
Abstract
Background and objectives
Heart failure requires complex and daily self-care that many patients struggle with for a range of reasons including limited health literacy, cognitive impairment, comorbidities, and emotional distress. This study describes the user-centred design and development of a mobile app (SmartHeart) to support comprehensive self-monitoring and improve self-care engagement for people with heart failure.
Methods
Building on previous co-design research and expert panel feedback, we developed an initial Figma prototype following user-centred design principles. Two online sessions were conducted with adults living with heart failure (n=7), including a focus group session and a follow-up individual feedback session. The same participants took part in both sessions to provide feedback on the functionality, aesthetics, navigation, and content. Data were analysed deductively based on heuristic principles of user interface design, with findings informing the iterative development of the SmartHeart mobile app. The functional app was tested in-home by two participants over two weeks to evaluate real-world usability and gather contextual feedback to inform further refinement.
Results
The SmartHeart prototype was developed through expert workshops and user feedback. Participants emphasised simplicity, leading to a streamlined design with clear navigation, adaptable graphics, and larger fonts. The app’s health tracking features were iteratively improved. User-driven modifications included personalised threshold alerts, simplified symptom reporting, and integrated medication reminders. Participants reported high satisfaction with the prototype interface and health monitoring capabilities; however, formative testing identified reliability issues that are being addressed prior to pilot evaluation. Findings primarily inform design refinements before evaluating clinical effectiveness.
Conclusion
The SmartHeart app was refined through user-centred design process involving direct feedback from individuals with heart failure, resulting in a self-care tool with user-friendly features, to be further evaluated in future research. These user-driven enhancements support self-care engagement and highlight the app’s potential for real-world use and broader clinical integration.
Introduction
Heart failure is a significant public health challenge worldwide.1–3 The global prevalence of heart failure was estimated to be between 1% and 3%, affecting 56.2 million people in 2019. 4 In Australia, it was estimated that approximately 511,000 people (2.1%) were living with heart failure as of 2017, with prevalence projected to rise due to population ageing, increasing prevalence of obesity and improved survival following cardiac events. 5 The burden of heart failure extends beyond individuals, exerting substantial pressure on families and the healthcare system. Around 75% of individuals hospitalised for heart failure are readmitted within 12 months, and approximately 30% die within one year of their initial hospitalisation, reflecting the serious and progressive nature of the condition. 5 Heart failure imposes a substantial economic burden on healthcare systems worldwide, with approximately 60% of the cost attributed to direct medical expenses such as hospitalisations and outpatient care, and the remaining 40% to indirect costs including lost productivity. 6 Notably, a large proportion of these hospitalisations are considered potentially preventable, underscoring the critical need for improved outpatient management and patient engagement in self-care. 5
Heart failure management guidelines recommend that people living with the condition engage in complex, daily self-care practices to help maintain health stability, reduce hospital admissions and mortality rates, and enhance their quality of life.7–10 This complex regimen includes monitoring symptoms (e.g., shortness of breath, fatigue, and oedema), tracking body weight to detect fluid retention, adhering to medication regimens, managing fluid intake and engaging in regular physical activity. 11 Barriers to self-care such as limited health literacy, cognitive impairment, comorbidities, and emotional distress, can impact on the ability and motivation to carry out these tasks.11–14
Digital health technologies, including wearable devices and smartphone applications (apps), have potential to improve self-care by continuously monitoring health parameters and behaviour (e.g., weight, blood pressure, physical activity, medication adherence) through connected sensors and ecological momentary assessment.15–19 These systems provide data-driven information about a person’s condition, detect potential deterioration, and deliver tailored, real-time feedback and recommendations, enabling timely responses and supporting earlier intervention and improved disease management. 18 When effectively designed and implemented, these technologies can contribute to improved clinical outcomes and enhanced quality of life for people with heart failure. 20
Despite their considerable potential, many previous heart failure self-care apps have been developed without adequate input from end-users, often leading to poor alignment with real-world needs, preferences, and capabilities. 21 This disconnect can result in usability challenges and low engagement and adherence.22–25 Incorporating user-centred design approaches (e.g., co-design workshops and iterative feedback loops) is critical for developing apps that are not only functional, but also user-friendly and effective in promoting sustained self-care behaviours. 26 One example is the Care4myHeart app, co-designed with people living with heart failure, caregivers, and clinicians. 27 The app enabled users to collect, track, and evaluate health data, and a 14-day usability study indicated that users recognised its potential to support self-care. However, features that required participants to manually enter data were used infrequently, highlighting the need for solutions that reduce user burden. 28 With advancing technologies, there is an opportunity to integrate connected devices (e.g., wearables and wireless sensors) that automatically collect information and deliver timely, personalised recommendations.
