
Abstract
Background
Short-form video platforms have become primary channels for the public to access health information; therefore, their influence in disseminating knowledge about psychosomatic disorders has garnered increasing attention. We aimed to systematically evaluate the quality, presentation formats and emotional narrative characteristics of short videos concerning cardiovascular disease co-occurring with anxiety and depression on the TikTok and Bilibili platforms.
Methods
A cross-sectional content analysis approach was employed. Popular Chinese-language short videos relevant to the research theme were selected from both platforms. Content quality was assessed using the Global Quality Score, modified DISCERN, and Journal of the American Medical Association frameworks, while the video content was analysed.
Results
Although certain videos conveyed basic medical knowledge, overall quality proved to be inconsistent. Videos from professional sources scored significantly higher than non-professional accounts, with Bilibili content generally demonstrating greater depth and scientific rigour than TikTok. However, in user engagement metrics, non-professional content outperformed professionally produced material. Most videos lacked a thorough discussion of multifactorial disease causes and individual variations, with some exhibiting excessive simplification.
Conclusion
Short-form video platforms hold potential for enhancing health awareness; however, significant tension exists between user preferences and scientific rigour. Multi-stakeholder collaboration and technological support are necessary to improve platform content quality and scientific accuracy.
Introduction
Cardiovascular diseases (CVDs) remain a leading cause of morbidity and mortality worldwide, with increasing recognition of comorbid depression and anxiety as significant contributors of poor clinical outcomes. 1 Epidemiological data indicate that patients with CVD presenting concurrent depressive or anxious symptoms exhibit markedly elevated risks of adverse events, including malignant arrhythmias, heart failure, post-infarction complications, and mortality following coronary intervention procedures. 2 Due to symptom cross-amplification, patients exhibit a heightened demand for information regarding concerns such as ‘stent dislodgement’ and ‘sudden death risk’. However, due to insufficient psychocardiology clinics, they often struggle to access continuous and integrated specialist guidance. 3 Furthermore, psychological distress not only impairs patients’ recovery trajectories but also exacerbates disease perception, intensifies health-related anxiety, and heightens the urgent need for accessible and reliable health information.
Traditionally, to acquire knowledge of CVD accompanied by anxiety or depression, patients have primarily relied on clinicians, hospital educational materials, and public health lectures. 4 However, due to the uneven distribution of healthcare resources, limited doctor–patient consultation time, and heightened patient awareness of proactive health management, an increasing number of patients are turning to emerging platforms, such as the internet and social media, to actively seek health information. 5 Recently, due to their convenience, efficiency, and intuitive visual nature, short-video platforms have become a significant channel for the public to access health-related knowledge. In the digital era, short-video platforms such as TikTok and Bilibili have emerged as primary sources of medical education content. Compared to traditional lengthy texts or specialised medical literature, short videos are more readily disseminated and comprehended. 6 This shift represents a fundamental transformation in health information dissemination, posing new challenges in ensuring the scientific accuracy and authoritative nature of health content. These platforms disseminate medical knowledge through vivid and accessible formats, lowering the threshold for medical science communication. They play a positive role in enhancing public health awareness and promoting patient education. Moreover, user interactions through likes, shares, and comments offer unique insights into patients’ information needs and preferences. Nevertheless, concerns regarding the accuracy, consistency, and overall quality of such content persist, particularly in the intersecting domains of mental health and chronic physical conditions. Existing research indicates that whilst short videos on topics such as lymphoedema, gastro-oesophageal reflux disease and cryptorchidism typically achieve high engagement metrics, their overall quality and credibility remain limited.7–9 Despite the growing popularity of health-related videos on these platforms, evidence assessing the reliability and educational value of information regarding depression and anxiety accompanying CVD remains scarce.
Given the complex interplay between CVDs and mental health disorders, inaccurate or overly simplistic content may mislead patients, exacerbate health-related fears and ultimately compromise clinical decision making. To date, no systematic evaluation has assessed the quality of short-video content associated with anxiety and depression co-occurring with CVDs. Against this background, the current study aimed to conduct a structured cross-sectional content analysis of TikTok and Bilibili videos using validated assessment tools. Additional variables, including video source, uploader identity, audience engagement metrics and content type, were also analysed to quantify the overall credibility, scientific rigour and educational comprehensiveness of the videos. This is a culturally and linguistically specific study. It focuses on short-video platforms featuring Chinese-language content, aiming to explore digital health issues within this particular context. Furthermore, the present study incorporated narrative analysis and the theoretical framework of post-traumatic growth (PTG) to explore the narrative therapeutic efficacy of the videos. By applying standardised assessment tools, this methodology sought not only to map the current landscape of digital health information on these platforms but also to provide empirical evidence supporting healthcare professionals’ engagement. This addresses a critical gap in current digital health communication research, aiming to produce and disseminate reliable health education content in the digital age.
Methods
Research design and ethical statement
In the current study, we evaluated video content related to CVD and depression or anxiety health education on mainstream short-video platforms. We obtained all data from publicly accessible online resources, and no participant's privacy or personally sensitive information was involved. Therefore, the current study did not require an ethical committee approval or informed consent.
