
Abstract
Objective
Men grappling with infertility often face emotional distress due to stigma and masculinity norms. Social support is vital in coping with infertility, and with the rise of digital health, much of it has shifted online. However, Dutch-speaking online infertility support groups (OISGs) remain unexplored, especially regarding male support inclusion. Existing research focuses on message content, offering limited insight into user demographics and usage patterns. Men's online support experiences are largely unexplored, and studies rarely examine online and offline networks together, despite their combined importance for support and wellbeing. This study addresses these gaps through three objectives: (1) explore the availability of Dutch- speaking OISGs and their inclusion of male-specific support; (2) map characteristics of male users and their usage of OISGs; and (3) understand how men experience online versus offline infertility support, and what factors shape their use.
Methods
A multistage mixed-method design was used in Flanders and the Netherlands, comprising three sequential components: (1) an environmental scan; (2) an online survey; and (3) online semi-structured interviews.
Results
Findings show that Dutch OISGs are scarce and male-specific support is not self-evident. Users are predominantly higher-SES, indicating selective access. Freya is the most used platform, with sustained but varied usage. Men's engagement is shaped by an interplay of digital and psychosocial factors, with perceived anonymity acting as a paradox. Online and offline infertility support are experienced as complementary, fulfilling different needs. The core distinction lies in the nature of relationships, peer versus intimate, rather than the medium. Support needs are dynamic across both settings.
Conclusion
These insights underscore the need for more, inclusive, and tailored support strategies that address the dynamic needs of men navigating infertility in both online and offline contexts.
Keywords
Introduction
Infertility affects millions worldwide, yet its global prevalence remains difficult to estimate due to inconsistent terminology and limited population-based data. 1 Male factor infertility accounts for approximately 30% of cases and contributes to up to 50% of all infertility diagnoses. 2 Defined as the inability to achieve a clinical pregnancy after twelve months of regular, unprotected intercourse, infertility can also refer more broadly to an impaired ability to reproduce. 3
Social support plays a crucial role in coping with infertility and improving psychosocial well-being. 4 However, support from family, friends, and health care providers is often insufficient, leading individuals to seek peer support.5,6 Support from those without similar experiences is perceived as less helpful. 7 Although effective, 8 professional counselling is not widely used, 9 since many value psychosocial support but do not feel they need psychological services. 10 The rise of digital health, accelerated by the COVID-19 pandemic, has shifted much of this peer support to online platforms.5,11 Increasingly, people experiencing infertility turn to the internet for both medical information and emotional support.12,13
Online peer support groups, also known as social support or self-help groups, enable individuals to share information, seek help, discuss challenges, and tell their stories to others with similar experiences. 14 These groups are often led by volunteers with personal experience on the topic, 15 and operate through forums, chat rooms, or messaging apps. 16
Men experiencing infertility face unique challenges. Stigma, threats to masculinity, and social expectations to suppress emotions contribute to significant emotional distress. 16 Research shows that men are generally less likely than women to seek help for sensitive health issues 17 or to engage in social support. 18 When they do seek help, they often prefer online over face-to-face support, particularly for stigmatized conditions like infertility. 19
Hegemonic masculine norms, emphasizing toughness, self-reliance, and emotional restraint, further discourage help-seeking. 20 Infertility can threaten men's sense of masculinity, given cultural associations between fertility, virility, and identity. 21 Qualitative studies show that men often feel pressure to be the emotional anchor in relationships, suppressing their own needs. 12
Digital environments may offer more acceptable spaces for men to seek support while navigating these gender norms. 22 Limited research suggests that men use online support groups to express hidden emotions and receive validation through shared experiences.12,23 These platforms are valued for their anonymity and accessibility, making them less threatening and more appealing.24,25
Despite growing interest in men's online help-seeking, no studies have explored Dutch-speaking online infertility support groups (OISGs), particularly regarding the inclusion of male-specific support. Existing research has focused primarily on English-speaking contexts such as the U.S., Canada, and the UK (e.g.,23,26–28), where reproductive systems differ from those in Belgium and the Netherlands, countries known for their progressive policies in assisted reproductive technologies (ART) and well-funded healthcare systems. 29 These contextual differences likely influence both the availability of OISGs and the degree to which they include male-specific support, highlighting the need for targeted research in Dutch-speaking contexts.
Additionally, most studies focus on message content (e.g.,23,26–28), offering limited insight into the sociodemographic profile of male users or their patterns of platform use.
Moreover, while gender norms shape help-seeking behavior, 30 and social support is key in coping with infertility,31,32 men's online support experiences remain under-researched compared to women. 28 In addition, although many individuals rely on both online and offline networks to cope, 33 most studies examine these separately, 34 despite evidence that both influence support and wellbeing. 35
These knowledge gaps restrict the ability to effectively support men dealing with infertility.12,26,36 Therefore, this study addresses these gaps through a multi-stage mixed method design conducted in Flanders (Belgium) and the Netherlands, with three objectives: 1) to explore the availability of Dutch-speaking OISGs and their inclusion of men, 2) to map information about the characteristics of men and their use of OISG, and 3) to understand how men experience online versus offline support, and what factors influence their use of these forms of support.