To address identified limitations, we developed the SmartHeart app as part of a broader research program that is building a smart health ecosystem (SmartHeart) for heart failure management in Australia 22 by integrating the app with connected devices for data collection, a conversational agent, and a clinician portal. An initial prototype of the app was developed prior to this study by drawing on prior research with people with heart failure and healthcare professionals. 29
This paper describes the co-design of the SmartHeart mobile app tailored to the self-care needs of individuals with heart failure in Australia. Through a collaborative, user-centred approach, we aimed to develop a technology-enabled solution that integrates self-monitoring capabilities with self-care support, enhancing the ability of people living with heart failure to manage their health, make informed decisions, and maintain long-term health independently.
Methods
Study design and app development process
This study utilised mixed-methods, user-centred design comprising a focus group and individual feedback sessions involving patients with heart failure, an expert panel exercise to prioritise feedback, and a two-week user testing period. The integration of qualitative feedback, structured prioritisation, and real-world usability testing enabled comprehensive identification and refinement of usability issues from both end-user and clinical perspectives.
This study adopted a formative, user-centred design approach aimed at identifying key usability issues and user needs to support iterative refinement rather than hypothesis testing or effectiveness evaluation. Accordingly, a formal sample size calculation or statistical power analysis was not performed, and the study did not aim to achieve theoretical saturation. Instead, data collection was guided by the point at which sufficient feedback was obtained to identify major usability concerns and inform design decisions.
Prior to this study, the research team developed a low fidelity prototype app using Figma (Figma Inc., San Francisco, United States of America), which allowed for an interactive wireframe simulation. 30 Prototype 1 included a symptom logging tool, visualisations of physiological data from connected devices (e.g., blood pressure monitor, smart scale, smartwatch), and personalised push notifications (i.e. messages that pop up on a mobile device and are used to deliver timely and relevant information to users even when they are not actively using apps.
To meet the aim of this study, feedback on Prototype 1 was obtained through a focus group session with people living with heart failure. Synthesised feedback from the focus group was prioritised by a research expert panel using the MoSCoW framework
31
and iteratively implemented over a two-month period to create a high fidelity prototype (Prototype 2). Participants then reviewed Prototype 2 in individual feedback sessions, and their insights guided the development of a functional app. This functional app was subsequently evaluated in a user testing stage with additional participants. An overview of the SmartHeart app development and design process is shown in Figure 1. SmartHeart app development process.
Ethical considerations
The study received ethical approval from the Deakin University Human Research Ethics Committee (HREC/76317/MH-202). Participants were fully informed about the study through a participant information sheet and consent form, which were emailed to them before data collection. Written informed consent was obtained from all participants during the pre-screening assessment prior to Focus Group session.
Reporting framework
This study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) to ensure comprehensive and transparent reporting of qualitative methodologies. 32 This structured approach enhances the credibility, transferability, dependability, and confirmability of the qualitative data presented. Specific details regarding each criterion are provided in the appendix (Supplemental File 1). In addition, the study was reported in accordance with the Good Reporting of A Mixed Methods Study (GRAMMS) checklist 33 (Supplemental File 2).
Participant eligibility, recruitment & screening
Eligible participants were adults aged 18 years or older, living with heart failure who had internet access, were able to read and understand English, and residing in Australia. Participants were recruited through two primary sources: (a) individuals who had previously taken part in related studies by the authors and had provided consent for future contact, and (b) through online advertisements on social media platforms, including Facebook and Instagram advertised across Australia.
A total of 16 patients expressed interest in participating. All were initially contacted via telephone for a brief pre-screening inte4rview to confirm key eligibility criteria, including diagnosis, language proficiency, internet access, and residence in Australia. Nine individuals were not enrolled because they either resided outside of Australia (n=6, ineligible) or were unavailable during the study period (n=3). Following the screening, seven participants met all eligibility criteria and were formally enrolled in the study.
Sample size was guided by established principles in usability and participatory design research, which indicate that small samples are sufficient to identify the majority of usability issues when participants are intensively engaged through qualitative methods such as focus groups, individual feedback sessions, and iterative testing.34,35 The final sample size for the qualitative design phase (n=7) was therefore considered appropriate and is consistent with participatory design approaches for prototype refinement,36,37 where intensive engagement with a small number of users enables in-depth exploration of experiences, preferences, and usability issues to inform iterative development. Participants were provided with full study details and invited to participate. Each consenting participant received a $100 voucher in recognition of their time and contribution.
