
Abstract
Background
Digital health misinformation on social media and emerging AI platforms poses a growing challenge for healthcare systems. Community pharmacists are often the first point of contact for patients influenced by online health content, yet limited evidence exists from Saudi Arabia, where social media engagement is among the highest globally.
Objective
To examine how community pharmacists in Saudi Arabia experience digital health misinformation, including its sources, patient impacts, confidence in addressing misinformation, and training needs.
Methods
A descriptive cross-sectional online survey was conducted among licensed community pharmacists in Saudi Arabia between March and April 2025. Using a convenience-plus-snowball sampling strategy, A total of 768 completed survey responses from licensed community pharmacists were included in the analysis. These responses were obtained through an anonymous, nationally distributed electronic questionnaire. The survey explored exposure to misinformation, pharmacists’ confidence, and preferred training modalities. Descriptive statistics and regression analyses were used to identify predictors of key outcomes.
Results
Most pharmacists (89.6%) reported encountering patient-derived digital health misinformation, with 51.6% experiencing such encounters weekly or daily. Facebook (39.3%) and WhatsApp (27.7%) were identified as the most common sources, while 10% of encounters involved AI-generated content. Common misinformation themes included supplement misuse (27.1%) and concerns about medication safety (25.7%). Only 34.5% of pharmacists felt confident in identifying or correcting misinformation. Age, years of experience, and frequency of exposure were significantly associated with higher confidence and with perceived patient-behaviour impact. More than half (59.5%) supported formal training in misinformation management.
Conclusions
Digital misinformation is now a routine component of community pharmacy practice in Saudi Arabia and has tangible implications for patient behaviour and medication safety. Although confidence in managing misinformation was low, digitally active community pharmacists expressed strong readiness for targeted training. These findings underscore the need for structured educational initiatives and coordinated policy responses to strengthen digital health literacy and misinformation management within pharmacy practice.
Introduction
Health misinformation has grown into what the World Health Organization now defines as an infodemic, an overwhelming flood of information, both accurate and false, that makes it difficult for the public to identify trustworthy sources and reliable guidance. 1 Systematic reviews have shown that a substantial proportion of widely shared health content on social media contains inaccuracies,2,3 and analyses of online networks indicate that false information can spread more rapidly and more widely than verified facts. 4 These dynamics have important public health consequences, influencing how people understand health risks, make decisions about prevention and treatment, and interact with healthcare systems.5,6
The rapid development of generative artificial intelligence has added a new layer of complexity to this information environment. 7 Large language models can now produce convincing but inaccurate medical content, sometimes including fabricated citations and authoritative-sounding explanations. 8 Analyses of generative language models and automated influence operations have highlighted the potential for these tools to be used in large-scale production and targeting of misleading narratives, including those related to health.9,10 Whereas earlier forms of digital misinformation typically required substantial human effort for content creation and coordination, generative AI can dramatically increase the volume and apparent credibility of false material, making it more difficult to detect, verify, and correct.7–10
In clinical practice, the impact of digital health misinformation is increasingly visible. Social media and online platforms have been linked to vaccine hesitancy and the spread of anti-vaccination narratives,11,12 as well as to confusion about appropriate treatments and prevention during public health emergencies.2,6 Such influences can contribute to risky self-medication behaviours and suboptimal treatment decisions, particularly when misleading information appears to come from trusted peers or persuasive online communities.5,6 For pharmacists, this often translates into longer and more complex consultations, in which they must correct false beliefs, address patients’ concerns, and preserve the therapeutic relationship in the face of conflicting digital information.13,14 The growing number of patients arriving with internet printouts or AI-generated advice presents challenges that traditional pharmacy education and existing practice guidelines have not fully anticipated. 14
Leading pharmacy bodies, including the American College of Clinical Pharmacy and the International Pharmaceutical Federation, have recently emphasised that pharmacists should play a proactive role in combating health misinformation through evidence-based communication, patient education, and collaboration with other health professionals.15–17 As some of the most accessible members of the healthcare team, community pharmacists are well positioned to intervene directly at the point of care and to support patients in interpreting health information obtained online. 17 Fulfilling this role, however, requires specific competencies, including digital health literacy, critical appraisal of online sources, and patient-centred communication strategies that are explicitly tailored to misinformation-related encounters.18,19
Saudi Arabia provides a particularly relevant context for examining these issues. The country has high levels of social media use, with more than 80% of the population actively engaged on digital platforms, 20 and the national Vision 2030 initiative has accelerated the digitisation of healthcare services. 21 At the same time, the rapid expansion of digital health has outpaced the development of comprehensive regulatory frameworks to address the quality and reliability of health information circulating online. Existing studies have reported substantial levels of misinformation and misunderstanding regarding topics such as stem cell therapies and COVID-19 vaccination among segments of the Saudi population.22,23 However, little is known about how healthcare professionals, and community pharmacists in particular, perceive and respond to digital health misinformation in their daily practice. Notably, digital health literacy and misinformation management have not yet been explicitly incorporated into continuing professional development requirements by the Saudi Commission for Health Specialties. 24
Thus, the present study aimed to provide an initial, exploratory account of how digitally active community pharmacists in Saudi Arabia experience digital health misinformation. Specifically, it examined the sources and perceived impact of misinformation on patient behaviour, pharmacists’ confidence and response strategies, and their views on training and policy needs related to social media and AI-generated health information.