Video retrieval and screening
The present study conducted a systematic search on the TikTok and Bilibili platforms. Video selection was based on the platform's overall ranking, which reflects the default sorting order presented to users at the time of sampling. To operationalise overall ranking, we performed searches using a pre-defined set of keywords, recorded the top results returned under the platform's default ranking, and included videos in descending order of appearance until the target sample size was reached. We did not manually reorder results or apply additional filters unless explicitly stated. Because platform ranking is generated by proprietary algorithms and may vary by user profile, location, and time, we standardised the browsing conditions as follows: (1) the same device type and browser settings; (2) a non-logged-in state and cleared cookies and watch history; (3) the same geographic region and language settings and (4) sampling performed within a prespecified time window. These steps were used to reduce personalization-driven variability and improve reproducibility of the selection process. The top 100 videos were retrieved from each platform for the initial screening based on their overall ranking, which was determined by the platform's algorithm. This ranking considers various factors, such as user engagement including likes, shares, comments and view counts, as well as the platform's recommendation system.
Videos were included only if they met the following criteria: (1) the video was published in Chinese; (2) its primary content was directly related to CVD and depression or anxiety, including aetiology, symptoms, diagnosis, treatment or prevention; (3) it had sufficient audio and visual quality to allow for accurate content evaluation and (4) metadata such as upload date, views, likes and comments were available.
Exclusion criteria were as follows: (1) duplicate videos appearing more than once across or within platforms; (2) content not substantively related to CVD and depression or anxiety; (3) explicit advertisements for commercial products or services, including medicines or health supplements and (4) formal academic lectures or conference recordings not intended for the general public.
Data extraction and video classification
For each video included in the analysis, the system recorded basic information such as the title, publication date, duration, as well as the number of likes, saves, comments and shares. Uploader identities were categorised into three types based on profile descriptions and certification status: (1) professional physicians, such as cardiovascular or psychiatric specialists; (2) other specialists, such as those in other disciplines, registered dietitians and other medical professionals and (3) individual users, including patients, health and lifestyle sharers, and other individuals without a medical background.
Evaluation tools
In the current study, a multidimensional evaluation system was developed to assess the quality and reliability of short videos related to CVD and depression or anxiety on TikTok and Bilibili. This framework was established to ensure the scientific rigour and validity of the analysis. Three internationally recognised instruments were used: the Global Quality Score (GQS), modified DISCERN (mDISCERN), and Journal of the American Medical Association (JAMA) benchmark standards. The GQS utilises a five-point scale to rate videos based on content completeness, dissemination effectiveness and scientific value. A score of one reflects low quality, whereas a score of five reflects high quality (Table 1). 10 The mDISCERN score was adapted from the original instrument to suit the characteristics of short videos, thus covering five domains: content accuracy, traceability, scientific basis, impartiality and risk disclosure. The total score quantitatively reflects the reliability of the information (Table 2). 11 The JAMA Benchmark criteria enable supplementary assessment of authority and transparency by evaluating authorship, source attribution, currency and conflict-of-interest disclosures (Table 3). 12 The integrated use of these tools enables a comprehensive, multilevel evaluation of the professionalism, scientific rigour, and educational value of CVD and depression or anxiety. The specific details of these three scales are set out in the Supplemental table.
The Global Quality Score (GQS) quality criteria.

The modified DISCERN (mDISCERN) quality criteria.

The Journal of the American Medical Association (JAMA) benchmark criteria.

To address the study's aim of exploring the ‘narrative healing efficacy’ of short videos, we first conceptualised this construct as the video’s potential to provide emotional validation, foster a sense of hope and guide adaptive coping, thereby supporting viewers’ psychological adjustment alongside disease management.
This conceptualisation is grounded in established theoretical and empirical literature. Empathetic expression is foundational to therapeutic communication and narrative understanding in healthcare; it validates patients’ distress and fosters trust, which are essential for psychological adjustment. 13 Hope orientation reflects a cognitive-motivational process involving goal-directed thinking and pathways to achieve goals; it is consistently associated with greater resilience and better adaptation in chronic illness populations. 14 Actionable advice such as the provision of clear, specific behavioural guidance can enhances self-efficacy, a key determinant of successful health behaviour change and self-management.15,16
Guided by this conceptual framework, we therefore pre-defined and coded three key emotional and narrative dimensions as operational indicators for assessing the presence and extent of narrative healing content in the sampled videos: (1) Empathetic Expression: whether the video contained understanding, validation and emotional support for the patient's distress; (2) Hope Orientation: whether it conveyed beliefs about symptom improvement, recovery possibilities or positive coping; (3) Actionable Advice: whether it provided specific, actionable behavioural guidance (e.g. seeking professional help, self-monitoring and practicing relaxation techniques).
Subsequently, during the results analysis stage, we introduced PTG theory as an interpretive lens to provide a deeper, theoretical understanding of these empirical findings and to evaluate the potential of the video content to facilitate positive psychological transformation beyond mere disease adaptation.
The evaluation team consisted of two attending physicians with qualifications in internal medicine who independently assessed all the sampled videos. To ensure scoring consistency, prior to the formal assessment, all raters underwent unified training. For cases with significant discrepancies, such as a difference of one point or more on any single item for the same video, a senior cardiovascular or psychiatric specialist made the final decision. The inter-rater reliability for both quality and reliability assessments was determined using Cohen's kappa coefficient. A value greater than 0.8 was considered as excellent agreement, 0.6 to 0.8 indicated substantial agreement, 0.4 to 0.6 represented moderate agreement, and values below 0.4 reflected a poor agreement.
Word frequency statistics
To conduct frequency analysis on the pre-processed data, a word frequency tool was employed. The occurrence count for each term was tallied and sorted in descending order of frequency, yielding a list containing the vocabulary alongside their respective frequency values.