This study enhances the understanding of men's help-seeking behavior in the context of infertility and broader sensitive health issues. 16 The findings aim to inform support strategies in both professional healthcare and informal peer networks. 37
Method
Study context
This study was conducted in two neighboring Dutch-speaking regions: Flanders, the northern part of Belgium, and the Netherlands. Both countries are recognized as global leaders in ART, which include all treatments involving the in vitro handling of human eggs, sperm, or embryos to establish a pregnancy. 38
Their leadership in ART is supported by progressive policies, well-funded healthcare systems, and fewer legal restrictions on access to fertility treatments compared to many other EU countries.29,39 As a result, they jointly top the European Fertility Treatments Policies Atlas with 86%, a ranking tool that evaluates 43 countries based on equal access to safe and effective fertility care. 29
In addition to medical treatment, psychosocial care has become an integral part of fertility care, as most patients experience emotional distress during treatment. 40 Psychosocial care helps individuals and couples manage the emotional and social impact of infertility. 41 However, fertility clinics often lack the staff and resources to provide adequate psychosocial care, revealing a gap between policy and practice. 39
In this context, many individuals turn to online support groups to fill the psychosocial support gap left by healthcare providers, family, and friends. 5 This disconnection between well-established medical care and under-resourced psychosocial services makes Belgium and the Netherlands particularly compelling contexts for studying OISGs.
Study design
This study used a multistage mixed-methods design, involving three sequential stages of data collection and analysis. 42 Quantitative data were collected and analyzed first, followed by qualitative data. 43 Integration at the methodological level occurred through connecting, whereby the quantitative and qualitative components were linked via the sampling frame: at the end of the survey, respondents were invited to volunteer for follow-up interviews by leaving their email address. At the reporting level, a contiguous approach was used, presenting quantitative and qualitative findings in separate sections within a single article. 42
First, an environmental scan was conducted to map Dutch-speaking OISGs for men, addressing the question: What Dutch-speaking OISGs are available for men with infertility, and to what extent do they include support specifically for them? Second, a survey was used to identify users’ sociodemographic and usage characteristics, asking: What are the sociodemographic and usage characteristics of men who use Dutch-speaking OISGs? Third, online semi-structured interviews explored men's experiences with online versus offline infertility support and the factors influencing their use, guided by the question: How do men experience online versus offline infertility support, and what factors influence their use of these support forms?
Stage one – environmental scan
In June 2024, an environmental scan was conducted to assess the landscape surrounding male infertility, following the five-step framework of Shahid and Turin. 44 First, the purpose was defined: to map Dutch-speaking OISGs and assess the support they offer for men. Second, the research population was identified, focusing on OISGs that could meet inclusion criteria, with initial online contact planned with the representatives of the OISGs to verify eligibility. Third, the feasibility of the research question was confirmed. Fourth, a web search using Google was conducted (chosen for accessibility and coverage of publicly available communities). Search terms were adapted from prior work on men's online support groups 12 and translated into Dutch: “forums and/or online support group + male infertility/ men/ fertility problems.” Inclusion criteria required groups to: (1) focus primarily on infertility, (2) offer online support, (3) be Dutch speaking, (4) be currently active, and (5) be openly accessible. Finally, two OISGs met the criteria, and online meetings with their representative's confirmed eligibility, provided context on support practices, and formalized collaboration for participant recruitment. Given that OISGs are communities rather than single individuals, their moderators were consulted as the appropriate stakeholder representatives.
Stage two – survey
Based on the input gathered from the first stage, a 52-item online survey was developed using Qualtrics XM (Qualtrics, Provo, Utah, USA). 45 It included questions related to demographic characteristics, desire for children and infertility status, usage characteristics, usage motivation, stigma and disclosure, social support, and overall satisfaction with the OISG. The survey combined existing psychometric scales with author-developed items and was piloted by four volunteers with infertility experience, whose feedback led to refinement.
Participants were recruited via a convenience sample through the two identified OISGs from stage one between October 2024 and March 2025. One moderator from each OISG posted the survey link on their website and in newsletters, with one repost to boost responses. Eligible participants were Dutch-speaking heterosexual men aged 18 or older who were experiencing or had experienced infertility, were undergoing or had undergone ART, and were visitors of the stakeholders’ OISGs. Infertility causes included male, female, mixed, or unexplained factors.
The survey data was analyzed by the first author using IBM SPSS Statistics (IBM Corp., Armonk, New York, USA) 46 and summarized using descriptive statistics to provide an overview of participants’ sociodemographic and usage characteristics.
Stage three – semi-structured interviews
At the end of the survey, participants could leave their email to volunteer for an online semi-structured interview. This online format helped address the topic's sensitivity and overcome geographic barriers. 47 Of the ten who shared their contact details, eight men agreed to be interviewed. Additionally, two stakeholder moderators participated, resulting in ten interviews in total.
Moderators were seen as valuable participants because they draw on diverse experiences and offer a dual perspective. Recruiting men for health research is challenging, 48 whereas moderators, through their continuous interaction with members, gain insight into a wide range of support experiences among men with infertility. Both moderators also have lived experience with infertility, enabling them to combine personal experience with an understanding of group dynamics.
