
Abstract
Objective
This study aimed to develop a Digital Urologic Home Care platform and evaluate its usability in supporting self-management among patients with benign prostatic hyperplasia (BPH).
Methods
Participants—including patients and healthcare staff—were recruited through purposive sampling from a tertiary hospital in Guizhou Province. Investigators provided instructions on using the platform, which required participants to continuously record urination patterns, fluid intake, and symptom self-assessments, as well as access a disease information database and engage in remote communication. After a three-day trial, the platform’s feasibility was assessed in terms of effectiveness, efficiency, and subjective satisfaction. Semi-structured interviews were also conducted to capture participants’ experiences and feedback, which informed subsequent revisions to the platform’s content.
Results
A total of 10 healthcare professionals and 50 patients (aged 58–72 years) participated in this study. The SUS questionnaire yielded a total score of 80.15 (SD = 3.60), and the Human-Machine Interface Usability Questionnaire produced a total score of 71.05 (SD = 3.32), indicating that participants were satisfied with the platform. Through semi-structured interviews, six themes were identified: enhancing knowledge and confidence, balancing professionalism and convenience, supporting preliminary self-assessment of the disease, high platform usability, recognition and recommendation, and suggestions for platform improvement.
Conclusion
After analyzing the study data, we successfully designed a home-based mobile management platform and confirmed its usability through data analysis. The platform enables automated tracking and analysis of fluid intake and urination patterns, supporting continuous interpretation and personalized feedback on patients’ voiding data. It also facilitates patients’ acquisition of preliminary self-assessment skills and-disease-related knowledge, while enabling remote communication between patients and clinicians. With further refinement and updates, the platform has the potential to support self-monitoring and home-based digital management for individuals with BPH.
Keywords
1. Introduction
The prostate is the largest substantial organ in the male genital parasympathetic glands, which grows and develops during three periods: fetal period, puberty, and middle age to old age. Benign prostatic hyperplasia (BPH), also known as prostatic hypertrophy, is a disease in which prostate enlargement is caused by hyperplasia of the stromal cells in the migratory zone of the prostate gland, which in turn compresses the bladder and urethra, resulting in a restriction of the flow of urine. 1 The prevalence of BPH increases with age, with one study showing a prevalence of 50% in men between the ages of 50 and 60, rising to 80% between the ages of 50 and 70.2,3 The pathophysiology of BPH is closely related to hormonal changes, especially the effects of androgens such as testosterone and dihydrotestosterone (DHT) on prostate tissue. 4 At present, BPH has become the most common benign disease of urinary disorders in middle-aged and old-aged men, which seriously affects the life of patients, and its main manifestation is the anatomical and histological enlargement of the prostate gland (PV) with bladder outlet obstruction and lower urinary tract symptoms (LUTS), including urinary frequency, urgency, dysuria, and hesitancy. The symptoms cause great life distress and psychological pressure to patients and their families. LUTS include frequent urination, urgency, dysuria and hesitancy, which bring great disturbances and psychological pressure to patients and their families.5,6
The comprehensive evaluation of LUTS in BPH is usually a history assessment, a Bladder Diaries (BD), and an assessment of urinary flow rate, with the voiding diary being the most critical. 7 BD is a non-invasive, prospective assessment tool in which patients record their voiding patterns and symptoms over a specific time period. 8 BD can accurately reflect the severity of the disease and assist physicians in formulating a treatment plan as well as evaluating the efficacy of treatment. 9 The current BD mainly relies on paper handwriting, but there are obvious shortcomings: for patients, the cumbersome recording process reduces patient compliance, if the failure to record in a timely manner leads to omission or later recall bias when making up the record, unable to ensure the continuity of the data, and the paper version is easy to be damaged or lost; for healthcare workers: manually counting and analyzing a large amount of paper data is time-consuming and prone to error, the burden of data processing is heavy, and the reliability of paper records is not high when the data are disputed. The reliability of paper records is not high in case of disputes.10,11 Therefore, in order to ensure that voiding diaries can accurately record patients’ urination, it is crucial to require timely, accurate, and convenient voiding diary devices for patients. 12
With the advent of the digital era and the influence of COVID-19 in recent years, the era of telemedicine has been initiated on a large scale.13,14 Telemedicine is the provision of remote treatment, counseling and evaluation of patients through various types of mobile communication devices, not only that, telemedicine also includes remote care, health education and data collection and management. 15 The European Association of Urology (EAU) in its guidelines for men with LUTS suggests that telemedicine and care can be used to monitor LUTS symptoms, including symptom scores and bladder diaries to record, detect and self-assess symptoms. 16
We observed that no relevant studies have been reported to date. To our knowledge, no researchers have developed a platform that integrates traditional paper-based voiding diaries with a mobile electronic system to enhance patients’ self-management. Based on this gap, this study aims to Therefore, this study designs and tests the feasibility of a smart mobile device-based patient intelligence management system (Digital Urologic Home Care platform) that integrates recording and storing data, symptom self-assessment, and knowledge learning to help patients achieve data continuity, increase disease awareness, and reduce healthcare worker time and errors to improve clinical outcomes.
