
Abstract
Objective
Frequency voiding charts are commonly used to gain better insight into the voiding and drinking behaviours of patients with voiding symptoms. Non-compliance when filling out a chart is known to be high. The use of a digital application might increase adherence, but little research has been conducted on this topic. The aim of this study is to compare the quality (number of correctly filled out charts) and quantity (number of complete charts) of digital versus paper frequency voiding charts among children and their parents.
Methods
A multi-centre parallel randomised controlled trial was conducted. Participants were assigned either a 48-h digital frequency voiding chart or a 48-h paper frequency voiding chart. Completion rates were scored based on a predefined scoring method and transcribed into a percentage. Secondary objectives included user friendliness, feasibility, degree of the child's participation, and attractiveness. Trail registry data: NTR NL9383.
Results
Ninety-seven patients were randomised to either a digital (N = 53) or paper (N = 44) frequency voiding chart. No significant difference in complete and accurately filled out frequency voiding charts was seen between the groups, with 35% (N = 18) for digital and 50% (N = 22) for paper, p = 0.12. Subjects considered the digital application more appealing, more educative, and more inviting compared to the paper chart (p < 0.05).
Conclusions
In this underpowered study, no significant difference appeared between the groups in the number of complete and accurately filled out frequency voiding charts. Implementation of e-health did not seem to improve compliance. In daily practice, personal preference might offer the best solution.
Introduction
Lower urinary tract dysfunction (LUTD) is a common problem in school-aged children and a frequent condition in paediatric health care.1,2 In school-going children, the prevalence of LUTD varies between 4.0% and 23%.2,3 Besides a thorough history, the International Children's Continence Society advocates additional tools like frequency voiding charts (FVCs) or voiding dairies for both initial diagnostic purposes and evaluation of treatment during follow-up.4,5 FVCs provide information about fluid intake; number of voids; voided volumes; and urine loss, including severity, for a 48-h period. 1 If executed correctly, the FVC, as a non-invasive tool can prevent unnecessary diagnostic delay or inaccurate treatment during follow-up. Nevertheless, compliance in filling out an FVC is moderate.6,7 In a survey conducted in our centre, participants mentioned several reasons for non-compliance in filling out a paper FVC, namely leaving the FVC at home, the FVC being time consuming, a lack of understanding of its purpose, and the FVC's unappealing design.
Because smartphones have become an inseparable part of modern living, digital health applications are increasingly available in health care. 8 Digital FVCs might be a promising way to improve compliance when filling out an FVC. In adults, digital FVCs resulted in higher completion rates with more correct and legible data.9–11 Digital FVCs were considered more user friendly, providing real-time data that can create an opportunity to offer instant feedback to the user. 12 A direct feedback mechanism can enhance motivation and therapeutic engagement. 13 Despite the possible advantages of digital FVCs in the adult population, it is not yet fully known whether digital applications also improve compliance in a population of children and their parents. The aim of this study was to compare compliance in filling out a digital FVC versus a conventional paper version in the paediatric population. We hypothesised an improved quality (higher number of correctly filled out FVCs) and a higher quantity (higher number of complete FVCs) using the digital FVC compared to the paper FVC.
Material and methods
A multi-centre parallel randomised controlled trial was conducted including all paediatric patients and their parents who were asked to fill out an FVC for diagnostic or therapeutic purposes. All eligible subjects seen in the paediatric outpatient urology or paediatric nephrology departments in two university hospitals located in the Netherlands were invited to participate and given written information along with a conventional paper FVC. All patients aged between 5 and 16 years with an indication for filling out an FVC were eligible for participation, as were their parents. Exclusion criteria were the absence of a digital device, language barrier, and severe intellectual or behavioural disabilities that are incompatible with filling out an FVC.