All interviews were conducted in April 2025 by the first author via Zoom (Zoom Video Communications, San Jose, California, USA), 49 a researcher trained in qualitative interviewing. A semi-structured interview guide was used to ensure consistency while allowing participants to elaborate freely. No major modifications were made to the interview guide during data collection, as the initial structure proved adequate. However, minor prompts were adapted iteratively based on emerging insights. Interviews lasted an average of 49 min (range: 31–61 min). With participants’ permission, all interviews were audio-recorded and transcribed verbatim. In addition, immediately after each interview, the researcher made a new audio recording to capture initial impressions, contextual observations, and early analytic thoughts that informed the early stages of coding. They were not treated as primary data.
The data was analyzed in Dutch in May 2025 using inductive thematic analysis of Braun and Clarke. 50 This approach was selected for its suitability to explorative research. Transcripts from online semi-structured interviews were coded for experiences with OISG and offline infertility support. Codes were organized into preliminary themes and sub-themes.
Triangulation was applied both during and after the analysis. First, researcher triangulation took place throughout the analytic process: the emerging thematic structure was iteratively reviewed, discussed, and refined in collaboration with the second and third author until consensus was reached. Coding continued until thematic saturation was achieved. Second, following thematic saturation, stakeholder checking was conducted. Representatives from the identified OISGs in stage one provided feedback on the preliminary findings and helped validate the themes for relevance and clarity.
Ethical approval and considerations
Approval for the study was granted by the Human Sciences Ethics Committee at the Free University of Brussels, Belgium, in September 2024 (code ECHW-549).
Results
Stage one – environmental scan
The environmental scan led to two identified OISGs who met the inclusion criteria: The Lost Stork in Flanders (in Dutch “De Verdwaalde Ooievaar” - www.deverdwaaldeooievaar.be) and Freya in the Netherlands (www.freya.nl). In what follows, these organizations, their purpose, and their offer of online support, including for men, are elaborated.
The Lost Stork (est. 2003) and Freya (est. 1985) support individuals and couples facing infertility and involuntary childlessness through accessible information, community activities, and advocacy. Both are run by steering committees of professionals and peer experts and funded by memberships, donations, and voluntary contributions, with Freya additionally receiving government grants.
Beyond physical support options, both organizations run public websites and social media channels that share information on infertility causes, treatment options, psychosocial care, and upcoming events. These platforms are open to everyone, regardless of membership status.
However, the two organizations differ in their approach to private online support, particularly in how they include support options for men. The Lost Stork runs three private Facebook groups tailored to themes such as “adoption” and “pregnancy after treatment”, but none specifically target men. It also hosts an active online forum with over 375,500 posts and nearly 9000 members (checked on 8/10/2025), yet usernames and discussion topics suggest that most participants are women or use pseudonyms, with minimal visible male involvement.
By contrast, Freya has created online spaces exclusively for men. During the COVID-19 pandemic, they launched a closed Facebook group called “FreyaMen” (211 members in 2024), followed by a WhatsApp group at participants’ request (44 members in 2024). In 2024, they also held seven online “Allies Evenings” via Zoom and one in-person meeting, giving men a dedicated space to share experiences and receive support. 51
Stage two – survey
In total, 34 men completed the survey, of whom 29 met the inclusion criteria. Table 1 summarizes participants’ sociodemographic and (in)fertility characteristics. The mean age was 40.28 years (SD = 9.16). All respondents were Caucasian of Dutch descent and lived with their partner. The majority had higher education (65.5%) and were employed (92.9%). Regarding their subjective perception of income, 79.3% reported living comfortably, while 17.2% stated they just met their income needs. More than half of the respondents identified as non-religious (51.7), followed by Protestants (24.1%) and Catholics (10.3%).
Sociodemographic characteristics of survey respondents

Regarding the (in)fertility characteristics, 72.4% of the respondents were childless, while 27.6% were already parents, either with their current partner or from a previous relationship. At the time of the survey, 65.5% were actively trying to conceive. The duration of fertility problems varied, with 47.4% having been trying to conceive for more than five years. The most common diagnosis was male infertility (44.8%), followed by unexplained infertility (27.6%). Just over half (55.2%) were undergoing treatment at the time.
