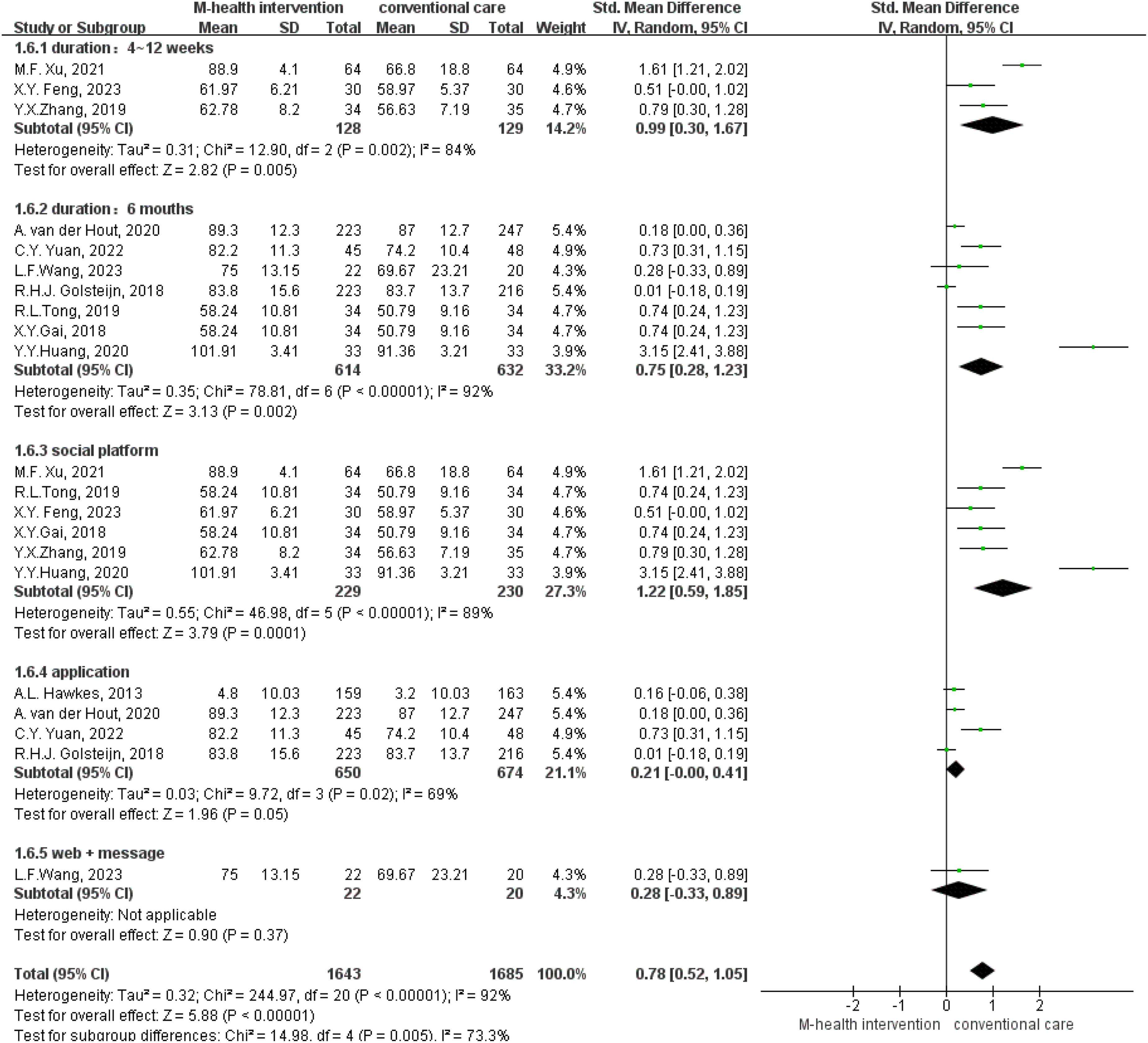
Eleven studies33–43 analyzed the effect of mHealth interventions on quality of life in postoperative colorectal cancer patients. There was high heterogeneity among the studies (I2=95%, P<0.00001), so a random-effects model was used for data analysis. Meta-analysis results showed that mHealth interventions significantly improved patients’ quality of life, with statistically significant differences (SMD=0.96, 95% CI (0.51, 1.41), Z=4.18, P<0.00001), see Figure 6 Forest plot of quality of life. Forest plot of subgroup-bowel symptoms. Forest plot of subgroup-self-care ability. Forest plot of subgroup-quality of life.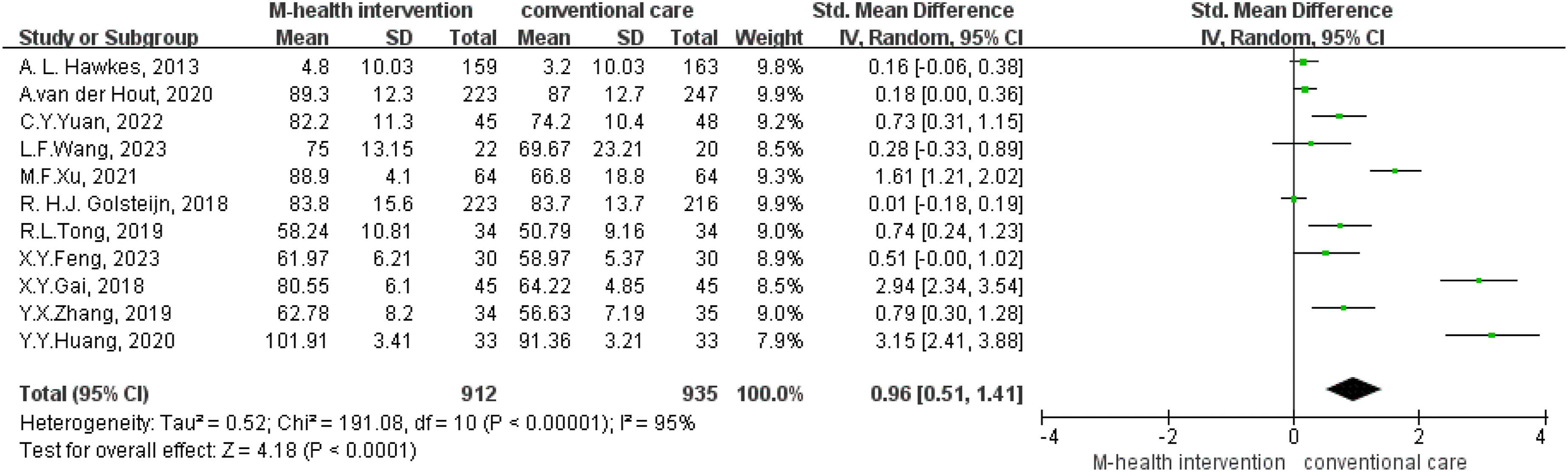
3.5 Subgroup analysis
(1) (2) (3)
3.6 Sensitivity analysis and publication bias