2. Method
2.1. Platform access point selection
With the global rise in mobile device ownership, especially smartphones, and their greater convenience and broader user base compared to personal computers, mobile applications provide a more accessible and user-friendly option. Accordingly, we developed a mobile application for the platform. The Digital Urologic Home Care Platform was developed by an external organization with experience in medical technology in conjunction with two caregivers. This platform can be used on devices running Apple’s iOS, as well as on mobile devices based on the Android operating system. Users can log in to the platform by registering a personal account. Caregivers or family members are allowed to assist in using the platform. The same account can be logged in on multiple devices, enabling caregivers and family members to help users—especially those with limited digital skills or reduced ability to manage daily activities—use the program more conveniently.
2.2. Platform operational interface design
The program consists of three operating terminals: the background control terminal, the medical and nursing operating terminal, and the patient input terminal. (1) Background control terminal: background operators are divided into senior administrators and junior administrators, senior administrators can carry out patient authentication, configuration and modification of various types of fields, knowledge push, remote information exchange, patient data export and modification of the background operation section, etc. Junior administrators can only view the data information and do not have the authority to modify the operation. (2) Medical and nursing operation terminal: Medical and nursing personnel can confirm and categorize patient information in the management platform, visualize and manage patient indicators, and communicate with patients remotely to clarify changes in patient conditions and give professional guidance. (3) Patient input terminal: patients can record their daily urination and water intake, and the relevant data will be stored in the background and can be viewed at any time; set up a questionnaire for relevant disease symptoms, so that patients can self-test at any time and get a preliminary understanding of their own disease; set up a database of information about the disease for knowledge learning; and finally, an online communication platform for communicating with doctors. When patients experience urgent urological conditions, such as acute difficulty in urination, high fever, chills, or hematuria, they may contact physicians through the app to obtain online medical advice and, if necessary, be advised to seek care at the nearest medical center.
2.3. Design of the user interface modules
There are five major sections: urination record, drinking water record, symptom management, disease information database, and remote communication. (1) Urination section: set up urination conditions such as number of times, time, volume, incontinence and accompanying status, etc., which will be stored in the background after being recorded by the patient. (2) Drinking water section: set the amount of explicit drinking water (water, drinks, soups, etc.) and non-explicit drinking water (fruits, vegetables, etc.), which are stored in the background after being recorded by patients. (3) Symptom management: incorporating the International Prostate Symptom Score (IPSS) and the International Erectile Function Questionnaire-5 (IIEF-5), patients can self-monitor their prostate symptoms and sexual function at any time, and make initial self-judgment of their condition. (4) Disease Information Library: Publicize the knowledge of BPH through pictures and words in diversified forms, including etiology, clinical manifestations, lifestyle and postoperative rehabilitation guidance. (5) Remote communication: The platform can realize barrier-free communication between patients and medical staff, provide patients with treatment plans and health guidance in a timely manner, improve the efficiency of discharge follow-up, reduce patients’ time and economic burden, provide patients with more convenient self-health management methods, use text to communicate with patients, enhance patients’ satisfaction with medical work, and enhance patients’ ability to manage symptoms at home.