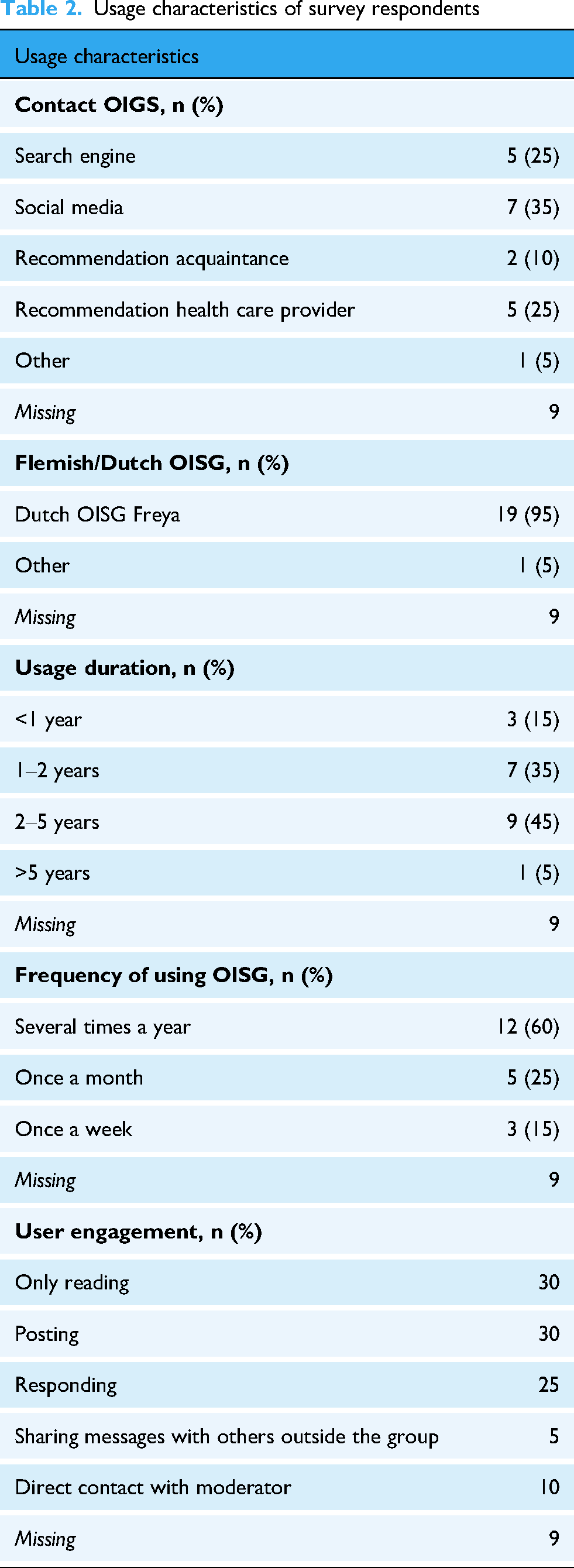
As shown in Table 2, usage characteristics indicate that respondents who were using OISGs at the time of the survey or had recently done so (68.97%) primarily discovered online support groups through social media (35%), a search engine (25%), or a health care provider (25%). The majority (95%) used the Dutch OISG Freya. Regarding duration of use, 45% reported being active for two to five years, and 60% visited the group several times a year. In terms of engagement, 30% of participants reported only reading messages, another 30% actively posted or asked questions, and 25% engaged by responding to others. Only 10% reported having direct contact with the moderator or sharing messages outside the group (5%).
Usage characteristics of survey respondents
Stage three-semi-structured interviews
As shown in Table 3, all participants were Dutch, averaging 40.3 years old (±6.57). Most were subfertile (impaired ability to reproduce); three were infertile, and one participant reported that both he and his partner faced fertility challenges. Parental status ranged from childless to expecting or already having children. All participants accessed both online support (e.g., Freya via Facebook, WhatsApp, Zoom) and offline support (e.g., family, friends), with one also using a U.S.-based WhatsApp group for men with infertility. The results first outline the factors influencing engagement in online and offline infertility support, followed by participants’ experiences with both types of support.
Sociodemographic characteristics of online interview participants.

Factors shaping support engagement
Participants’ use of online and offline infertility support was influenced by various facilitators and barriers. Key online facilitators included perceived anonymity, the availability of peer support, platform accessibility, and willingness to support, while navigating others’ reactions posed challenges. Offline, concerns about disclosure encouraged engagement, whereas concerns of non-disclosure discouraged it.
Online infertility support: facilitators
Perceived anonymity facilitated engagement with OISGs for most participants. Not knowing each other personally and not interacting face-to-face created a sense of anonymity that made it easier to share fertility challenges. Paradoxically, all participants reported using their full names when posting or responding, suggesting they did not feel the need to hide their identities. One even did so intentionally to promote openness. Thus, despite using identifiable information, participants still felt anonymous, which enabled disclosure. Ean (37, one child via intrauterine insemination [IUI]) described this as follows: “It felt freer to share there, because those people don’t know you, your partner, or your home situation. It's especially those relational tensions that you don’t talk about with family or friends, because they often know your partner well too. That makes it easier that they’re strangers.”
Availability of peer support was another facilitator for online engagement. Participants reported turning to OISG because they lacked peer support offline. Many linked this absence to societal taboos around infertility, which made them feel unable to speak openly about their situation. Consequently, they were drawn to OISG for its broader reach and larger community. As Peter (35, one child via donor conception) explained: “I didn’t know anyone close to me dealing with infertility or an unfulfilled desire for children. That made me seek out others who were. It was important to talk to people who truly understood who was going through the same thing. Online, you have a group around you that feels very far away, and that you wouldn’t otherwise have.” “WhatsApp works best for me because it can be used ad hoc. (…) If I feel the need to get something off my chest tonight, I just drop it in the WhatsApp group, and maybe three, four, or even ten men will respond with, ‘Oh, I recognize that.’ And that's really an advantage of online support, that's really the beauty of WhatsApp.”