Methods
Study design and participants
This study used a descriptive, cross-sectional design to examine community pharmacists’ experiences with digital health misinformation in Saudi Arabia. Data were collected electronically between 15 March and 30 April 2025.
Target population
The study focused exclusively on licensed community pharmacists because they represent the primary point of contact for the public and routinely address patient inquiries influenced by online and social media health content. Eligible participants were registered with the Saudi Commission for Health Specialties (SCFHS) and were actively engaged in patient-facing activities such as medication dispensing, counselling, and therapeutic guidance. Pharmacists were expected to access social media at least on a weekly basis for professional or informational purposes. This expectation reflects current practice in Saudi community pharmacy settings, where routine digital engagement is common. Intern pharmacists, pharmacy technicians, and individuals working in non-patient-facing roles were excluded.
Sampling strategy
A convenience-plus-snowball sampling approach was used. Initial recruitment was conducted through several large community-pharmacy communication hubs, including national franchise networks and established professional digital platforms that routinely distribute information to pharmacists across the country. This process ensured broad, nationwide dissemination of the survey link. After completing the survey, participants were invited to share the link with eligible colleagues, generating additional recruitment waves through snowball sampling and allowing the survey to reach pharmacists who might not be connected to the initial distribution channels.
The target population of community pharmacists in Saudi Arabia was estimated at approximately 21,600.
25
The minimum required sample size for a cross-sectional survey was calculated using the single-proportion formula
Data collection and data management
The questionnaire was administered through Microsoft® Forms and distributed nationally via pharmacy societies, regional professional WhatsApp groups, LinkedIn® networks, and community pharmacy franchise communication channels. The link could be shared within these networks, generating additional recruitment waves typical of convenience-plus-snowball sampling. The platform allows only one submitted response per active browser instance, which reduces the likelihood of unintentional repeat submissions while preserving respondent anonymity. No personal identifiers, login credentials, or device-level metadata were collected, and all survey data were stored securely in encrypted form on university servers.
A total of 768 completed survey submissions from licensed community pharmacists were retained for analysis. Because Microsoft® Forms requires all mandatory items to be answered before submission, only complete entries appear in the dataset. As all items were mandatory in the online form, no missing values were present, and analyses were performed on the complete dataset (complete-case by design). Furthermore, the design does not allow verification of unique individuals across different devices or browser sessions. The distribution strategy through multiple independent networks enhanced the diversity of respondents and provided a broad snapshot of pharmacists’ experiences across the Kingdom.
Instrument development
The survey instrument was developed specifically for this study based on a review of published literature related to digital health literacy, misinformation exposure, and community pharmacy practice. Items were drafted to capture relevant constructs pertaining to pharmacists’ encounters with online health content and patient misinformation. Three senior community pharmacists with experience in digital health and survey methodology reviewed the draft instrument for content relevance, clarity, and alignment with study objectives. A pilot test was then conducted with 20 licensed community pharmacists from local practice networks to examine item coherence and comprehension. These pilot participants were not included in the final analysis. Feedback from both expert review and pilot testing resulted in minor refinements to item phrasing and order to enhance clarity and interpretability. The final questionnaire contained 18 items organised into five sections: (1) demographic and practice characteristics, (2) frequency and sources of misinformation encountered in practice, (3) perceived impact of misinformation on patient behaviours, (4) pharmacists’ confidence and response strategies, and (5) training and policy perspectives. The complete survey instrument is provided in Appendix A (Survey Instrument).