Focus group feedback
A 100-minute online focus group session (using Zoom Videoconferencing platform) was conducted with seven participants in April 2023. The session was facilitated by four digital health researchers (AS; female PhD student, RD & PJ; both male research fellow) experienced in qualitative studies, user-centred design, and app development. Among the facilitators, one served as the lead moderator (RD), guiding the discussion and ensuring all key topics were covered. The remaining facilitators supported participant engagement, took notes, and managed technical aspects of the session. The discussion followed a semi-structured topic interview guide (Supplemental File 3), adapted from established mHealth usability and quality evaluation approaches,38–40 and developed collaboratively by the research team based on a review of existing literature, prior user feedback, and the objectives of the SmartHeart project. While the interview guide was not formally validated, it was reviewed by the multidisciplinary research team and pilot-tested internally to ensure clarity, appropriateness of wording, and relevance to the study aims before use in data collection.
The session commenced with a welcome and introductions, followed by an overview of SmartHeart system’s purpose and features. We then facilitated a discussion using event scenarios, which were developed by the research team in consultation with clinicians and based on common self-care challenges in heart failure (e.g., symptom monitoring, medication management, and monitoring blood pressure and heart rate). The scenarios were used to explore user needs, preferences, and expectations. In the latter half of the focus group, participants engaged in prototype testing and provided task-driven feedback on usability and functionality. Participants were asked to interact with Prototype 1 to complete navigation tasks and assess design elements such as layout, colour schemes, and menu organisation. Questions addressed prior experiences with health apps and devices, as well as assessing SmartHeart prototype for ease of navigation, functional features (e.g., menu labels), preferences for aesthetics, and content quality (e.g., usefulness of information). Privacy and security concerns were also assessed participants’ concern about SmartHeart app. Facilitators concluded the focus group by providing a summary of key insights gathered in the session and outlining how participant feedback would be used to inform the next phase of development.
Prioritisation exercise
Over the course of five meetings lasting 60 minutes each, an expert panel of digital health researchers, health care providers with expertise in managing heart failure (a cardiology physician and a cardiology nurse), software engineers, and a user experience designer (n=8) reviewed findings from the focus group. The panel applied the MoSCoW framework (Must have, Should have, Could have, and Won’t have for now) to prioritise user-identified needs and preferences for the SmartHeart app. 31 The prioritisation process was informed by a structured discussion and consensus. Each proposed feature was evaluated individually, in terms of clinical relevance, feasibility, and impact on the user. Each proposed feature was evaluated individually in terms of clinical relevance, feasibility, and impact on the user. During the MoSCoW prioritisation process, user-requested features were evaluated not only on perceived usefulness but also on clinical relevance, technical feasibility, safety considerations, resource requirements, and alignment with the scope of early-stage prototype development. Some features categorised as “Could have” or “Won’t have (for now)” were not dismissed as unimportant; rather, they were identified as requiring additional governance structures, ongoing moderation, or system-level integration that could not be adequately addressed within the current study phase. The process adopted group consensus to reach decisions, rather than voting, to ensure that every expert voice was considered appropriately. Once the features were prioritised, we undertook approximately two months of refinements, resulting in the development of Prototype 2 in Figma.
The following features were identified as Must Haves and were incorporated into the high-fidelity prototype (Figure 2): a) A one-click access point for key icons to enhance usability b) Timely reminders for measuring blood pressure, taking medications, and weighing in c) Grouping of reminders to reduce notification fatigue and minimise interruptions d) Line charts displaying trends for each biological sign (e.g., heart rate) e) A traffic light indicator system (green, amber, red) to reflect normal, borderline, and critical values f) Improved data presentation within each data tab to reduce user confusion and enhance clarity Prioritising SmartHeart features based on MoSCoW framework.

Individual feedback
Once Prototype 2 was developed, we carried out individual online feedback sessions (using Zoom Videoconferencing platform) with the same participants to understand whether the new features aligned with their expectations and their potential willingness to include the SmartHeart app as a part of their daily activities. These sessions each lasted for approximately 50 minutes and were conducted by one researcher (RD) in the month of September 2023. Participants were presented with Prototype 2 and were asked to complete a series of tasks that reflected the app’s core elements (e.g., symptom tracking), and to comment on usability, clarity of content, and overall relevance toward their self-care needs.
