
Abstract
Objective
To conduct a comprehensive health systems policy analysis of the Sindh Telemedicine and Telehealth Act 2021 by examining its contextual drivers, governance and stakeholder dynamics, implementation barriers and facilitators, and policy content, and by comparing it with telemedicine policies in neighboring low- and middle-income countries (LMICs).
Methods
Our study applied Walt and Gilson's policy triangle to examine context, content, process, and actors. A desk review of relevant policy documents from Sindh and other LMICs (India, Bangladesh, and Nepal) was conducted, followed by in-depth interviews with 28 stakeholders (July–October 2023) until data saturation was reached. Participants were recruited using purposive and snowball sampling strategies. Thematic analysis was done using Qualitative Data Analysis Software (QSR NVivo v12) to identify barriers and facilitators to policy implementation.
Result
The contextual drivers behind the formulation of the Act included the coronavirus disease 2019 pandemic, limited healthcare access, and the growth of telehealth providers in private sector. The Act provides a regulatory framework for healthcare providers registration and training requirements, guidelines for patient consent, emergency care, and data privacy. However, it lacks clarity on the cost of telemedicine services and measures for cross-border telemedicine. Stakeholder analysis showed government bodies hold the highest power in telemedicine policymaking. Telemedicine service providers and healthcare providers expressed support for the Act but were excluded from policymaking process. Service users also had minimal involvement in the policymaking process. Policy implementation varies, facing financial and technological barriers, while strategic financial planning and public–private partnerships, identified as facilitators in overcoming these challenges.
Limitations
The study may be subject to limitations, including potential selection bias while identifying stakeholders and the constraints of desk review in capturing details.
Conclusion
The Act is an important step towards addressing healthcare disparities, with its success contingent on overcoming implementation barriers through inclusive and strategic policymaking and investment in digital infrastructure.
Introduction
Telemedicine has the potential to completely transform the way healthcare is delivered, 1 especially in low- and middle-income countries (LMICs), where access to healthcare services is often constrained by geographical and health system barriers. The coronavirus disease 2019 (COVID-19) pandemic triggered a boom in the digital health landscape, increasing the adoption of digital technologies within health services, particularly in telemedicine, bringing about innovations in healthcare delivery models in both high-income countries and LMICs. 2 In 2024, there were over 116 million users of online doctor consultations worldwide, up from around 57 million in 2019. 3 While telemedicine promises to provide more convenient and cost-effective access to physicians compared to traditional approaches, 3 the adoption of this technological change in LMICs may be constrained by a less favorable policy and regulatory environment. 2
In Pakistan, where 61.2% of the population resides in rural areas, 4 health systems face constraints due to inadequate healthcare infrastructure, a dual burden of communicable and non-communicable diseases, and a shortage of healthcare workforce relative to globally recommended standards, with only 1.1 medical doctors per 1000 population 5 and 0.5 nurses per 1000 population as of 2019. 6 Numerous tele-health initiatives have been introduced to address these health system gaps. The Aga Khan Development Network Digital Health Program leverages information and communication technologies to connect health care institutions and health care providers within and across Afghanistan, Kyrgyz Republic, Pakistan, and Tajikistan. 7 Telehealth clinics, such as those established by Commission on Science and Technology for Sustainable Development in the South (COMSATS) and Sehat Kahani, offer access to quality healthcare for underserved populations. Additionally, platforms like doctHERs and Oladoc enable patients to book appointments and connect with doctors online. These initiatives are primarily led by the private sector but often operate in silos due to a lack of governance, which allows their implementation without following recommended standards or ensuring these are interoperable with other systems. 8 In addition, research had highlighted the urgent need for a telemedicine policy to encourage acceptance and effective utilization across the country. 9
In 2019, a draft for the National Telemedicine Policy was formulated in the wake of the COVID-19 pandemic, without it being finalized. 10 In 2022, the National Digital Health Framework for Pakistan 2022–2030 was established, marking a crucial step towards the digitization of the country's healthcare infrastructure. 11 Leveraging the health programing, policymaking and legislative autonomy granted to the provinces by the 18th constitutional amendment, Sindh became the first among Pakistani provinces to formulate a legislation for telemedicine, enacting the Sindh Telemedicine and Telehealth Act 2021. 12 From here on, we use the term “Act” to refer to the Sindh Telemedicine and Telehealth Act 2021. This Act was a significant step in formally recognizing telemedicine within the province.