Ethical approval
The study protocol was approved by the Institutional Review Board of Umm Al Qura University (Approval No. HAPO-02-K-012-2025-03-2591) and adhered to the principles of the Declaration of Helsinki (2013 revision). The opening page of the survey described the study purpose, procedures, voluntary participation, and data-handling processes. Only respondents who selected ‘I agree’ proceeded to the questionnaire. No personally identifying information was collected, and all anonymised data were stored on password-protected servers accessible only to the research team.
Scoring methods
A composite score was constructed to quantify pharmacists’ perceptions of how digital misinformation influences patient behaviour. The score was derived from four items assessing whether patients refused prescribed medications due to misinformation, self-medicated based on information obtained from social media or AI platforms, changed their medication regimens based on unverified online sources, or expressed greater trust in social media influencers than in healthcare professionals. Each item was rated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), and the items were summed to produce a total score ranging from 4 to 20. Higher scores indicated a greater perceived impact of misinformation. These four items correspond directly to the outcomes reported in the Results section and served as the dependent variable in the linear regression model.
Statistical analysis
Descriptive statistics were used to summarise demographic and practice characteristics, with categorical variables reported as frequencies and percentages. The composite misinformation-impact score was treated as a continuous dependent variable, consistent with established practice for summed Likert-type scales. Visual inspection of histograms and residual plots did not indicate substantial departures from normality or homoscedasticity for the linear regression models. Ordinal logistic regression was used to examine predictors of pharmacists’ confidence in identifying misinformation. The proportional odds assumption was evaluated using model-based diagnostics and showed no evidence of violation. Regression results were presented as beta coefficients or odds ratios with 95% confidence intervals, and statistical significance was defined as p < .05. All analyses were conducted using RStudio (version 2024.9.1.394) with R version 4.4.2.
Results
Demographic and occupational characteristics
The analysis is based on 768 completed survey responses. The demographic characteristics of these responses are summarised as follows. The majority of participants were aged 36–45 years (41.1%), followed by those aged 46 and above (24.3%) and 26–35 years (21.6%). More than half of the participants were male (55.3%). In terms of professional experience, 38.3% had 6–10 years of experience and 27.1% had less than one year. A majority (56.3%) reported having received formal training on digital health literacy or misinformation management (Table 1).
Demographic and occupational characteristics.

n (%).
Characteristics of misinformation encountered by patients
Most pharmacists reported encountering misinformation from patients either rarely (38.0%) or a few times per week (32.3%), while 19.3% faced it daily. Facebook® (39.3%) and WhatsApp® (27.7%) were the most frequently cited platforms, followed by TikTok® (23.0%), Snapchat® (17.1%), and Twitter/X® (16.3%). The most common types of misinformation encountered involved misuse of supplements (27.1%), medication safety concerns (25.7%), and self-medication practices (23.4%) (Table 2).
Characteristics of misinformation encountered by patients.

n (%).
A multiple-choice item; Note: Percentages may exceed 100% because respondents could select more than one option.
Impact of misinformation on patient behaviour
Among participants, 40.9% agreed or strongly agreed that patients frequently refused prescribed medications due to misinformation. In terms of self-medication based on social media or AI information, 30.8% agreed or strongly agreed. About 39.9% agreed or strongly agreed they had encountered patients who changed their medication regimens based on unverified online sources. Regarding patient trust, 34.8% agreed or strongly agreed that patients expressed more trust in social media influencers than in healthcare professionals (Figure 1) (Table 3).
