
Abstract
Objective
In blended care therapy, clients and therapists work together in synchronous psychotherapy sessions and asynchronous guided practice sessions, in which therapists assign digital tools (e.g., video lessons, written exercises) and provide guidance. This model of care is effective at scale, but the therapist experience of delivering this care has not been thoroughly examined. This study explores the therapist experience of using digital tools in blended care therapy delivered via telehealth and the perceived benefits and challenges of working within this model.
Methods
Therapists (n 276, including marriage and family therapists, professional counselors, social workers, and psychologists) were invited to complete a survey on how the digital components of the therapy platform impact care delivery. Twelve participants completed a semi-structured interview about their experience using digital tools while delivering care. Transcripts were analyzed using thematic analytic methods.
Results
The majority of survey participants reported that digital tools had positive effects on their mental health care delivery. Nearly all respondents (93.68%) reported learning new clinical skills from the tools. Three primary themes were generated through thematic analysis. First, we summarize ways in which blended care impacts therapeutic relationships. Then, we describe how the structure of digital tools supports clients and therapists to develop and practice skills. Finally, we discuss how delivering blended care impacts therapist time and energy.
Conclusion
Results provide insights into the experience of delivering blended care therapy. Well-integrated digital tools appear to bring unique value to therapists that goes beyond their past experiences delivering care in traditional systems.
Introduction
Evidence-based psychotherapies have been established for a wide range of mental illnesses and are frequently used in clinical care.1,2 Typically, evidence-based treatments include routine meetings between the therapist and the client and recommendations for tasks (i.e. homework) for clients to complete in between sessions. Completion of between-session tasks is typically associated with stronger therapeutic outcomes. 3 However, many individuals face barriers to engaging with evidence-based psychotherapies, with barriers observed both for attending sessions (e.g. time, transportation, caregiving responsibilities) and for engaging with between-sessions tasks (e.g., tasks being perceived as being too difficult, vague, or irrelevant).4–6
Blended care interventions are intended to increase the efficiency and effectiveness of evidence-based treatments by combining synchronous (i.e., face-to-face therapy sessions) and asynchronous (i.e., between-session tasks) components of care. While initial models of blended care psychotherapy typically combined in-person psychotherapy sessions with digital interventions,7–10 the use of telehealth sessions in place of in-person services has become increasingly commonplace in blended care therapy programs.11–14 In traditional models of psychotherapy, clients have synchronous therapy sessions, and are often assigned homework or between-session tasks. However, there is usually no contact between sessions, symptom assessments are typically not routinely administered, and therapists have little ability to observe client progress outside of therapy sessions. 15 Different models of blended care interventions have been established around the world, which share a common format of combining face-to-face therapy sessions with asynchronous care. Their differences lie in what that combination looks like and the activities that are included. Some programs focus primarily on combining face-to-face contact with structured digital interventions16–18 and others integrate the synchronous and asynchronous components of psychotherapy to deliver flexible, personalized interventions.14,19
In one well-studied model of blended care therapy, clients and therapists work together in both synchronous face-to-face telehealth sessions and asynchronous guided practice sessions, which serve to help clients learn and generalize skills from therapy.19–21 As seen in Figure 1, synchronous telehealth therapy sessions typically occur weekly for 50 minutes. For guided practice sessions, clients receive digital tools from their therapist to complete and then therapists can provide asynchronous support and feedback in between synchronous sessions. The digital tools include animated video lessons that use a storytelling approach, following fictional characters as they learn and apply therapeutic skills; written psychoeducational guides; interactive exercises that support skills practice; and symptom assessments. The assigned digital tools are intended to reinforce key concepts and skills that were discussed in synchronous sessions. This is a highly personalized form of care, in which therapists select the digital tools to share with their clients based on their presenting problems and goals for therapy. Thus, specialized therapeutic protocols (such as dialectical behavior therapy [DBT]) can be followed within the overarching model of blended care therapy. Clients and therapists can also message one another through the platform between sessions. The symptom assessments are used to support therapists in following best practices for measurement-based mental health care.22,23 Results from these assessments are viewable by both the client and the therapist, and can be used to address symptom change trends with clients in session as they arise. Depiction of the synchronous and asynchronous components of blended care therapy.
In this blended care therapy model, attending therapy sessions via telehealth and completing digital video lessons and exercises all demonstrate unique value to clinical symptom improvement. 20 This model has demonstrated clinical effectiveness for treating depression and anxiety at scale with sample sizes of over 33,000 adults in the United States.20,21 Recent research on this model of care demonstrates that therapeutic gains in anxiety and depression in the year after treatment remained largely stable and high with a small percentage of individuals returning for additional therapy. 24 While some therapists report concerns about technical skills and system usability as potentially interfering with clinical care delivery, past studies on attitudes toward blended care therapy, which defined blended care as when online treatment components are used in combination with face-to-face contact, demonstrate generally favorable perceptions of blended care by therapists working in European countries.25,26 An early systematic review of blended care therapy research trials demonstrated that offering blended care therapy can lead to lower client drop-out rates and save therapists time by offering general psychoeducation outside of therapy sessions. 27
However, in the United States, blended care therapy has been less mainstream. 28 Most therapists-in-training do not receive specialized instruction on delivering blended care therapy or on integrating digital tools into psychotherapy29–33 and little is known about how comfortable therapists feel delivering blended care therapy. Further, while increased attention is being paid to therapist burnout34,35 and how technology may make aspects of mental health care delivery more efficient,36–38 the ways in which blended care models of delivery support or impede therapist wellness have not been thoroughly explored in the literature to date.
The therapist experience of delivering this innovative blended model of care has not been thoroughly examined, particularly in the context of the United States mental health services delivery system. This study aimed to: 1) examine the therapist experience of delivering a model of blended care therapy delivered via telehealth with included digital tools, and 2) understand therapists’ perceived benefits and challenges while working within this model of blended care therapy.
Methods
Study procedures
This study was a mixed methods study conducted in November and December of 2023. All study procedures took place online within the United States. Participants were recruited via an email that included a brief description of the voluntary research study on how having access to the Lyra Care platform impacts their clinical work, along with a link to an online consent form. To be eligible for this study, participants needed to be employed by Lyra Clinical Associates as a mental health therapist and be 18 years of age or older.
