
Abstract
Objectives
The optimal utilization of routine health data remains underdeveloped in many developing countries, largely due to complex institutional and systemic factors. Although multiple initiatives have been introduced to promote data use, their impact has been inconsistent. This study explores the current practices of routine data utilization within the Tanzanian health system, identifying challenges and opportunities for strengthening the Health Management Information System (HMIS) for institutionalized data-driven decision-making.
Methods
This qualitative study employed in-depth interviews with 18 key informants, purposively selected based on their direct involvement in routine health data management, service monitoring, and policy implementation. This included facility HMIS focal persons, in-charges and council program coordinators from two selected districts of the Dodoma region. Data were analyzed thematically using the Performance of Routine Information System Management (PRISM) framework as a lens to routine data use.
Results
The study revealed that foundational components for establishing a data-driven health system are emerging. However, progress is constrained by persistent challenges, including data fragmentation across multiple platforms, limited technical capacity in data analysis and interpretation, and insufficient resources for maintaining data quality and promoting evidence-based practices. These barriers collectively weaken the institutionalized use of routine health data in decision-making processes.
Conclusion
To institutionalize the routine use of health data in Tanzania, a comprehensive and sustained approach is required. This should include system integration, capacity-building initiatives for health personnel, and improved institutional support mechanisms to enhance data quality, accessibility, and utilization for informed health sector decisions.
Introduction
The concept of “data use” refers to the analysis, synthesis, review, and interpretation of data to support decision-making processes such as program monitoring, policy development, and resource allocation, regardless of the data source. 1 Effective data use, therefore, extends beyond routine data collection and reporting; it requires the capacity to interpret data and derive meaningful insights. This often involves the application of indicators, which serve as measurable benchmarks that consolidate information from multiple sources. 2 In this regard, strengthening Health Information Systems (HIS) is essential for generating the data required to monitor and improve the quality of healthcare services. 3 When health data are effectively utilized, countries are better able to track progress, identify areas requiring improvement, and make informed decisions in pursuit of universal health coverage (UHC). 4
Most low- and middle-income countries (LMICs) rely on Routine Health Information Systems (RHIS), also known as Health Management Information Systems (HMIS), or in Tanzanian Swahili, Mfumo wa Taifa wa Usimamizi wa Huduma za Afya (MTUHA)—to systematically and regularly collect health data. 5 With increasing recognition of the value of routine data, substantial efforts have been made across developing countries to strengthen data collection, management, and use. These initiatives have focused on enhancing data quality, analytical capacity, visualization tools, and interoperability among electronic systems.6–8 Further, the adoption of digital platforms such as the District Health Information System (DHIS2) 9 Electronic medical records (EMR),9,10 and innovations, including dashboards and scorecards, have improved data accessibility and analysis, allowing healthcare workers to interpret complex information more efficiently.11,12
Despite these technological and structural investments, the effective use of routine data in many LMICs remains limited. A review of literature indicates that data collected at sub-national levels—such as district and facility levels are insufficiently used to guide local decision-making.13,14 Instead, these data are often viewed primarily as inputs for national-level reporting, rather than resources to support local planning and action. 15 Consequently, a significant proportion of collected data either “sits on shelves” or is used sporadically, often only in response to specific issues. 16 This pattern reflects a broader systemic weakness in formalizing and standardizing the use of routine data for strategic planning and performance monitoring. Persistent data quality challenges, limited technical capacity among health workers, and inadequate data governance structures are recurrent barriers.15,17 Additionally, limited skills in data analysis and interpretation, coupled with a disconnect between data collectors and end users, create significant bottlenecks. In a review by 18 identified shortages of human and financial resources, inadequate supervision, the absence of standard operating procedures, and fragmented vertical health programs. Collectively, these institutional challenges inhibit the consistent and effective use of routine data to inform health system actions.
Although several initiatives have been implemented within the Tanzanian health system to promote improved data management and use,19–21 their execution and documented impact have varied considerably. As a result, a substantial knowledge gap remains regarding actual data-use practices at the operational level. This study seeks to address this gap by qualitatively examining the landscape of routine data utilization within the Tanzanian health system, by assessing existing practices, identifying key challenges, and highlighting potential opportunities for institutionalization. The study aims to produce actionable insights that can strengthen the Health Management Information System (HMIS) and advance data-driven decision-making in public health.
The remnants of this paper are structured into the following sections: conceptual framework, methods, results, discussion, and conclusion.