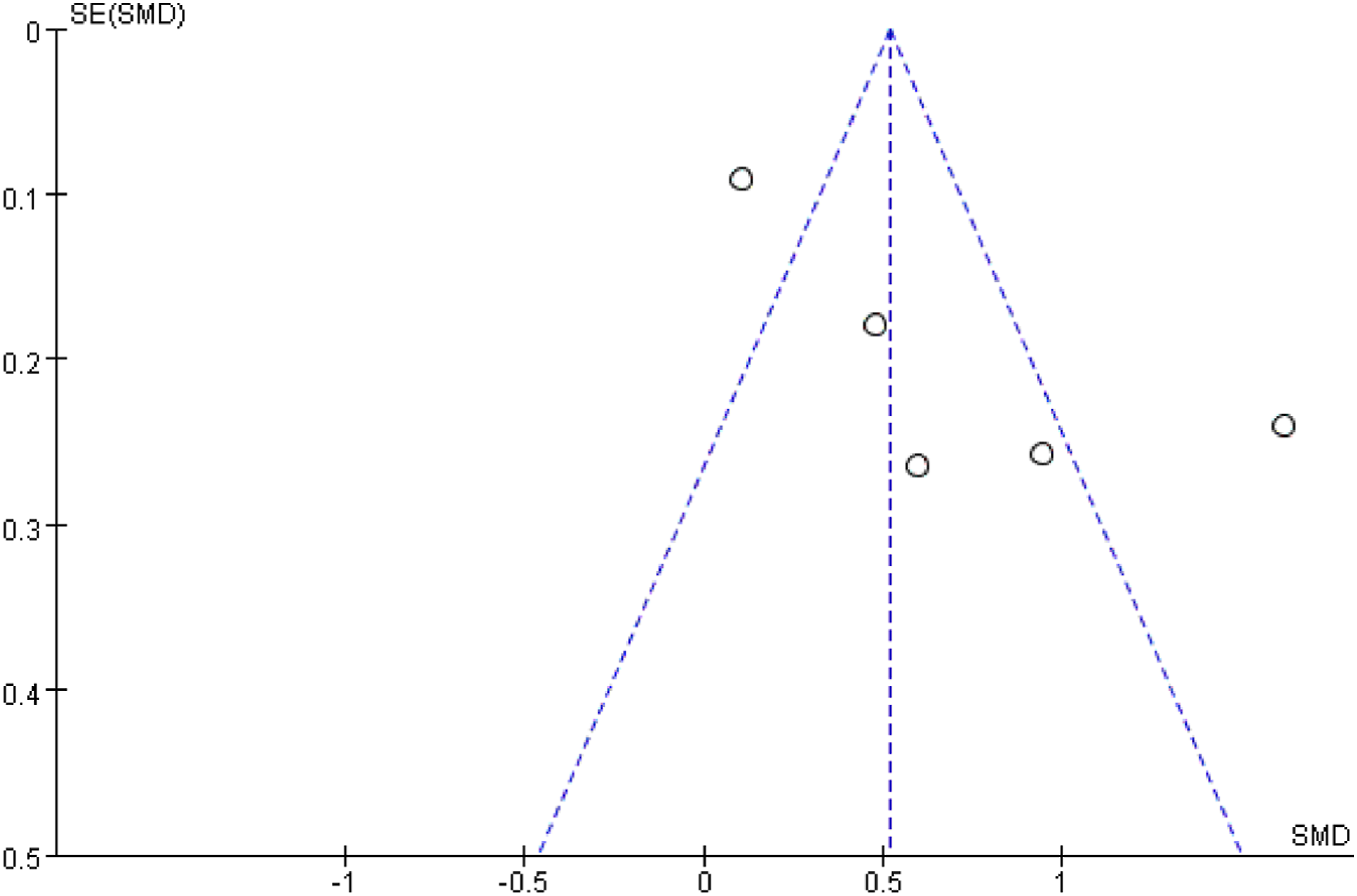
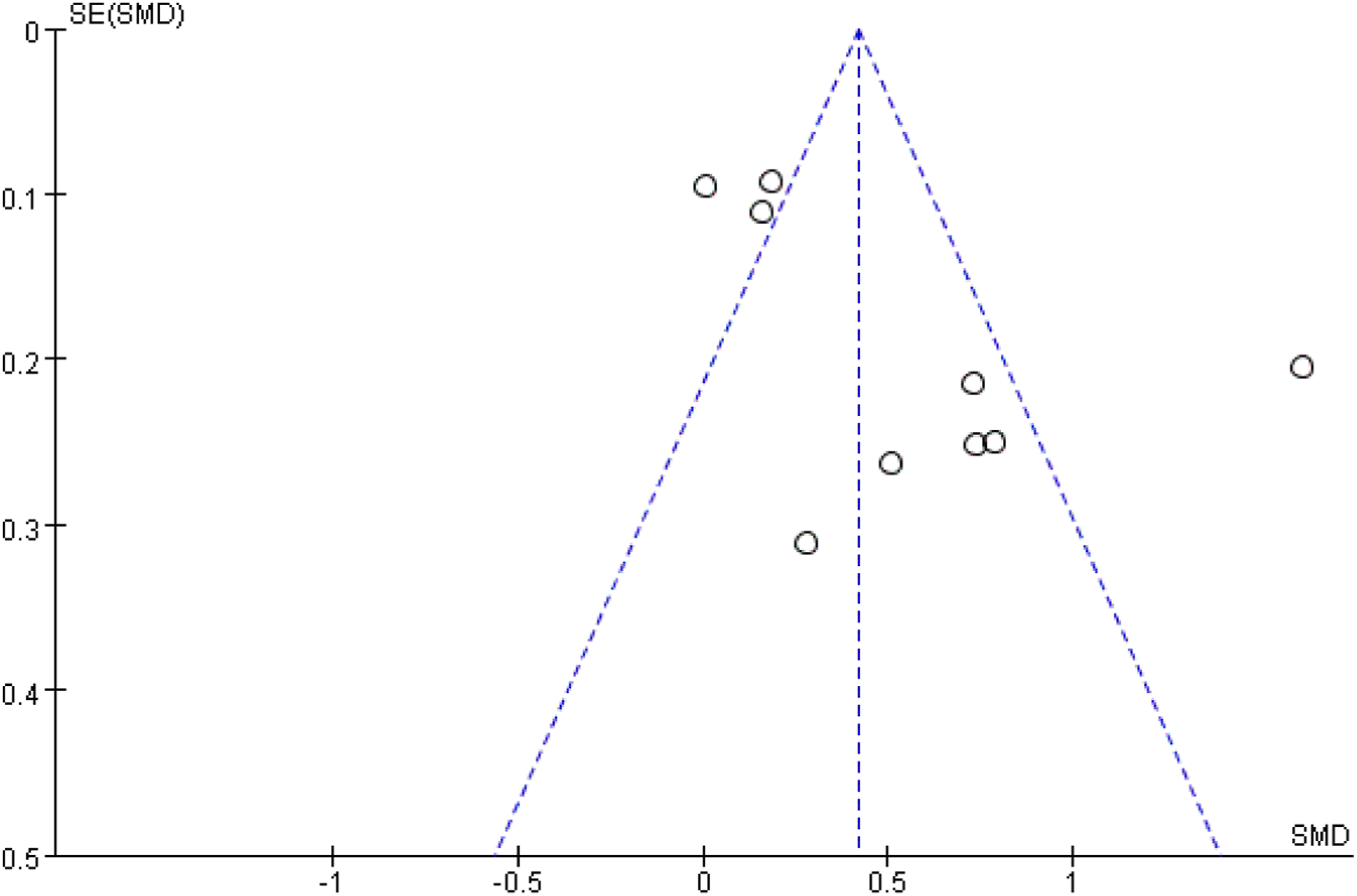
Based on the subgroup analyses above, the duration and form of mHealth interventions may be sources of heterogeneity in this study. Sensitivity analysis using a leave-one-out method showed no significant changes in the combined effect sizes, indicating that the meta-analysis results are relatively stable (see supplemental materials, Table S2). According to the Egger’s test (P=0.09) and funnel plot (Figure 10), the index of bowel symptoms is less likely to have publication bias. However, there may be some publication bias in the two indicators of self-care ability (Egger’s test: P<0.001, funnel plot see Figure 11) and quality of life (Egger’s test: P<0.001, funnel plot see Figure 12). Funnel plot of bowel symptoms Funnel plot of self-care ability Funnel plot of quality of life.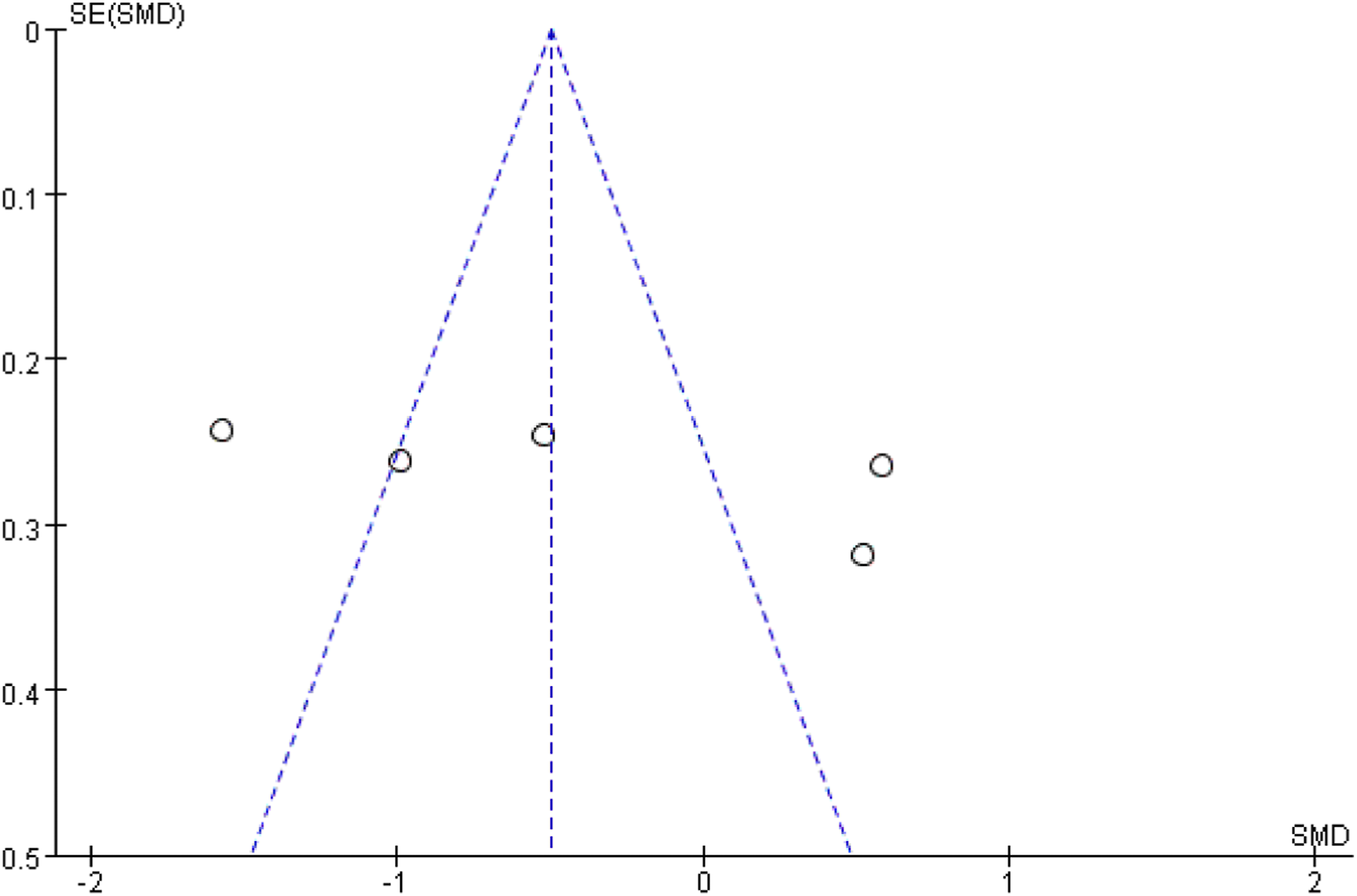
4. Discussion
This systematic review and meta-analysis of 12 RCTs suggests that mHealth interventions significantly improve self-care ability and overall quality of life in colorectal cancer survivors following sphincter-preserving surgery. Crucially, our subgroup analyses identified two key moderators of intervention success: delivery via social platforms and a minimum duration of six months. These findings have important implications for optimizing digital health strategies in this patient population.
4.1 Interpreting the non-significant effect on bowel symptoms
The overall meta-analysis did not demonstrate a significant improvement in bowel symptoms following mHealth interventions, a finding that contrasts with some prior studies. 44 We postulate that this discrepancy may stem from the chronic and complex nature of bowel dysfunction after sphincter-preserving surgery. The bowel symptoms often persist for over a year, 45 and the improvement depends on patients’ long-term acquisition and maintenance of behavioral modifications, including pelvic floor muscle exercises, dietary adjustments, and scheduled bowel movements. From the perspective of behavioral change mechanisms, effective symptom management requires the sustained application of behavioral change techniques. Through repeated reinforcement of core techniques such as self-monitoring (e.g., bowel movement diaries), goal setting, and immediate feedback, patients are assisted in gradually internalizing healthy behaviors as daily habits. 20 If the intervention lasts for a short period of time, it is insufficient to complete the full process of behavioral change and improvement of symptoms. Subgroup analysis indicated that interventions lasting six months were associated with greater improvement in bowel symptoms, suggesting the potential importance of a longer intervention duration. Nevertheless, this finding is derived from a small number of studies and should be regarded as exploratory and hypothesis-generating. Future research should be designed to prospectively test whether extending intervention duration indeed leads to better.