Allocation and randomisation
Within a few weeks of being invited to participate, subjects were contacted via telephone by one of the research members. If subjects agreed to participate and signed the informed consent – including their authorised representatives – they were randomised to fill out either a conventional paper FVC or a digital FVC. If allocated to the paper FVC group, subjects already had an FVC provided at their last appointment and were instructed to fill it out before their next appointment. If allocated to the digital FVC group, subjects were provided with installation details of the application for mobile phones or tablets and user instructions by telephone and afterwards by email. By means of the computer programme CASTOR EDC, simple unstratified 1:1 randomisation was executed. An independent member of the research team who had neither a professional relationship with the patients nor involvement in the study's conceptualisation or data analysis completed enrolment, allocation, and study instructions. The health care providers were blinded to the allocation; the subjects were not. At the next appointment, subjects provided either the paper FVC or a printout of the results of the digital FVC. Within the next week or two, participants were contacted by phone for a short evaluation to collect experiences concerning the use of the FVC.
Outcome parameters
The primary outcome was the percentage of complete and correctly filled-out FVCs. If the FVC was not available at the time of their next appointment with the health care provider, patients were once again asked to fill out their FVC. If the FVC was not delivered at the subsequent appointment, subjects were considered non-compliant, and completeness was scored at 0%. Percentages of completeness and correctness were determined according to a scoring method designed by the research team. Two authors (LW/CB) independently scored all FVCs. Cases of disagreement were resolved through discussion until consensus was reached. The two days filled out on the FVC were scored separately. Afterwards, a total score was calculated. The scoring method used is shown in Table 1. Secondary outcomes were assessed using an evaluation form and included user friendliness, feasibility, understanding of the purpose of the FVC, the degree of the child's participation and the attractiveness of the FVC (see Appendix 1 in Supplemental Material). This was scored on a four-point Likert scale ranging from 1 (totally disagree) to 4 (totally agree) and transcribed into a percentage. Other objectives were the usability of the data for clinical purposes, the reasons for incompleteness, and the existence of gaps.
Scoring system of FVC.

Frequency voiding chart
An FVC consists of two separate columns, with one for drinking and one for voiding. Participants are instructed to measure the exact time and amount of each fluid intake and each voided volume for a total of 48 h. Additional information such as the urge to void; the occurrence of urinary incontinence; and, if applicable, diaper weight is also registered. An FVC offers an insight into the voiding and drinking behaviour of a child and provides detailed information about the daytime and night-time voiding frequency; minimum, maximum and average bladder capacity; and amount of fluid intake, which can help in the initial diagnosis and evaluation of treatment during follow-up. The digital FVC used in this study was realised in collaboration with patients and their parents, health care providers and technical/IT professionals. After a pilot study of 20 patients, the developers made adjustments to optimise the use of the application. Thereafter, the application was launched in the Netherlands for both Android and iOS. The application could be downloaded on a smartphone or tablet (if children did not have a smartphone themselves). In daily practice, the child fills out the FVC (either digital or paper) with or without the parents’ help. In general, younger patients often require more help compared to older ones not only with entering the exact time and amount of voided volume in the chart but also with initiating going to the toilet, voiding into a cup, measuring the amount of voided volume and writing this information down in the FVC. Child participation was one of the parameters measured to determine differences between the digital and paper FVC. Figures 1 and 2 show the layouts of the paper FVC and the digital FVC.