Conceptual framework
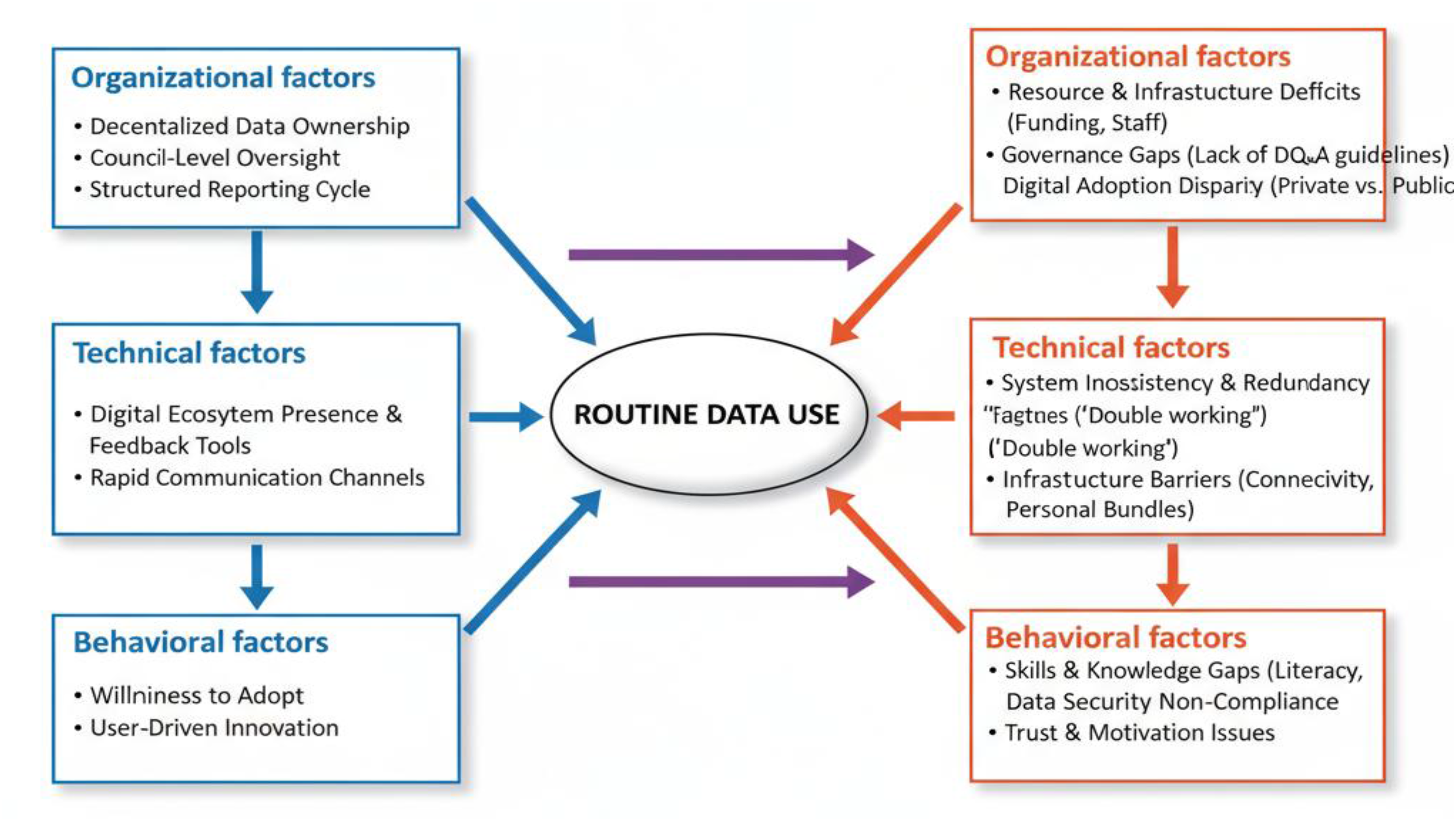
This study employs the Performance of Routine Information System Management (PRISM) framework 22 to conceptualize routine data use practices, along with the associated opportunities and challenges (Figure 1). The PRISM framework was developed to assess, strengthen, and evaluate the Routine Health Information System (RHIS) performance at both national and sub-national levels. Consistent with 14we apply the framework to categorize the determinants of data use into technical, organizational, and behavioral dimensions.

Conceptual framework (source: author's own customization from PRISM framework).