User-testing
Two male adults (both aged 66 years, Australian, and retired; one with a bachelor’s degree and high school diploma, respectively) with heart failure were recruited to use the functional SmartHeart system (mobile app and measurement devices) for two weeks. These participants were recruited separately from those involved in the focus group and individual feedback sessions, but using the same eligibility criteria described above to ensure consistency in participant selection. A trained researcher installed the system in each participant’s home, provided a demonstration, and addressed any questions to facilitate usage. To further support engagement, participants received a written user guide and weekly phone calls. Via the broader SmartHeart system, the app collected data on blood pressure, heart rate, weight, physical activity (steps), medication use, and symptoms. Medication use was supported by a generic Bluetooth-enabled motion sensor placed either on a participant’s pillbox or on the drawer/cabinet where medications were stored, depending on individual routines. The sensor detected movement events (e.g., opening or handling), which were timestamped and used as a proxy indicator of medication access, complementing patient self-reported medication confirmation via the app or voice interface. Usability was assessed at the end of two weeks using the System Usability Scale (SUS).41,42 Any challenges or issues with the system were documented during home visits and phone calls to support problem resolution and inform iterative improvements to the app after the testing period.
Analysis
Focus groups and individual feedback sessions were recorded and transcribed verbatim, and data were analysed in NVivo (Version 14, QSR International Pty Ltd). Quantitative data, including participant demographics and SUS scores, were summarised using descriptive statistics (means, standard deviations, and ranges) to characterise the sample and provide an overview of usability outcomes. A deductive content analysis based on heuristic principles of user interface design 43 was conducted to systematically categorise feedback about core app features and known areas of usability (function, navigation, aesthetics, clarity of content, and potential improvements). The analysis involved an initial phase where the researchers (AS and RD) undertook a process of familiarisation with the data, and independently read and re-read transcripts and documented relevant excerpts linked to the pre-existing categories. All transcripts were divided into discrete units of meaning and coded. An initial coding table of categories was developed with AS and RD, which was then refined iteratively through the analysis process to capture any subtleties of user feedback that extended the original categories. RD carried out the primary coding, and themes within categories were reviewed, validated, and approved by both researchers to improve reliability. The findings were synthesised to address design modifications for the app’s next version, as the research provides insight into potential modifications of that iteration of the app.
Results
Participants
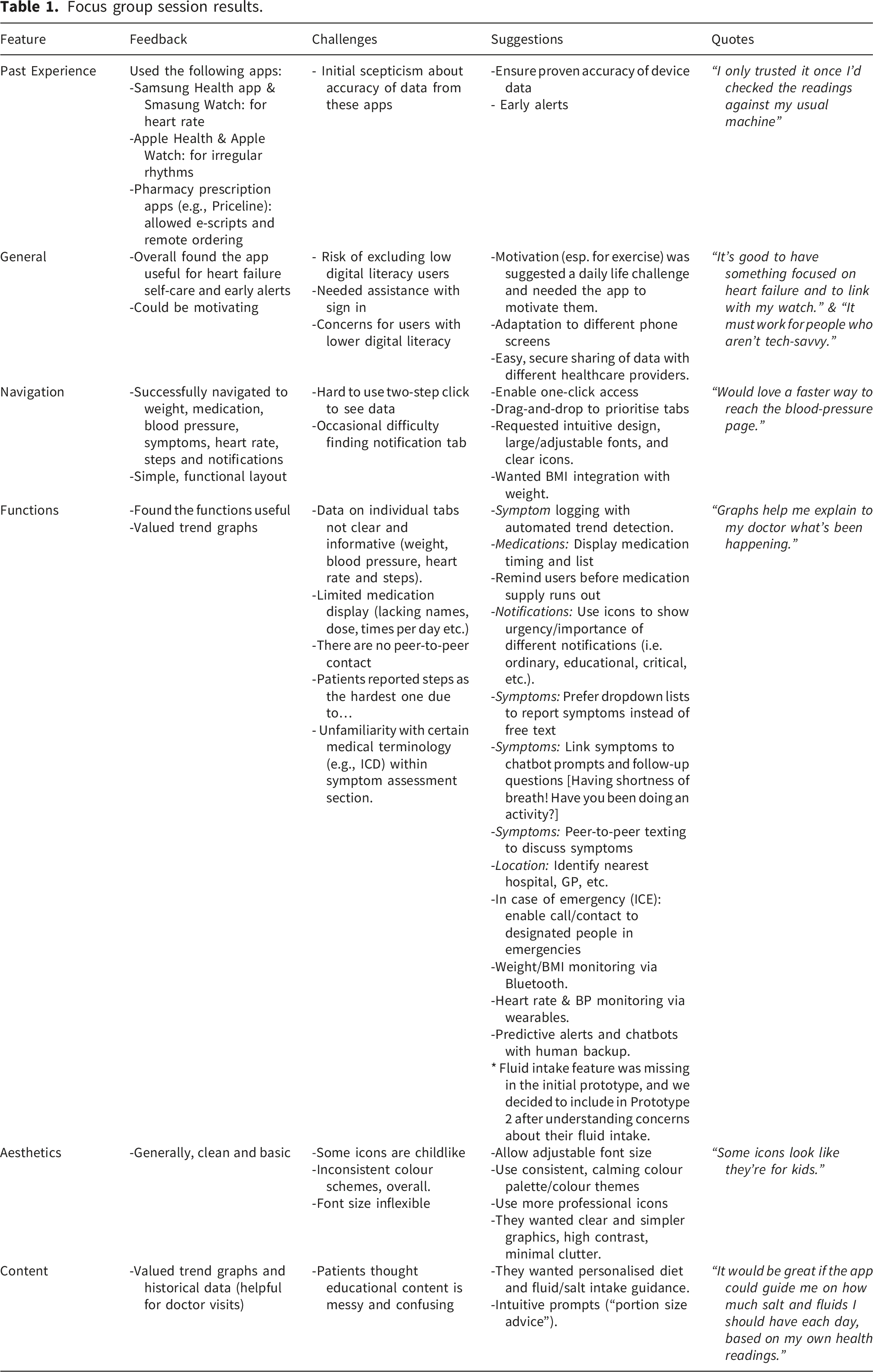
Focus group session results.