Statistical analysis
To assess the normality of each variable's distribution, we first used the Shapiro–Wilk test. For variables following a normal distribution, the descriptive statistics were reported as the mean and standard deviation. Comparisons between two groups of non-normally distributed data were conducted using the Mann—Whitney U test, while comparisons involving three or more groups were performed using the Kruskal—Wallis H test. To further explore the relationships between user engagement metrics and video quality or reliability scores, Spearman's rank correlation coefficient was calculated. The strength of the correlations was categorised according to the absolute value of the coefficient. Descriptive statistics were used to summarise video characteristics. A p-value of less than 0.05 was considered statistically significant.
Results
Uploader characteristics
A total of 155 videos were included in the analysis, with 68 obtained from Bilibili and 87 from TikTok (Figure 1). In the present study, video uploaders were primarily categorised as professional physicians (cardiovascular or psychiatric specialists), other specialists and individual users (Figure 2(a)). The categorisation of uploaders was primarily based on the information available in their profile descriptions, which may indicate their professional background or area of expertise. On TikTok, professional physicians dominated with a 59.30% share of uploads, followed by other specialists, while individual users accounted for a smaller percentage. On Bilibili, professional physicians remained the primary uploaders at 44.12%; however, unlike TikTok, individual users contributed more than other specialists (Figure 2(b)). Figure 2(c) shows that professional physicians uploaded 52.26% of videos, other specialists accounted for 24.52%, and individual users contributed 23.23%. Figure 2(d) reveals that, on TikTok, professionals contributed to 87.36% of content, with non-professionals accounting for 12.64% only. Conversely, on Bilibili, professionals contributed 63.24%, whereas non-professionals constituted 36.76%. In summary, professionals are the primary content contributors on both TikTok and Bilibili, with this trend being particularly pronounced on TikTok.
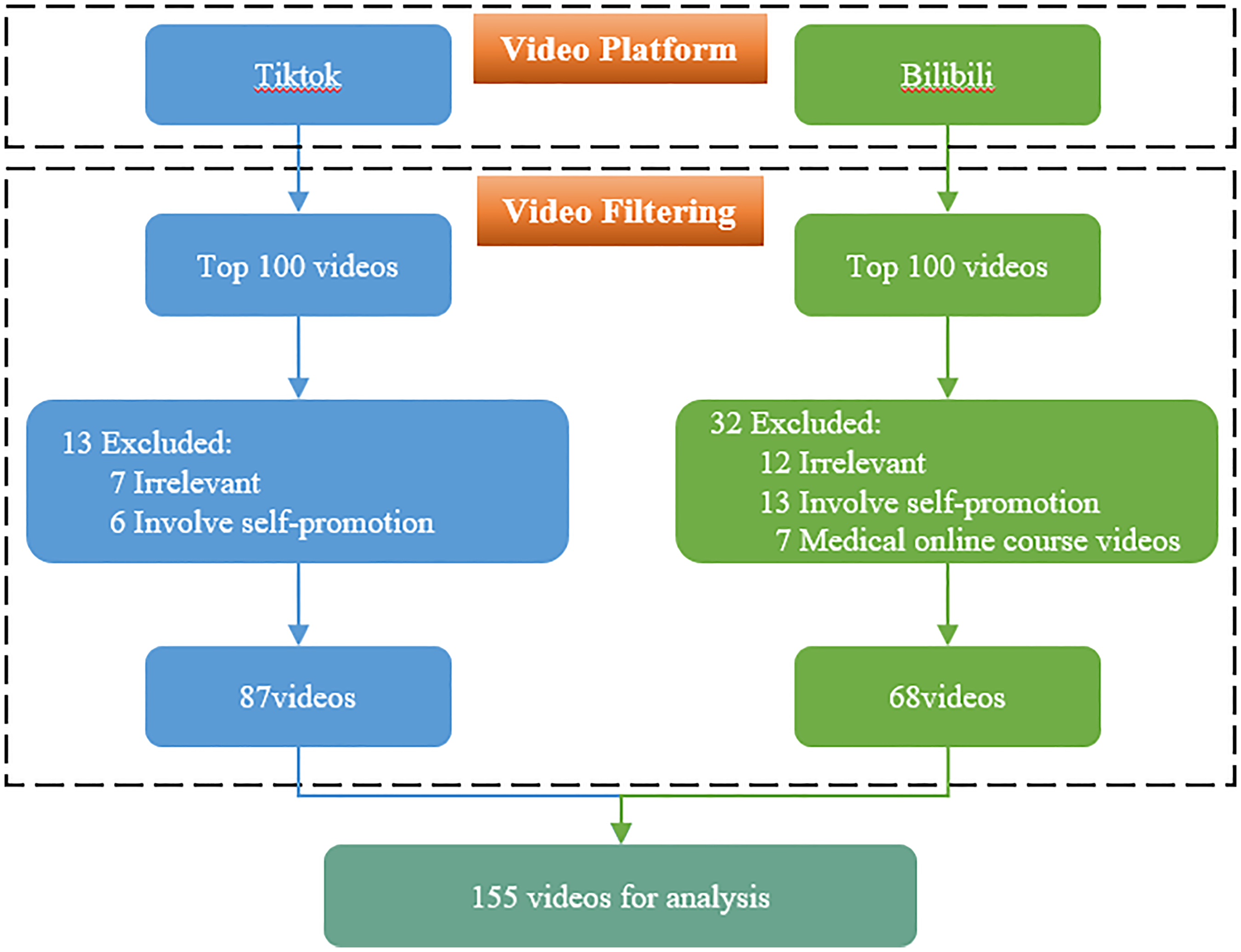
Flowchart illustrating the video selection process on TikTok and Bilibili.

Distribution of video uploaders on Bilibili and TikTok.