From Figure 1, we conceptualized the determinants of routine data use across three primary categories that collectively influence core RHIS processes. Technical factors, such as HIS design, software complexity, and the structure of reporting tools, interact with organizational factors, including governance arrangements, planning practices, resource availability, and training systems, to shape the operational environment. Together, these factors influence behavioral determinants among staff, including data demand, data quality assessment skills, confidence, and motivation to perform HIS-related tasks. The conceptual framework provides lens for analyzing RHIS processes, from data collection, analysis, action, and feedback mechanisms. These categories are used as themes for data analysis.
Methods
Study design
This study adopted a qualitative interpretive research approach 23 to generate in-depth insights into the challenges and opportunities shaping the use of routine health data within the Tanzanian health system. A qualitative interpretive design was selected because it enables exploration of social processes, contextual meanings, and the real-world dynamics surrounding data-use practices, elements central to understanding how routine health information systems (RHIS) function in practice.
Study setting
The research was conducted between November 2024 and March 2025 in two councils within the Dodoma Region: Dodoma City Council (urban) and Bahi District Council (rural). These sites were purposively selected to capture variation in organizational structures, levels of RHIS activity, and the degree of institutionalization of data-use practices, an approach consistent with qualitative sampling strategies aimed at maximizing contextual diversity. 24
Research team and reflexivity
The research team comprised three male researchers with dual academic training in qualitative research methods and Health Management Information Systems (HMIS). The first author is a PhD candidate with an MSc in Health Informatics. The two co-authors are senior researchers (PhD) specializing in health information systems, and they are supervisors to the first author. Collectively, the team possessed relevant expertise in digital health, health informatics, HMIS operations, and interpretive qualitative methodologies. This disciplinary alignment enhanced the rigor of data collection and interpretation, while reflexive awareness of the researchers’ backgrounds helped minimize potential biases throughout the research process. 25
Ethical considerations
The study adhered to established ethical standards for qualitative health research. Ethical clearance was obtained from the University's institutional review board, and formal approval was granted by the regional and council authorities in Dodoma. Participants were fully briefed on the academic purpose of the study, specifically its focus on examining data-use practices in routine health systems. Written informed consent was secured from all participants prior to interviews.
Participant selection and data collection
Sampling strategy and sample size
Data were collected through key informant interviews and direct observation. A total of 18 key informants were purposively selected based on their direct roles in routine health data management, decision-making, service monitoring, reporting, and policy implementation, consistent with purposive sampling principles for identifying information-rich cases. 26
As presented in Table 1, participants included HMIS focal persons responsible for managing DHIS2 data, facility in-charges responsible for facility management, planning, and quality improvement, and other healthcare workers who are also council health management team (CHMT) members engaged in RHIS activities, .e., council program coordinators such as Reproductive, Maternal, Newborn, Child and Adolescent Health (RMNCAH), Malaria and Immunization. No invited participant declined or withdrew. The majority of participants’ professional careers were Clinical officers (in charge of health facilities), followed by nurses acting in the role of HMIS focal persons. This provides more details on the normative driver of data use.
Roles distributions of participants.

Data collection sites
Data collection was conducted across 12 public health facilities—six within each council—complemented by interviews with two council-level managers. Facilities were purposively selected based on their active operational use of electronic data systems, specifically DHIS2, and were stratified across various service levels as detailed in Table 2. While two co-authors had previously implemented a health information system strengthening project within these districts, the Principal Investigator (PI) maintained no prior contact with the participants, mitigating potential researcher bias. Methodological rigor was ensured through formal research approvals from the university and relevant regional authorities. Before data collection commenced, the PI obtained written informed consent from all participants during the initial field visits.
Distribution of facilities included in the study.

Interview procedures
All interviews were conducted face-to-face by the first author at participants’ workplaces, typically during break hours, either in a private office or a reserved room. Only the interviewer and participant were present to ensure confidentiality. A semi-structured interview guide, pilot tested in one health facility, was used to maintain consistency while allowing flexibility for probing questions. Interviews lasted 25–30 min, were audio-recorded with participant permission, and supplemented with field notes. No repeat interviews were conducted. Data collection ceased once thematic saturation was reached, indicated by the absence of new insights from subsequent interviews. 27
Data analysis
Audio recordings were transcribed verbatim in Microsoft Word. The analysis followed a hybrid deductive–inductive thematic analysis approach. 28 To ensure methodological rigor, two researchers (BK and MM) independently reviewed and coded an initial subset of transcripts to develop a preliminary codebook through collaborative consensus (Table 3 attached as supplementary material). Findings within the manuscript are supported by verbatim participant quotations. To maintain anonymity while providing context, these quotations are attributed using labels that represent the participants’ respective duties/roles and facility service level, such as Facility In-Charge, Dispensary, Council Coordinator, etc.