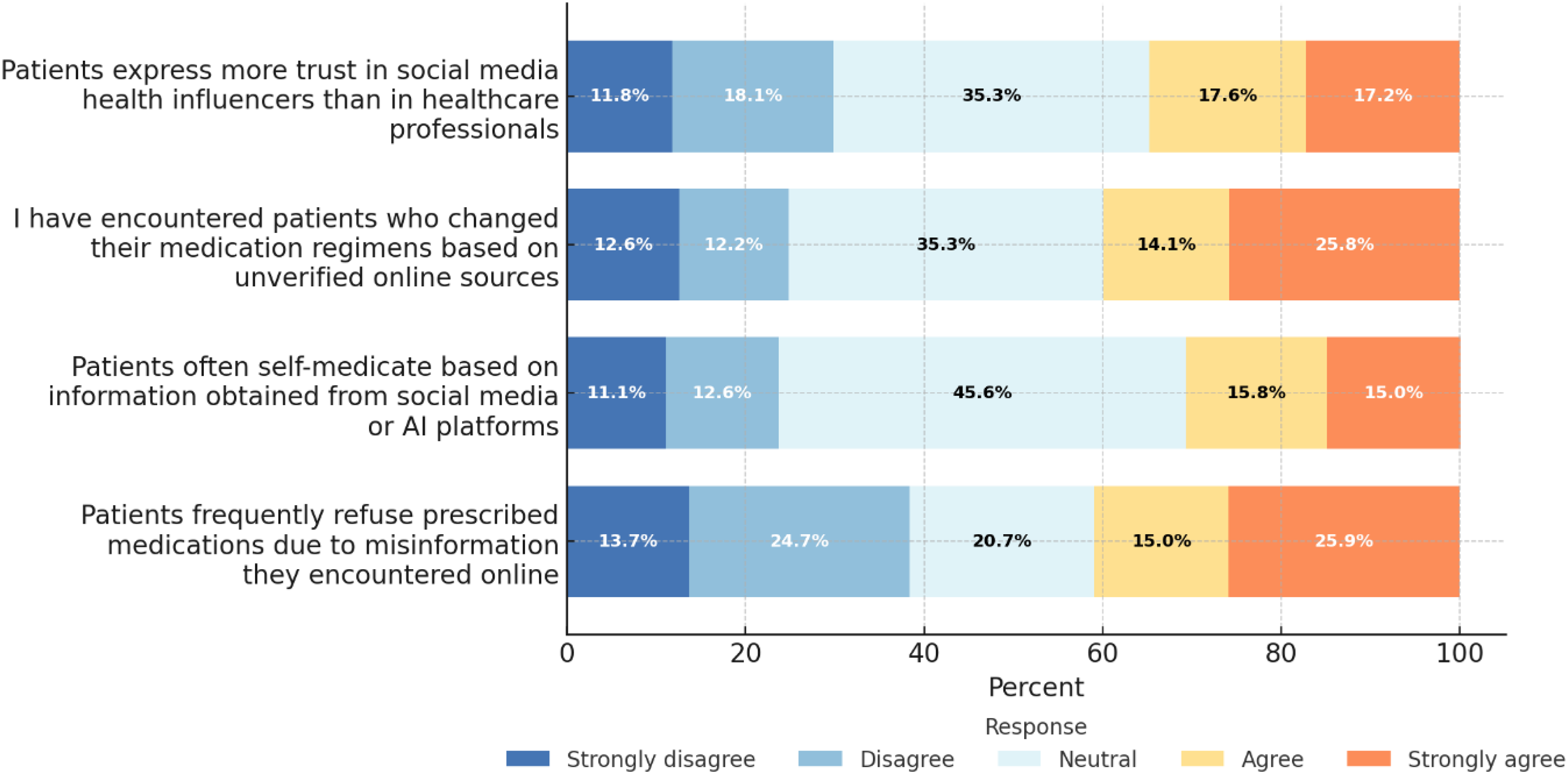
Pharmacists’ observations of patient behaviours influenced by digital health misinformation (N = 768).
Description of participants’ responses regarding the impact of misinformation on patient behaviour.

Predictors of higher impact of misinformation on patient behaviour
Age and years of experience were significantly associated with a perceived higher impact of misinformation. Compared to pharmacists aged 18–25, those aged 26–35 (beta = 1.32, 95% CI, 0.56 to 2.09, p < .001) and 46 and above (beta = 1.52, 95% CI, 0.71 to 2.33, p < .001) reported significantly higher perceived impact. Similarly, pharmacists with 6–10 years (beta = 1.25, 95% CI, 0.62 to 1.89, p < .001) and more than 10 years of experience (beta = 1.07, 95% CI, 0.41 to 1.73, p = .002) had significantly higher scores. Frequency of misinformation encounters was also significant, with higher perceived impact among those who encountered misinformation rarely (1–2 times/month) (beta = 1.16, 95% CI, 0.37 to 1.96, p = .004) or daily (beta = 0.97, 95% CI, 0.14 to 1.80, p = .022), compared to those who never encountered it (Table 4).
