
Abstract
Introduction
Nursing shortages in the United States have worsened in recent years, with a decline of more than 100,000 registered nurses between 2020 and 2021. These shortages strain health systems, increasing nurse workloads and negatively impacting patient care. The rise of telehealth solutions, accelerated by the COVID-19 pandemic, has increased the use of virtual nursing (VN) as a potential solution to support bedside nurses and reduce burnout. However, there is limited research on VN's implementation and integration into existing nursing workflows. This study examined the challenges and effective strategies perceived by stakeholders for the implementation and integration of VN, providing insights for health systems planning to adopt or scale VN services.
Methods
This qualitative study was conducted with 18 stakeholders of a VN program at a large urban hospital in the southeastern United States: six virtual nurses, nine bedside nurses who utilized VN in their patient care workflow, and three members of the program's VN leadership. Participants completed a 30-min semi-structured interview about their experience with implementation of the VN program.
Results
Four themes emerged related to VN implementation and integration. (1) Training: Bedside and virtual nurses described the need for formal and hands-on training. Virtual nurses cited ongoing group sharing as beneficial. (2) Technology challenges and benefits: Bedside nurses experienced some challenges related to functioning of the tablets and the need for live technical support. Confidentiality was maintained through virtual nurses’ use of private space and headphones. (3) Communication and collaboration: The secure chat system was seen as integral to bedside and virtual nurses’ ability to collaborate and coordinate patient care. (4) Leveraging experienced nurses: VN leadership and bedside nurses perceived the hiring of experienced bedside nurses for the role of virtual nurses as beneficial for mentoring and supporting bedside nurses.
Conclusions
The perceptions of VN program implementation from nurse and leadership perspectives as identified in this qualitative study informed recommendations for effective strategies for addressing challenges and facilitating VN implementation. The findings and recommendations can be used by health systems as they plan to integrate or scale VN.
Introduction
Health care systems nationwide are faced with nursing shortages due to burnout, an aging nursing workforce, and challenging work environments.1–4 While nursing shortages are associated with poor patient outcomes, they also exacerbate nurse workloads, leading to increased burnout and lower job satisfaction. 5
During the COVID-19 pandemic in 2020–2021, more than 100,000 registered nurses (RNs) in the United States left the workforce due to stress, burnout, or retirement,6,7 accelerating the adoption of innovative telehealth tools and transforming healthcare nationwide. 8 As telehealth became more ubiquitous, virtual nursing (VN) emerged as a transformative care delivery model. VN offers a solution to alleviate nursing burnout and turnover, leveraging technology and remote nursing expertise to reduce the burden on bedside nurses. 9 It enables nurses to complete patient care tasks remotely by using telehealth tools such as audio/video communication tools, remote patient monitoring, and electronic health records (EHRs).10,11 Virtual nurses are often experienced former unit nurses who want to remain in the nursing workforce but in a capacity removed from the bedside.
Approximately 52% of organizations reported plans to introduce VN programs in 2024, the highest planned adoption growth for the second consecutive year. 12 Some hospital leaders have expressed reluctance to implement VN programs due to concerns about integration into an already complex nursing workflow. 13 Nursing workflows encompass the frequency, duration, and pattern of activities and processes nurses must perform to provide patient care. These include, for example, patient assessments, vital signs checks, and medication administration; documentation in EHRs; communication with providers and other staff; transfer of information during shift handoff; supply management; and patient discharge. 14 In a recent needs assessment conducted by Khairat et al., virtual nurses and unit nurses reported workflows as a key process factor required for VN. Streamlining workflow processes is crucial for facilitating operational efficiency, optimizing the patient care experience, and reducing healthcare costs.
Given the novelty of VN and stakeholder concerns about its integration into workflows, research is urgently needed to better understand VN implementation. Specifically, gaps exist around how VN fits into existing nursing workflows and the challenges stakeholders, and health systems more broadly, face during implementation of VN. In addition, guidance for addressing these challenges is lacking. This qualitative study aimed to explore perceived challenges and effective response strategies among stakeholders involved with the implementation and workflow integration of a VN program.