A conducive policy environment supporting integration of telemedicine into the health systems promises to address major health system challenges of access and quality of service delivery in Pakistan and other LMICs. The aim of this study was to conduct a comprehensive policy analysis of the Sindh Telemedicine and Telehealth Act 2021. Specifically, the study examined the contextual factors influencing telemedicine in Sindh, conducted a stakeholder analysis, identified key barriers and facilitators to implementation and conducted a content analysis of the Act alongside a comparative review of telemedicine policies in neighboring LMICs including India, Bangladesh, and Nepal to identify gaps and similarities to Act.
Methodology
Study design
The study employed a qualitative case study design to conduct policy analysis of the Sindh Telemedicine and Telehealth Act 2021.
Conceptual framework
For this study, we used the Walt and Gilson policy triangle framework for policy analysis, 13 providing a structured approach to analyzing telemedicine law in Sindh. This framework is renowned for its comprehensive perspective on policy analysis and is particularly pertinent for examining the complex nature of telemedicine policy. It presents a simplified approach to a complex set of interrelationships among contextual factors, policy content, policy processes, and the roles of various actors. Figure 1 illustrates the adaptation of this framework in accordance with telemedicine policy analysis, also highlighting key research questions framed according to the various elements in the framework.

Model for health policy analysis for telemedicine.
In addition, a Political, Economic, Social, Technological, Legal, and Environmental (PESTLE) analysis was conducted to understand the multifaceted contextual factors that shaped the landscape of telemedicine in Sindh.
Study setting
Sindh is the second-largest province in Pakistan, with a population of 55.7 million, approximately 46.03% of which resides in rural areas. 14 A 38% of the population lives below the poverty line of $3.65. 15 Sindh's public sector health infrastructure comprises 8 teaching hospitals, 16 district headquarters hospitals, 18 major hospitals, 50 Taluka hospitals, 128 Rural Health Centers, 793 basic health units, and 1378 dispensaries. 16 Despite having over 14,000 doctors, 2000 nurses, and 12,000 paramedics, the province faces significant challenges in healthcare access. Many rural health facilities are ill-equipped, understaffed, and underutilized, leading to disparities in healthcare access and quality. 17 This study was conducted from July to October 2023.
Sampling strategy and study participants
The study utilized purposive and snowball sampling methods to carefully select participants with direct or indirect involvement and experience in telemedicine services. Purposive sampling was used to ensure representation across key stakeholder groups involved in telemedicine policy and implementation, while snowball sampling supported identification of additional relevant informants. We acknowledge that snowball sampling may introduce network bias and limit diversity of perspectives; however, this risk was mitigated by initiating recruitment across diverse institutions and sectors like policymakers, telemedicine service providers, healthcare providers and service users. Similar mixed sampling approaches have been commonly used in qualitative digital health research in LMIC settings to access diverse stakeholder perspectives. 18
A total of 28 participants were selected to provide a comprehensive understanding of the policy. The sample size was determined by the point of data saturation, meaning the interviews continued until additional conversations no longer provided new or relevant information. No participants who were approached declined participation or withdrew from the study. The respondent groups included 9 provincial government officials from the Health Department, Sindh Healthcare Commission (SHCC), Planning and Development Department, and Population Welfare Department. Additionally, the study engaged 7 patients, 8 healthcare providers, and 4 telemedicine service providers, see Table 1.
Study Participants and Inclusion Criteria.