Predictors of higher impact of misinformation on patient behaviour as perceived by community pharmacists.

CI: confidence interval.
Pharmacists’ response to misinformation
Nearly half of the respondents (46.4%) reported a neutral level of confidence in identifying and correcting health misinformation, while 17.6% were confident and 16.9% were very confident. Others expressed low confidence, with 10.3% not very confident and 8.9% not confident at all. Regarding verification methods, the most commonly used approaches included checking official medical sources (33.5%) and searching Google or AI chatbots (23.8%). Commonly cited challenges included insufficient training (29.9%) and unclear regulatory guidelines (27.1%) (Table 5).
Description of pharmacists’ response to misinformation.

n (%).
Predictors of higher self-reported confidence
Years of experience and training status were significantly associated with higher self-reported confidence. Pharmacists with more than 10 years of experience had higher odds of confidence (OR = 2.00, 95% CI, 1.31 to 3.06, p = .001) compared to those with less than one year. Additionally, those who received formal training were less likely to report low confidence (OR = 0.57, 95% CI, 0.41 to 0.78, p < .001). Encountering misinformation more frequently was also linked to greater confidence: pharmacists who encountered it rarely (1–2 times/month) (OR = 2.13, 95% CI, 1.22 to 3.70, p = .008), a few times per week (OR = 1.78, 95% CI, 1.03 to 3.08, p = .040), or daily (OR = 2.81, 95% CI, 1.57 to 5.05, p < .001) were significantly more confident than those who never did (Table 6).
Predictors of higher self-reported confidence in identifying and correcting health misinformation presented by patients.

OR: odds ratio, CI: confidence interval.
Training and policy needs
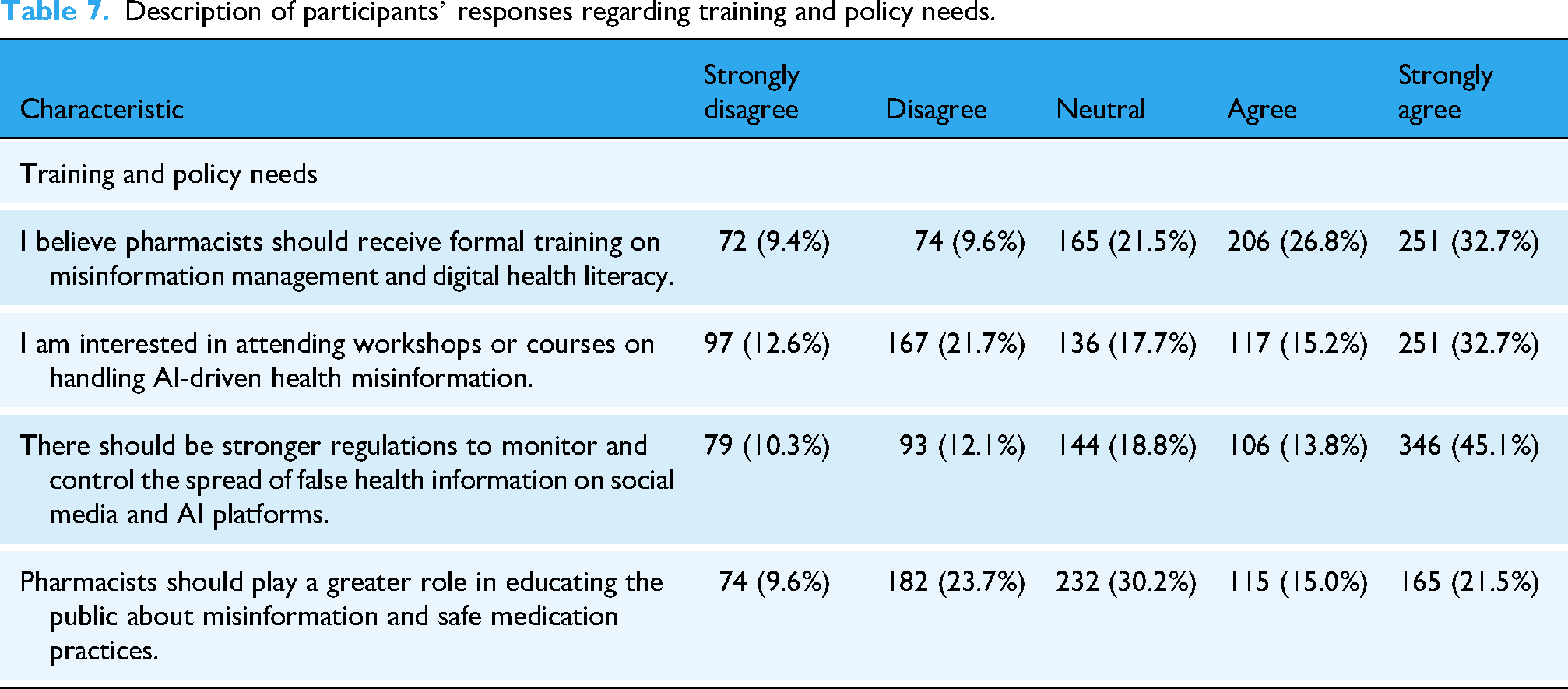
A majority of participants supported enhanced training and regulation, with 59.5% agreeing or strongly agreeing that pharmacists should receive formal training on misinformation management and digital health literacy. Similarly, 47.9% expressed interest in attending workshops or courses on this topic. Stronger regulations to control misinformation were supported by 58.9% of respondents, while 36.5% agreed or strongly agreed that pharmacists should play a greater role in public education (Figure 2) (Table 7).