Facebook was viewed as a less favorable platform. Some participants were not active on Facebook, and those who were noted minimal interaction, which reduced their motivation to participate. Unlike WhatsApp or Zoom, Facebook felt less accessible. For example, the threshold to make a “post” was perceived as higher than the ease of sending a WhatsApp message.
Lastly, many participants actively responded to others in OISG, with “willingness to support” emerging as a key engagement theme. This was true even for those who had conceived and no longer needed support themselves. Their engagement stemmed from three reasons: compensating for the lack of support in their own fertility journey, wanting to share experiential knowledge to give meaning to their experiences, and a desire to give back after receiving similar support earlier, as Peter (35, one child via donor conception) explained: “(…) because I personally received a lot of support, and I hope that I can offer the same to others who are just starting this journey or have just received the difficult news. I want to give something back, because I’m still grateful to the people who helped me.”
Online infertility support: barriers
Navigating online responses was experienced as a barrier to engage in OISGs by some participants. This was not only about responding itself but was linked to hesitation to disagree, reluctance to dampen the optimism of those early in their fertility journey, discomfort after critical comments, uncertainty about what to say, and concern about how messages might be interpreted without non-verbal cues. Harold (40, trying to conceive) elaborated on this latter point: “I do experience some hesitation when it comes to responding, afraid my words might be misinterpreted. Sometimes I start typing and then decide not to send it. Without eye contact or body language, it's hard to express nuance. In person, I could explain myself better, but since I don’t have the space to do that fully online, I just leave it.”
Offline infertility support: facilitators
Disclosure was a common facilitator for engaging in offline infertility support, enabled by the intentions behind it. By sharing their fertility challenges, participants hoped to reach other men facing similar issues, including those who had not yet spoken about it, and to make the topic more open and less taboo. In addition, some participants disclosed simply because they felt it was important to share such a crucial part of their lives with their social network. They did not want to hide their experiences or pretend everything was fine. Moreover, most participants disclosed their challenges to gain understanding for the difficult times they were experiencing. They hoped that being open would help their network be more considerate of their situation. Marijn (41, trying to conceive), for example, disclosed his situation so others would understand why he and his partner would not attend certain occasions: “When I open up offline, it's because I want others to understand why we act the way we do, why we don’t visit newborns or respond to that kind of news. As happy as we are for them, for us it's hell, every single time. You hope that by explaining, they’ll understand what it does to you.”
Offline infertility support: barriers
Non-disclosure was a key barrier to engaging in offline infertility support, and, as with disclosure, the reasons behind it strongly shaped participants’ level of engagement.
The intensity of the fertility trajectory was one reason for withholding disclosure. The emotional rollercoaster and fast pace of the process required time to be processed individually before participants felt ready to share. Daily interactions, for example with colleagues, also posed a barrier. Participants feared that disclosing their situation would trigger unwanted frequent conversations or change how others perceived them. Further, some participants felt their offline social network would not understand what they were going through, leading them to question why they should share something so personal if it would not be truly understood. Finally, the main barrier was the emotional toll of disclosure. Some initially planned to share their struggles but found it too distressing when others had children or were expecting. For others, disclosing meant reliving painful experiences, which felt too overwhelming, as Marijn (41, trying to conceive) experienced: “Maybe it's selfish not to share, but it's self-protection. You’re already feeling completely down yourself, and repeating bad news only adds to the burden. Sure, people might offer support, but in my experience, that support doesn’t outweigh the burden of having to share it again. After many attempts, we stopped telling anyone.”
Comparing online and offline infertility support experiences
The following sections compare participants’ experiences with online and offline infertility support, first outlining key differences in experiential expertise and personal contact, and then addressing shared themes such as the dynamic need for support.
Differences
A central theme across participants’ experiences was the value of practical and emotional experiential expertise in online versus offline infertility support. Practically, participants often turned to online groups for tailored tips and advice. As Jeroom (40, involuntary childless) explained: “After finding out I was infertile, I really searched for answers, like whether children from donor sperm would see me as their father. Advice from outsiders felt empty, but hearing from someone with shared experience gave me real confidence and helped me make the decision.” “You find a sense of recognition there, which reassurances, like, I'm not overreacting for finding this upsetting. But also, just that feeling of not belonging among my friends, because we’re the ones without children. Here (in OISG), you do feel like there are people who understand you, like you do belong there.”
This disconnect was evident in the reactions they received. Although often well-intentioned, these responses were difficult to hear. In some cases, people did not respond at all, changing the subject or avoiding the topic, which participants also experienced as hurtful. As Ean (37, 1 child via IUI) puts it together: “People close to you mean well, but comments like ‘it’ll be fine’ or ‘take a vacation’ hurt. All well-intentioned, but they cut deep. Those who’ve lived it know better, they say, ‘that's tough’ or ‘stay strong.’ Both come from good intentions, but it's different when someone hasn’t truly experienced it themselves.” “What I did find unfortunate is that sometimes the dominant theme is about how infertility affects your sense of masculinity. I personally don’t struggle with that, so it's hard to relate. The topics I care about were rarely addressed. That's why I didn’t use them much. (…) If certain people dominate the conversation, I think others start to disengage. That was the case for me at least.” Interviewer: “Can you give examples of times when you turned to your close ones for support?” Jaron: “I think it's in those moments when you wonder whether things still fit into your daily and private life. Your close ones see the full picture and help you reflect on what you have space for, not just the hospital visits, but also the emotionally heavy weeks that follow. They understand that and help ease the burden. They’re the ones who truly know what's going on.” “It's so complementary, so different. If you need support in the broader context of daily life, that's more likely to come from friends and family offline. But for specific experiences related to the fertility journey, support is more often found from peers online. It really depends on the kind of need you have.”