Coding process
The coding process was structured hierarchically:
Primary categories informed deductively by the study's conceptual framework:
Opportunities Challenges Sub-categories aligned with the technical, organizational, and behavioral dimensions commonly used to assess RHIS performance.
22
Weekly peer debriefing meetings allowed the research team to refine emerging codes, discuss discrepancies, and ensure inter-coder reliability. The first author then applied the validated codebook to the remaining transcripts, with periodic checks by the full team.
Theme development
Deductive themes were initially aligned with the research questions, capturing existing “data-use practices” and “areas of data use.” Further thematic refinement drew on the conceptual framework (Figure 1), producing three major deductive dimensions:
1.Technical Factors: system design, software usability, reporting tools. 2.Organizational Factors: governance structures, human resources, supervision, and training. 3.Behavioral Factors: data skills, staff motivation, accountability.
Inductively, several new themes emerged from participant narratives, including:
Digital ecosystems and informal communication channels (technical dimension). Adoption disparities between public and private facilities (organizational dimension). User-driven innovation (behavioral dimension).
Results
The findings are presented in three major parts. First, the section describes existing data-use practices and the areas in which routine health data are applied. Second, it outlines the opportunities (enablers) and challenges (constraints) affecting data use, organized according to the PRISM framework dimensions: technical, organizational, and behavioral. Participant quotations are used to support key themes and are labeled according to the respondent's role.
Data use practices
Across facilities, routine data were being used in several ways despite notable limitations. Four dominant data-use practices were identified: visual performance monitoring, data discussion meetings, feedback mechanisms, and observational decision-making.
DHIS2-Derived paper-based visual monitoring
Many facilities produced printed visualizations from DHIS2—often displayed on noticeboards—to track trends, service coverage, and disease patterns. These A3 poster-style displays helped health workers interpret performance and identify areas for improvement. Some facilities demonstrated clear follow-up actions based on these visuals. For instance: “…In medical supply and ordering, we review data, especially the top ten reports, to see which medicines to order according to the burden. For example, our facility now orders medicine related to NTDs like Pressure and Diabetes… It's because our data shows we do get these patients.” (Facility In-Charge, Dispensary, Dodoma City)
Data discussion meetings
Most facilities held monthly or quarterly meetings to review key indicators and develop action plans. While no standardized format existed, these sessions consistently involved discussions on facility-mandated indicators and strategies for improving performance. When indicators were beyond the facility's sphere of influence, additional discussions occurred during quarterly council meetings. “…. We use staff meetings (daily brief meeting), health committee meetings, and HMT…” (Facility In-Charge, Health Centre, Bahi Council)
Feedback from higher levels
Feedback loops—primarily from council program coordinators—played a central role in helping facilities interpret their data. Coordinators frequently shared scorecards and performance dashboards through formal channels or WhatsApp groups, prompting facilities to take corrective actions. One participant described receiving monthly immunization performance updates: “…Sometimes we get feedback from the council, e.g., IVD scorecard shared monthly…” (Facility In-Charge, Dispensary 1, Dodoma City)
Observational decision-making
Health workers often made decisions based on observable trends not captured within formal systems. These “informal data” practices usually involved reviewing paper-based registers to identify recurring cases or community-level patterns. For example: “Sometimes we use observational data… we receive pregnant mothers from a nearby village where their culture promotes the use of traditional medicine… as a result, a mother is brought late and in bad conditions …” (ANC Coordinator, Hospital 1, Bahi Council)
These examples indicate that data use extends beyond DHIS2 and includes both formal and informal information sources.
Areas of data use
Routine health data supported multiple decision-making processes across facilities and councils. The main areas of application included:
Outbreak identification and response
Data trends were routinely monitored to identify unusual increases in disease incidence. In Dodoma City, an observed rise in malaria cases prompted a CHMT investigation, revealing that university students arriving from other regions contributed to the spike. Outreach interventions were then planned for student populations. “In one of our data review meetings, we noticed that Malaria cases are high in November and March… these cases are associated with University students…” (Participant, Health Center 1)
Service delivery improvement
Facilities used indicator performance, such as antenatal care timeliness or hemoglobin levels, to identify service gaps, investigate root causes, and implement targeted interventions (e.g., increased outreach, skill enhancement).
Resource allocation and procurement
Facilities relied heavily on “top ten diseases” data and disease burden patterns to guide budgeting and ordering of medical supplies. In one case, a dispensary began ordering supplies for non-communicable diseases after data revealed unexpected patient volumes for hypertension and diabetes.