Therapists employed by Lyra Clinical Associates deliver a specific model of blended care therapy, Lyra Care Therapy, to adults in the United States who are eligible for an employer-sponsored mental health benefit, Lyra Health. They receive training on this model of blended care as part of their job onboarding, and receive continuing supervision.
Consented participants completed an approximately 8-minute online survey (see Supplementary File #1 for the consent information sheet). On the consent document, participants were informed that participation was completely voluntary, their employment status would not be impacted by what they share in this survey, and their responses would not be shared with their employer in an identifiable manner. Members of the research team had no supervisory relationships with the research participants.
The survey was developed for this specific study (see Supplementary File #2) and the technical functionality of the survey was tested by the research team prior to survey deployment. The survey asked participants about how the digital components of the blended care platform (i.e., messaging clients; receiving assessment data; assigning and reviewing digital exercises, video lessons, and guides) impact their mental health care delivery. As seen in Supplementary File #2, the questions on the survey were primarily on Likert scales. At the end of the survey, participants could indicate interest in being contacted to participate in a semi-structured interview by providing their email address.
A subset of survey participants were contacted by email to participate in a semi-structured interview. To better capture diversity in therapist experience with digital tools in the delivery of blended care therapy, stratified sampling was used to identify potential interviewees. Participants were stratified by age, gender, and race/ethnicity. Some therapists provide blended care therapy in specialty programs that use specific therapeutic protocols (e.g. a comprehensive dialectical behavior therapy [DBT] program, a trauma treatment program, a substance use and mental health recovery program). The components of the blended care model are similar across specialty and non-specialty programs. To capture feedback from therapists who do and who do not provide specialty services, invitations to participate in the semi-structured interviews were also stratified based on participation in these programs. We intentionally included a range of professional training backgrounds (e.g. marriage and family therapists, professional counselors, social workers) who had been licensed for a range of years. Finally, participants were also stratified based on reported satisfaction with the digital tools on the survey to ensure that we could interview a subset of participants who were less satisfied with the existing digital tools.
Prior to starting the interview, participants provided verbal informed consent (see Supplementary File #3). Interviewers disclosed that they were also employed by Lyra Health, and were interested in learning from the participant provider experiences. Interview participants were encouraged to share honest feedback with the interviewers with explicit instruction that the interviewers were just as interested in hearing about what doesn’t work well for them as they were about what may have worked well. Interview questions focused on participants’ experiences using digital tools while delivering blended care therapy, particularly in relation to delivering other forms of mental health care (see Supplementary File #4). Interview participants were asked about how the different components of blended care therapy impacted their practice of mental health care delivery, and to share examples of clients for whom this model of blended care therapy seemed like a particularly good or particularly poor fit as a mental health service model.
All study procedures were approved by an external institutional review board (the Western Copernicus Group Institutional Review Board - WCG IRB, IRB #38910195.0) prior to enrolling participants.
Data analysis
Descriptive statistics were calculated to characterize the quantitative data collected from the online survey. To summarize Likert-type survey responses and generate high-level insights, we binned similar responses together in the results section (i.e., we report percentages of respondents who responded that a feature either slightly or significantly strengthened care delivery, versus the feature not impacting care delivery, slightly weakening care delivery, or significantly weakening care delivery). Full survey results are available in Supplementary File #5.
Interviews were transcribed and then analyzed in Dedoose. 39 The qualitative data analysis was guided by codebook thematic analysis.40,41 This descriptive analytic approach allows researchers to become increasingly familiar with the data as they systematically code transcripts, organize the coded data, and generate themes from the interviews. Authors (EGL and LD) first reviewed the transcripts for thematic content, and identified the primary themes that were used to create a codebook. Then, a second round of review took place in which the authors reviewed the codebook, made edits as needed, and completed a final round of coding. The authors met weekly throughout the analytic process to discuss these codes and ensure validity. Consistent with a codebook thematic analytic approach, themes were conceptualized as topic summaries. 41 The Standards for Reporting Qualitative Research checklist was followed to guide the reporting of these findings. 42
While this study employed a largely sequential mixed methods design (i.e., quantitative survey data was collected prior to the majority of the qualitative data, and survey data informed the development of interview protocols), the quantitative and qualitative data were collectively examined to inform the findings reported in this manuscript.
Positionality statement
The authors all have experience in the design, development and implementation of technology-enabled mental health services and have trained as clinical psychologists or physicians. The majority of the authors have experience in delivering evidence-based psychotherapy to individuals across the lifespan and all are current or former employees of Lyra Health. None of the authors have worked as full-time blended care therapists, nor were they in any supervisory relationships with any of the research participants. The authors drew on their professional experiences while designing the study and interpreting the data. Throughout qualitative data analysis, the authors took their own positionality and identities into account centered the study aims of understanding the therapist experience of delivering blended care therapy and understanding the perceived challenges and benefits of this model of care while analyzing the data.
Results
Participants
Demographics of N=276 survey respondents.

Demographics of N=12 interview participants.

Quantitative results
Summary of therapist survey responses.