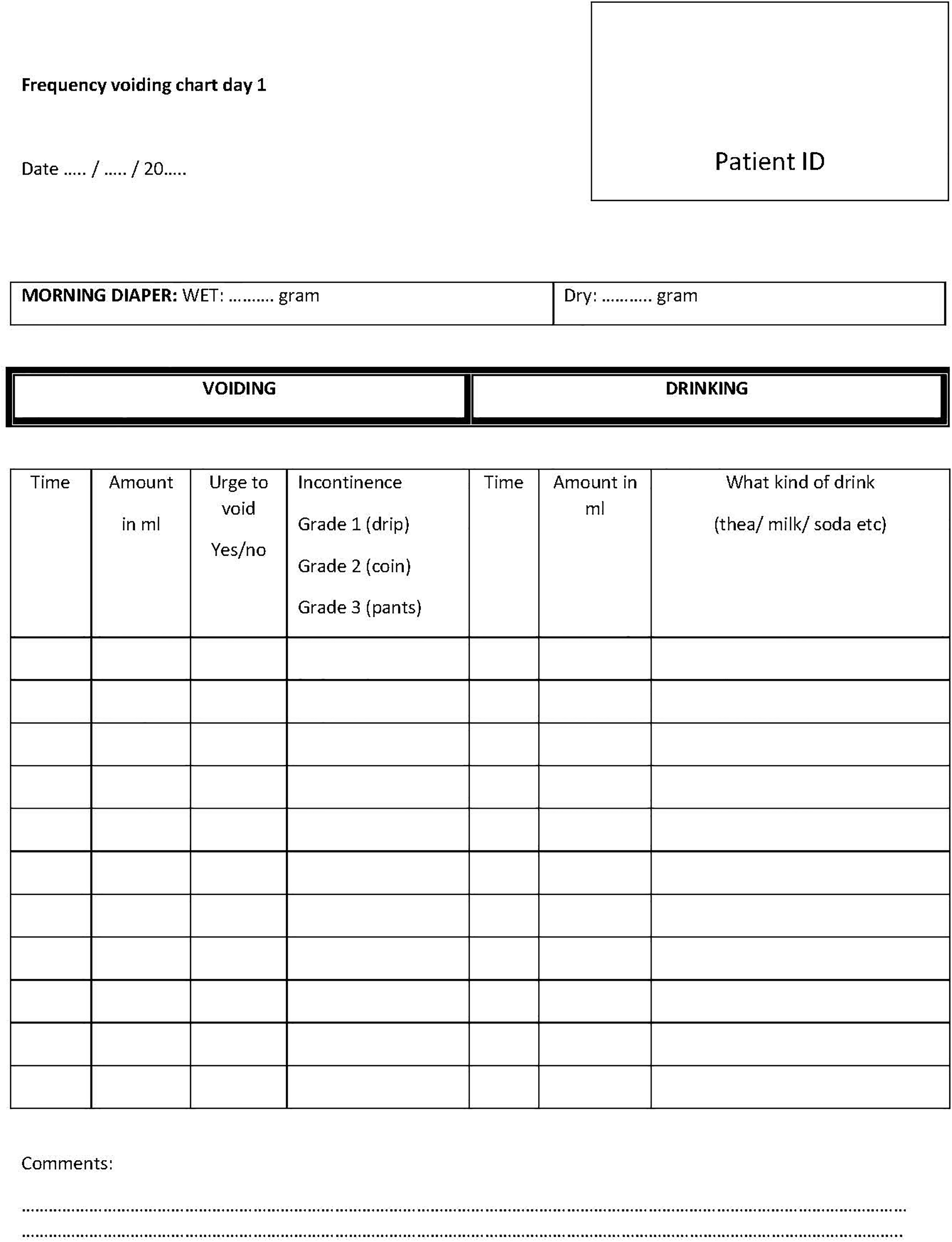
Layout of the paper frequency voiding chart (FVC).

This figure presents several screenshots of the digital frequency voiding chart (FVC). When translated into English, screenshot left side: How much did your drink? (cup/glass/fruit/dessert), screenshot in the middle: Did you void? Screenshot on the right: Did you have an accident for urine, and if so, what was the amount of urine loss (drip, coin, underpants wet, trousers wet)?.
To study the primary outcome, participants were instructed to fill out the FVC for 48 h. However, it was possible to extend the registration period if subjects wanted to monitor their voiding/drinking habits for a longer period. The first 48 h were used for analysis of our primary outcome.
Statistical analyses and Ethical aspects
A power analysis with a hypothesised 25% increase in completeness in those filling out a digital FVC versus a paper version (α = 0.05, β = 0.20, drop out 10%) suggested a sample size of 127 participants in total. The 25% increase was based on a pilot study performed at our institute in 2020. The study was approved by the local Research Ethics Committee (NL71348.091.19) and registered in an accessible study registry (NTR NL9383). The conduct and reporting of this study followed the CONSORT guidelines (see Appendix 2 in Supplemental Material).
Demographics were expressed as numbers and proportions (mean ± standard deviation [SD]) for normal distributed data and medians for non-normal distributed data. An unpaired t-test or one-way ANOVA was performed for normally distributed continuous data, and a Mann-Whitney U test was used for non-normally distributed continuous data. A chi-square or Fisher's exact test was performed for binary and nominal data. The data were analysed using SPSS Statistics 25.0. Differences were considered statistically significant at p < 0.05.