2.4. Usability evaluation
Usability testing not only improves user satisfaction and loyalty, but also optimizes product design, improves operational efficiency, increases user engagement. 17 So the aim of this study is to design and explore the usability of Digital Urologic Home Care platform.
2.4.1. Ethical approval
“This study was approved by the Ethics Committee of Guiyang Second People’s Hospital, with the approval number JYYY-2025-WZ-07.”
2.4.2. Participants
This study was a prospective investigation in which participants used the platform for 14 days. Upon completion of the usage period, usability was assessed using the System Usability Scale (SUS) and the Human–Computer Interaction Usability Questionnaire, followed by semi-structured interviews to explore user experiences and feedback.
Sample size determination: According to Nielsen’s research, five evaluators can identify approximately 75% of usability problems. 18 In this study, sample size was determined based on data saturation. A total of 60 individuals participated in this phase, including 50 patients and 10 healthcare professionals.19,20
2.4.2.1. Patient inclusion criteria
Patients were eligible for inclusion if they met the following criteria: they satisfied the international diagnostic criteria for benign prostatic hyperplasia (BPH), were aged ≥55 years, had stable clinical symptoms, were able to independently and proficiently access the internet and use applications on smartphones or other mobile devices, and possessed adequate literacy skills.
2.4.2.2. Patient exclusion criteria
Patients were excluded if they had significant urethral stricture, urinary tract infection, prostate cancer, neurological disorders, a history of pelvic surgery, or a history of prostate surgery; had other unstable medical conditions; had participated in other clinical studies within the past two weeks; or declined participation or had incomplete dat. 21
2.4.2.3. Healthcare professional inclusion criteria
Healthcare professionals were eligible for inclusion if they possessed a valid healthcare practitioner qualification certificate, were engaged in the medical or nursing care of patients with BPH, and were willing to participate in the study.
2.4.2.4. Healthcare professional exclusion criteria
Healthcare professionals were excluded if they were on leave or attending external training, or if they were visiting scholars, trainees, or residents in standardized training programs.
2.4.3. Measurement tools
Evaluation criteria using ISO 9241.11 International Organization for Standardization definition of usability: The effectiveness, high efficiency and subjective satisfaction of a product in a specific use environment for a specific use by a specific research subject: effectiveness: task completion; high efficiency: completion time; subjective satisfaction: user satisfaction.
2.4.3.1. Demographic questionnaire
A self-designed demographic questionnaire was used to collect participants’ basic information prior to enrollment, including age, employment status, lifestyle habits, smoking and alcohol history, medical history, educational level, and use of mobile electronic devices.
2.4.3.2. System Usability Scale (SUS)
The SUS consists of 10 items across three dimensions: learnability, usability, and satisfaction. Participants completed the questionnaire themselves. The scale demonstrated good reliability, with a Cronbach’s α of 0.84, an inter-item correlation (r) of 0.807, and a KMO value of 0.879. For positively worded items (odd-numbered), the score was calculated as: score = raw score – 1; for negatively worded items (even-numbered), the score was calculated as: score = 5 – raw score. The total score was obtained by summing all adjusted item scores and multiplying by 2.5, resulting in a range of 0–100. Scores <60 indicate dissatisfaction, 60–69 indicate low satisfaction, 70–79 indicate moderate satisfaction, 80–89 indicate satisfaction, and >90 indicate very high satisfaction.
2.4.3.3. Human-machine interface usability questionnaire
This questionnaire evaluates five dimensions: functionality, learnability, efficiency, interactive experience, and satisfaction, and includes 20 items, each scored from 0 to 5, with a total score ranging from 0 to 100. A total score <50 indicates that participants consider the system or product infeasible; a score of 50–70 indicates borderline feasibility; and a score ≥70 indicates satisfactory feasibility.