Health education and promotion
Data were used to identify community health concerns and tailor education campaigns, such as addressing high diarrheal disease rates or adolescent UTIs.
Planning and monitoring
Data were central in preparing annual plans (CCHPs), monitoring service coverage, and evaluating progress toward targets.
Enablers and constraints to data use (PRISM framework)
Figure 2 summarizes the enablers and constraints identified in Dodoma and Bahi. Below, these are elaborated across organizational, technical, and behavioral dimensions.
Summary of enabler (blue text) and constraints (red text) dimensions.
Opportunities: enablers of data use
Organizational enablers
Decentralized data ownership
All public health facilities now conduct self-entry of data into DHIS2, improving data ownership and reducing delays previously caused by centralized data entry. Council teams have shifted toward verification and quality assurance. “…currently all public health facilities in Dodoma are reporting their data electronically through DHIS2…” (HMIS Coordinator, Dodoma City) “…Facility data entry has significantly improved not only data quality but also data ownership…” (HMIS Coordinator, Bahi Council)
Structured reporting cycles
Facilities adhered to monthly reporting deadlines, supported by an internal cycle where departments submit summaries before the 5th of each month. Some facilities also performed structured data-quality checks before DHIS2 entry. “….. we are keeping up with the deadline of reporting… this gives time to consolidate all the reports and do data entry early…” (DHIS2 Focal Person, Dodoma City). It was further reported, “…we… sit to check for quality of submitted data… If we note anything suspicious, we return the form… for validation …” (DHIS2 Focal Person, Dispensary, Dodoma City)
Technical enablers
Presence of a Digital Ecosystem: A robust suite of digital platforms, DHIS2, GoTHOMIS, eLMIS, and others supported planning, patient monitoring, supply chain tasks, and performance review. “…we use DHIS2 CCHP tables to generate data during the planning phase…” (In-Charge, Hospital, Dodoma)
“GoTHOMIS helps me to check staff workload… and make informed actions.” (In-Charge, Health Center, Dodoma)
Supportive HIS Design: Visualization tools such as the DoE Dashboard, RCH scorecards, and immunization scorecards simplified presentation and interpretation of key metrics. “… we have various visualization tools in DHIS2… these tools help to visualize and easily understand data…” (DHIS2 Focal Person, Bahi Hospital)
Informal Communication Channels: WhatsApp groups were widely used for rapid sharing of performance scorecards, reminders, and feedback. “I have a WhatsApp group of all MTUHA focal persons… this helps me in sharing feedback…” (HMIS Coordinator, Dodoma City) “…I often use a WhatsApp group to share a monthly scorecard… no one wants to see his/her facility has poor records.” (Malaria Coordinator, Dodoma City).
Behavioral enablers
Staff demonstrated motivation, willingness to adapt, and peer-learning initiatives.
Willingness and Motivation to Adopt: Training and peer support helped accelerate DHIS2 adoption. “…we have health workers who are highly motivated to do data work… we use them to train their peer workers…” (HMIS Focal Person, Dodoma City).
User-Driven Innovation: Staff created locally customized tools, such as Excel-based scorecards, to meet their analytical needs. Some printouts were kept on the notice board for the community to see, as shown in Figure 3. For instance, the immunization coordinator has customized an Excel-based scorecard and analytical figures to track vaccination coverage in the Dodoma city council.