Completeness and correctness of FVCs as our primary outcome were determined based on all FVCs collected. If complete and correct, a score of 100% was given. In cases where patients did not fill out an FVC at all, a score of 0% was given. As a result of this method, there was no missing data. Data were analysed according to an intention-to-treat analysis; if subjects filled out a paper FVC but were intentionally randomised to the digital FVC, they were scored according to their allocated group. Regarding prognostic factors, compliance in filling out an FVC was analysed using a binary logistic regression model based on the value of independent predictors and a subsequent multivariable backward model. Parameters included were gender, age younger or older than 8 years, reason for filling out an FVC (diagnostic or therapeutic), experience with filling out an FVC (yes/no) and number of days filled out.
Results
Between June 2021 and February 2023, 166 patients were asked to participate. After being contacted, 126 (76%) patients agreed to participate, while 40 (24%) declined for several reasons such as a lack of interest or time, a specific wish for either a paper or digital FVC or the child having no motivation to participate. Of the 126 patients who initially agreed to participate, six patients were excluded because they did not meet the inclusion criteria (age, language barrier or severe intellectual/behavioural disabilities), and 23 patients never signed an informed consent form despite being contacted twice. Ninety-seven subjects were randomised; 44 (45%) patients were allocated to the paper FVC and 53 (55%) patients were assigned to the digital FVC. All of these except one (unexpected death after signed informed consent) were included in the final analysis (see also Figure 3). The trial ended before reaching the required number of participants according to the power analysis (goal N = 127, agreed to participate N = 126, randomised N = 97). The reason for the pre-term closure of the study was the need for several costly software updates. To justify these costs, an analysis of the data was performed.

Flow chart of enrolment according to the CONSORT guidelines.
Study group
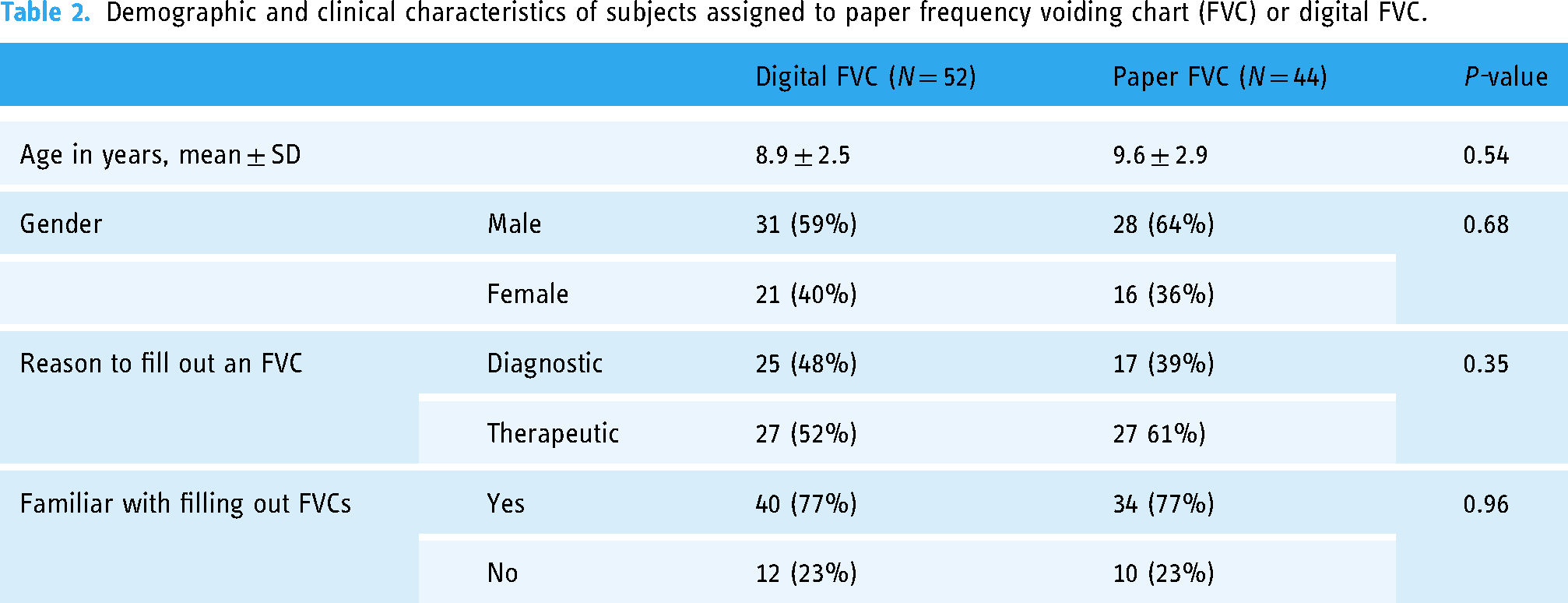
The medical urological diagnosis of the whole group varied from unknown in 9% (N = 9) where the FVC was used for screening purposes (e.g., routine screening of paediatric kidney recipients), overactive bladder with or without urinary incontinence in 47% (N = 45), dysfunctional voiding in 15% (N = 14), recurrent urinary tract infections in 9% (N = 9), enuresis in 12% (N = 11) and neurogenic bladder in 8% (N = 8). The mean age was 9.3 ± 2.7 years. The study group was considered representative of the total number of children treated in a third-line clinic at the urology or nephrology department. Demographics and clinical characteristics were not significantly different between the paper FVC and digital FVC groups concerning age, gender, reason to fill out an FVC and familiarity with filling out FVCs (Table 2).
Demographic and clinical characteristics of subjects assigned to paper frequency voiding chart (FVC) or digital FVC.
Completeness of FVCs