Data collection and analysis
In-depth interviews were conducted in either Urdu or English using an interview guide (see Supplemental file 1) developed on the basis of the conceptual framework, which was piloted and refined prior to data collection. The interviews were conducted by a female member of the research team, who held postgraduate qualification in public health and health systems research and was working as a health systems researcher at the time of the study. Participants were approached via telephone and were informed about the purpose of the study and the researcher's role prior to providing consent. The interviews ranged from 30 to 45 min and were carried out either face-to-face or virtually. Repeat interviews were not conducted, and no non-participants were present during the interviews. Audio recordings of the interviews were made with the verbal consent of the participants and field notes were taken during the interviews to capture non-verbal cues. Literature search and desk review of policy documents of the Act and neighboring LMICs (India, Bangladesh, and Nepal) were conducted. Additionally, any publicly available information on the Act from provincial health department and annual reports from telemedicine providers like Sehat Kahani were also reviewed. Data was analyzed using thematic analysis to extract insights on the barriers, facilitators, and prospects of telemedicine with the help of NVivo software version 12. Initial coding was conducted by the lead author, with regular discussions among the research team to refine and validate themes. To minimize potential interviewer bias, the interview guide was applied consistently across participants, and probing was guided by the conceptual framework rather than individual assumptions. Interview transcripts were not returned to participants for comment or correction. This qualitative study is reported in accordance with the Consolidated Criteria for Reporting Qualitative Research checklist (see Supplemental file 2)
Results
Themes were derived inductively from the data and organized deductively using the Walt and Gilson policy triangle framework. Using this framework, thematic analysis identified four overarching themes that structure the results presented in this section. These included: (1) Contextual factors influencing the development and implementation of telemedicine policy in Sindh; (2) stakeholder roles, power dynamics, and positioning within telemedicine policymaking; (3) implementation barriers and facilitators affecting the operationalization of the Sindh Telemedicine and Telehealth Act 2021; and (4) strengths and gaps within the policy content, informed by analysis of the Act and comparative review of telemedicine policies in neighboring LMICs. These themes are presented sequentially in Sections “Contextual factors” to “Comparative analysis of Sindh Telemedicine and Telehealth Act 2021 with implemented telemedicine policies of India, Bangladesh, and Nepal.”
Contextual factors
The Act was developed to standardize the use of digital technologies to make healthcare more accessible, particularly in remote and underserved areas. Its implementation is shaped by various factors, including political priorities, economic conditions, social acceptance, technological infrastructure, legal frameworks, and environmental considerations as shown in Table 2.
Political, Economic, Social, Technological, Legal, and Environmental (PESTLE) Analysis of the Contextual Factors for Sindh Telemedicine and Telehealth Act 2021.

The stakeholders analysis
The implementation of Act relies on the collaborative efforts of various stakeholders, each bringing unique strengths and influence. We presented stakeholders’ sources of power, power, and their positions in Table 3. Our analysis did not identify any opponent groups through document reviews or stakeholder interviews.
Stakeholder Analysis for Sindh Telehealth and Telemedicine Act 2021.

PTA: Pakistan Telecommunication Authority; MoNHSRC: Ministry of National Health Services, Regulations and Coordination; WHO: World Health Organization.
Stakeholder power was assessed based on perceived influence over policy formulation and implementation, decision-making authority, and control over regulatory or financial resources, drawing on interview data and document review.
The Ministry of National Health Services, Regulations and Coordination (MoNHSRC) and Sindh Health Department hold substantial power and authority in telemedicine policy. They are central to policy formulation and implementation but demonstrated only moderate support for the Act. The SHCC ensures compliance with health standards through its significant regulatory power and expertise, thereby influencing the quality and standards of telehealth services, thus being highly supportive of this Act.
The Planning and Development Department and the Population Welfare Department play supportive roles by integrating health policies with broader developmental goals and providing policy support for population health management. Both departments demonstrated moderate support and are pivotal in aligning telehealth policies with overall development strategies.
The Pakistan Telecommunication Authority (PTA) plays a crucial role in regulating telecommunication infrastructure, ensuring robust connectivity and data security with a moderate power level. Telemedicine Service Providers and Healthcare Providers are vital for operationalizing the Act, advocating for resources, and delivering healthcare services. Despite their slightly lower power their roles are essential and were found to be highly and moderately supportive, respectively.
Patients, as primary beneficiaries, provide valuable feedback essential for continuous service improvement, although their individual power is minimal and were moderately supportive. Academic and research institutions hold influence through evidence-based research, shaping policy with critical insights. The World Health Organization (WHO) Country Office and Global Health Agencies and donors offer essential funding and technical assistance for health projects, also reflecting high support.