Individual feedback session results.


Iterated version of SmartHeart app.
Focus group findings
Overall, focus group session demonstrated interest in digital tools specific to heart failure self-care and identified priorities to improve usability, personalisation, and integration with clinical care.
Past experience with digital health/tech/apps: Participants described gradual trust-building with commercial health apps once accuracy was confirmed (e.g., “I only trusted it once I’d checked the readings against my usual machine”). They valued convenient self-monitoring and emergency alerts (e.g., Apple Health) but expressed scepticism about initial data accuracy and reported difficulty sharing results with multiple healthcare providers. General aspects: The app’s purpose—supporting heart-failure self-care and providing early warning i.e. alerts—was well received. However, participants highlighted the complexity of information exchange across different clinicians and emphasised the need for strong privacy safeguards and easy, selective data-sharing functions (“It’s good to have something focused on heart failure and to link with my watch”). The app was seen as a motivational self-management aid, but there was concern it might exclude those with limited digital literacy levels. Suggestions included comprehensive onboarding tutorials and multi-platform support. Although live sign-in was not yet implemented, participants expected a simple, step-by-step process compatible with both iOS and Android (“It needs to be easy to start, like one clear button to get in”). Navigation: Users found the interface simple and functional, with clearly recognisable icons, but complained of “too many taps” to reach specific data. They recommended one-click shortcuts and the ability to reorder tabs. Functional aspects: Key functions (e.g., symptom logging, blood-pressure and medication tracking) were valued, and trend graphs were found useful for clinical consultations (“Graphs help me explain to my doctor what’s been happening”). Gaps included incomplete medication histories and lack of peer-to-peer communication. Suggestions focused on improving health management by adding structured symptom logging with automated trend detection, dropdown-based reporting (e.g., fluid intake), chatbot follow-ups, peer-to-peer support, and predictive alerts backed by human assistance. Participants suggested that medication management should include clear timing displays, refill reminders, and notification icons that highlight urgency levels, while monitoring features cover weight or body mass index (BMI), heart rate, blood pressure, and now fluid intake. Participants suggested that emergency support could be enhanced through quick access to contacts, nearby hospitals or GPs, and designated in case of emergency (ICE) calls. Aesthetics/visual design: a generally clean appearance was appreciated, but some icons were perceived as “child-like”, colours inconsistent, and fonts non-adjustable. Participants recommended using professional icons and adjustable fonts. Content & information: Participants wanted concise but customisable summaries and the ability to record symptom “triggers.” They also sought personalised dietary guidance, including fluid and salt limits (“It would be great if the app could guide me on how much salt and fluids I should have each day, based on my own health readings”.
Individual session findings
Individual sessions confirmed the value of iterative design. Prior concerns about aesthetics and clarity were largely resolved, and attention shifted to enhanced personalisation, broader content (diet/fluid guidance), and seamless clinical integration for future development. General aspects: The app was viewed as purpose-built and senior-friendly, with clear colour coding (i.e. traffic light indicator) and labelling. Sustaining long-term engagement and providing continuous clinical linkage were identified as next challenges. Building on earlier exposure, participants reported increased confidence and motivation to engage with a heart-specific app. They mentioned the importance of data privacy and ongoing technical support. The live registration page (name, email, phone, password) was judged “very straightforward,” though testing revealed minor confusion from developer placeholder names. Visual cues and assisted onboarding were advised for less tech-confident users. Navigation/usability: One-touch access to blood-pressure, weight, step count and symptom pages was praised (“They’re easy to see—you can figure them out from the picture as well as the written text”). Occasional difficulty returning to the home screen (either by pressing the home button or backwards arrow) suggested the need for quick-start guides and on-screen tips. Functional aspects: Comprehensive self-monitoring with automated colour-coded alerts and historical trends was valued. Participants requested flexible manual entry for extra readings and linkage of medication changes to blood-pressure trends. Aesthetics/visual design: Colours and fonts were balanced and easy to read. Users welcomed options for light/dark mode, colour-blind accessibility and more compact tiles. Content & information: Trend graphs and reminders were highly regarded, but participants wanted broader fluid-intake tracking with drop-down icons for different fluids such as tea, coffee and soups, and optional wellbeing prompts such as mindfulness or relaxation. Other/future concepts: Enthusiasm emerged for longer-term innovations such as service robots or smart-home sensors to deliver medications and monitor vital signs, while recognising cost and feasibility constraints.