To address these gaps, this study was guided by the Consolidated Framework for Implementation Research (CFIR), a meta-theoretical framework that synthesizes constructs from existing implementation theories to identify determinants of implementation success. 15 CFIR organizes factors into five domains: Intervention Characteristics (e.g., complexity and adaptability of the intervention), Outer Setting (e.g., external policies and patient needs), Inner Setting (e.g., organizational culture and readiness), Characteristics of Individuals (e.g., knowledge and beliefs of implementers), and Process (e.g., planning and engaging stakeholders). By applying CFIR, this qualitative study aimed to explore perceived challenges and effective response strategies among stakeholders involved with the implementation and workflow integration of a VN program, providing theoretically grounded insights for health systems.
Methods
Study design and objectives
This qualitative study consisted of semi-structured interviews with VN stakeholders to explore their nuanced perceptions of the implementation of the VN program, including the challenges they had encountered and their ideas and experiences of effective response.
VN program description and setting
The VN program is implemented in a major hospital in an urban community in the southeastern United States with more than 600 inpatient beds. Virtual nurses within this hospital system have several years of experience as bedside nurses, giving them the expertise to engage in informed clinical decision-making. They complete key tasks such as admission assessments, medication reconciliation, patient education, and patient discharges through the audio/video calls on a tablet, using the institution's EHR. The VN program helps to distribute the nursing workload, freeing up time for bedside nurses to focus on physical care tasks and spend more time with their patients.
Additionally, the VN program is located adjacent to the hospital, which is often a preference among virtual nurses and patients given the virtual nurses’ familiarity with the health system. Patients must be alert and oriented to participate in a VN session. Once the patient agrees to see a virtual nurse, the bedside nurse initiates the VN workflow via the EHR and the virtual care tablet. Additional information about this workflow process has been published elsewhere. 10
Recruitment and study sample
The study team used purposive sampling to identify key informants to interview. The health system's Virtual Care Center provided a list of potential candidate names and contact information for the following stakeholder categories: virtual nurses employed at the hospital's Virtual Nurse Center; bedside RNs employed at the health system who worked on units with access to VN services; and VN leadership staff employed in the health system. Members of the team sent screening surveys to the potential candidates to determine eligibility and interest in participating voluntarily. Participants who were deemed eligible and interested were then sent calendar invitations to participate in a 30-min interview with the study team's nurse informatician (Jennifer Morelli). The primary study team (Saif Khairat, Jennifer Morelli) had no prior relationship with any of the participants prior to interview sessions. Participants were informed that the study was being conducted by the study team to gather information about the VN program, and that participation was voluntary.
In total, six virtual nurses, nine bedside nurses (five charge, four unit), and three members of VN leadership were interviewed. No participants refused to participate or dropped out after signing up.
Data collection
The study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist to ensure rigor and transparency in reporting qualitative methodology (Supplemental File A). 16
The interview guide for each stakeholder group (virtual nurses, bedside nurses, and VN leadership) was developed by the study team with oversight from the hospital's leadership and nursing staff. Each guide focused on VN implementation and how each respective group of participants had integrated VN into their workflow. The guides were piloted prior to finalization and use. (See interview guides in Supplemental File B).
Semi-structured interviews were conducted from July 2023 through December 2023 by the study team's nurse informatician (Jennifer Morelli), who was trained in facilitating semi-structured interviews. Interviews took place in person or via Zoom, in a private setting with only the participant and study team present, and were audio recorded. Interviews lasted approximately 30 min. Participants were offered a $25 gift card for their participation.
Data analysis
Audio recordings from the interviews were transcribed using the Microsoft Word transcription feature. A qualitative analyst on the study team checked the transcriptions for accuracy by reviewing approximately 25% of each transcript. When accuracy was flagged for quality, the entire transcript was reviewed and edited; no repeat interviews were deemed necessary. The qualitative analyst also reviewed the transcripts for content on an ongoing basis to determine when thematic saturation had been reached in the three stakeholder groups, i.e., when no new information was emerging in the interviews. 17 Upon thematic saturation in each group, no further interviews were conducted.
For the thematic analysis, data were coded and analyzed using Dedoose and Excel software to identify themes across participants. 18 First, transcripts were read by the qualitative analyst, who then developed a codebook with emergent parent and child codes. A second qualitative research assistant reviewed four transcripts independently to ensure consistent understanding and application of codes. Minor differences in code definition and application were reconciled by consensus. Preliminary themes were identified inductively through discussion and consensus among the study team and were then organized by parent codes to identify key insights and relevant excerpts.