Implementation barriers and facilitators of the Sindh telemedicine and telehealth act 2021
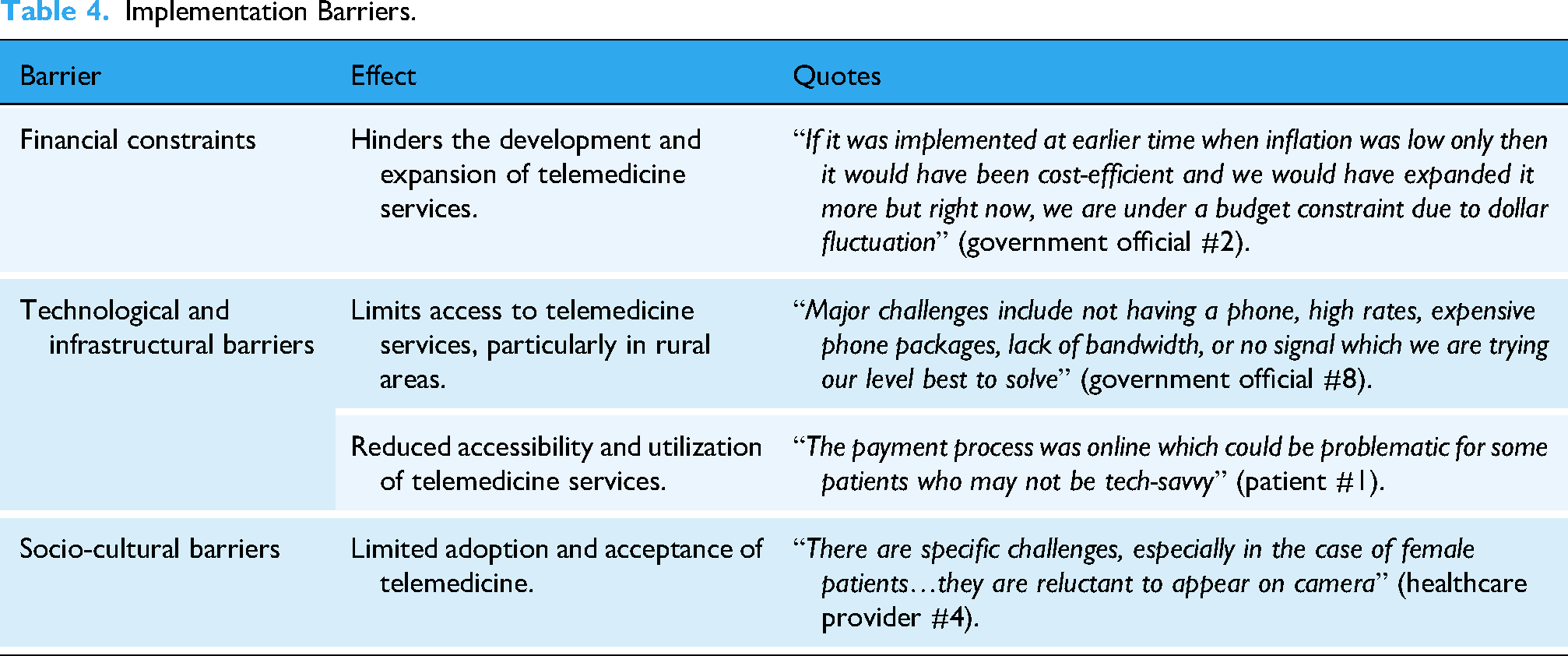
The implementation of Act encountered several challenges and opportunities on ground, particularly in rural areas. Tables 4 and 5 provide detailed overviews of the specific barriers and facilitators identified during the implementation process.
Implementation Barriers.
Implementation Facilitators.

KPI: key performance indicator; PPP: public-private partnership.