Pharmacists’ training needs and policy perspectives regarding digital health misinformation (N = 768).
Description of participants’ responses regarding training and policy needs.
Discussion
This study suggests that digital health misinformation is a pervasive and routine challenge within community pharmacy practice among digitally active pharmacists in Saudi Arabia. Nearly all participants reported encounters with misinformation from patients, and most identified social media platforms as the main source. Facebook® and WhatsApp® predominated, with TikTok® emerging as a growing source of misleading content. These patterns mirror global work describing an ongoing ‘infodemic’, in which social media accelerates the spread of rumours and unfounded health advice and frequently outpaces official, evidence-based guidance.2,5,26 Such dynamics have been linked to vaccine hesitancy, confusion about preventive measures and increased anxiety among patients and the wider public.27,28
The present findings add a pharmacy-specific perspective from Saudi Arabia to this literature. They suggest that community pharmacists often occupy the point where digitally shaped beliefs, circulating through social networks and online communities, meet professional recommendations delivered in the pharmacy, positioning community pharmacies as a key interface between the wider information environment and the safe, effective use of medicines. 29
Prevalence, platforms and the Saudi digital context
The very high proportion of pharmacists in this study who reported exposure to misinformation, and the frequency of those encounters, indicate that digital misinformation is now embedded in routine community pharmacy consultations. Although direct quantitative comparisons with other countries should be made cautiously because of methodological differences, the exposure levels observed here are broadly similar to those reported in studies of pharmacists and other health professionals in Europe and North America.29–31
The platforms most often cited by participants reflect the digital communication landscape of Saudi Arabia, where messaging and social networking applications are widely used for health-related information. National surveys have documented extensive engagement with platforms such as WhatsApp, Facebook and Twitter/X during the COVID-19 pandemic and highlighted related challenges with misinformation and public trust.32,33 Concerns have also been raised about conflicting advice on vaccines and antimicrobial use circulating via these channels and its potential to undermine public health initiatives.32,34 The present results are consistent with these observations and suggest that community pharmacists in Saudi Arabia are routinely required to interpret, evaluate and respond to content that patients have encountered within a complex and sometimes contradictory digital information ecosystem.35,36
Emerging role of AI-generated content
Only a minority of pharmacists in this sample explicitly identified AI-generated content as a source of patient misinformation, yet its presence in consultations is notable. Recent evaluations of large language models and other generative AI tools have shown that they can produce highly plausible but factually inaccurate or decontextualised health information and may therefore contribute to the wider infodemic when used without appropriate safeguards (Spitale et al., 2023; Germani et al., 2024). Studies examining models such as ChatGPT have demonstrated that, while they can provide helpful overviews on some topics, they may also omit important qualifiers, misinterpret evidence or reproduce outdated or incorrect guidance.37,38
The relatively low proportion of pharmacists in this study who recognised AI-generated misinformation may reflect limited patient uptake of such tools, reluctance to disclose their use or the difficulty of determining whether a given message originated from an automated system. Given projections of rapidly increasing public adoption of generative AI for health information, it is plausible that AI-originated misinformation is currently under-recognised rather than genuinely rare.39,40 This reinforces the need for pharmacists to develop skills in identifying characteristic features of AI-produced content and in discussing the strengths and limitations of these tools with patients as part of routine counselling.41,42
Impact on clinical practice and patient behaviour
The influence of digital misinformation on patient behaviour was apparent across multiple facets of community pharmacy practice in this study. Pharmacists reported encounters with patients who refused prescribed medications, initiated self-medication or modified existing regimens on the basis of online claims. Such behaviours mirror patterns documented internationally, where misinformation has been associated with poor adherence, unsafe self-treatment and delays in seeking professional care.29,43 For community pharmacists, these behaviours translate into more complex consultations in which they must assess the reliability of patients’ information sources, correct inaccurate or incomplete understandings and maintain trust while recommending safer alternatives. 44
The perception among roughly one-third of pharmacists that some patients place greater trust in social media influencers than in healthcare professionals is particularly concerning and echoes reports from the COVID-19 period of shifting trust away from expert guidance.2,45,46 When patients arrive with strong prior beliefs shaped by online communities, conventional information provision is often insufficient. Pharmacists require advanced communication skills to explore patients’ concerns, acknowledge the emotional and social dimensions of their digital experiences and gradually re-anchor discussions in evidence-based recommendations.43,47