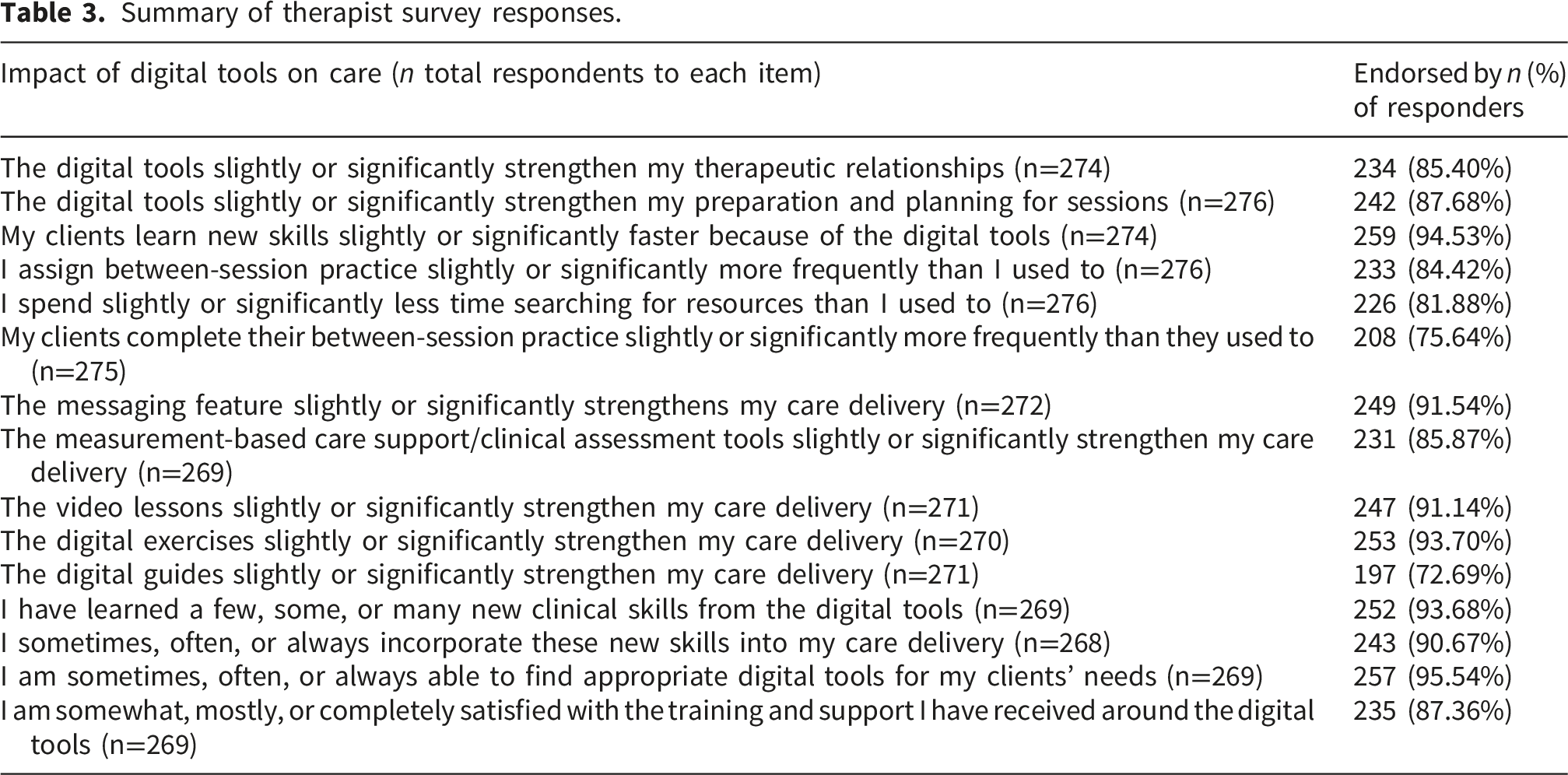
The vast majority of respondents reported that the digital tools strengthened their therapeutic relationships (85.40%), strengthened their session planning (87.68%), and helped clients learn new skills faster (94.53%). Most respondents also reported that the digital tools increased their frequency of assigning activities to practice between sessions (84.42%), reduced the time they spent searching for resources (81.88%), and increased client completion of between-session practice (75.64%). For all types of digital tools (i.e., video lessons, digital guides, digital exercises), the vast majority of respondents reported that the digital tools strengthened their care delivery.
Additionally, the vast majority of respondents reported learning new clinical skills from the digital tools (93.68%) and using these skills in their care delivery (90.67%), showing that the blended care model supports therapists continuing to grow in their use of evidence-based practices. The vast majority of respondents (87.36%) also reported satisfaction with the training and support provided around the digital tools and the appropriateness of the tools for their clients’ needs.
Qualitative results
Participants in the interview portion of the study provided feedback across a number of topics related to blended care therapy delivery. Their feedback centered on the following themes: 1) How blended care impacts therapeutic relationships; 2) How blended care provides structure for both clients and therapists to develop and practice skills; and 3) The impact of blended care on therapist time and energy.
How blended care impacts therapeutic relationships
Participants reflected on how delivering blended care therapy with the use of digital tools impacted their therapeutic relationships with clients. These reflections focused on the model’s ability to: 1) allow for more accessible care and 2) make both synchronous and asynchronous aspects of care more personalized to each client.
Increased therapeutic accessibility in care
Participants provided insights on blended care’s ability to increase care accessibility by providing services to diverse clients in a wide range of geographic locations, including disparate areas. This was considered a notable strength of the model that had the potential to strengthen therapeutic relationships.
For example, one participant (Pt #11) described: “I mean, I’m licensed in 3 states, and, you know, I live in one, right? So I’m able to talk to people, you know, who live, you know, hundreds, thousands of miles away. I don’t know thousands, but many miles away [...] It’s hard to find somebody who’s like liberal, you know, like a person of color. And so there’s that, there’s that, like, access piece.”
Here, this participant highlighted the value of providing telehealth services to make themselves more accessible to clients who may otherwise have difficulty finding a good therapist fit.
Some participants added that the flexibility of blended care allowed clients to join virtual therapy sessions at times when they typically wouldn’t be able to access traditional care, further enhancing accessibility.
For example, Pt #8 commented: “Another thing about [this blended care] model is, I think, what really helps is, people are jumping on therapy that normally wouldn’t in the traditional old fashioned way, going in. What I noticed is clients really like just jumping on during the day. They figure out their schedule they could jump on when they’re not in a meeting or at lunch or something, so I think it’s great as far as access goes. No one is asking me for after 5 o’clock appointments or weekends. Everyone wants to do it during their workday. So that’s great.”
This type of flexibility appears to help both clients in integrating therapy into their days, and helps therapists who want to maintain more traditional business hours have space for their clients.
Participants also highlighted that blended care increases accessibility by facilitating more therapeutic contact throughout the week.
As Pt #2 mentioned: “But the blended care part does highlight to clients, because, you know, when I’m doing my intake I will bring that up, and I’ll be like, ‘Here’s how blended care is different. The word blended refers to having assignments throughout the week, you know, which keep me present and attuned to what’s happening with you, because I can see your replies, and I can give you feedback on them. So it’s like I'm with you throughout the week, even though I’m only seeing you for 50 minutes once a week.’ And clearly, that is the difference, right? It’s like we are constantly in the client’s sphere of awareness because they’re filling out their assignments. We’re tracking their anxiety, their depression. And we can see how they’re progressing or no–both are okay. So that’s the main difference.”
This extension of care between therapy sessions was viewed as facilitating a stronger, more consistent therapeutic relationship.
Participants referenced specific components of guided practice sessions (e.g., messaging, symptom tracking, digital activity assignment and feedback) that allowed them to gain additional insights about clients’ experiences and deepen the therapeutic relationship.