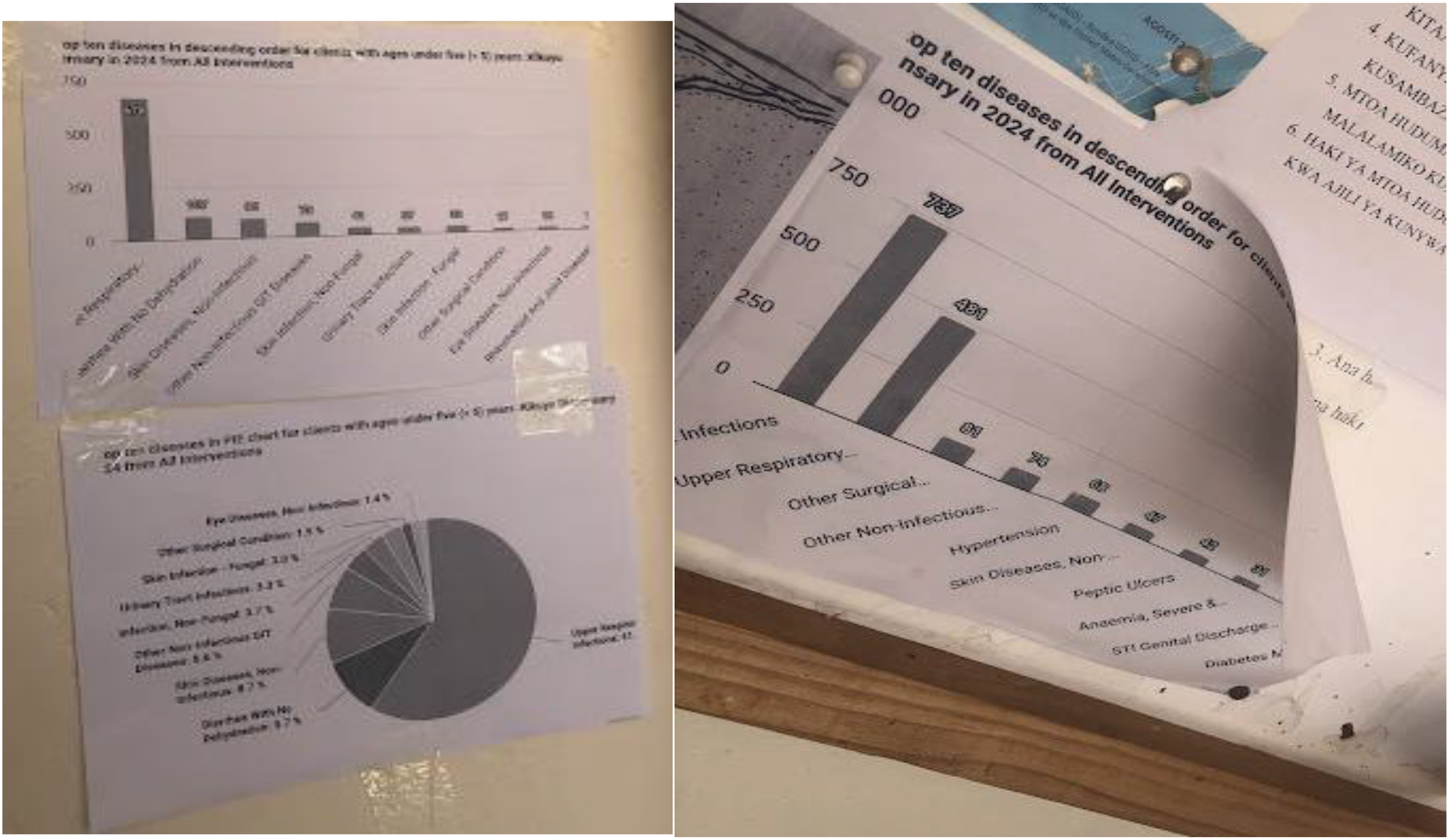
Print-out display on the facility's notice board.
Challenges: constraints to data use
Organizational constraints
Resource and infrastructure deficits
Shortages of funding, equipment, and staff weakened DQA efforts and placed heavy burdens on existing personnel.
Governance Gaps and Trust Issues: Irregular review meetings, absence of standardized DQA guidelines for digital systems, and unrealistic targets contributed to mistrust in the data. “Sometimes it's difficult to track the plan because you may set an activity… and then the fund is disbursed… so we go according to the availability of funds.” (Facility In-charge, dispensary 3, Dodoma city)
Digital Adoption Disparities: Private facilities still rely on paper submission, creating a two-tier data-entry system and undermining consistency. The HMIS coordinator responded that “We have managed to go paperless in public facilities, but in private facilities, still submit their paper summary form to the council for data entry.” (HMIS Coordinator, Dodoma council) “Their reliance on paper forms reduces data ownership and data quality; as a result, they don’t analyze their data for local use” (IVD coordinator, Dodoma city)
Technical constraints
System inconsistency and redundancy
Multiple parallel systems collect similar data. For instance, an HIV positive pregnant mother has to be registered in more than three systems, i.e., GoTHOMIS, CTC, Kituoni App, and later aggregated to DHIS2. This created duplication and inconsistencies between paper and digital records. “…The duplication of GoTHOMIS and registers… creates a duplication of work…” (MTUHA Focal Person, Dispensary 2, Dodoma City).
Fragmented systems
There are silos of electronic systems that do not communicate (un-integrated systems). For instance, DHIS2, GoTHOMIS, eLMIS, FFARS, CTC, AfyaSS, NHIF, and others operated in silos with little interoperability.
Poorly managed updates
Frequent, uncoordinated updates caused mismatches between tools and summary forms.