Video characteristics
Comparison of the platforms revealed significant differences in multiple key indicators. The Bilibili group had longer video forms than those from TikTok (p < 0.001), reflecting TikTok's preference for rapid and concise content. Regarding user engagement, Bilibili videos received significantly fewer likes (median: 9, interquartile range [IQR]: 3–149) and collections (median: 7, IQR: 3–33.5) compared to TikTok. However, no statistically significant differences were observed between the two platforms regarding comments and shares (p > 0.05), suggesting that engagement behaviours vary depending on platform design and content circulation mechanisms; specific parameters are shown in Table 4. As shown in Table 5, video length differed among the groups (p < 0.001), with individual users having the longest median duration (median: 241, IQR: 126–376), followed by other specialists (median: 117.5, IQR: 48.25–164.75) and professional physicians (median: 98, IQR: 67–167). No statistically significant differences were observed in likes (p = 0.661) or collections (p = 0.188). Comments showed statistically significant variation (p = 0.003), with individual users having the highest median count (median: 82.5, IQR: 5–246.75), compared to other specialists (median: 8, IQR: 2–19.75) and professional physicians (median: 8, IQR: 3–27). Further, shares differed significantly (p = 0.034), with individual users having the highest median shares (median: 36, IQR: 4–158), followed by professional physicians (median: 9, IQR: 3–37) and other specialists (median: 8, IQR: 3.25–17.75).
The general information of videos on TikTok and Bilibili.

The general information of videos about uploader on TikTok and Bilibili.

Video quality
The GQS score was significantly higher on Bilibili than on TikTok (Figure 3(a)). Similarly, both the mDISCERN score (Figure 3(b)) and the JAMA score (Figure 3(c)) were higher for videos on Bilibili. These results suggest that the overall quality and reliability of videos on Bilibili were superior to those on TikTok, specific parameters are shown in Table 4. Table 5 show that professional physicians had higher GQS scores compared to individual users and other specialists (Figure 4(a)). Professional physicians and other specialists had higher mDISCERN scores compared to individual users (Figure 4(b)). Professional physicians had a higher upper quartile JAMA score compared to individual users and other specialists (Figure 4(c)). The results of the Cohen's kappa test showed strong consistency in the scoring process, with kappa coefficients of 0.836 for GQS scores, 0.761 for mDISCERN scores, and 0.781 for JAMA. These coefficients of reliability were specifically calculated.

Comparison of quality and reliability scores between TikTok and Bilibili.

Distribution of quality and reliability scores across different types of uploader groups.
Video content
As shown in Table 6 and Figure 5, 52.9% of the videos presented treatment-related information. These videos discussed both pharmacological interventions for cardiovascular symptoms and psychological approaches, such as anxiolytics, antidepressants and structured cognitive support. Aetiological explanations appeared in 48.39% of the videos. These included recognised risk factors, such as hypertension, atherosclerosis, emotional stress, sleep disturbances and autonomic dysfunction. This aligns closely with the results of the word frequency analysis, where high-frequency terms such as anxiety, depression, autonomic nervous system, heart disease and hypertension frequently appeared, indicating that the public has developed a basic understanding of how emotions affect the body. Symptoms were addressed in 45.16% of the samples; commonly reported symptoms included palpitations, chest tightness, insomnia and fatigue, aligning closely with high-frequency keywords such as chest tightness, palpitations, insomnia, anxiety and depression. Diagnostic procedures were mentioned in 59.35% of the videos and covered standard cardiovascular assessments, including electrocardiography and echocardiography, alongside mental health screenings using validated tools such as the Generalised Anxiety Disorder seven-item scale and the Patient Health Questionnaire-9. Population-level characteristics were described in 54.19% of the videos, while prognostic considerations were present in 57.42% of the content. These included recurrence risk, the potential for emotional triggers to exacerbate cardiac conditions, and the importance of ongoing follow-up. Some videos emphasised that a lack of intervention in dual-heart disease, wherein patients suffer from both CVD and a comorbid mental health condition such as depression or anxiety, could lead to the mutual deterioration of both cardiovascular and mental health, highlighting the basic risks of disease progression (Supplemental Tables S1 and S2).

Comparative content quality assessment of videos between TikTok and Bilibili.
The video content on TikTok and Bilibili.