For example, Pt #12 referenced:
“It’s usually about the logistics of the session or, I mean, the feedback that I give sometimes on the assignments impacts how we run the session cause I might say like, ‘Oh, that was so interesting. I’m curious to learn more about why you chose that value.’ Or ‘Oh, wow! That’s something that happened that was really distressing for you. Let’s make sure we talk about that in session.’”
By communicating in these ways between sessions, therapists are able to access client insights and plan for more connected and responsive therapy sessions.
The sending of between-session messages appeared to be a powerful tool in building rapport with clients. In the context of rampant barriers to mental health care access in the United States, this combination of synchronous and asynchronous support from the therapist was perceived as a particular strength. As Pt #10 commented,
“I think a lot of clients will come to me and feel really disillusioned with access… I can think of like this one client I have…, and she had a lot of trouble. She has low income. She had a lot of trouble accessing therapy in the past, and then she could work, started working at [company], and she was like, ‘Oh, my God! I'm so appreciative that you’re actually a person who, like, thinks about me and cares, and is present’ because I like, asked a question or something on the chat about, like, she was like, ‘I’m gonna be out because I have to…’ I can’t remember if it was like a family obligation. And I had said, like, ‘I hope you’re doing well and looking forward to seeing you next.’ And she was, she commented on that like later. It was like, ‘You’re a person who’s like actually available and has bandwidth to like... you know me. And you remember me.’ So I think things like that are really powerful for people.”
Having access to and strategically using the digital messaging tool can support strong rapport and engagement between the client and therapist.
Client motivation and time emerged as an important factor for determining how much benefit clients could derive from the blended care therapy model. Several participants discussed having challenges with client completion of digital assignments, whereas others found their clients more motivated and engaged with the between-session practice sessions than they expected. As Pt #2 highlighted: “A lot of people love the guides and the exercises. I get a lot of engagement on the exercises, like a lot. And again, beyond my expectation cause I always thought people would be like, ‘Oh, I don't have time for this,’ and whatever. But they’ve really engaged, which is really great news.”
The digital tools appear to support clients in integrating ways to learn and practice what they are working on in therapy throughout the week and, in conjunction with therapist insights, help guide the following session. Feedback from participants highlighted that the combination of synchronous in-session and asynchronous between-session work may be key for supporting meaningful access to therapeutic support and practices.
Support for personalized care delivery
Participants discussed how the blended care therapy model allows therapists to personalize care based on client needs and preferences, which can strengthen therapeutic relationships. Responses reflected how personalization of care can occur on various levels (e.g., types of content assigned, customization within digital tools). Overall, participants highlighted that there are advantages to this flexibility over more standardized digital content, such as having a singular digital curriculum to follow.
In examples of personalizing guided practice sessions, participants discussed how they strategically assigned digital tools that represented their clients’ experiences to help normalize their experience. As Pt #12 noted:
“I love it. I feel like the lessons are super relevant and helpful for people.[...] some woman I just had was like, ‘I just... I don’t really feel like I’m depressed’ And then she was like, ‘What is depression? I’m not a depressed person,’ you know, like… So I was like, ‘Some of the symptoms that you're having tend to fall into this category of depression,’ and “Would you like to learn more about what depression is like?’ Yeah, like, so I feel like it’s really helpful, and the clients love it. And they often say, like, ‘Were you looking into my life?’ like it’s so universal, and they feel... they get an automatic bump because it’s universal. They don’t feel so isolated and lonely in their symptoms.”
Participants also provided several examples of presenting concerns and experiences that were not represented across all different formats of the digital content library and suggested that incorporating a larger range of content would further improve representation of clients’ experiences. Several participants noted that the lack of some representation in particular types of digital content was a challenge for supporting the therapeutic relationship and their work with clients. For example, Pt #5 reflected: “I would love to see some [more] queer representation. I think I would also really like to see representation of those lower socioeconomic status problems. So we do have, like, you know, a couple of people that are characters who work retail and things like that and take the bus. Wonderful! I love that.”
Digital lessons are created and released on an ongoing basis, and identity-related content is often first available in written tool format prior to being available in video lesson format. Because a core component of this blended care model of therapy is digital video lessons, it is important that the featured characters are as representative and relatable to the target client base as possible.
Participants further highlighted the value of being able to customize digital content (e.g., by editing the instructions of digital activities) to make it better suit clients’ needs, preferences, and experiences. As Pt #4 noted, “Okay, we’ll start with what I like about it is the ones that are customizable. I think, I love, right, flexibility. Those are the ones that are really helpful and supportive, and really allows the client to feel like it’s tailored.”
Overall, this model of blended care therapy appears to support strong therapeutic relationships between the client and the therapist. While there remains room for continued iteration and improvement within the digital content library (e.g., adding video lessons with more LGBTQIA+ representation), therapeutic relationships appear to benefit from increased accessibility to therapeutic care in this model and from the ability of therapists to personalize care to individual clients.
Structure for both clients and therapists to develop and practice skills
Participants indicated that the blended care therapy model provided a flexible structure for both therapists and clients to develop and practice skills associated with high quality clinical care. Participants reflected on ways in which this care model is different from other models within which they’ve practiced. They primarily spoke of advantages they have found in this model relative to other models of delivering care.
Structure for therapists
Participants described developing and honing their skills within this model of care through a variety of ways. For example, they referenced how the symptom assessments built into the platform supports therapist adherence to evidence-based practices (e.g., symptom tracking and discussing symptom change in session), and these practices can generalize to therapists’ clinical care delivery outside of this blended care model. This point was discussed by Pt #3: “I think it’s been really eye-opening to see how much I wasn’t using it before. I still have a private practice that’s pretty small on the side. And so I’ve started, like, just on my own, like putting the numbers in spreadsheets and making graphs for my clients so that I can show them something similar, because I think that that’s really valuable. [...] I’m much more cognizant of talking about those things and bringing them up in session, like at the beginning of each session.”
The structure imposed by digital activity assignments was seen primarily as a benefit to therapists who strive to adhere to best practices for between-session assignments.
For instance, Pt #7 shared: “Okay. So when I start out with the assignments, I think the assignments have actually, in a lot of ways made me a better therapist. Especially with CBT because of the structure. I thought I knew CBT really well when I came in, but I discovered that I kind of strayed away from the protocols. And now I reach the point where I’m using all the assignments.”