Content analysis of the Sindh telemedicine and telehealth act 2021
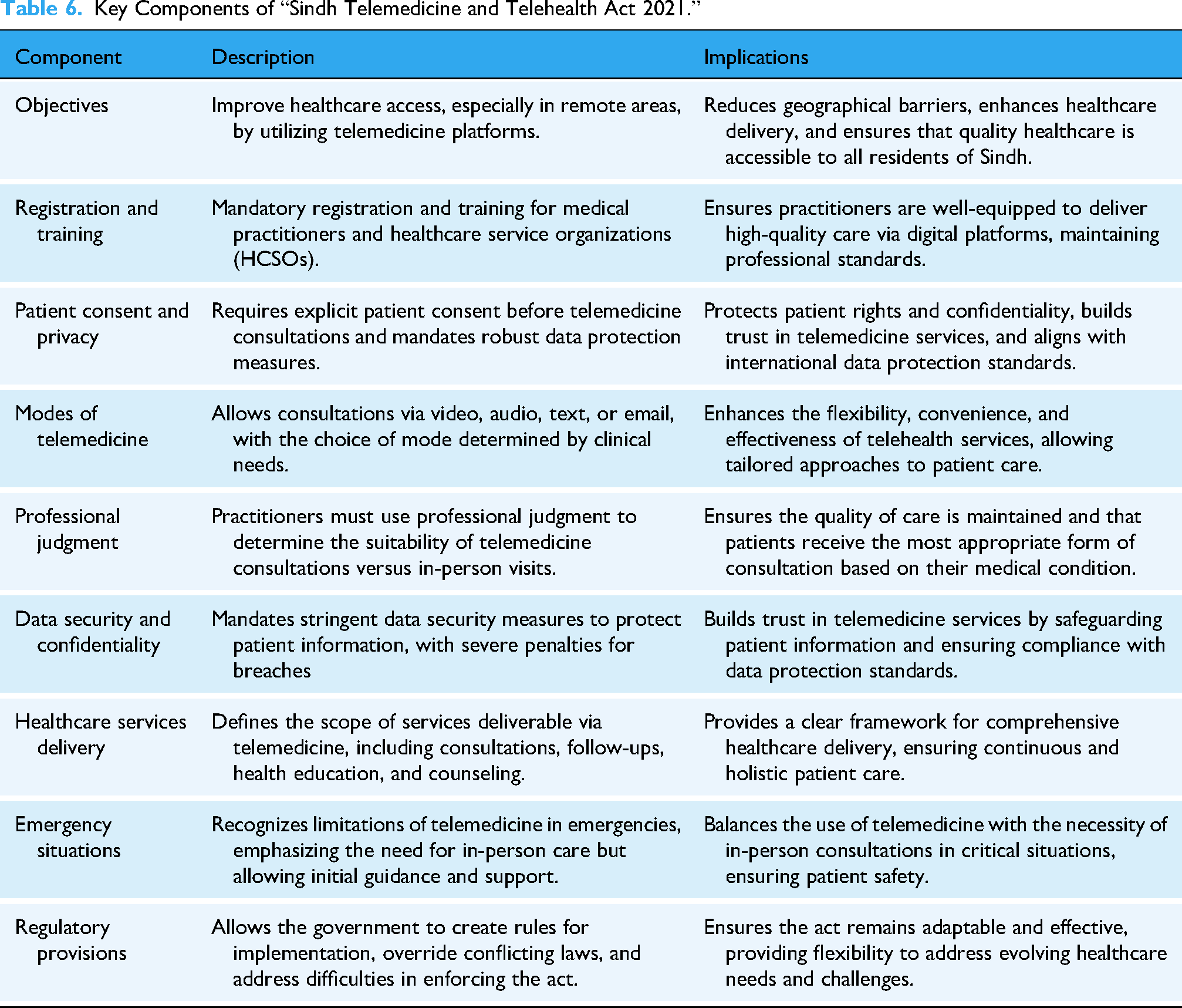
The Act aims to enhance healthcare delivery through telemedicine platforms, focusing on accessibility, quality, and security. The Act provides a comprehensive framework for remote healthcare services, addressing the shortage of healthcare professionals and promoting equitable healthcare access across Sindh. Table 6 summarizes the key components of the Act and its implications.
Key Components of “Sindh Telemedicine and Telehealth Act 2021.”