The number of complete and accurately filled out 48-h FVCs did not significantly differ between the paper FVC and digital FVC at 50% (N = 22/44) and 35% (N = 18/52), respectively (p = 0.12). The overall completion rate of the whole group was 42% (N = 40/96). In both groups, the number of completed FVCs was higher on the first day of the 48-h period compared to the second day. Significantly more subjects in the paper FVC group scored 100% completeness for the second day compared to the digital FVC group (see also Table 3). Additionally, we calculated an effect size because the number of included participants was insufficient according to the predefined power analysis. This revealed a Cohen's d of 0.5, indicating that accurate and complete FVC. 0.5 SD was seen more frequently in the paper group compared to the digital group. The number of inaccurately or completely filled-out FVCs was not significantly higher in the digital FVC group versus the paper group at 65% (N = 34/52) and 50% (N = 22/42), respectively (p = 0.12). The number of incomplete FVCs was significantly higher in the digital FVC (19/52, 37%) versus the paper FVC (5/44, 14%, p = 0.02). Incompleteness (missing time points or measurements) was similar between the two groups. Four patients were analysed according to the intention to treat principle and filled out the opposite form of FVC as intentionally assigned to them.
Primary and secondary outcomes of frequency voiding chart (FVC) parameters.

Time gaps: These are time points in the frequency voiding chart (FVC) not registered (for example no data collection at school).Measurement gaps: These are gaps were time is registered but not the volume in the FVC (for example because of simultaneously stool during voiding). Missing data: In the FVC only the intake or only the voided volumes are registered
Child's participation
The percentage of children's participation was not significantly different between the digital FVC and paper FVC, with a median of 40% in both groups (p = 0.19). When subclassified according to different age groups, a significantly lower percentage of children's participation was seen in the younger children compared to the older ones, p = 0.01. This suggests help from parents with filling out the FVC in the younger children. There were no significant differences between children's participation among the different age groups and types of FVC (digital or paper). This is shown in Figure 4. The number of complete and accurate filled-out FVCs was not different between the different age groups and types of FVCs either, p = 0.92 (data not shown).

Percentage of child's participation among the different age groups (5–12 years) and type of frequency voiding chart (FVC). A chi-square test was performed for each age group, and p-values are shown. Because age groups from 13 to 16 years contained fewer than two participants each, they were not included.
Evaluation of frequency variance charts by subjects
Individual aspects of either the digital or paper FVCs were evaluated and are shown in Figure 5. Subjects considered the digital FVC significantly more appealing and educational, the design more inviting and the digital FVC the preferable way to fill out an FVC.