Participants highlighted how, broadly, the digital content within the blended care model promotes the use of more structured, goal-oriented therapy. In one example, Pt #10 described how specific digital tools allowed them to easily formalize therapy goals with a client: “Well the exposure assignments, in particular for the prolonged exposure therapy that I do, make it really easy to do exposure work. [...] But the therapeutic goals… so like the log where you write, actually like formalize the goals, I’ve always really liked that where in like the second session, we’ll have a conversation and about what they’re working on, and when I share my screen and I’m writing down what they’re saying and they’re helping me edit it. I feel like that really helps me be collaborative about the goals. And I’m like a huge visual learner, and I’m, you know, being a teacher before I was a therapist, and then in settings in face to face settings, I’ve always relied on like a whiteboard. I just really like being able to share my screen and have them be part of what I’m writing when I use those goals, when I - when we - come up with goals, I feel like, that’s really good.”
Relatedly, participants reported that receiving weekly assessment information from clients provides scaffolding that directly informs the structure and focus of sessions. As one participant (Pt #11) described:
“It’s just like a lovely thing to kind of track their experience a little bit better [...]. Let’s say we were doing really well. And all of a sudden their anxiety, just like suddenly goes through the roof. I have something tangible that I can kind of point to and say, ‘Hey, you know, I saw in your assessment that anxiety is really high, are you okay?’ You know. So there might be something going on that they weren’t going to share. [...] I don’t know that they always actually look at it themselves, but certainly, if I share it, I think it gives them a little bit clearer understanding of the fact that they’ve improved. You know, I show them. ‘Look! Your anxiety was severe, and now it’s mild, and that’s significant.’ So that’s helpful.”
Participants highlighted that the blended care model allowed them to develop a skill set for flexibly using tools that best fit their clients’ needs. As one participant (Pt #12) described, “I will say it cuts to the chase. [...] Okay, I relate everything to art. But it’s like being in an art studio like, okay, you want to make a collage. You go to your bin that has, like your collection of papers. Like you wanna make painting? You go to your easel where you have either acrylics, oils, or watercolors. You wanna do sculpture, then pull out your clay bin. Like you have these materials that allow me to consider. Like, the client brings something to the materials and the materials bring something to the client like. It’s a reciprocal relationship that I’m looking for, and it’s my art training prepared me for that. And I use that. But it’s more in a virtual way.”
Similarly, Pt #10 reflected: “I never had a clinical product that was like it. [...] I never had as much scaffolding and I feel like that works for me really well. I feel like we’re trained really well on how to use the clinical product, and also provided a really good amount of freedom to allow me to like, improvise, and use my clinical skills to determine what I use. But the ‘what’ is very clear. So that’s great. And that's not like any place I’ve been.”
Here, participants highlight the value of being able to retain autonomy in assigning content that aligns with their personal therapeutic style and the needs of their individual clients.
Participants also discussed how clinical training and supervision offerings provided through the broader organizational system (e.g., consultation groups and continuing education) supported their skill development and ongoing use of evidence-based practices. In one example, Pt #3 discussed how their consultation team supported them in learning best practices for prompting clients to complete validated outcome assessments to support practice of measurement-based care. “And at first I felt perhaps not adept at using those [assessments] or getting clients to complete them, and have since learned strategies by talking with my consultation team about what other people do in terms of like, you know, just messaging a client a few minutes before session like, ‘Hey, please complete your weekly assessment before you show up.’ Right like, I know, they already get reminders automated. But like it’s different if it’s coming from a therapist or like the therapist’s actually taking it seriously of like, ‘Oh, you’re in session! Great! Would you mind hopping out and just like completing it, and then coming back in like. Would you be willing to do that?’ And like I mean, they pretty much always say ‘yes,’ and if they said ‘no,’ I’d roll with that. But it’s nice to have the data, and I think if they know that they, the therapist thinks it’s important, then they’ll also be willing to do.”
With the structure of having routine access to consultation teams, participants reflected that they were able to effectively adapt to delivering this model of blended care.
Structure for clients
Participants described how this blended care model helps clients learn and practice new skills. They noted that the different components of the model (e.g., frequent interaction with the therapist, digital content) enhanced clients’ learning, use of skills, and symptom improvement. In one example, a participant (Pt #8) remarked, “And then, she, she’s watching the videos and doing the exercises…. It was probably within 6 to 8 sessions. It just completely transformed her thinking, her behaviors. She went from high expectations on herself of work and self-critical, and not doing anything in her life besides work to taking pottery class, doing yoga, seeing her friends without guilt - she just became alive and enlightened, and her thinking, all of her thinking, changed so much healthier, so much better.”
Another participant (Pt #10) discussed how the self-guided nature of the digital content made learning more accessible for clients by allowing them to use the tools at their own pace: “I think just, it’s easier for clients to get appointments than most other places. It’s easier for them to have therapists that are really available that you know, you don’t have to wait 3 weeks to get the next appointment with me. It’s easier that they can chat with... Well, that’s something - I can chat with them between sessions. And I’m available in that way. And I think for the clients’ experience, like, the structure of the digital content provides them with a lot of resources to interact with the skills. But I think still, a person can only change at a rate that they’re capable of changing. So even if they have all of this, the tools available to them, I don’t think that necessarily… I’ve seen people be like, “Oh, yeah, cognitive distortions!” like, “Because I watched that video, I get it so much faster than I would otherwise” like, I still think people need time to like, digest on their own and get insight at the pace that they would move at.”
Participants remarked that the digital tools help to normalize or destigmatize mental health challenges. When clients feel understood and validated by their therapist and the broader care system, they may engage more deeply in therapy and skills practice. As Pt #4 reflected, “A lot of times I will get this: if you, if you guys spent that much time to make a cartoon and record, it must not be that abnormal, and I said it. That validation in itself is the intervention that this platform does, that you you can’t bottle anywhere else, really.”
Here, we observed that the perceived time and effort that go into making the video lessons to address concerns similar to what clients experience themselves provides a powerful sense of normalization and validation about common presenting problems.
However, some participants highlighted that there is a misfit of the model for a subset of clients.
For example, they highlighted that the model may not be a good fit for clients who do not want to complete between-session activities or who prefer a less structured therapy format.