Comparative analysis of Sindh telemedicine and Telehealth Act 2021 with implemented telemedicine policies of India, Bangladesh, and Nepal
The Telehealth Act of Sindh is comprehensively designed; however, there are a few domains where the Act is lacking compared to those in India, 19 Bangladesh, 20 and Nepal. 21 For instance, the Sindh policy does not address the use or standardization of technology platforms for telemedicine, which is crucial for ensuring interoperability and consistency across different telemedicine services. In contrast, India, Bangladesh, and Nepal have established standards for technology platforms, facilitating a more integrated and efficient telehealth ecosystem.22–24 These interoperability frameworks enable secure data exchange, continuity of care, and integration with national health information systems.
Moreover, the Act does not cover regulations or guidelines for cross-border telemedicine, which could facilitate international consultations and collaborations. Nepal have incorporated guidelines for cross-border telemedicine, thus expanding the reach and scope of telehealth services beyond its national borders. Additionally, there is no provision or guideline regarding the cost of telemedicine services in the Sindh Act. Clear guidelines on the cost of services are important for ensuring affordability and transparency for patients. India, Bangladesh, and Nepal have recognized the need of preventing arbitrary pricing and ensuring affordability of telemedicine in making telemedicine accessible to a wider population. To address this need, they included cost-related provisions in their telemedicine policies. Table 7 provides a comparative analysis of the telemedicine policies implemented in India, Bangladesh, and Nepal with that of Sindh, highlighting these key gaps.
Comparative Analysis of Sindh Telemedicine and Telehealth Act 2021 with Implemented Telemedicine Policies of India, Bangladesh, and Nepal.

Discussion
Telemedicine is a transformative digital health intervention that offers flexible, patient-centric care delivery models. The COVID-19 pandemic accelerated its adoption globally, emphasizing the urgent need for effective telehealth policies in LMICs such as Pakistan. 25 The Sindh Telemedicine and Telehealth Act 2021 is a commendable step toward formalizing telehealth services, addressing key healthcare delivery challenges in Sindh's predominantly rural population. However, for its full potential to be realized, several enhancements to the policy and its implementation must be considered. The expansion of telemedicine initiatives hinges on overcoming barriers such as funding challenges, limited technological infrastructure in remote areas where such programs are most needed, and socio-cultural resistance as also reported in one of the studies. 26
The content and comparison analysis of the Act shows that Sindh Telemedicine and Telehealth Act 2021 covers important aspects for regulating telemedicine practice by addressing critical areas such as patient consent, data security, and professional judgment in remote consultations. However, significant gaps remain when compared to telehealth policies in neighboring countries like India, 19 Bangladesh, 20 and Nepal. 21 These gaps include the lack of standardized technology platforms to ensure interoperability, absence of clear cost regulations to ensure affordability and equitable pricing, and the omission of provisions for cross-border telemedicine consultations. In contrast, India has operationalized a national digital health architecture through the Ayushman Bharat Digital Mission to enable interoperability across health information systems, 22 Nepal has placed interoperability at the center of its digital health agenda by adopting OpenHIE as a reference framework for standardized health information exchange, 24 and Bangladesh has implemented interoperability mechanisms linking sector-specific information systems with the national DHIS2 platform to support integrated data sharing and health system decision-making. 23 Addressing these gaps by incorporating lessons from neighboring countries could enhance the policy's robustness and adaptability to evolving healthcare needs. For instance, India's telemedicine guidelines provide detailed guidelines on doctor-patient consultation in specific scenarios and for different medical conditions, that may ensure consistency in service delivery if followed. Similarly, Bangladesh has articulated clear categorization of medicines for different situations while Nepal specifically mentions cost for services and cross-border telemedicine. Careful consideration for these components would not only enhance the effectiveness of the Act but also ensure its successful implementation.
From stakeholder analysis we identified that effective implementation of the Act requires active engagement and commitment from various stakeholders. Provincial governments must lead implementation efforts by allocating resources strategically to ensure policy compliance. SHCC should be the lead regulator overseeing the policy implementation. SHCC should establish monitoring and evaluation mechanisms to track telehealth performance, assess compliance with standards, and identify areas for improvement. Through structured licensure processes, SHCC should ensure that only qualified and accredited healthcare providers are authorized to offer telemedicine services, maintaining professional integrity and patient safety. Quality of care monitoring should be implemented by setting benchmarks, conducting regular assessments, and ensuring that telehealth services align with established clinical and ethical standards. A feedback mechanism should be developed to allow patients and providers to report concerns, ensuring continuous service improvement and timely policy adjustments.