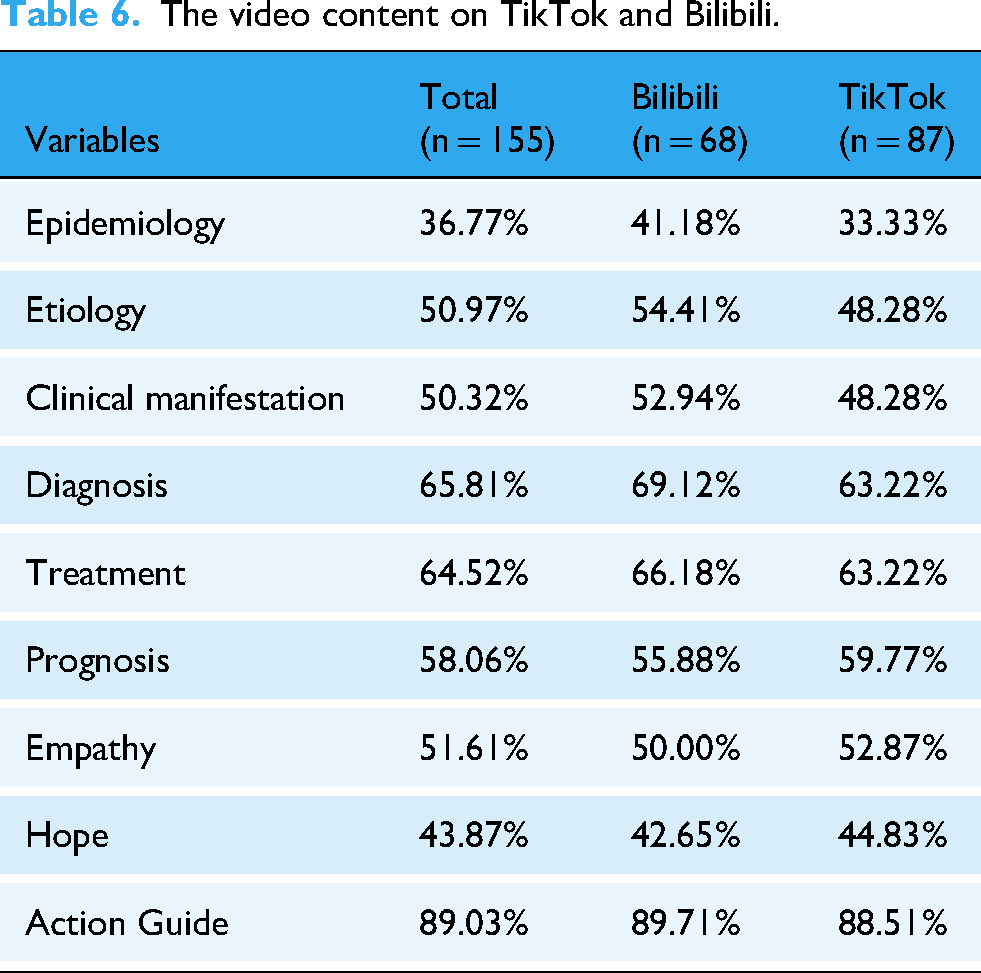
Empathy-related content appeared in 51.61% of the total video sample. The presence of empathy was slightly more frequent on TikTok, where 52.87% of videos expressed empathetic content, compared to 50% on Bilibili. Hope-oriented communication was found in 43.87% of all videos; these messages often focused on recovery potential, the benefits of early intervention, and the capacity to manage dual heart disease with proper support. TikTok again showed a marginally higher inclusion rate at 44.83%, compared to 42.65% on Bilibili. In contrast to the relatively modest inclusion of emotional elements, action-oriented guidance was strongly represented across the platforms. A total of 89.03% of videos included explicit action suggestions, such as seeking medical evaluation, monitoring blood pressure or practising stress management techniques. The proportions were nearly identical across the platforms, with 89.71% for Bilibili and 88.51% for TikTok (Table 6 and Figure 5).
Correlation analysis
To examine the relationships between user interaction metrics and video quality scores, Spearman correlation analysis was performed. The results are summarised in the correlation matrix shown in Figure 6.
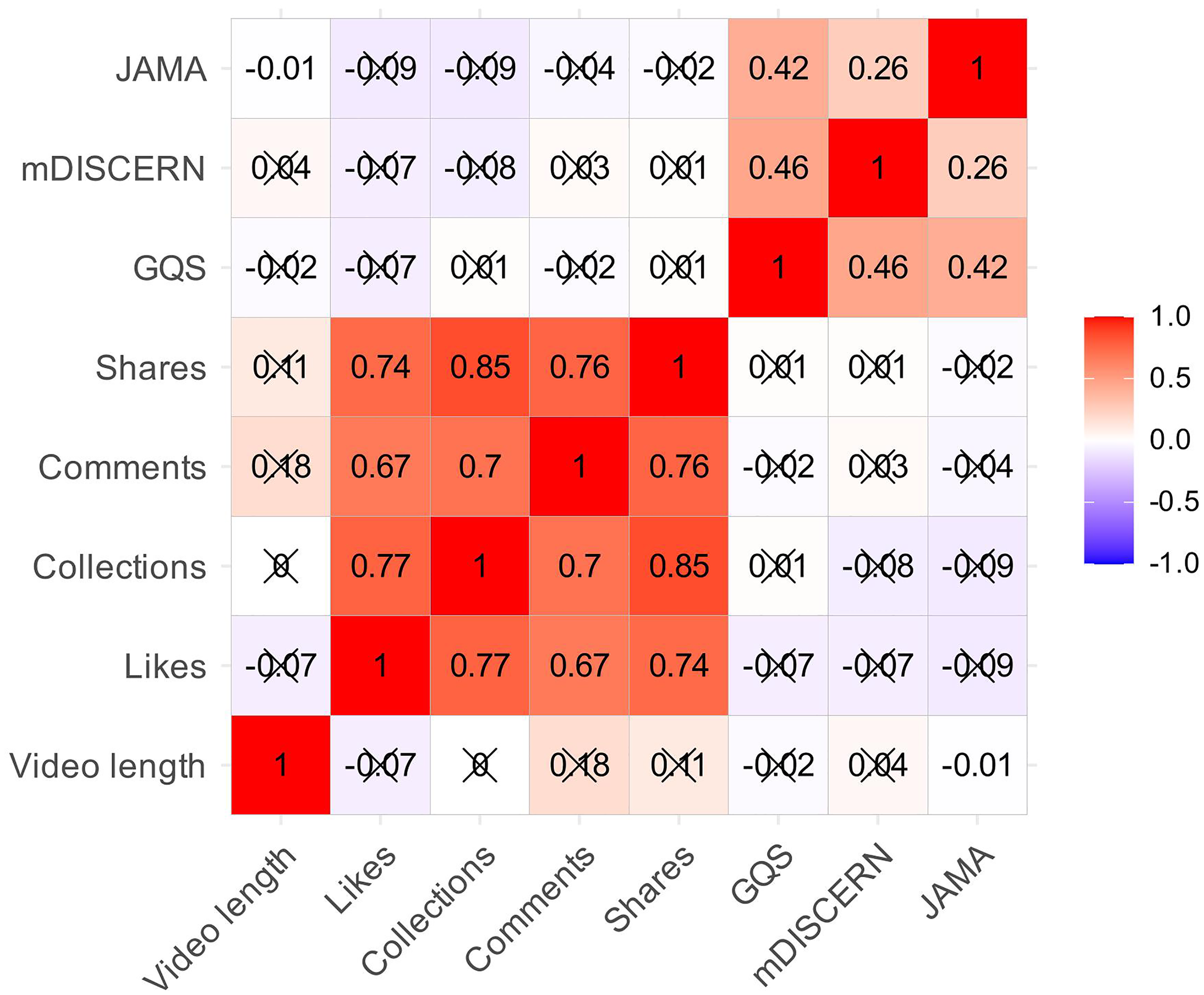
Correlation matrix of Spearman's correlation analysis between video metrics and quality scores.