2.4.4. Testing procedure
After signing the informed consent form, participants scanned a QR code to access the trial version of the platform, where they registered and signed the platform-specific electronic consent form as instructed. Following registration, patients completed baseline information, including age, sex, contact details, and disease-related data. Once the registration information was submitted, a unique binding code was generated for each patient, enabling investigators to access and utilize the data captured by the Digital Urologic Platform within specific research projects. Upon verification, the program could then be used.
The main sections of the platform are urination diary, drinking water diary, scale self-measurement, health education, remote communication, which can realize electronic BD recording, analysis, storage and realize real-time communication and exchange of knowledge and messages.
The experimental period was 14 days, and usability was analyzed in terms of effectiveness, efficiency, and subjective patient satisfaction, and one researcher acted as an assistant to record any problems participants might encounter during the task and assist in solving them. Finally, the research team set up a semi-structured interview outline:①How do you feel about using the BPH Smart Platform for self-management of LUTS symptoms?②Do you think there are deficiencies in the platform’s operational functions? How do you suggest to modify it?③Do you think the existing interface presentation (reasonable) meets your usage habits? Why?④Do you have any problem with the operation of the platform? If yes, where?⑤Would you recommend other participants to use this platform for self-management of LUTS symptoms? What are the reasons? One-on-one semi-structured interviews were conducted with the participants to express user experience and feedback, and the interviews were recorded with a tape recorder, then transcribed verbatim, and then transcribed verbatim for analysis.
2.5. Data analysis
Quantitative data: descriptive analysis was used, while measures were expressed as X±S, and counts were presented as number of cases and percentages.
Qualitative data: Colaizzi (Thematic analysis) was used to analyze the participants’ usability problems and objectivity was maintained during the analysis.
3. Results
3.1. Design of the interactive program
The platform comprises three operational interfaces: a back-end control interface, a healthcare provider interface, and a patient input interface. Within each interface, multiple functional modules were designed to support the platform’s core features (Figure 1). Architecture of the digital urology platform, including backend management, healthcare professional, and patient terminals with corresponding functional modules.
3.2. The interactive interface comprises five main modules: Health record management, risk assessment, symptom management, disease education, and remote doctor–patient interaction
The health record management module enables systematic collection, storage, and updating of patients’ demographic information, clinical data, and follow-up records, thereby supporting continuous monitoring and long-term disease management. The risk assessment module evaluates patient conditions based on clinical indicators and patient-reported data, providing timely alerts for potential complications and facilitating early intervention. The symptom management module allows patients to record urinary symptoms, medication use, and changes in health status, supporting dynamic tracking and individualized management. In addition, the disease education module delivers structured and accessible educational content related to benign prostatic hyperplasia, including disease knowledge, lifestyle recommendations, medication guidance, and self-management strategies, which helps improve patient understanding and treatment adherence. The remote doctor–patient interaction module supports real-time communication, online consultation, and follow-up feedback between healthcare providers and patients, enhancing accessibility to medical services and continuity of care. Together, these modules establish an integrated interactive system that improves patient engagement and promotes effective home-based digital health management. (Figure 2). Overview of the platform’s interactive interface modules: (a) Healthcare provider communication interface; (b) Fluid intake diary; (c) Main interface; (d) Disease education interface; (e) Voiding diary.
3.3. Effectiveness
Task completion rates.