As Pt #12 commented, “Yeah, I just had a client like this morning. We went through the intake, and I had explained the homework and she just messaged me, and she was like, ‘I’m not feeling it’ […] Sometimes people who are super busy don't like the idea of doing more activities. I feel like people sometimes just more want to vent or have less structure in their lives than another thing to do, and I try not to explain it like a thing to do. I don’t think of it like that. But I feel like sometimes people like, open the thing [referring to the client-facing platform], and they like, see 3 activities. And they’re like, ‘Ughhh.’ So, maybe just that kind of client that isn’t wanting to do more things.”
While between-session activities have demonstrated the ability to improve client outcomes, some clients come to therapy looking for a less structured therapeutic approach and are disinterested in engaging in between-session activities. This model of blended care appears to resonate less with those clients.
Impact on therapist time and energy
The ways in which blended care models of delivery support or impede therapist wellness has not been thoroughly explored in the literature to date. This is important to consider given that therapists are often at high risk of burnout.
Participants discussed the impact of this blended care therapy model on therapist time and energy in generally positive terms. These impacts were primarily discussed in terms of a tighter role definition as a blended care therapist, and the impacts of the model on their workflow as a therapist.
Role definition
In the workplace, role definition refers to having clarity regarding the responsibilities, tasks, and expectations for a job. Participants within this study highlighted that, as blended care therapists working within this particular organization, their roles typically felt more clearly defined than in past therapist positions they’ve held. As Pt #4 noted, “[The organization’s] business model is conducive to allowing therapists to be experts and hold space for their clients, and I feel everyone in leadership honors that and supports that. My experience with the prior platform was ‘get this client hooked and keep them forever.’ And it was not about, ‘hey! What are we addressing here?’ [...] It was more like, ‘keep finding problems to keep them paying the subscription as long as possible’. It felt like a salesperson job, versus a clinical job. That’s a big difference.”
This participant highlighted the tension of providing high quality care to a client with conflicting business needs found in other settings. By having clear expectations for setting goals for each episode of therapy and graduating clients from therapy, this participant felt that they are able to provide the type of support that their clients can benefit from.
Some participants discussed being able to see more clients than they otherwise would because they were able to focus exclusively on the delivery of therapy while business or administrative tasks were automated or streamlined. As one participant (Pt #5) referenced: “So this is the first time I’ve ever been part of, you know, a program where people had a a robust library to draw from of evidence-based exercises and videos, like clinical product, you know, that’s really designed to be, you know, be a big net to catch most people with most things. And it’s been really great. I will say because of [this company] and its structure and its resources, I’m able to see more clients than I ever have in my life. So I worked in, you know, like I said, community mental health. And I worked in private practice also. I could never see this many clients like 25, 30 without getting burnt out, because I don’t have to deal, it takes away a lot of the work that I would normally have to do.”
This was viewed favorably. Some participants reflected on challenges in other care settings in which they needed to focus on selling their services or spent substantial time and energy on administrative tasks.
Having role ambiguity or role conflict is a known contributor to burnout, and having tighter role definition in this role appeared to support a healthier work/life integration for many of the participants. As Pt #4 noted, “10 out of 10 for me. Let me put it this way. When I, before I came [here], I was very imbalanced with both my physical health. And so I’m gonna speak for me, personally, I’ve lost over a hundred pounds since coming [here], so I’m able to balance my personal life, my care for patients, for all of that. It provides balance in my life. I can’t be more thankful for it.”
Similarly, Pt #12 reflected, “I’m a single mother, and I am a person who likes a lot of creative freedom in my life. So the ability to schedule my own time and have control over that allows me to take really good care of myself, and to be connected with my creative energies and inner life at the same time that I’m able to, or that I want to, create an experience of healing for others.”
By having a full-time, benefits-eligible position with flexible hours (i.e., therapists chose their open appointment hours), multiple participants reflected that they were able to strike a healthier balance than had felt possible in past job roles.
Impact on workflow
Participants discussed the value of technology-enabled communication and the digital library as primarily positive contributors to their workflow efficiency. Some participants referenced that they had been initially wary of additional communication with clients between sessions. There were concerns about the time and energy that between-session communication would take up, and they largely found that the messaging with clients was not as time- or energy-consuming as they initially feared. As Pt #7 referenced, “It hasn’t turned out to be the big time sink I thought it would be. There are times where it’s a little bit annoying. Now, there’s 4 messages this morning, but again that’s me in big, whiny baby mode. When that happens [e.g., there are a lot of messages], it’s kind of nice to be able to interact with them [my clients]. I just have to be really careful, because with some clients–I want to be really clear, this is not most–it can turn into sort of de facto therapy or non-session therapy. But that’s a matter of, I just have to draw good boundaries around that.”
Other participants highlighted that they were able to maintain appropriate boundaries with their clients while using messaging, and that they were generally able to determine how much communication was the “right” amount in terms of both feasibility and enhancing therapeutic outcomes. For example, Pt #8 noted, “Oh, yeah, [messaging is] fantastic, because for one, clients for me haven’t used it in a way that harms the care. Like the boundaries seem to be really good. But it’s just a few touches of me commenting on the homework. It’s usually commenting on the homework, or someone needs to reschedule, or maybe a quick check-in of like, ‘Hey, did you schedule?’ Just, I’ll say, ‘Hey, message me when you schedule that [program] phone call’ you know, or someone is like in a crisis, not a crisis situation, but like a mentally or emotionally difficult situation sometimes giving a, ‘How did that job interview go?’ So just a few touches is really effective.”
Multiple participants discussed how technology-enabled communication (e.g. messaging, the receipt of assessment results prior to sessions) generally saved time and made care feel more efficient. For example, Pt #10 highlighted,
“Yeah, it progresses more quickly…. Here’s an example of a client… She is having a really hard time with validation, like she invalidates herself. She has sort of some chronic family of origin issues which taught her not to trust her own feelings, and I gave her an exercise about, like, anger. In particular, she doesn’t feel comfortable being angry. She was angry at her wife. I asked her to do a log, like a homemade log, like, ‘When are you feeling angry this week? And what is the anger teaching you about your needs?’ And her answer was, like, not what it was teaching her about her needs. It was, like, how to get over the anger like, ‘I need to take space or something.’ I’m like… I commented on that. So, she was able to think about it and then identify what she actually needed. And then, instead of, like, going through all that in session, she came to the session being like, ‘Oh, I needed acknowledgement.’ And so we were like… well, I guess that is a more efficient way. It makes the progress more efficient because my comment allowed her to think about it in between the session.”
By providing strategic between-session feedback, the client was able to reflect and learn in between sessions, and the time in the subsequent session was able to be spent more meaningfully.