A significant positive correlation was observed between user interaction variables. For instance, the correlation coefficient was r = 0.77 between likes and saves, r = 0.74 between likes and shares, and r = 0.85 between saves and shares. Moreover, moderate to strong positive correlations were observed between likes and comments (r = 0.67), saves and comments (r = 0.70), and comments and shares (r = 0.76). These findings indicate that, in actual audience behaviour, interactive actions often occur in tandem. That is, when a video receives a high number of likes, it is frequently accompanied by increased bookmarking, commenting and sharing.
Discussion
This study conducted a cross-sectional content analysis to systematically evaluate the quality, reliability, and narrative features of short-form educational videos related to CVD accompanied by anxiety or depression on TikTok and Bilibili. Using validated tools, including the GQS, mDISCERN and JAMA, to explore the emotional and therapeutic depth of the content, we assessed 155 videos for scientific rigour, source credibility and user engagement metrics. Additionally, we incorporated narrative analysis based on the PTG framework.
Our findings revealed substantial variability in video quality across platforms and uploader types. Compared to videos produced by individual or non-specialist users, videos by healthcare professionals consistently demonstrated higher-quality and reliability scores. Despite receiving fewer user interactions, Bilibili videos exhibited significantly superior performance on three evaluation scales compared to those on TikTok. However, user engagement metrics such as likes, comments, and shares were higher on TikTok, underscoring a significant disconnect between content popularity and scientific reliability. Notably, most videos lacked depth in communicating multifactorial disease mechanisms or supporting emotional growth, with limited integration of PTG-oriented therapeutic narratives. The significance of the present study lies in its contribution to the empirical understanding of digital health content dissemination in psychosomatic contexts. Further, it highlights the pressing need to balance scientific accuracy with user engagement in the evolving landscape of health communication. These findings offer practical implications for clinicians, digital content creators, and platform governance bodies aiming to improve the quality of public-facing medical information, particularly in the context of chronic diseases complicated by mental health comorbidities.
Currently, the GQS, mDISCERN and JAMA scoring tools are widely employed to evaluate health science communication content on digital platforms.17,18 Our findings indicate that videos on the Bilibili platform achieved significantly higher scores across all three assessment frameworks compared to TikTok videos. This disparity may relate to platform architecture and content ecosystems: Bilibili supports extended, structured knowledge dissemination and encourages in-depth interaction within comment sections, facilitating comprehensive scientific communication chains. In contrast, TikTok prioritises short-form, high-frequency information delivery, often employing entertainment formats to enhance content expressiveness. This observation aligns with prior research, indicating that differing platform support for content presentation and knowledge depth may directly influence health information quality. 19
Furthermore, the present study found that videos created by professional physicians and other specialists outperformed those by individual users across all three assessment frameworks such as GQS, mDISCERN and JAMA. This finding reaffirms the critical role of professional expertise in ensuring content quality and scientific credibility. Further, our results align with existing literature, indicating that expert-generated content is more likely to adhere to evidence-based medicine standards.20–22 However, user engagement metrics for such specialised content, such as likes, comments and shares, typically lag behind those of videos posted by individual users. This suggests a potential disconnect between users’ assessment of information quality and scientific standards. Spearman correlation analysis further confirms this viewpoint. Particularly within short-form video platforms, audiences often demonstrate greater receptiveness to intuitive, vivid forms of expression, while showing limited interest in medically structured yet somewhat austere content.
This trend aligns with prior research findings on short-video platforms, indicating that videos with high engagement metrics do not necessarily possess greater informational credibility or educational value. Although higher engagement may reflect content appeal, it does not inherently indicate that the content is more educational. Engagement metrics are often influenced by factors such as emotional resonance, accessibility, entertainment value and cultural relevance, which can increase the appeal of content without enhancing its educational value. Thus, user preferences may prioritise aspects like entertainment or relatability over the quality or accuracy of the information presented. For instance, in the current study, videos emphasising patients’ personal experiences, emotional expression and lifestyle advice garnered higher engagement rates, whereas content covering pathological mechanisms, drug mechanisms, or prognostic assessments remained relatively niche. In fact, compared to material laden with technical jargon or specialised discourse, videos featuring an accessible style and plain language were markedly more popular. This phenomenon raises concerns about the risk of misleading content on platforms, as it may inadvertently amplify misinformation, exaggerate the efficacy of certain interventions, or even delay patients’ access to standard medical advice. In the intersection of mental health and CVD, misleading information could have more severe consequences, such as increasing health anxiety, reinforcing catastrophic ideation, or even undermining patients’ adherence to established treatment regimens.