The SmartHeart functional app
Using user design principles and incorporating user feedback we iterated the app to ensure features aligned with user needs and preferences. These requirements directly informed the final feature specifications, which were tailored to support self-care among patients with heart failure. The primary features of SmartHeart end-product included 1 Weight tracking: integration with a Bluetooth-enabled weight scale allowed for automatic transfer and monitoring of daily weight data. 2 Blood pressure monitoring: A Bluetooth-enabled blood pressure cuff was used to record blood pressure measurements. 3 Physical activity monitoring: physical activity data, including steps taken and heart rate, were collected through a smartwatch equipped with an accelerometer and heart rate sensor. 4 Fluid intake tracking: the app allowed users to manually log their daily fluid intake through an easy-to-use interface. 5 Medication intake: users confirmed their medication intake using the app or a voice-assisted device. A medication sensor (i.e. motion sensor) detected pillbox movement (i.e. openings) serving as a proxy of medication use, adding an extra layer of data for verifying adherence. 6 Symptom reporting: daily symptom check-ins enabled users to report symptoms such as fatigue, shortness of breath, and swelling. 7 Real-time syncing: data from connected devices were synced in real time (within one minute, except for steps data), allowing for up-to-date monitoring. 8 Alerts: the app generated threshold-based alerts for abnormal weight, blood pressure, or symptom changes, helping prompt early action. 9 Accessibility and customisation: users could adjust font size, switch between dark/light modes, tailor the interface to their preferences, include or exclude implantable cardioverter defibrillator (ICD) use. 11 Personalised user profiles: the app supported entry of individualised parameters such as dry weight and daily fluid restriction targets to enable tailored self-care tracking.
User testing results
The average SUS score was 71.25 (individual scores: 70.0 and 72.5). SUS consists of 10 items; each rated on a 5-point Likert scale ranging from strongly disagree 1 to strongly agree. 5 Scores below 50 indicate poor usability, 50–68 suggest below-average usability, 68–80 reflect good usability, and above 80 are considered excellent. Participants provided suggestions for improvements based on regular weekly contacts feedback and task-specific challenges. The main challenges participants reported included unreliable data syncing between the sensors and the app, slow app refresh rates on all pages, errors in the blood pressure graph made it difficult to distinguish between systolic and diastolic readings, and frequent loss of sensor Bluetooth connectivity with all sensors. Participant suggestions included improving data syncing and overall app performance, clearly distinguishing systolic and diastolic blood pressure readings, and resolving issues with fluid intake submission.
Discussion
The SmartHeart app was developed as part of a larger project to develop a remote monitoring ecosystem to support people with heart failure to self-care at home and to reduce avoidable heart failure-related hospitalisation. 22 Building on previous formative research, 29 we undertook a user-centred design process to develop the SmartHeart mobile app. The user-centred approach was chosen to align app features and design with user’s needs, and to enhance usability and functionality. Engaging participants in iterative sessions provided valuable insights into their challenges, preferences, and expectations that influence self-care behaviours for people with health failure, ensuring that the SmartHeart app offered practical and meaningful support for heart failure management.
The use of multiple data sources enabled triangulation of findings, whereby usability concerns identified in early qualitative sessions were confirmed and refined during real-world testing. Expert prioritisation further contextualised patient-identified needs within clinical workflows, ensuring that design modifications were both user-responsive and clinically appropriate.