Interview participants were not given the opportunity to review their transcripts or the emergent codes and themes. The terms “challenges” and “key strategies” were not defined for participants; rather, these categories represent participant-reported perceived barriers and facilitators to VN implementation and integration.
Results
Table 1 shows the participant demographics. Of the 18 total participants, six (33%) were virtual nurses, nine (50%) were inpatient nurses, and three (17%) were VN leadership staff. Sixteen (89%) were female and 17 were white (94%). Virtual nurses had a high average of years of nursing experience at 26.7 years, while inpatient nurses averaged 6.7 years of experience. The average year of experience for both nurse groups was 14.7 years. VNs had more experience in the institutional EHR used, at 10.5 years compared to 3.9 years of EHR experience among bedside nurses.
Participant demographics (N = 18).

Themes
Parent and child codes derived from interviews are shown in Figure 1.

Parent and child codes related to VN implementation.
Four themes emerged from the interviews related to VN implementation and integration: (1) training; (2) technology challenges and benefits; (3) communication; and (4) leveraging experienced nurses.
Training
The bedside and virtual nurse participants reported several needs around training during the rollout of VN.
Bedside nursing staff expressed the need for clear communication around what the VN program is, who it is for, and when it is available from VN and hospital leadership. They reported instances of miscommunication from hospital administration in the early days of VN implementation which had led to confusion and frustration: It was confusing for a little while because at first, we were told they're going to be here seven days a week. They were always available. But then it was like, oh, they're not there on Sundays, or they stop at 6:00 p.m.—Bedside (unit) nurse As for support from them and the rollout, I don't think we really [had any]. We just had a piece of paper that had the steps on how to log in, which wasn't very helpful. I ended up remaking it for my better understanding and to help other people. Nurses … we got to do it ourselves to figure it out.—Bedside (charge) nurse They had virtual nurses come in person and help us learn how to set them up. They actually set patients up with the [tablet]. They sat with us and worked through any issues, and that was very helpful, in my opinion. I liked that they weren't virtual. They actually came in person. They were able to answer our questions and troubleshoot things.—Beside (charge) nurse It's a lot of steps to me …. People who are not as comfortable with technology, they're scared to just push buttons. Unless they've been told, like, three times, this is the one to push. So, it could be a little bit hard for them.—Beside (charge) nurse Things come up, and learning on the fly might not be the best idea. I almost think it would be good if you held a class and talk to [new VNs] about how you approach people, how do you initiate the conversation? Do you look them in the eye, or do you look at your keyboard the entire time? There's a lot of things that would be helpful.—Virtual nurse Every other month we have a virtual nurse meeting, where we go over the data and are given an opportunity to put our thoughts out there. And we very much use the “sharing is caring” philosophy around here. So when one of us finds something that works great, we share it so others can give it a try and see if it works great for them as well.—Virtual nurse
Technology challenges and benefits
Bedside nurses frequently reported challenges related to technology. For example, they described negative experiences related to the setup of the tablet to connect the patient to the virtual nurse. The process required many steps and, occasionally, the tablets would not load correctly. They also reported that for privacy reasons, the virtual care tablet must be reset between patient encounters, which is a tedious process. The [tablets] are not super user friendly to set up. It seems kind of silly that … every time you use it, the [tablet] has to wipe itself clean and then restart, versus just having some device that is only used for this program and it's ready to go. Oftentimes you have to try three or four different [tablets] to even get it to work, and so for people who are not comfortable with technology, they don't even use it.—Unit nurse I would not call IT for anything … I've never heard them say anything about [VN] ….They always talk about software issues to do with [the EHR] and your desktop and all that stuff, but nothing to do with this tablet. So I don't know who services them or handles any issues that come up other than rebooting them and praying to God that it works.—Virtual nurse We have to submit a ticket, and then who knows how long it takes …. It all comes back to having a very heavy workload, and then if the [tablet] is not working, and they don't have time to sit down, put a ticket in, wait for a response.—Bedside (charge) nurse I rate [VN availability] pretty high, especially during the week. There are usually several nurses on board who are available to help, especially during our heavy discharge time.—Bedside (charge) nurse I've got my black background blurred …. Our headsets are noise canceling, and so when we have headsets on, nobody can hear any of the responses that the patients are giving. [Other virtual nurses may] hear us ask the questions, but they don't hear [the patient's] responses because we have noise canceling headsets.—Virtual nurse We'd really rather [the VNs] not work at home. You need dedicated bandwidth. You need to be no distractions, no dogs, no lawn mowers. You need all of those things, and you need to know you're at work. And so when you're at work, you want to be able to carry yourself like you're at work and not worry about the slamming door and the doorbell ringing, et cetera.—VN leadership
Communication and collaboration
Communication through a secure chat messaging system was described by both the bedside and virtual nurses as integral to successful collaboration to coordinate patient care as part of the nursing workflow. The system was integrated within the EHR, allowing for quick and secure communication between the two groups. They described it as one reason why bedside and virtual nurses have been successful in communicating with each other, even when juggling other responsibilities. It provides a way to collaborate on patient care tasks, for bedside nurses to remain informed about tasks virtual nurses are performing with patients, and for the communication of needed information from the virtual nurse to the bedside nurse if concerns or issues arise during the patient and VN session.