In this study, the composite patient behaviour impact score provided a quantitative summary of pharmacists’ perceptions of how strongly misinformation affects patient decisions. Regression analyses indicated that higher impact scores were associated with specific pharmacist characteristics and patterns of exposure reported in the Results section. Although this composite measure is exploratory and has not yet undergone full psychometric validation, the observed gradients are consistent with research in other professional groups where differences in age, experience and digital exposure have been linked to variation in perceived challenges and in digital health literacy.48,49 These patterns suggest that some subgroups of pharmacists may experience the consequences of misinformation as particularly disruptive and that tailored support for those at earlier stages of their careers or with heavier digital exposure may be warranted.
Community pharmacists’ role, confidence and digital health literacy
The present findings support a growing body of work that positions community pharmacists as front-line actors in responding to digital health misinformation. Prior studies have documented that pharmacists and pharmacy teams are frequently consulted about information patients encounter online but often feel underprepared to address misleading or conflicting claims, particularly when they relate to contentious topics such as vaccines or novel therapies.44,50,51 The relatively low confidence levels observed in this study, with only about one third of pharmacists feeling adequately equipped to manage misinformation, are consistent with this broader pattern and align with the regression findings that showed higher confidence among those who had received relevant training.47,52
Evidence from other settings suggests that targeted training in digital health literacy, critical appraisal and risk communication can improve pharmacists’ self-efficacy and performance when engaging with misinformation-influenced patients.16,47 More generally, digital health literacy is increasingly recognised as a core competency for healthcare professionals, encompassing not only technical skills but also the ability to evaluate online sources, interpret algorithmically curated content and support patients in navigating digital tools.48,53 Studies in nursing and other professional groups indicate that structured training programmes can enhance digital competence and, in turn, improve the quality of patient counselling and engagement.49,54,55 The present results suggest that similar approaches may be beneficial in community pharmacy practice in Saudi Arabia, where pharmacists already face high expectations from patients regarding the interpretation of online information.16,56
Policy implications and future directions
The strong support expressed by pharmacists in this study for enhanced training, clearer regulatory guidance and better access to trustworthy digital resources indicates that they view misinformation management as a shared institutional responsibility rather than an individual burden. This perspective is closely aligned with the World Health Organization's infodemic management framework, which emphasises coordinated monitoring of the information environment, capacity building for health workers and collaboration with multiple stakeholders to counter harmful content.57–59 The framework also highlights the importance of ethically grounded social listening, rapid detection of misinformation trends and timely, authoritative counter-messaging.60,61
In the Saudi context, these findings suggest several practical directions that link directly to the training and policy needs identified in the Results. National and professional bodies could consider integrating competencies related to digital health literacy, online risk communication and responsible use of AI into undergraduate curricula, licensure requirements and continuing professional development.36,62 Previous work in Saudi Arabia has highlighted both the promise and the challenges of using social media for health communication, including concerns about misinformation, limited training in digital communication and the heavy workloads that constrain pharmacists’ ability to engage extensively in patient education.32,35,56 Providing pharmacists with curated repositories of reliable digital resources, structured protocols for responding to misinformation and, where appropriate, access to validated decision-support tools may help to standardise responses and reduce the cognitive burden on individual practitioners.63,64
Future research should build on this exploratory work by including pharmacists with lower levels of digital engagement, employing probability-based sampling where feasible and incorporating validated measures of digital health competencies and misinformation-related outcomes. 48 Qualitative studies with pharmacists and patients could further elucidate how misinformation is negotiated in consultations, how trust is built or eroded in digitally saturated environments and how AI tools are being used in practice.50,51 Within these constraints, the present study provides an early, context-specific snapshot of how digitally active community pharmacists in Saudi Arabia experience and respond to digital health misinformation and identifies educational and policy levers that could support them in this evolving role.