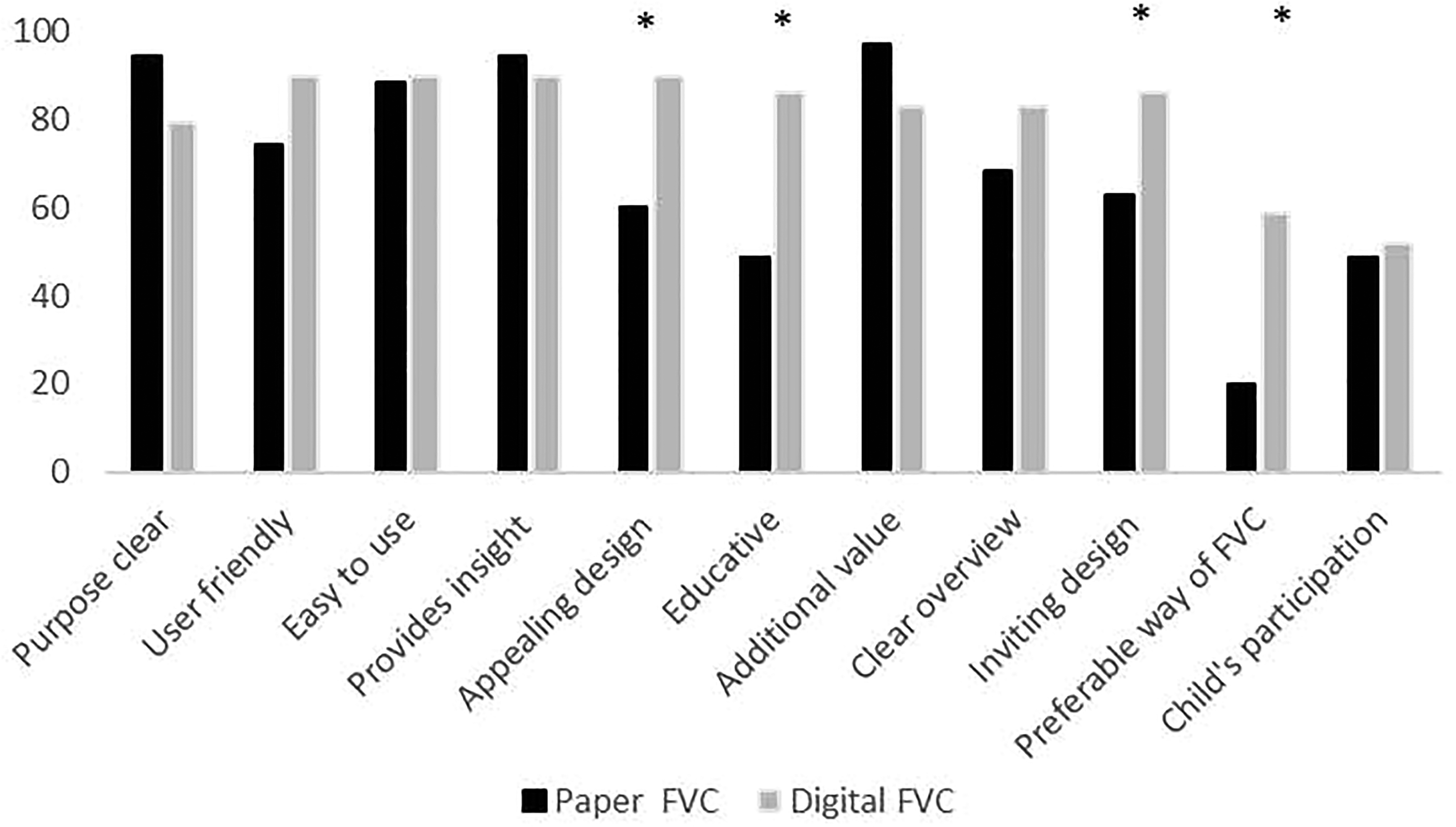
Evaluation of subjective aspects of frequency voiding charts (FVCs) reported in percentages. The four-point Likert scale was re-categorised into two categories: Totally, agree and agree into one group and totally not agree/not agree into another group. The percentages shown represent the number of subjects who agree/totally agree with the statement *p < 0.05.