Our user design approach led to the development of a mobile app that patients with heart failure perceived as usable, though further research is needed to assess real-world applications and effectiveness on behavioural and clinical health outcomes. These findings align with prior studies demonstrating that early assessment of patient needs and iterative stakeholder involvement enhance usability and adoption of mobile health applications. For example, Reimer et al. (2024) showed that applying a user-centred framework in the development of a cardiovascular prevention app enabled the identification of features and interface elements that improved usability and user satisfaction through structured, iterative feedback. 44 Similarly, Koumpouros (2022) reported that participatory design processes involving patients, clinicians, and technical experts facilitated the identification of user requirements and barriers during mobile health development. 45
Furthermore, research evidence suggests that involving potential users directly in design processes leads to higher acceptability, greater perceived relevance, and improved usability of digital tools—factors critical to long-term engagement and adoption. 46 Participants in our study emphasised the need for simplicity in design, tailored notifications, and visual clarity of graphs, which aligns with prior studies in cardiovascular care, where older adults frequently report technology-related barriers such as cognitive overload, low health literacy, and small device interfaces. 47 Most study participants indicated willingness to use the system daily, provided that these usability challenges are adequately addressed.
The integration of self-monitoring features including weight, blood pressure, and symptom tracking was viewed positively by participants, aligning with existing evidence that such tools may support behavioural activation, symptom recognition, and timely intervention in heart failure. 48 A recent meta-analysis of mobile health interventions for heart failure found improvements in self-care behaviours and reductions in hospitalisations when mobile health tools provided real-time feedback and interactive features. 49 SmartHeart’s combination of sensor and self-report data entry options addressed the need for both passive data collection and user control, a dual approach shown to increase compliance. 18
Several smartphone applications have been developed to support heart failure self-management. For example, Medly is a clinically integrated remote monitoring platform that combines symptom reporting with physiological monitoring and automated feedback, demonstrating feasibility and user acceptability across implementation studies.50,51 Both Medly and SmartHeart enable daily tracking of weight, blood pressure, and symptoms to support early detection of deterioration and reduce avoidable hospitalisation. 52
However, Medly has largely been implemented within specialised tertiary programmes and relies heavily on clinician dashboard monitoring and algorithm-triggered alerts. Published evaluations of Medly have identified challenges related to digital literacy, caregiver dependence, and integration within structured clinical workflows. 53 In contrast, SmartHeart was developed using an iterative, user-centred framework that prioritised usability, behavioural engagement, and adaptability across broader care contexts. Features such as a simplified interface, hybrid passive–active data entry, tailored context-sensitive notifications, and fluid tracking were incorporated to enhance autonomy and reduce user burden. Unlike more mature platforms such as Medly, SmartHeart has not yet undergone large-scale clinical evaluation or real-world implementation. A clinical trial is currently underway, representing an important step toward establishing its effectiveness, equity, and scalability across broader care contexts.
Participants also highlighted the importance of personalised, context-sensitive notifications and encouragement (i.e. data-driven messages and more proactive messages targeting behaviour change), which can enhance perceived usefulness and reduce alert fatigue. 54 This aligns with principles from persuasive systems design and just-in-time adaptive interventions, where context-specific tailoring of message content, timing, and tone improves digital intervention effectiveness. 55 Additionally, participants’ feedback on features such as fluid intake tracking, chatbot support, and ICE functionality points to the increasing demand for holistic, integrated support systems. These suggestions support calls from digital health researchers for designing comprehensive platforms that consider physical, psychological, and social determinants of health. 56
The SmartHeart app demonstrated above-average usability, which indicates good usability and user satisfaction. 57 Although only two participants were involved in testing the app and the findings should therefore be interpreted with caution, this finding is promising given that both participants were older adults, a population often reported to experience greater challenges when adopting digital health.58,59 Technical issues including data syncing failures, delayed refresh rates, graphical errors in blood pressure visualisations, and frequent sensor Bluetooth disconnections can significantly impact sustained engagement and adherence. 60 Addressing these technical shortcomings is critical to enhance user experience, especially those who may be less resilient of inconsistent system performance. 61 Technical issues experienced in our study were resolved with subsequent iterations of the SmartHeart app with the aim of prioritising technical reliability and intuitive design modifications informed by user-centered feedback.