Infrastructure limitations
Poor network connectivity, reliance on personal internet bundles, and limited access to performance dashboards constrained effective data use. “There is only one MTUHA focal who has access to the DHIS2 system…” (Facility In-Charge, Dispensary, Bahi Council)
Behavioral constraints
Skills and knowledge gaps
Despite the computerization in most facilities, the healthcare workers’ ability to use these computers is still low. We observed that low computer literacy, limited analytical skills, and difficulty interpreting scorecards hindered effective data use.
Data security risks
While WhatsApp accelerated communication, it also introduced risks to data confidentiality and integrity. Some health workers acknowledge sharing their personal devices with relatives, which could breach data security.
Trust and motivation issues
At the council level, there are experienced trust issues with data that are submitted from private facilities. It was noted that some submissions contain unrealistic data, often influenced by external pressure, indicating weak motivation for data validation and compromised system reliability.
Discussion
This study provides valuable insights into the Tanzanian health system's progression in routine data use, highlighting both notable achievements and persistent challenges. The findings are consistent with, and in some cases extend, the existing literature on the underutilization of routine health data in low- and middle-income countries (LMICs).13,29 As in many LMICs, the results confirm that although Tanzania has established core components of a digital health ecosystem—including the rollout of DHIS2 the system remains fragile. This fragility stems from persistent issues such as data fragmentation across vertical programmes, limited technical and analytical capacity, and continued dependence on informal data-sharing pathways.6,30,31
The analysis deepens understanding of how behavioral and organizational factors intersect with technical constraints to limit evidence-based decision-making in LMIC settings. Consistent with studies from Ethiopia and Nigeria32,33 the findings demonstrate that despite the availability of routine data, its use in local decision-making processes remains low. This gap is largely attributable to weak behavioral and organizational determinants within the PRISM framework. Participants frequently reported limited capacity in data analysis, interpretation, and visualization—deficits that diminish their confidence and motivation to engage with information generated by the RHIS.8,20,34
A striking finding of this study is the pervasive reliance on instant messaging platforms, specifically WhatsApp, for sharing routine health data, particularly for quick decision-making and performance monitoring. While the use of readily accessible social media technology like WhatsApp is a common global phenomenon, it often serves as a practical solution to communication barriers, network instability, and the perceived complexity of formal systems.35,36 This highlights a critical failure in digital health governance 37It exposes risks that create a parallel, ungoverned data flow that bypasses established security and ethical protocols, raising serious concerns regarding patient confidentiality and data security.35,37 The present findings thus underscore the urgent need for Tanzania's national digital health strategy to issue clear protocols that either prohibit the use of unapproved platforms for patient and aggregate data, or formally integrate and govern their use under strict security guidelines.
Further, the identification of fragmented reporting across multiple platforms (DHIS2, GoTHOMIS, paper-based forms) is consistent with the fragmentation of HIS observed across digital health ecosystems in most LMICs. 8 This study's finding that staff must manually cross-reference data from different systems for monthly reports mirrors the challenges reported in Kenya and Uganda, where vertical applications hinder the development of a holistic system.38,39 The resultant lack of system interoperability imposes a heavy triple burden on health workers: increased workload, duplicative data entry, and decreased trust in data accuracy. 40 In that way, the National investments must pivot from piloting new, isolated systems to prioritizing a cohesive, interoperable digital backbone that integrates the various data sources at the point of care.
However, the innovative motivation of some staff, like using workaround solutions like MS Excel scorecards, provides a unique contribution, highlighting a key organizational opportunity. This aligns with the principle that data use is driven not just by technical capability but by data demand and accountability mechanisms.13,14 By formally leveraging these innovations mandates and integrating their data needs into the RHIS feedback loop, the system can cultivate the “information culture” that is frequently absent in LMIC health systems. The intervention is not merely technical training for data clerks, but strategic capacity building for managers and governance bodies (HFGC, CHMT) to effectively use data as a mechanism for performance management. 1
Limitation
This study offers substantial qualitative insights into the challenges and opportunities influencing routine data use within the Tanzanian health system; however, two key limitations should be acknowledged. First, the focus on only two councils, Dodoma City Council and Bahi District Council, constrains the generalizability of the findings to the broader Tanzanian health system or to other low- and middle-income regions without similar initiatives. Nonetheless, these councils were purposively selected to reflect contrasting resource environments, thereby capturing a degree of institutional diversity. Second, the study's reliance on key informant interviews, while valuable for eliciting perspectives from CHMT and HFGC members, may introduce bias, as participants could portray their practices or perceptions more favorably. Future research should include a larger number of councils and adopt a longitudinal approach to validate and extend the findings reported here.