In terms of video content, certain videos offer overly simplistic lifestyle or dietary advice that often lacks scientific rigour, overlooking individual variations, the multifactorial nature of diseases and the importance of medical intervention. For instance, some content portrays a single food or behaviour as a cure for heart disease or a cure for depression and anxiety, yet such claims disregard the multifactorial aetiology of CVDs and associated psychological disorders, including genetics, environment, behaviour and psychology.
23
Furthermore, such recommendations frequently fail to account for variables such as the patient's age, sex, comorbidities, or social support systems, and they overlook the critical role of healthcare professionals’ clinical assessments and the importance of personalised treatment pathways. When disseminated without context, such content may be misinterpreted as universally applicable advice, potentially leading audiences to forgo seeking professional medical counsel. This not only undermines public understanding of disease complexity but may also delay early diagnosis and timely intervention.
24
To examine the narrative therapeutic efficacy of the video, the present study further incorporates narrative analysis and the theoretical framework of PTG. PTG theory posits that individuals, following the resolution of highly challenging life crises, do not merely return to their previous state but undergo significant and profound transformations. These changes manifest as substantial enhancements in adaptive capacity, functional status or life awareness, particularly within three domains: interpersonal relationships, self-perception and life philosophy.25,26 This differs from mere psychological resilience, emphasising a transformative transcendence and growth. 25 A CVD diagnosis accompanied by anxiety or depression undoubtedly constitutes a traumatic event capable of destabilising an individual's core belief system, thereby creating the preconditions for PTG to occur.
To further examine the narrative healing efficacy of the video content, this study incorporated the analytical perspective of PTG theory. PTG posits that individuals may experience positive transformation across several core domains such as interpersonal relationships, self-perception and philosophy of life following a major trauma. However, our analysis reveals that current video content shows significant deficiencies in supporting such deep growth narratives, and these shortcomings correspond directly to key PTG domains. In the domain of interpersonal relationships, content predominantly focuses on the patient's individual symptoms and solitary struggles, lacking depictions of how illness could serve as an opportunity to deepen family support, build therapeutic alliances or connect with peer support groups. In the domain of self-perception, content emphasises guiding patients to ‘prevent risks’ or ‘manage symptoms’, rarely empowering them to recognise and narrate the resilience, newfound personal strength or regained sense of control over life demonstrated during their coping process. In the domain of philosophy of life, most content is confined to a ‘restoring health’ narrative framework, seldom guiding viewers to reconstruct life meaning and priorities, or to explore a deeper appreciation for life fostered by the illness experience. Even the 43.87% of videos conveying hope-oriented messages mostly remain at the level of general encouragement, failing to integrate with the specific PTG growth dimensions mentioned above. This analysis, which directly connects the PTG theoretical framework to identified content gaps, highlights the originality of using this theory to illuminate the deep healing value of health videos.
However, our analysis indicates that current content fails to effectively support this process. At the interpersonal level, the videos predominantly portray patients’ solitary struggles rather than demonstrating how illness may serve as an opportunity to deepen bonds with family members and individuals with the same conditions. Regarding self-perception, content predominantly instructs patients to avoid vulnerability, such as guarding against sudden death, yet scarcely empowers them to recognise the newfound strength and sense of efficacy emerging from their disease management journey. Regarding life philosophy, content largely remains confined to the restorative narrative of disease management, lacking guidance on reconstructing meaning. 27 Even the 43.87% of videos conveying hope-oriented messages fail to explore deeper dimensions, such as reassessing life priorities or cherishing the present, which could foster a higher-order quest narrative. 28
The absence of this PTG perspective results in a fundamental deficiency in the therapeutic efficacy of platform content. Further, numerous videos, particularly those from non-professional sources, unconsciously reinforce chaos narratives, exacerbating viewers’ catastrophic thinking and feelings of powerlessness. This runs counter to the original intent of emotional healing and squanders opportunities to utilise creative expression for profound psychological transformation.
The characteristics of relevant video content reveal significant patterns in contemporary health communication. A substantial proportion of the reviewed videos present treatment strategies and symptom explanations, indicating growing recognition of the need for integrated care addressing both physiological and psychological dimensions. This aligns with recent clinical discussions emphasising the bi-directional relationship between emotional health and cardiovascular function, a perspective supported by psychosomatic medicine research. The parallel presentation of pharmacological and psychological interventions reflects a shift in public health communication towards more comprehensive care models. 29 Numerous videos incorporate information on aetiology, clinical symptoms, and diagnostic processes, indicating that public-facing content creators are progressively aligning with the medical frameworks outlined in professional guidelines. Such content contributes to enhancing public health literacy, particularly when introducing clinically validated screening tools and specialised terminology. However, notably, variations in depth and accuracy persist in materials shared by non-professional creators.
The majority of videos offer action-oriented advice, such as seeking medical assistance or managing stress. Existing research indicates that emotionally resonant information enhances recall, trust and adherence to guidance, with this effect being particularly pronounced in mental health contexts. 30 Consequently, although videos provide practical guidance, the absence of an emotional tone may diminish their effectiveness. Of particular note is the relative scarcity of discussion on epidemiological context and disease prognosis within the video samples. The results show that only 36.77% of videos mention the epidemiological context, and 43.87% offer hope-oriented narratives. This finding suggests that a significant portion of the videos lack critical epidemiological information, which could potentially skew viewers’ understanding of their own health risks. Additionally, the relatively low percentage of hope-oriented or PTG-based narratives could limit the therapeutic potential of these videos for individuals facing both heart-related and mental health challenges. The absence of these important elements may reduce the videos’ ability to offer meaningful psychological support and health education, ultimately affecting their public health impact. Without situating health information within broader population frameworks, audiences may develop distorted perceptions of personal risk or treatment urgency. This observation aligns with previous research highlighting the importance of contextual framing for precise risk communication. 31 Furthermore, overly simplified descriptions of treatment outcomes may mislead audiences into overlooking the chronic and often fluctuating nature of CVD co-occurring with mental health conditions.