Similarities
A key theme across both online and offline settings was the dynamic need for infertility support. This shift occurred in two ways: changes in participants’ own need for support and changes in the support needs of their offline social networks. Thus, as the fertility journeys of both participants and their social network progressed, their infertility support needs shifted accordingly, shaping how participants perceived the support they received and influencing their relationships.
In offline social networks, some participants noticed that when other couples with fertility challenges conceived their willingness to talk about it with them decreased or disappeared. Conversely, when a participant conceived, a peer who was still struggling broke off contact.
Similar patterns were observed within the OISG. Participants reported that their sense of connection and need to engage in the group changed after their trajectory, particularly among those who had conceived a child or who were involuntarily childless and further along in their coping process. Richard (36, trying to conceive), also described this dynamic need for support throughout his fertility trajectory: “For many people, it's all new, and that's when they become active in a group like this. But after years of treatment, it becomes harder to connect. Someone might be devastated after their first failed IUI, while we’ve had five attempts, eight embryo transfers, and two IVF rounds. Then it feels a bit oversensitive. When I think of successful peer contact, it's when it's aligned with the phase you’re in yourself.”
Discussion
This is the first study to examine the availability of Dutch-speaking OISGs, their inclusion of male-specific support, the characteristics of male users in both regions, how they experience online versus offline infertility support, and the factors that influence their use of these support forms. Based on the results of a multistage mixed-methods design, four major findings emerge: (1) scarcity of Dutch-speaking OISGs and limited male support inclusion; (2) predominance of higher-SES users; (3) influence of perceived anonymity on engagement; and (4) complementary nature of online and offline infertility support, with a dynamic need for infertility support emerging across both forms.
Scarcity of Dutch-speaking OISGs and limited male support inclusion
The environmental scan first reveals that Dutch-speaking OISGs are scarce, and the inclusion of male-specific support in these groups is not evident. This contrast is illustrated by Freya's targeted initiatives for men, compared to The Lost Stork's more general support approach for people with infertility.
On one hand, the limited availability of psychosocial support for men with infertility is not unique to these regions. Many health systems worldwide, even in high-income countries, lack dedicated services for men, 52 reflecting a broader pattern of structural neglect of infertility as a health priority, a traditional focus on women, and persistent stigma and masculinity norms.53,54 Even in progressive settings such as Belgium and the Netherlands, countries that rank among the highest in Europe in terms of gender equality, traditional gender norms and stereotypical health attitudes continue to persist, shaping health-seeking behavior and social expectations. 55 As a result, psychosocial care for men often remains secondary to clinical treatment, leaving their support needs unmet and limiting the development of male-specific support options. 52
On the other hand, the availability of OISGs and the inclusion of men-specific support services differ across countries; shaped by specific socioeconomic conditions, national healthcare policies, and the organization of psychosocial care. 52 These structural factors, therefore, limit the extent to which the findings can be applied to other health system contexts.
Compared with English-speaking countries in the Global North, the scarce availability of Dutch-speaking OISGs becomes even more apparent. For example, RESOLVE (https://resolve.org/) (USA) and Fertility Network UK (https://fertilitynetworkuk.org/) have become professionalized institutions, and newer USA groups like “The Broken Brown Eggs (https://thebrokenbrownegg.org/)” support specific communities such as women of color. Although Freya is recognized as an established institution, 53 the fact that only two Dutch-speaking OISGs met the inclusion criteria, of which just one offers specific online support for men, highlights a clear gap in diversity and availability.
This underrepresentation can further be linked to low awareness among men about infertility support groups. In a global survey of De Jonge, Gellatly, 56 fewer than 25% of respondents knew of male-specific groups in their country, with awareness in Europe below 15%. Even when support is available, it may remain inaccessible due to visibility and outreach challenges.
Overall, this finding reveals a disconnect between the advanced clinical infertility services offered in Belgium and the Netherlands and the underdeveloped psychosocial care available to men through Dutch-speaking OISGs. This gap suggest that structural neglect and persistent gendered assumptions continue to shape the availability of online infertility support and the inclusion of men in it, potentially leaving men underserved in an otherwise progressive healthcare landscape.
Predominance of higher-SES users
Building on the survey results, the second finding reveals that men engaging with OISGs form a relatively homogeneous group: Dutch, highly educated, employed, comfortable financial situation, in stable relationships, and often childless while actively trying to conceive. Most had been dealing with fertility challenges for several years, with male-factor infertility being the most common diagnosis. Their usage, primarily through Freya, was relatively sustained over time, with varying levels of interaction.