Conclusion
This study concludes that while the foundation for a data-driven health system exists in Tanzania, its potential is significantly limited by the systemic interplay of technical fragmentation, weak digital governance, and underdeveloped behavioral competencies, consistent with broader challenges in most LMICs. The reliance on informal channels like WhatsApp for data sharing is a pragmatic coping mechanism for system failures, yet it simultaneously creates critical risks related to data security and integrity. To truly transition from data collection to meaningful information use, the policy focus must shift from merely deploying silos of digital tools to prioritizing interoperability, institutionalizing data demand and accountability mechanisms, and enforcing clear protocols that govern both formal and informal information flows. Strengthening these interconnected determinants, technical, organizational, and behavioral, is essential for cultivating a sustainable culture of data use that supports evidence-based health decision-making.
Recommendation
To strengthen data use practices, we have drawn the following recommendations, targeted at relevant stakeholders (policymakers, HMIS implementers, and Health workers)
Strengthen Governance and Institutional Support for Routine Data Use by:
Developing guidelines for Data Quality Assurance (DQA) in digital systems. Formalizing and resourcing routine data review meetings at both facility and council levels. Ensuring targets are collaboratively set and context-specific to reduce unrealistic reporting and rebuild trust in the system. Improve Interoperability and Harmonization of Digital Health Systems by;
Accelerating implementation of interoperability standards and national enterprise architecture. Reducing redundant data entry by integrating clinical, administrative, and reporting systems. Providing clear communication before system updates to minimize confusion and mismatched tools. Build Workforce Capacity in Data Literacy, Analysis, and Use, by
Provide continuous, on-the-job training focused on data interpretation, use of DHIS2 dashboards, and basic analytics. Expand system access beyond focal persons so in-charges and relevant staff can directly interact with performance data. Promote peer-learning models by formalizing the roles of internal “data champions” who can mentor fellow health workers.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261433642 - Supplemental material for Routine data use practices: Opportunities and challenges for institutionalization at sub-national levels of the Tanzania health system
Supplemental material, sj-docx-1-dhj-10.1177_20552076261433642 for Routine data use practices: Opportunities and challenges for institutionalization at sub-national levels of the Tanzania health system by Bigten Kikoba, Masoud Mahundi and Wilfred Senyoni in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076261433642 - Supplemental material for Routine data use practices: Opportunities and challenges for institutionalization at sub-national levels of the Tanzania health system
Supplemental material, sj-docx-2-dhj-10.1177_20552076261433642 for Routine data use practices: Opportunities and challenges for institutionalization at sub-national levels of the Tanzania health system by Bigten Kikoba, Masoud Mahundi and Wilfred Senyoni in DIGITAL HEALTH
Footnotes
List of abbreviations
Acknowledgments
I would like to express my sincere gratitude to all the individuals and organizations who made this work possible. My deepest thanks go to the University of Dodoma, under the HEET Project, for generously funding my PhD studies, and to the University of Dar es Salaam for granting the necessary research clearance as a PhD candidate. I also extend my heartfelt appreciation to my family, especially my wife Mariam and daughter Editha, for their unwavering support and encouragement throughout this research journey. Finally, I am grateful to the journal Editor and reviewers for their insightful comments and feedback, which significantly improved the quality of this manuscript.
Ethical considerations
Research clearance for this study was secured from the Vice Chancellor of the University of Dar es Salaam. This authority is granted under the Government Circular Letter Ref. No. MPEC/R/10/1, dated July 4, 1980, which authorizes the Vice Chancellor to issue research clearances to University staff and students on behalf of the Government and the Tanzania Commission for Science and Technology (COSTECH). The clearance document was subsequently submitted to the Regional Administrative Secretary and District Executive Directors to obtain final ethical approval. Ethical integrity was maintained throughout the study: Informed consent was obtained from all participants before data collection, and their confidentiality and anonymity were strictly maintained.
Consent to participate
Written informed consent was secured from all participants prior to interviews
Consent for publication
Not applicable, as no data from a third person (including individual details, images, or videos) were used in this manuscript.
Author contributions
B.K.: Research conceptualization, methodology design, data collection, and writing the main manuscript; M.M.: Validation of data collection tools, transcript coding, review analysis scheme, review, and editing of manuscript. S.W: Supervision, Validation of data collection tools, review, and editing of manuscript.
Funding
This research was undertaken as a PhD study of the first author, sponsored by the University of Dodoma, under the HEET Project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data underlying this article are available in the article and in its online supplementary material.
Supplemental material
Supplemental material for this article is available online.
Author biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.