4.2 Enhancement of self-care ability
Our findings confirm that mHealth interventions significantly enhance self-care ability in post-surgical CRC patients, aligning with previous research.46,47, 28 mHealth interventions provide patients with continuous behavioral modeling and positive reinforcement through health education (e.g., perianal care skills, pelvic floor muscle training guidance), real-time progress monitoring, and remote professional feedback. Simultaneously, features such as timely reminders and goal-setting promote adherence to daily health behaviors, significantly enhancing patients’ self-efficacy (i.e., confidence and ability to manage their own disease) and activation levels (i.e., willingness and capacity to actively engage in disease management),21,22 thereby substantially enhancing self-care ability.
4.3 Improvement in quality of life
The positive impact of mHealth interventions on QoL is consistent with existing literature. 30 mHealth interventions integrate postoperative health education (including pelvic floor muscle training, bowel function rehabilitation, perianal care, pain management, and complication monitoring), personalized dietary and exercise guidance, along with dynamic physiological data monitoring and alerts. This approach helps patients establish standardized self-management routines, effectively alleviating bowel symptoms such as diarrhea and fecal incontinence; By establishing an online doctor-patient interaction module that provides immediate professional consultation and psychological support, it significantly reduces uncertainty and anxiety associated with illness, enhances treatment confidence and self-efficacy, thereby optimizing psychological adaptation; Simultaneously, peer support modules facilitate experience sharing and emotional exchange among patients, fostering mutual-aid communities to mitigate postoperative loneliness and social isolation. Combined with ongoing professional accompaniment, this approach builds a multidimensional social support network, thereby enhancing social integration and a sense of belonging. mHealth interventions collectively enhance patients’ overall quality of life through the synergistic mechanism of physiology-psychology-society.
4.4 The potential superior efficacy of social-platform-based delivery
An exploratory observation from our subgroup analysis was that social-platform-based mHealth interventions (e.g., WeChat groups) yield superior outcomes compared to other formats such as standalone apps or websites. mHealth interventions based on social platforms activate patients ' self-efficacy through information and emotional support, thus promoting positive health behavior changes. 48 Specifically, mHealth interventions based on social platforms not only provide patients with professional guidance on bowel symptoms but also enable them to access symptom management experiences shared by peers. This strengthens patients’ belief in their ability to manage symptoms and significantly enhances their self-efficacy. In terms of emotional support, patient communities effectively alleviate postoperative loneliness and social isolation through continuous interaction and shared values. When patients receive peer encouragement and feel understood, their psychological resilience and motivation for long-term persistence are strengthened. As the core mediating variable in this process, health self-efficacy transforms information and emotional support into actual behavior change motivation, through interaction and sustained engagement, thus promoting the transformation of health behavior and improving self-care ability and quality of life. 49 However, these findings were derived from a limited number of studies, and the observed benefits were likely driven by specific features, such as interactivity and sustained engagement, rather than by digital delivery alone. Therefore, these findings are exploratory and need to be confirmed by more rigorous experimental design in the future.
4.5 The eight components of mHealth interventions
In this study, we identified eight key components of mHealth interventions, including health education, dietary intervention, physical activity intervention, peer support, etc. These eight components together constitute the framework of mHealth interventions, which may also be applicable to the management of other chronic diseases. However, their integration is particularly relevant in the context of colorectal cancer survivorship after sphincter-preserving surgery. 48% to 82.6% of CRC patients after anus-preserving surgery often suffer from persistent and complex bowel dysfunction (e.g., urgency, incontinence, and frequent bowel movements), 9 which may last for years after surgery and is often accompanied by significant psychosocial burden, such as social isolation, stigma, and anxiety. 14 More importantly, the management of these symptoms mainly relies on long-term self-care behaviors, including dietary regulation, pelvic floor muscle training, bowel habit training, and symptom monitoring. 17 Therefore, CRC survivorship care is especially dependent on patient engagement and adherence to complex self-management strategies, making it a highly relevant target for mHealth interventions.