The measurement-based care model was generally viewed as well-integrated. Many participants highlighted that tracking client symptoms weekly was new to them when they began working in this blended care program and has been beneficial to their care delivery. As Pt #8 commented, “Okay, I love it. And I never knew I would love it. So I just love it. So what’s really helpful is that the clients do the assessments, and that we have easy access to it. So in my job before, they would do the GAD-7 and the PHQ-9 and it would just… I don’t know what they were, what our administration was looking at, and we weren’t really trained how to apply it clinically. That it meant… the most is if someone flagged, like, suicidal ideation, then we would do the safety plan so... but other than that, it was like, I don’t even know if I would look at it, or there wasn’t even an easy way for me to look at it. So, being able to see the assessment results, I click, before every session, I click on my last progress. I love that, and then I click on the assessments. [...] So the graph and I actually bring it into the care. So I’ll share my screen and talk with my clients about, you know ‘Is this accurate?’, ‘What’s going on?’, and that actually really helps guide my care. I can make adjustments. It really gives a platform for me to ask curious questions of what’s going on with them and the homework.”
Participants highlighted that the embedded digital content library makes the process of assigning between-session activities seamless and efficient. In contrasting this experience to other practice settings, participants noted that this efficiency improved their clinical practice. As Pt #4 commented, “Outside of [this job], it was more of, I had to do it myself, like I had to kind of create this, like, little resource guide and figure out a way to share that that feedback loop, and then I would have to kind of take it upon myself. It was a lot of my own work that I had to do. [...] I would say, for clients what's improved there is their buy-in is right in there from the beginning. It’s not this, like, weird clunky system that I had to create with no technical expertise. So yeah, it’s a time saver, in my opinion.”
As Pt #5 commented, “I don’t do nearly the prep that I used to for each session, because I already know what we’re gonna talk about because of the in-between session homework.”
Some participants noted that the flexibility inherent in this model was key for supporting their good clinical practice, in that they are able to pull in and assign external resources and tools to give their clients (in addition to content from our proprietary digital content library).
While the logistics of this model of blended care therapy delivery often supported a more efficient workflow, it was not without intermittent constraints. Technical and usability issues were raised by several participants, including related to the organization of digital tools within the platform. Pt. #3 commented,
“I think the parts that are just slightly challenging are remembering which skills are linked in each video based on like the titles, right? So like, I have to remember that like the Impact of Self Care [lesson] is the PLEASE skills and also missing links analysis.”
Participants also reported difficulties with video session functionality and the impact of dropped calls and platform outages on care that were consistent with challenges commonly cited in telehealth delivery. Some participants reported desires for functionality available on platforms such as Google Meet (such as screen sharing audiovisual files), and highlighted confusion that has occurred when changes have been implemented on the therapist platform. As Pt #2 reflected on the platform, they noted “they’re constantly enhancing things, which is wonderful,” and then noted that keeping track of communications about changes to the platform can be challenging, and they intermittently find out about changes while in session and thinking to themself “Oh, I don’t know how to do this anymore.” Through existing internal technical reporting channels to the engineering team, the majority of these technical and usability issues reported in this study were able to be remedied prior to or soon after this data was collected.
Discussion
Results show that participants generally viewed the blended care therapy model positively and believed that well-integrated digital clinical tools bring substantial value to their clinical practice. This experience appears unique relative to their past experiences delivering mental health care in traditional systems. From this study, we gained an understanding of the ways in which this model of blended care therapy (i.e.,delivered via telehealth, with the support of flexibly assigned digital tools) impacts therapeutic relationships and how the structure provided by digital tools in this model supports both clients and therapists to develop and practice skills. Finally, we identified ways in which delivering this model of blended care therapy impacts therapist time and energy.
In mental health care, therapeutic alliance between the therapist and client is a critical factor that is strongly associated with psychotherapy outcome. 43 The model of blended care therapy explored in the present study was previously evaluated in a large-scale quantitative study focusing on therapeutic alliance and symptom trajectories of depression and anxiety. The previous study demonstrated that therapeutic alliance scores were generally strong and improved over the episode of care. Additionally, this previous evaluation found that higher therapeutic alliance was associated with both lower anxiety and depressive symptoms overall and a steeper decline in symptoms over time. 44 These previous findings support that this model of blended care therapy fosters high therapeutic alliance and enhances client outcomes.
The present study adds color to these previous findings by highlighting how blended care therapy with digital tools supports strong therapeutic relationships. Therapists in this study reported that this model makes care more accessible (stemming from telehealth sessions, digital tools that can be accessed on demand, and between-session messaging), and the personalized nature of the program (i.e.,it is flexible rather than being a rigid, linear therapeutic protocol, therapists flexibly select and edit digital activities) allows clients to receive highly individualized treatment plans. This model of blended care fosters strong therapeutic alliance, and therapists seem to partly attribute the strong alliance fostered to specific aspects of the blended care model and included digital tools. Specifically, the included messaging, symptom tracking, and feedback received from clients on assigned digital activities allow therapists to gain additional insights about clients’ experiences and deepen the therapeutic relationship. By communicating in these ways between sessions, therapists reported that they are able to plan for more connected and responsive therapy sessions. These aspects are largely unique compared to traditional mental health care delivery systems and speak to the potential benefits of integrating aspects of blended care into more systems.
Technology-enabled mental health services are recognized for their potential to improve and expand mental health care services by increasing access to evidence-based care, more actively engaging clients in treatment, increasing the use of evidence-based practices, and helping clients maintain therapeutic gains after formal treatment has concluded. 45 As rates of both mental health therapist burnout 46 and rates of depression, anxiety and other mental health disorders have been on the rise, 47 designing mental health services that serve both clients and therapists well is key for sustainability of high quality mental health care. As described below, findings from this study highlight some ways in which blended care therapy can be a sustainable and high quality mental health care delivery model.