Similarly, the Pakistan Medical and Dental Council (PMDC) should be responsible for overseeing professional standards in telemedicine. PMDC should regulate medical practitioners engaged in telehealth by ensuring they adhere to ethical guidelines, maintain patient confidentiality, and uphold professional integrity in virtual consultations. PMDC should also provide continuous guidance on ethical considerations and ensure that healthcare professionals receive adequate training on telemedicine best practices.
If we see the barriers and facilitators for the implementation of Act, the role of the private sector cannot be overstated. This finding aligns with international experiences demonstrating the effectiveness of public–private collaboration in telehealth scale-up. 27 Public–private partnerships can play a pivotal role in expanding the use of telehealth in at least two distinct ways. Firstly, the government-operated facilities in remote and rural districts could be contracted out to private telemedicine suppliers. Secondly, broadband providers should work on expanding access and mobile connectivity in rural areas while also focusing on development of scalable telemedicine platforms. The private sector's role is indispensable in enhancing service delivery, and their participation can be incentivized through tax benefits and grants. Investments in reliable internet infrastructure, complemented by the establishment of telemedicine kiosks with power backups, are essential to mitigate infrastructural challenges. Culturally sensitive awareness campaigns, engaging local leaders and influencers, can help build trust and promote telemedicine adoption, especially among women who face privacy concerns. Comprehensive training programs for healthcare professionals and digital literacy initiatives for communities can further ensure effective utilization of telehealth services.
An additional socio-economic barrier affecting telemedicine adoption in Sindh relates to the prevalence of informal, cash-based financial practices. Telemedicine models that rely primarily on digital payments may inadvertently exclude unbanked and underbanked populations, particularly low-income households and rural users with limited access to formal banking systems, mobile wallets, or digital literacy. In the absence of explicit policy guidance on alternative or hybrid payment mechanisms such as cash-based options, telemedicine risks reinforcing existing inequities in healthcare access. Addressing financial inclusion within telemedicine policy design is therefore critical to ensuring equitable uptake and sustainable scale-up.
This mirrors the approach taken in other countries, where public-private partnerships have been key to successful telehealth implementation. For example, the successful implementation of Technology-enabled Remote Healthcare in India showed that e-health in a public-private partnership (PPP) mode in a developing country is eminently doable. 28 Similarly, Aga Khan University (AKU)'s tele-ICU project enabled doctors across Pakistan treating patients in ICUs and HDUs to receive 24/7, free-of-cost consultations from AKU consultants. This initiative was launched in collaboration with the Government of Pakistan, as well as the Governments of Sindh, Punjab, and Khyber Pakhtunkhwa. 29
Active participation from all stakeholders is also critical for the successful implementation of the policy. Communities and patients, as end-users, should be actively engaged through feedback mechanisms. Clear metrics are needed to assess the policy's impact. Key performance indicators (KPIs) should evaluate improvements in healthcare access, patient satisfaction, and cost reduction for patients and providers. Regular evaluations and feedback loops will allow for continuous improvement, ensuring the policy remains responsive to emerging needs and challenges.
The policy should incorporate rigorous training for healthcare professionals in telehealth services, including periodic re-examinations. It must establish standards and regulations to ensure patient privacy and data security are upheld and are meeting the Health Insurance Portability and Accountability Act privacy rules. Additionally, the policy should facilitate partnerships between the public and private sectors to enhance service delivery. Addressing licensing and reimbursement issues is essential, as is integrating telehealth for emergency response strategies. Furthermore, regulations should be implemented for various telehealth platforms, including pricing structures, to ensure transparency, fairness and standardization in service delivery.
We conducted policy analysis of the Sindh Telemedicine and Telehealth Act 2021, which included reviewing the policy context, content, process, and stakeholders. The study highlights the status of telemedicine policy in Sindh and the challenges encountered by stakeholders as well as the barriers and enablers for the adoption of telemedicine policy across the province. We hope our findings will provide a roadmap for other provinces on how to strategically integrate telemedicine into their healthcare systems, thus improving service access and delivery, and ensuring enhanced healthcare accessibility for all.