However, we can not isolate and quantify the independent effect of each individual component based on the available data. Our subgroup analyses provide some indirect insights. We found that mHealth interventions delivered via social platforms were more effective than those delivered through standalone applications or websites. These platforms typically incorporate interactive features such as peer support, real-time communication with healthcare providers, and continuous feedback, suggesting that interactivity may play a critical role in improving outcomes. In addition, interventions with a duration of at least six months were associated with better improvement in bowel symptoms, highlighting the importance of sustained engagement. However, this can only be regarded as inference and not as conclusion. Future research should employ more rigorous study designs (such as component-based network meta-analysis) to clarify the relative contributions of each component.
4.6 Limitations
Several limitations should be considered in this study. First, restricting the search to English and Chinese studies may have omitted relevant data from other regions, potentially limiting generalizability. Second, due to high risk of bias in included studies and substantial heterogeneity across outcomes, the overall certainty of evidence was low according to GRADE assessment.Therefore, the research findings should be interpreted with caution. Finally, the inaccessibility of some full texts and incomplete data may have influenced the comprehensiveness of our synthesis.
4.7 Implication
(1) Clinical Practice: Clinicians and healthcare organizations should actively integrate social-platform-based mHealth interventions into routine follow-up care for CRC survivors. Emphasis should be placed on maintaining intervention continuity for at least six months to maximize benefits, particularly for managing bowel symptoms. (2) Future Research: Subsequent studies should move beyond evaluating generic mHealth efficacy and focus on designing and testing interventions that are both prolonged and specifically target mechanisms of bowel symptom improvement. Incorporating mixed-methods approaches will help elucidate patient experiences and contextual factors influencing engagement and effectiveness. (3) Health Policy: Policymakers and administrators are encouraged to support the implementation of sustainable mHealth programs within standard care pathways. This includes developing infrastructure, ensuring reimbursement mechanisms, and establishing guidelines for the ethical and effective use of social media in clinical care.
5. Conclusion
This systematic review and meta-analysis demonstrates that mHealth interventions may be effective in enhancing self-care ability and quality of life for colorectal cancer survivors following sphincter-preserving surgery. An exploratory finding of this study is the identification of two key factors for optimizing intervention efficacy: the utilization of social-platform-based delivery and ensuring a minimum intervention duration of six months, the latter being critically important for improving bowel symptoms. These findings offer evidence-based guidance for clinicians and researchers aiming to implement effective digital health strategies in the supportive care of colorectal cancer survivors. However, given the low certainty of evidence, these conclusions should be interpreted with caution. High quality randomized controlled trials are needed in the future to confirm the results.
Supplemental material
Supplemental material - The effectiveness of mobile health interventions on bowel symptoms, self-care ability, and quality of life in colorectal cancer patients after anus-preserving operation: A systematic review and meta-analysis
Supplemental material for The effectiveness of mobile health interventions on bowel symptoms, self-care ability, and quality of life in colorectal cancer patients after anus-preserving operation: A systematic review and meta-analysis by Yaolan Wang, Yujie Li, Chun Zhang, Caili Li, Lan Li, Mingjun Huang in DIGITAL HEALTH
Footnotes
Acknowledgements
We thank the National Natural Science Foundation for funding this study
Ethical considerations
Ethical approval and informed consent were deemed unnecessary, as all data used in this study were sourced from previously published articles.
Authors contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Natural Science Foundation of China, Grant/Award Number: 72104157.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study was all from published literature. The datasets analysed during the current study are not publicly available due the confidentiality of the research but are available from the corresponding author on reasonable request.
Guarantor
Corresponding author (Mingjun Huang) is the guarantor.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.