Study limitations
This exploratory study has several limitations that affect how the findings should be interpreted. The sample was obtained through non-probability, convenience-plus-snowball recruitment and was restricted to licensed community pharmacists who reported at least weekly professional or informational use of social media. This approach may have over-represented digitally engaged pharmacists and under-represented those with limited online activity, so the results are not statistically representative of all community pharmacists in Saudi Arabia. Furthermore, as with all anonymous online surveys, there remains a possibility that a respondent could complete the questionnaire more than once using a different device or browser. Efforts taken during data collection substantially reduced the likelihood of duplication. This possibility is considered minimal to have influenced the observed patterns. The anonymous, self-administered online format also means that responses are subject to recall and social desirability bias, and although the survey platform limited submissions per device and required completion of core items, duplicate or ineligible entries cannot be ruled out completely. In addition, the cross-sectional design precludes causal inference about relationships between exposure to misinformation, confidence and perceived patient behaviours. Also, platform-specific personal usage intensity was not measured, limiting the ability to assess whether misinformation recognition differs by pharmacists’ own platform use. Finally, although the questionnaire was informed by literature, expert review and pilot testing, the measures, including the composite patient behaviour impact score, have not undergone full psychometric validation. The findings should therefore be viewed as preliminary and hypothesis generating rather than definitive.
Conclusion
This exploratory survey provides an initial account of how digitally active community pharmacists in Saudi Arabia perceive and experience digital health misinformation in daily practice. Encounters with misinformation were frequent, and pharmacists reported clinically relevant consequences such as treatment refusal and unsupervised changes to medication regimens, alongside a perception that some patients place considerable trust in social media influencers. Despite prior training being relatively common, only a minority felt confident addressing misinformation, and many expressed a need for further education and clearer institutional or regulatory support. Given the non-probability, self-selected sample and reliance on self-report, these findings cannot be generalised to all pharmacists in Saudi Arabia or treated as precise estimates of the prevalence or impact of AI-generated misinformation. Nevertheless, the results provide baseline evidence of emerging pressures on community pharmacy practice and highlight priorities for intervention, particularly in digital health literacy, infodemic management and communication skills. Future research using more rigorous sampling, validated instruments and longitudinal or interventional designs is needed to confirm these findings and identify the most effective educational and organisational strategies.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261428231 - Supplemental material for Digital health misinformation in pharmacy practice: A foundational cross-sectional survey of Saudi pharmacists’ experiences with social media and AI-generated health information
Supplemental material, sj-docx-1-dhj-10.1177_20552076261428231 for Digital health misinformation in pharmacy practice: A foundational cross-sectional survey of Saudi pharmacists’ experiences with social media and AI-generated health information by Mohammed M Aldurdunji in DIGITAL HEALTH
Footnotes
Acknowledgments
Appreciation is extended to the community-pharmacy organisations and professional groups that facilitated survey circulation via their internal platforms.
Ethics approval and consent to participate
Approval was obtained from the Biomedical Research Ethics Committee, Umm Al-Qura University (Approval No. HAPO-02-K-012-2025-03-2591). Electronic informed consent was obtained from all participants.
Contributorship
Study conceptualisation and methodology were undertaken by M.M. Aldurdunji. Data curation, cleaning, and formal analyses were performed by M.M. Aldurdunji. Figures and tables were prepared by M.M. Aldurdunji. The manuscript was drafted and revised by M.M. Aldurdunji, who approved the final version.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The survey instrument is provided as Supplementary File 1. The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
AI tool disclosure
ChatGPT (OpenAI) was used solely for language editing and formatting assistance. All analytical decisions, data interpretation, and final text were reviewed and verified by the author prior to submission, in accordance with journal policy.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.