Study strengths and limitations
The study's strength lies in its multi-method case study approach, incorporating desk review and in-depth interviews with diverse stakeholders for a comprehensive analysis of Telehealth Act in Sindh. This approach, using Walt and Gilson's policy triangle, provides an in-depth understanding of policy factors and implementation barriers and facilitators affecting telehealth platforms. However, the study faces limitations, including potential selection bias while identifying stakeholders and the constraints of desk review in capturing detailed policy implementation realities. Future research should aim for broader stakeholder engagement and empirical analyses of telemedicine implementation, with longitudinal studies to understand the adoption dynamics over time in Sindh.
Conclusion
The Sindh Telemedicine and Telehealth Act 2021 represents a significant legislative step toward formalizing telemedicine within Pakistan's healthcare landscape. This study demonstrates that while the Act provides a necessary regulatory foundation, its effectiveness is contingent on implementation factors such as governance arrangements, technical readiness, and socio-economic context. The analysis identifies critical gaps related to interoperability, pricing regulation, cross-border care, and financial inclusion, while also highlighting the enabling role of strategic public–private partnerships, workforce training, and digital infrastructure investment. By drawing on lessons from neighboring countries and situating these findings within a health systems policy framework, the study offers practical insights to strengthen telemedicine governance in Sindh and provides a transferable reference for other provinces and comparable LMIC settings.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261430096 - Supplemental material for Making policy to bridge gaps in health care access in Sindh, Pakistan: An analysis of the Sindh telemedicine and telehealth act 2021
Supplemental material, sj-docx-1-dhj-10.1177_20552076261430096 for Making policy to bridge gaps in health care access in Sindh, Pakistan: An analysis of the Sindh telemedicine and telehealth act 2021 by Samrah Jawed, Hasan N Tahir, Mustafa Hassan, Lorena Guerrero-Torres, Sara S Khurram and Shifa S Habib in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076261430096 - Supplemental material for Making policy to bridge gaps in health care access in Sindh, Pakistan: An analysis of the Sindh telemedicine and telehealth act 2021
Supplemental material, sj-docx-2-dhj-10.1177_20552076261430096 for Making policy to bridge gaps in health care access in Sindh, Pakistan: An analysis of the Sindh telemedicine and telehealth act 2021 by Samrah Jawed, Hasan N Tahir, Mustafa Hassan, Lorena Guerrero-Torres, Sara S Khurram and Shifa S Habib in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors gratefully acknowledge the time and valuable insights shared by all stakeholder participants in this study.
Ethics approval
Ethical approval for this study was obtained from the Ethical Review Committee at the Aga Khan University, Karachi (ERC # 2023-8997-26440).
Consent to participate
All participants provided informed verbal consent prior to the interviews. Confidentiality and anonymity of all participants were strictly maintained. The study was conducted in accordance with the principles of the Declaration of Helsinki
Consent for publication
Not applicable.
Authors’ contributions
SJ: Conceptualization, methodology, formal analysis, investigation, writing – original draft preparation, and writing—review & editing.
HNT: Literature review, data analysis support, and writing—review & editing.
MH: Writing—review & editing and technical review of the manuscript.
LGT: Methodology, technical input and validation, and writing—review & editing.
SSK: Contribution to discussion, and writing—review & editing.
SSH: Conceptualization, methodology, supervision, data interpretation, writing—review & editing, and overall study oversight as senior author
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: This work received financial support from the Alliance for Health Policy and Systems Research (Alliance). The Alliance is able to conduct its work thanks to the commitment and support from a variety of funders. These include our long-term support from the Swedish International Development Cooperation Agency (Sida) and the Norwegian Agency for Development Cooperation (Norad), as well as designated funding for specific projects within our current priorities. For the full list of Alliance donors, please visit ![]() .
.
Alliance for Health Policy and Systems Research
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data analyzed during the current study consist of anonymized interview transcripts and field notes from 28 stakeholders. This data is not publicly available due to participant confidentiality and ethical restrictions. However, they are available from the corresponding author upon reasonable request, subject to approval from the Aga Khan University Ethical Review Committee.
Supplemental material
Supplemental material for this article is available online.