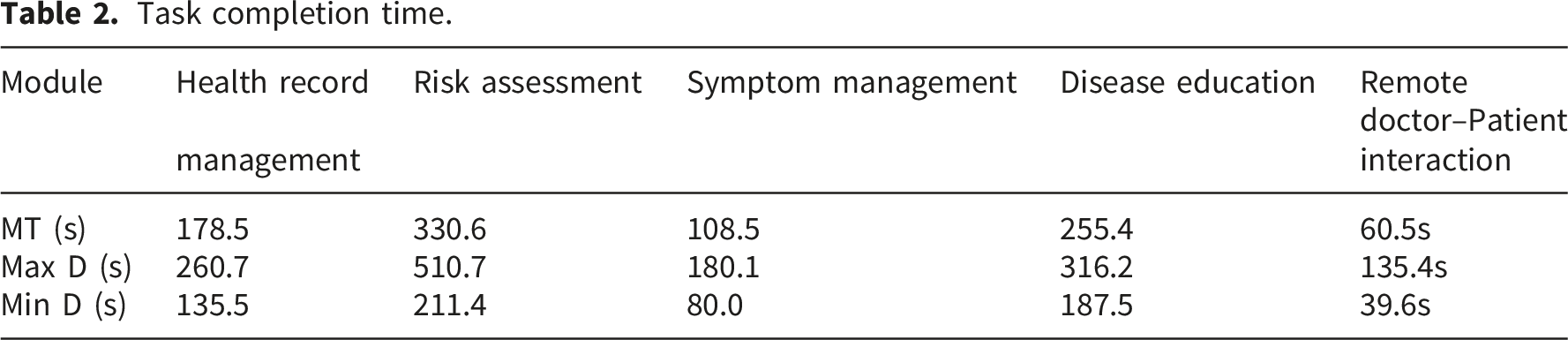
3.4. Efficiency
Task completion time.
3.5. Participants’ subjective satisfaction
SUS item scores (X ± SD).

3.5.1. Human–machine interface usability questionnaire
Scores of the human–machine interface usability questionnaire by dimension.

3.6. User experience and feedback
User experience and feedback.

4. Discussion
4.1. Designing a management platform based on traditional voiding diaries and user needs is key to constructing an efficient home-based management system
Currently, many mobile health applications for chronic disease management suffer from low user retention and high dropout rates. The main reasons are insufficient implementation of a user-centered design approach and a lack of iterative usability testing and deep multidisciplinary team involvement. Compared with traditional development models dominated by expert opinions or experience-based judgment, this study adopted a user-centered approach throughout the development of the home-based management platform for BPH patients. The platform design was based on the traditional voiding diary, integrating prior research findings and feedback from patients, family members, and healthcare providers, ensuring that platform functions closely align with users’ daily management scenarios. This user-driven design strategy aims to significantly enhance platform practicality and promote long-term engagement.
4.2. Constructing a structured, multidimensional self-management platform based on internet technology demonstrates good usability and potential as a BPH home management tool
Voiding diaries are an important tool for assessing BPH symptoms; however, paper-based diaries are prone to loss, cumbersome data organization, and low long-term adherence. In this platform, the classic tool was digitalized and structured while retaining its clinical core value, and its functions were expanded through internet technologies. The platform integrates five core modules—health records, risk assessment, disease education, medication reminders and follow-up, and doctor–patient communication—forming a comprehensive management system that goes beyond simple record-keeping.
This transformation allows patient symptom data to shift from static records to dynamic, analyzable information streams, enhancing self-management capabilities and providing an efficient, objective means for doctor–patient communication, potentially improving clinical efficiency and decision-making quality.
A mixed-methods approach combining quantitative and qualitative analyses was used to evaluate platform usability in terms of effectiveness, efficiency, and satisfaction. Results indicated that: 1. 90% of participants completed all modules. 2. The time to complete each module was less than 10 minutes, meeting efficiency standards. 3. Participants reported satisfaction across all items in the SUS and Human–Machine Interface Usability Questionnaire, reflecting high satisfaction with the platform. 4. Qualitative interviews further confirmed usability, with most participants indicating that the platform facilitated disease management, was simple and easy to navigate, and would be recommended to others. Suggestions included enlarging font size and adding notification sounds for remote interactions to improve timely communication.
4.3. Establishing a “Healthcare Provider–Patient–Family” collaborative digital humanistic care model
BPH primarily affects middle-aged and older men, who generally have lower digital literacy, cognitive capacity, and familiarity with technology. To address this, the platform design incorporated age-friendly principles, including a simple and intuitive interface, enlarged clear fonts, and concise operation steps, while also enabling family involvement to assist patients in disease management.