This profile indicates limited ethnic and socioeconomic diversity, suggesting a selective access of OISGs among men with higher socioeconomic status (SES). SES is a well-established predictor of online help-seeking.28,36 Individuals with higher SES engage more effectively with digital health resources, while those with lower SES face barriers such as limited digital skills and health literacy, 57 reflecting the broader digital divide. 58 Migration background also influences online help-seeking, though findings are mixed. Research shows that minority group members actively engage in various online social support activities and may benefit from targeted online communities. 59 In contrast, a study found that migrants were 44% less likely to seek health information online, even when SES was comparable. 60 This disparity may be further explained by reduced access to social and informational support, language barriers, 36 and cultural beliefs such as traditional health views.61,62
This finding highlights a limitation in the reach of current OISGs. While the internet is often seen as a tool to overcome geographical, socioeconomic, 36 and stigma-related barriers, 63 persistent access challenges remain. The homogeneity of the sample underscores that men with lower SES and/or migration backgrounds are likely underrepresented or underserved.
Influence of perceived anonymity on engagement
Regarding the third finding, the qualitative results show that engagement in OISGs and offline infertility support is determined by an interplay of digital platform features and psychosocial factors. Anonymity played an important role in engaging with OISGs. However, a paradox emerged: although participants shared identifiable information, such as their name, they perceived the OISG as anonymous, which encouraged the disclosure of their fertility challenges.
This finding reinforces prior research showing that online platforms offer emotional safety through anonymity and distance, helping men navigate stigma and dominant masculine norms.23,27,28 Importantly, this study highlights that it is the perception of anonymity, rather than technical anonymity, that facilitates disclosure. 64 Technical anonymity exists when any information that could reliably identify you or others is removed from the exchanged content, 65 whereas perceived (or social) anonymity refers to the extent to which individuals perceive that their personal identity is unknown to others or that they are unidentifiable as an individual. 66
In the current digital landscape, technical anonymity is rare, yet perceived anonymity shapes willingness to engage, highlighting a distinction from prior research that treats anonymity as a binary condition. 66 Moreover, the study nuances the assumption that anonymity always facilitates disclosure. In one case, perceived anonymity led to distrust, illustrating the “trust paradox”: while anonymity can feel protective, excessive anonymity may undermine trust, especially in spaces where mutual vulnerability is essential. 67
Thus, this study challenges the common assumption that anonymity in online settings is universally beneficial for disclosure. 28 It shows that anonymity can both support and hinder openness, not due to anonymity itself, but depending on how it is perceived by users.
Dynamic need for infertility support
Men with infertility viewed online and offline support as complementary, each meeting different needs. OISGs provided experiential expertise tailored to the fertility trajectory, while offline relationships offered personal contact shaped by one's history and life context. The key difference lies in the relational nature of support, between peers and intimates, rather than simply between online and offline settings. In both contexts, support needs were dynamic, shifting as men and their social networks moved through their fertility journeys, which influenced how they perceived support, its usefulness, and its impact on their relationships.
This finding aligns with broader research on chronic illness and caregiving research, where support needs change over time.68,69 This can be understood through the optimal matching model, 70 which posits that support is most beneficial when it fits the seeker's goals and stressors, reducing distress when expectations are met. 71 Recent research further emphasizes the importance of timing, personal context, and evolving needs in shaping support effectiveness, with mismatches potentially reducing its impact.72,73
In male infertility, hegemonic masculine norms shape how men navigate infertility and how their support needs unfold over time.74,75 These norms, emphasizing stoicism, emotional control, rationality, and self-reliance, can constrain men's willingness to disclose distress or seek help.74,75 Over time, as men adapt and integrate infertility into their identities, some adopt forms of “emergent masculinity,” balancing sensitivity, partner-focused behaviors, and selective help-seeking. 74 However, even with these shifts, hegemonic expectations continue to shape which concerns men disclose, the timing of seeking support, and the contexts in which they feel safe to express vulnerability.74,75
Vickery 76 argues that men's peer support spaces operate as communities of practice, 77 which provides an additional lens for interpreting these findings. Such communities share norms, identities, and social practices, 78 and these norms can create space for emotional expression that might otherwise threaten masculine status in other settings. 79 In this way, communities of practice can support the reshaping of masculinity in more health promoting directions. The complementarity between online and offline infertility support similarly reflects how men move between contexts that enable different forms of identity and vulnerability. This underscores that OISGs function not only as sources of experiential expertise, but as relational spaces where masculine identities are negotiated and supported.
Thus, while social support reduces psychosocial distress among people with infertility,31,32 this finding highlights that its effectiveness depends on alignment with the fertility journey phase. Masculinity norms and communities of practice offer useful interpretive frameworks for understanding why men's support-seeking is dynamic. Moreover, it expands the understanding of support needs among people with infertility, mainly examined in clinical settings (e.g.,80–82), by applying it to informal online communication environments used by men.
Limitations
While this study offers valuable insights into men's help-seeking behavior, several limitations must be acknowledged. First, using Google and specific search terms may have favored certain support groups due to search engine optimization, potentially overlooking less organized/informal ones. However, stakeholder consultations confirmed that the selected groups reflect the current OISG landscape in Flanders and the Netherlands.