Supporting therapist skill development and adherence to evidence-based mental health care is a priority area for ensuring a high quality mental health services workforce. 48 While the majority of states in the United States have continuing education requirements for licensed mental health providers, the requirements vary substantially from state to state.48,49 Further, while continuing education is generally viewed positively by mental health providers, the ways in which this education is integrated into clinical practice settings is highly variable.50,51 In this study, we have identified benefits of this blended care model on therapist skill development and adherence to evidence-based clinical practices. The majority of therapists surveyed reported that the digital tools strengthened their care delivery, that they learned new skills from the digital tools, and that the measurement-based care model was a strength. By integrating these evidence-based tools into the workflow of therapists, therapists appear to strengthen their clinical skills. This appears to both serve clients they work with while delivering blended care, as well as the therapists’ clinical practice in other concurrent work settings (e.g. using these strategies in external private practice work). Therapists in this study also noted that this model of blended care therapy supported clients in learning and practicing therapy skills, which are emphasized in evidence-based treatments as factors that drive symptom improvement.52–54 It appears that the structure imposed by the model, including the digital tools, provides clients with accessible opportunities between sessions to practice therapy skills.
The digital tools and structure of the blended care model appear to help define the therapist’s role as providing clinical services, which has numerous benefits for therapists. Multiple therapists in this study said that this model of care supported a healthier work-life balance by more clearly defining their role as focused on providing clinical services. Therapists highlighted that not having to focus on generating business (e.g., marketing themselves and their clinical practice) and not having to oversee business operations (e.g., managing the receipt of payments from clients or their insurance companies) provided them with more clarity to focus on clinical service delivery. This is consistent with past research indicating that role stress and ambiguity are significant risk factors for the development of occupational burnout and job dissatisfaction.55,56 Therapists also reflected on how the measurement-based care model had a positive impact on their clinical workflows, and their overall time and energy as therapists. These findings are aligned with previously documented therapist benefits to using routine outcomes monitoring 57 and with Barber and Resnick’s viewpoint highlighting that adopting measurement-based care is likely to reduce burnout in mental health clinicians. 58 To support a healthy workforce of therapists, continued attention should be paid to enhancing role clarity and supporting measurement-based practice across settings that employ therapists. Doing so could help therapists provide meaningful care for more clients (thus reducing the treatment gap) and reduce their risk of burnout.
Limitations
Participants worked for the same employer and delivered a specific model of blended care therapy, Lyra Care Therapy. Due to contextual factors inherent in a work setting, their experiences delivering Lyra Care Therapy may not fully represent the experiences of therapists delivering blended care therapy models in other settings. The study sample included primarily participants who identified as female, which is consistent with mental health workforce trends. The survey used in this study was developed specifically for this study and had been tested for technical functionality but had not been externally validated with a separate sample of participants. To capture a range of therapist experiences, participants from the survey study were stratified based on reported satisfaction with the digital tools to ensure that we could interview a subset of participants who were less satisfied with the existing digital tools. While we were able to interview a range of therapists, there may have been some bias in who chose to complete the initial study survey. Finally, the participants were aware that the researchers were employed by Lyra Health. While participants were encouraged to provide honest feedback about what doesn’t work well for them as well as information about what does work well, there may have been bias in participant responses.
Conclusions
This study provides insights into the therapist experience of delivering blended care therapy via telehealth. In this model of blended care therapy, well-integrated digital clinical tools bring unique value to therapists beyond their past experiences delivering mental health care in traditional systems. In this study, therapists were employed full-time by the same employer and set their own hours of remote clinical practice. While blended care therapy can present technical difficulties for therapists, this model of blended care therapy appears to improve care accessibility, efficiency, role definition, and work-life balance for therapists.
Supplemental material
Supplemental material - Understanding the provider experience with digital tools in blended care therapy delivered via telehealth: A mixed-methods evaluation
Supplemental material for Understanding the provider experience with digital tools in blended care therapy delivered via telehealth: A mixed-methods evaluation by Emily G Lattie, Laura D’Adamo, Miranda L Beltzer, Alethea Varra, Connie Chen, & Anita Lungu in Digital Health
Supplemental material
Supplemental material - Understanding the provider experience with digital tools in blended care therapy delivered via telehealth: A mixed-methods evaluation
Supplemental material for Understanding the provider experience with digital tools in blended care therapy delivered via telehealth: A mixed-methods evaluation by Emily G Lattie, Laura D’Adamo, Miranda L Beltzer, Alethea Varra, Connie Chen, & Anita Lungu in Digital Health
Supplemental material
Supplemental material - Understanding the provider experience with digital tools in blended care therapy delivered via telehealth: A mixed-methods evaluation
Supplemental material for Understanding the provider experience with digital tools in blended care therapy delivered via telehealth: A mixed-methods evaluation by Emily G Lattie, Laura D’Adamo, Miranda L Beltzer, Alethea Varra, Connie Chen, & Anita Lungu in Digital Health
Supplemental material
Supplemental material - Understanding the provider experience with digital tools in blended care therapy delivered via telehealth: A mixed-methods evaluation
Supplemental material for Understanding the provider experience with digital tools in blended care therapy delivered via telehealth: A mixed-methods evaluation by Emily G Lattie, Laura D’Adamo, Miranda L Beltzer, Alethea Varra, Connie Chen, & Anita Lungu in Digital Health
Supplemental material
Supplemental material - Understanding the provider experience with digital tools in blended care therapy delivered via telehealth: A mixed-methods evaluation
Supplemental material for Understanding the provider experience with digital tools in blended care therapy delivered via telehealth: A mixed-methods evaluation by Emily G Lattie, Laura D’Adamo, Miranda L Beltzer, Alethea Varra, Connie Chen, & Anita Lungu in Digital Health
Footnotes
Ethical considerations
All study procedures were approved by the Western-Copernicus Group Institutional Review Board (WCG IRB) prior to enrolling participants.
Consent to participate
Participants provided written consent to participate in the survey portion of the study, and provided verbal consent to participate in the interview portion of the study.
Author contributions
EGL, MLB, AV, CC and AL conceptualized the study. EGL and MLB designed the survey and interview guide and collected study data. EGL, LD, and MLB conducted data analyses and were the primary contributors in writing the manuscript. AV, CC, and AL provided review and feedback on the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Lyra Health. The funder of the study was involved in study design, data interpretation, and writing of the report, and informed during data collection and data analysis.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EL, MB, AV, and AL are employed by Lyra Health and Lyra Clinical Associates, receive income from Lyra Health and Lyra Clinical Associates, and have been granted equity in Lyra Health. LD is a former employee of Lyra Health, and CC is a former employee of both Lyra Health and Lyra Clinical Associates who had been granted equity in Lyra Health.
Data Availability Statement
Given the small data set, interview data are not publicly available to ensure participants’ privacy. For questions about the data set, please contact the corresponding author.
Supplemental material
Supplemental material for this article is available online.