This design reduces barriers for older users and enhances family roles in medication supervision, record assistance, and emotional support, forming a collaborative model of “healthcare provider–patient–family” management. This approach improves platform usability, user-friendliness, and the sustainability of home support, embodying a “digital humanistic” approach to patient care.
4.4. Preliminary construction and application of an AI-based multi-symptom integration and tiered risk prediction model for BPH
The platform’s AI-based risk warning module systematically integrates and analyzes patient-reported storage-phase symptoms (e.g., frequency, urgency, urge incontinence), voiding-phase symptoms (e.g., difficulty urinating, weak stream, incomplete emptying), and symptoms of severe complications (e.g., hematuria, acute urinary retention, renal impairment). This enables a shift from passive record-keeping to proactive risk management.
Through a tiered warning system (green–yellow–red), the platform automatically identifies and categorizes low-, moderate-, and high-risk conditions based on symptom patterns and severity, allowing stratified patient management and early risk detection.
This module assists patients and healthcare providers in early identification of high-risk situations such as acute urinary retention, urinary tract infections, and renal function impairment, providing timely and critical medical interventions and strengthening the foresight and safety of home-based health management.
4.5. Limitations
Although this study confirmed the usability and potential of the smart BPH platform, it could not quantify the effect of specific platform functions on improving clinical symptom levels or self-management behaviors. Furthermore, this study did not include a paper-based voiding diary control group. Future clinical trials are needed to evaluate the platform’s practical application and clinical effectiveness.
5. Conclusion
Internet-based self-management is becoming more and more common as a way of adjuvant medical treatment to manage complex diseases. In this study, we developed and evaluate the usability of a smart platform for benign prostatic hyperplasia (Digital Urinary Home Care platform).
5.1. Principal findings
In this study, we designed and developed a BPH Wisdom Platform, known as the Digital Urinary Home Care Platform, based on the needs of BPH patients and the traditional voiding diary. We conducted a usability analysis focusing on effectiveness, efficiency, and patient satisfaction, which demonstrated that the platform possesses a high degree of usability and utility in practical applications. To further explore and optimize the user experience, we conducted semi-structured interviews with users. These interviews provided direct feedback on various platform functions and allowed us to identify and summarize specific challenges and areas for improvement. In response to the identified user experience barriers, we undertook an iterative process to enhance the platform. Ultimately, following a series of usability evaluations and corrective measures, the platform exhibited considerable potential as an effective tool for the self-management of patients with Benign Prostatic Hyperplasia (BPH). This underscores the platform’s feasibility for application in real-world healthcare management scenarios and offers a valuable reference framework and practical insights for the development and optimization of similar smart healthcare platforms in the future.
Footnotes
Ethical considerations
The study was approved by the Institutional Ethics Committee of Guiyang No. 2 People’s Hospital (JYYY-2025-WZ-07) and was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Consent to participate
All patients provided written informed consent.
Consent for publication
Consent for publication was obtained from the participants.
Author contributions
Miaoqing Cai (First Author): Conceptualization, Data Curation, Fommal Analysis, Investigation, Writing-Original Draft, Jianrong Zhang: Writing-Review & Editing, Qiangqiang Chen: Methodology, Sofware, Jiamei Wang(co-author).Wen Zhou. Sudan Zeng. Qiangqiang Cheng. Huan Wang. Beibei Yan: ethodology, Supervision, Data Curation. Aobing Mei(Corresponding Author): Conceptualization, Funding, cquisition. Resources, Supervision, Validation, Writing-Original Draft, Writing-Review &Editing, Mei Chen: Supervision. Validation, Funding Acquisitio, Wei Wang: Data Curation. Investigation, Funding Acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received the Science and Technology Fund project of Guizhou Provincial Health Commission (No. gzwkj2021-141); Guizhou High-level innovative Talent selection and Training Program Project (Guizhou Committee leader issued [2022] No. 3; Support of Chuke Contract -GCC[2022] No. 16).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, author-ship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.