The sample size was small, limiting statistical power and allowing only descriptive insights. This highlights the broader challenge of including men in research on sensitive issues, particularly those involving intimacy and sexuality. 48 It is also reflected in findings of De Jonge, Gellatly, 56 where only four Belgian and 77 Dutch men participated, and awareness of support groups was low (25% of Belgium and 44% in the Netherlands, own calculation). The actual response rate remains unclear, as it is unknown how many forum members saw the survey but chose not to participate. As such, the sample represents self-selected OISG users.
The convenience sample may have limited diversity and representativeness, excluding men who use other forms of online support. Yet, it mirrors typical demographic and socioeconomic profiles in online surveys for academic research.83,84 The sample also mainly includes men who felt comfortable disclosing their experiences. As a result, it is difficult to determine whether certain groups are underrepresented because they struggle with disclosure, participate less in research surveys, have less need for online support, or face access barriers. Likely, a combination of these factors is at play.
In addition, inclusion criteria further restricted diversity and representativeness by excluding non-Dutch speakers, LGBTQIA + individuals, and men who had not used ART but still experienced infertility-related stress. As a result, the sample shows limited variation in ethnicity, sexuality, and infertility experiences outside clinical pathways, limiting the ability to examine how social background may shape patterns of online support use.
While online interviews may helped overcome stigma and geographical barriers, 47 they limited personal connection and access to non-verbal cues, which are important for discussing sensitive topics. Moreover, the study reflects experiences from Freya in a Dutch context, limiting transferability to other OISGs or cultural settings. This limitation is compounded by the absence of analyses based on infertility diagnosis, which may shape experiences differently.
Future directions
Given that Dutch OISGs are scarce, male-specific support is not self-evident, and research suggests that this can be linked to low awareness among men about infertility support groups. 56 General practitioners, nurses, and other primary care professionals need to be aware of the local online support groups available and use them as a low-threshold and non-clinical referral option. 76 Future research should examine how established platforms, such as those in the Global North, became institutionalized and how their models can be adapted to the Flemish and Dutch contexts.
As current user insights reflect limited socioeconomic and ethnic diversity, support organizations and platform developers could employ co-design approaches with men from varied backgrounds to enhance effectiveness and accessibility for a broader range of users. 4 Future research should purposively include diverse groups to build a more inclusive understanding of men's online support-seeking experiences.
Considering that perceived anonymity plays a crucial role in enabling men to disclose infertility-related concerns in OISG, future research should explore how perceived, rather than technical anonymity encourages disclosure in online spaces. This is important, as perceptions of anonymity vary among men and shape their engagement, affecting the impact of peer support. Further, platform features beyond anonymity and accessibility, such as privacy, immediacy, and informality, may shape support dynamics and therefore deserve closer attention when designing online support initiatives.
As this study shows that the support needs of men with infertility are dynamic, and this can be understood by hegemonic masculine norms,74,75,85 tailored interventions that give explicit attention to masculinity are required to meet these evolving needs. 86 Moreover, while research has begun to explore men's support needs in online support groups (e.g.,27,28), more is needed to understand how these needs shift across different stages and diagnoses. Different phases may require tailored moderation or communication strategies. In addition, given WhatsApp's high engagement in this study, subgroups within the app could offer phase-specific peer support.
Lastly, because men described online and offline infertility support as complementary but meeting different needs, integrating these pathways may enhance their overall support experiences. Rather than assuming uniform benefit, interventions should treat OISGs as one component within a broader support landscape. 76
Conclusion
Using a multistage mixed-methods design, this study highlights the scarce availability of Dutch-speaking OISGs for men, with limited inclusivity of male-specific support. Men who engage with these platforms largely belong to higher-SES groups, indicating selective access. Usage is mainly via Freya, sustained over time, with varying levels of interaction. Engagement is shaped by a complex interplay of digital features and psychosocial factors, with perceived anonymity emerging as a paradox. Men experience online and offline infertility support as complementary resources, each fulfilling distinct needs. The core distinction lies in the type of relationship, peer versus intimate, rather than the medium. A dynamic need for infertility support occurs in both settings. These insights underscore the need for more, inclusive, and tailored support strategies that address the dynamic needs of men navigating infertility, both in online and offline settings.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076261430610 - Supplemental material for Fertile ground for social support? Understanding men's use of online infertility support groups
Supplemental material, sj-pdf-1-dhj-10.1177_20552076261430610 for Fertile ground for social support? Understanding men's use of online infertility support groups by Lobke Van Ryckeghem, Anna Wallays, Ella Oelbrandt and Veerle Buffel in DIGITAL HEALTH
Footnotes
Acknowledgements
We are grateful to The Lost Stork, Freya, and all respondents for participating in this research project.
Ethical considerations
Approval for the study was granted by the Human Sciences Ethics Committee at the Free University of Brussels, Belgium, in September 2024 (code ECHW-549).
Consent to participate
Respondents gave written consent for review and signature before starting interviews.
Author contributions
Lobke Van Ryckeghem: review & editing, writing original draft, visualization, validation, resources, project administration, methodology, investigation, formal analysis, data curation, conceptualization.
Anna Wallays: review & editing, formal analysis.
Ella Oelbrandt: review & editing, formal analysis.
Veerle Buffel: review & editing, validation, supervision, project administration, methodology, data curation, conceptualization.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.