Multivariate analysis
To identify predicting parameters for compliance, several factors were analysed in a backward regression model. Of the included parameters (gender, reason to fill out FVC, number of days filled in on the FVC, age below or above 8 years, familiarity with filling out an FVC), none were predictive. The results of the multivariate analysis are shown in Appendix 3 in Supplemental Material.
Discussion
This underpowered, randomised, controlled, multi-centre study could not find any significant difference in either the quantity (number of complete charts) or quality (number of correctly filled out charts) of 48-h digital or paper FVCs used by children and their parents. However, the digital FVC was significantly more appealing, more educational and more inviting compared to the paper FVC.
FVCs are non-invasive and important tools used for both diagnostic purposes and during follow-up to evaluate therapeutic interventions in the urological/nephrological paediatric population. 4 In addition to valuable insight into a child's voiding and drinking behaviour, the FVC offers a way to gain important urodynamic information such as bladder capacity without the need for otherwise invasive, stressful procedures. 4 Despite this importance, compliance with filling out an FVC is known to be moderate. Non-compliance rates seem to be even higher in the paediatric population compared to the adult population.6,10,14 In our study, an overall completion rate of only 42% was observed without a difference between the digital FVC and the paper version. Another study by Johnson et al. found an overall completion rate of 69% in children without a difference between digital and paper FVCs. 10
Higher completion rates of FVCs have often been observed in the adult population compared to among children.6,15 Oh et al. 15 found a completion rate of 94% in adults with an increase of 10% if the treating physician communicated clearly about the purpose of the FVC in advance. In our study, most subjects understood the purpose of the FVC because 88% chose “agree/totally agree” on the item “The purpose of filing-out a FVC was clear to me”. Other authors have correlated compliance with the total number of filled-out days and found a decrease in adherence with each additional day an FVC needed to be filled out. The authors advocated a maximum duration of three days for the adult population. 6 Our study used a 48-h duration based on international paediatric guidelines. 1 Because the purpose for filling out an FVC seemed clear and the FVC was filled out for only two days instead of three or more days, other factors are likely to have played a role in the low compliance rates seen in our paediatric subjects and their parents. Lack of motivation in either the child or his or her parents, busy schedules with lack of time to help fill out an FVC for their child, relying on others (e.g., teachers at school) to fill out an FVC and other hindering factors like co-parenting among divorced parents might explain the differences observed in the paediatric population compared to the adult population. This is confirmed by the low percentage of child participation reported by parents in our study (40%). Another factor might have been reluctance to fill out an FVC yet again. Most of our subjects were familiar with filling out an FVC, and it seems they could not find motivation to fill out another FVC.
Other authors have suggested gamification as a way to improve motivation and adherence in filling out an FVC. 10 However, in a study by Nieuwhof-Leppink et al., 16 a serious game did not increase intrinsic motivation in children when treated for their voiding complaints despite the fact that children considered the addition of a digital game in their treatment attractive. Furthermore, the addition of the game did not influence treatment outcome. This was also observed in our study. Subjects and their parents considered the digital FVC more appealing and inviting and scored significantly higher on the item “Preferred way of filling out a FVC” but did not improve completion rates. In addition, child participation in this study was low (40%), and parents are most likely not attracted by the gamification of an FVC, nor will it increase their compliance. In contrast to published literature concerning the positive effect of medical mobile software on compliance rates in adults, this study did not show this effect with the digitalisation of an FVC for children and their parents.9,11 In our study, the number of not filled-out FVCs differed significantly between the digital FVC and paper FVC (Table 3), which suggests problematic use of the digital FVC and might explain the results.
Digital FVCs could offer several potential advantages. They facilitate digital communication with the health care provider in an easier and faster way. FVCs can be uploaded from mobile phones to the electronic patient record, enhancing remote consultation and automatically generated calculations (e.g., average voided volumes/total amount of intake, etc). Notifications can stimulate the patient to participate and incorporated feedback mechanisms can give the user instant insight. However, disadvantages include the increasing privacy and security regulations concerning data transfer and/or storage and the need for regular software updates to keep an application functioning. Another concern is the ever-expanding number of applications available. The number of digital smartphone healthcare applications in the Google Play Store increased from 23,955 in 2015 to 54,546 in 2022.8,17 It is imaginable that patients could become overwhelmed and over-digitalised.