Despite these promising findings, this study has several limitations. Participants who chose to take part in the study may have had a greater interest or comfort in using technology, potentially introducing selection bias. Future studies should seek to include a more diverse sample and explore accessibility across varying health and digital literacy levels. Furthermore, while qualitative feedback offers insights into usability and user perceptions, the study did not collect objective usage data. In addition, clinical characteristics of participants (e.g., left ventricular ejection fraction or LVEF, B-type natriuretic peptide, New York Heart Association [NYHA] class) were not collected. As a result, it was not possible to examine how underlying heart failure severity or overall health status may have influenced app engagement, usability perceptions, or feedback. Future research should incorporate clinical profiling to better understand the relationship between patient disease characteristics and digital health intervention use. Although the semi-structured interview guide was informed by established mHealth usability frameworks, reviewed by a multidisciplinary team, and pilot-tested internally, it was not formally validated, which may have limited the comprehensiveness or consistency of the data collected. Additionally, medication adherence was inferred using a motion sensor placed on a pillbox or medication storage location; while this provided an objective proxy of medication access, it does not confirm actual medication ingestion. The small sample sizes across the qualitative and user-testing phases limit the generalisability of findings; however, this aligns with formative usability research, where intensive engagement with a small number of participants is used to identify key usability and interaction issues to inform iterative refinement. User testing with two participants enabled detailed observation of real-world system use but captured limited variability in user experiences. These stages formed part of a staged evaluation approach, and a larger pilot study has subsequently been completed to provide a broader assessment of usability and user experience. Although formal saturation analysis was not conducted, the formative usability focus meant that later sessions yielded largely repetitive feedback. Future studies with larger and more diverse samples may identify additional user needs. Incorporating real-world usage patterns, such as feature engagement rates and app session frequency and duration, cross-sectionally and longitudinally, could help quantify app impact on user engagement and guide adaptive refinement. We acknowledge these limitations and aim to address them in the next phase of evaluation, which is currently underway. This subsequent stage will involve a larger and more diverse group of participants, allowing for more robust findings and a stronger assessment of the app’s usability and overall effectiveness.
Conclusions
This study illustrates the value of iterative, user-centred design in developing a digital health intervention for heart failure management. The SmartHeart app demonstrated relatively positive levels of acceptability, perceived usefulness, and usability across key health self-care domains. These findings lay the groundwork for subsequent pilot testing and real-world trials to assess engagement, clinical outcomes, and scalability.
Supplemental material
Supplemental material - User design and testing of SmartHeart: A mobile app for heart failure self-care
Supplemental material for User design and testing of SmartHeart: A mobile app for heart failure self-care by Reza Daryabeygi-Khotbehsara, Paul Jansons, Yuxin Zhang, Rebecca Amy Nourse, Jonathan Rawstorn, Ann Tresa Sebastian, Dominika Kwasnicka, Teketo Kassaw Tegegne, Tilman Dingler, Vassilis Kostakos, Jo-Anne Elizabeth Manski-Nankervis, John Atherton, Brian Oldenburg, Rajesh Vasa, Gavin Abbott, Andrea Driscoll, Paul Scuffham, Anthony Maeder and Ralph Maddison in Digital health.
Supplemental material
Supplemental material - User design and testing of SmartHeart: A mobile app for heart failure self-care
Supplemental material for User design and testing of SmartHeart: A mobile app for heart failure self-care by Reza Daryabeygi-Khotbehsara, Paul Jansons, Yuxin Zhang, Rebecca Amy Nourse, Jonathan Rawstorn, Ann Tresa Sebastian, Dominika Kwasnicka, Teketo Kassaw Tegegne, Tilman Dingler, Vassilis Kostakos, Jo-Anne Elizabeth Manski-Nankervis, John Atherton, Brian Oldenburg, Rajesh Vasa, Gavin Abbott, Andrea Driscoll, Paul Scuffham, Anthony Maeder and Ralph Maddison in Digital health.
Supplemental material
Supplemental material - User design and testing of SmartHeart: A mobile app for heart failure self-care
Supplemental material for User design and testing of SmartHeart: A mobile app for heart failure self-care by Reza Daryabeygi-Khotbehsara, Paul Jansons, Yuxin Zhang, Rebecca Amy Nourse, Jonathan Rawstorn, Ann Tresa Sebastian, Dominika Kwasnicka, Teketo Kassaw Tegegne, Tilman Dingler, Vassilis Kostakos, Jo-Anne Elizabeth Manski-Nankervis, John Atherton, Brian Oldenburg, Rajesh Vasa, Gavin Abbott, Andrea Driscoll, Paul Scuffham, Anthony Maeder and Ralph Maddison in Digital health.
Footnotes
Acknowledgements
We thank all participants for their valuable input through focus groups, interviews, and user testing. Their contribution informed the design and development of SmartHeart mobile app.
ORCID iDs
Consent to participate
All participants provided written informed consent before participating in the study.
Author contributions
RM: Conceptualisation, Supervision, Software conceptualisation, Writing, review & editing. RD: Conceptualisation, Methodology, Investigation, Formal analysis, Software prototyping, Writing, original draft. PJ: Investigation, Software conceptualisation, Writing, review & editing. AS: Investigation, Formal analysis, Writing, review & editing. YZ: Software development, Prototyping, Validation, Writing, review & editing. RAN: Methodology, Writing, review & editing. JR: Methodology, Writing, review & editing. All authors reviewed, made changes and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a National Health and Medical and Research Council grant (grant number 2018698). However, the funding agency did not play a part in the design, execution, analysis, or interpretation of this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.