The current study offers important insights into the quality of health-related content on short-form video platforms. Nonetheless, to provide a balanced understanding of the findings, it is crucial to acknowledge the current study's limitations.
The first limitation is the platform scope. This study focused on TikTok and Bilibili due to their popularity in China, enhancing cultural relevance but limiting broader applicability. Future studies should include international platforms like YouTube and Instagram for wider comparisons. Additionally, personal profile descriptions may not always accurately reflect uploaders’ qualifications, and misclassification is possible. In general, engagement-driven signals can increase a video's likelihood of being surfaced, whereas information accuracy is not necessarily an explicit ranking objective. As a result, videos that are more attention-grabbing or emotionally salient may achieve higher visibility even when their scientific quality is suboptimal. Accordingly, our results should be interpreted as reflecting the information environment encountered by typical users under default ranking conditions, rather than an evaluation of all available videos. Future research could improve classification accuracy by reviewing video content or cross-referencing credentials. Second, the study used a cross-sectional design, which captures data at a specific point in time. This approach may not fully capture evolving trends or the rapid changes that are common on algorithm-driven platforms. As video quality and engagement metrics can fluctuate over time owing to shifts in platform algorithms, user behaviour, and content trends, longitudinal research is required to track the evolution of these factors. Without such an assessment, our findings are limited to a snapshot of the video content and engagement at the time of data collection. Future studies employing a longitudinal design would provide valuable insights into the dynamic nature of digital content and its engagement over time. Third, although standardised evaluation tools were used, video quality assessment remains partially subjective, as differences in reviewer interpretation may affect consistency. Future research should consider automated content analysis for greater objectivity. Fourth, the absence of demographic data on viewers limits analysis of how different groups respond to video content. Including factors like age, sex, and health literacy would improve intervention targeting. Lastly, although we attempted to control for personalisation by focusing on videos that were broadly ranked highly across the platforms, notably, platform-specific ranking algorithms may still influence video visibility. These algorithms often prioritise content based on user behaviour and engagement patterns. Therefore, although our selection methodology aimed to capture a representative sample of popular videos, the influence of these algorithms on visibility remains a potential limitation. Moreover, although restricting retrieval to top-ranked videos may prioritise capturing popular content, we opted for this approach to focus on videos with the highest visibility and engagement, assuming these are most likely to reflect broader trends and themes within digital health communication. However, it may not fully represent all types of content, especially less popular but potentially valuable educational videos. Future research could explore a more diverse sample to balance popularity with informational representativeness.
Taken together, these limitations highlight the requirement for further research that is both methodologically rigorous and sensitive to the evolving digital landscape. Expanding the scope of platforms, improving evaluation techniques, and integrating user-level data will help build a clearer picture of how short-form videos contribute to public health communication.
Conclusion
The current study reveals disparities in the quality, presentation formats and dissemination effectiveness of short video content concerning CVDs co-occurring with anxiety and depression across TikTok and Bilibili platforms. Although some content possesses educational value, overall quality remains inconsistent, with insufficient professionalism being a prevalent issue. Platform structures and user preferences exert a degree of influence over the scientific rigour of content and its dissemination reach. Given the quality-popularity paradox identified in the present study and the significant lack of a PTG perspective, current Chinese short-video platforms urgently require the development of a novel health narrative for content on dual heart disease. This narrative must integrate scientific rigour with emotional healing, effectively guiding positive psychological transformation while having a favourable audience reach. Research limitations include temporal constraints on the sample period, a narrow selection of platforms and the subjective nature of content evaluation. Future studies should broaden the scope of platforms, integrate artificial intelligence tools to enhance content analysis, and explore more precise models for assessing user receptivity and intervention effectiveness, thereby providing stronger empirical support for digital health communication.
Supplemental Material
sj-xlsx-1-dhj-10.1177_20552076261430066 - Supplemental material for The quality and reliability of short videos on cardiovascular disease combined with anxiety or depression and their narrative healing efficacy
Supplemental material, sj-xlsx-1-dhj-10.1177_20552076261430066 for The quality and reliability of short videos on cardiovascular disease combined with anxiety or depression and their narrative healing efficacy by Jianing Li, Mingxiao Ren and Tao Shi in DIGITAL HEALTH
Footnotes
Acknowledgements
We extend our gratitude to all participants and the consortia for their valuable contributions.
Ethics approval
This study did not involve human participants, clinical data, experimental animals or histological research. All analysed data were sourced from publicly accessible video content, with data collection fully adhering to the video platform's terms of service. No private or personally identifiable information was collected or processed, nor was any interaction undertaken with users. Consequently, ethical approval was not required.
Consent for publication
Not applicable.
Author contributions
Jianing Li: Methodology; Formal analysis; Writing – Original Draft.
Mingxiao Ren: Conceptualization; Investigation; Writing – Review & Editing.
Tao Shi: Supervision; Project administration; Writing – Review & Editing.
All authors have read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Innovative Research Program of Heilongjiang University of Chinese Medicine (2024yjscx106).
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Guarantor
JL.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.