Limitations and strengths
The strength of this study was the randomised, controlled design of the trial. In addition, this is one of the few studies about FVCs in the paediatric population, which is different from the adult population because as previously stated, other factors determine compliance. Because today multiple applications are being designed and implemented without previous research concerning the influence on the quality of the tool itself and its assessment, we consider this study important. Not reaching the number of participants according to the power analysis is a limitation of this study. Another limitation is that instructions for how to download and use the application were initially explained by telephone. By the time participants wanted to fill out an FVC, some of them had forgotten how to use the digital FVC and did not fill anything out or filled out the paper FVC with which they were familiar. We addressed this by e-mailing the instructions after we learned about this problem, but this still affected completion rates.
Conclusion
This underpowered study could not reveal any significant difference in compliance and quality between digital and paper FVCs. Digital FVCs were considered more appealing, more educational and more inviting compared to paper FVCs. Because both FVC methods might result in similar quantitative and qualitative data, they seem equally suitable to use in daily practice. The personal preferences of patients might offer the best solution to optimise adherence.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231207577 - Supplemental material for Challenges in e-Health: The effect of digitalisation of frequency voiding charts on compliance in paediatric patients. Randomised controlled trial comparing digital and versus paper frequency voiding charts
Supplemental material, sj-docx-1-dhj-10.1177_20552076231207577 for Challenges in e-Health: The effect of digitalisation of frequency voiding charts on compliance in paediatric patients. Randomised controlled trial comparing digital and versus paper frequency voiding charts by Liesbeth L de Wall, Elisabeth AM Kragt, Eline HM Van De Wetering, Johanna GL Cobussen-Boekhorst, Joyce Mantel-van Stel, Barbara BM Kortmann, Wout F Feitz and Charlotte MHHT Bootsma-Robroeks in DIGITAL HEALTH
Supplemental Material
sj-doc-2-dhj-10.1177_20552076231207577 - Supplemental material for Challenges in e-Health: The effect of digitalisation of frequency voiding charts on compliance in paediatric patients. Randomised controlled trial comparing digital and versus paper frequency voiding charts
Supplemental material, sj-doc-2-dhj-10.1177_20552076231207577 for Challenges in e-Health: The effect of digitalisation of frequency voiding charts on compliance in paediatric patients. Randomised controlled trial comparing digital and versus paper frequency voiding charts by Liesbeth L de Wall, Elisabeth AM Kragt, Eline HM Van De Wetering, Johanna GL Cobussen-Boekhorst, Joyce Mantel-van Stel, Barbara BM Kortmann, Wout F Feitz and Charlotte MHHT Bootsma-Robroeks in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076231207577 - Supplemental material for Challenges in e-Health: The effect of digitalisation of frequency voiding charts on compliance in paediatric patients. Randomised controlled trial comparing digital and versus paper frequency voiding charts
Supplemental material, sj-docx-3-dhj-10.1177_20552076231207577 for Challenges in e-Health: The effect of digitalisation of frequency voiding charts on compliance in paediatric patients. Randomised controlled trial comparing digital and versus paper frequency voiding charts by Liesbeth L de Wall, Elisabeth AM Kragt, Eline HM Van De Wetering, Johanna GL Cobussen-Boekhorst, Joyce Mantel-van Stel, Barbara BM Kortmann, Wout F Feitz and Charlotte MHHT Bootsma-Robroeks in DIGITAL HEALTH
Footnotes
Contributorship
LdeW as the principal investigator designed, directed and coordinated this study. HC-B and JM-vS are nurse practitioners who conducted the screening and asked the patients to participate. EK and EvdeW completed the informed consent procedure, data input and data management. BK, WF and CB-R provided conceptual and intellectual guidance for all aspects of the project. In addition, C.B-R was the second evaluator of the voiding charts and supported the data analysis conducted by LdeW and EK. The manuscript was written by LdeW and commented on by all authors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
Ethical approval
The study was approved by the local Research Ethics Committee (NL71348.091.19)
Guarantor
Liesbeth L de Wall
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.