One bedside nurse described appreciating how well VN is integrated into the workflow process thanks to communication processes and practices: They do a great job… [A VN] usually will respond back to me and give me a time frame for when they will connect. If there's any complications, they will secure-chat me directly there… And at the end of the session, they will send a very detailed report on what they talked about, any concerns the patient might have, anything that the patient might have left to do for discharge. That way, I know what needs to be done to proceed with, getting that patient home.—Bedside (charge) nurse When we set it up, we send a secure chat to the virtual nurse and let them know that our patient's ready for admission or discharge… And then afterwards, the virtual nurse sends us a message…anything that they learned during the admission process that would affect their care or things that we need to know … I like secure chat because I can refer back to it if I'm busy.—Bedside (unit) nurse I hate [secure instant messaging] because sometimes there's 10 messages popping up on the screen …. This is distracting at times. But it's there for a purpose.—Virtual nurse
Leveraging experienced nurses
VN leadership described the program's leveraging of experienced nurses who value patient care as a key factor in its success. Recruitment has focused on experienced bedside nurses who are no longer able or do not want to continue providing bedside care to transition into a role that allows them to provide patient care virtually. They reported that the first virtual nurses recruited to form the VN team were purposefully selected and included experienced nurses passionate about providing the best possible patient care. They reflected that this was helpful in building the initial team and helped ensure the program's success. Another goal of the program, obviously, is to retain experience and expertise in the nursing workforce… Every nurse that we approached said, “I don't want to leave my patients. I'm going to miss interacting with the patients.” And I think that's part of the key to our success, that our nurses love their patients and that shines through over the screen, which is really hard to do.—VN leadership I had great hesitation at leaving the bedside because it's such a passion and love for me being with patients. As I've transitioned to this side and realizing that I still can be a very good nurse and connect virtually and still learn things … I don't feel stagnant at all and I feel excited to be able to do this. And yet have a little bit of the less bedside stress that was there for a very long time especially.—Virtual nurse Our virtual nurses have a combined experience level of over 200 years between nine nurses. And so that's someone that you as a nurse can trust your patient with.—VN leadership
However, recruiting nurses with this level of experience was described as not feasible for all VN teams in their health system. In particularly, recruitment for virtual nurses at smaller community hospitals has been more difficult than at their main hospital. As a result, the smaller hospitals have virtual nurses with less experience, which can be negative for bedside nurses who draw on experienced virtual nurses as mentors to answer patient care or nursing questions. Our large community hospital has put only those with experience behind the camera. Our smaller hospitals have had less experience, behind the camera, which I think if you're using it in a mentoring fashion, you really need to have the more experienced nurse.—VN leadership
Discussion
To our knowledge, this was the first qualitative study to explore VN implementation from a nurse and leadership perspective through the lens of implementation science. Guided by the CFIR, our findings were structured around four key domains that correspond to the emergent themes: (1) Intervention Characteristics (technology challenges and benefits), (2) Inner Setting (workflow integration, communication, and collaboration), (3) Characteristics of Individuals (leveraging experienced nurses), and (4) Process (training and rollout strategies). This structured approach not only contextualized our findings within an established implementation framework but also provided actionable insights for health systems seeking to adopt or scale VN programs (Figure 2).

CFIR aligned thematic map of virtual nursing implementation. Intervention Characteristics captured technology challenges and perceived benefits. Inner Setting reflected workflow integration and collaboration enabled by EHR embedded secure chat. Characteristics of Individuals emphasized the role of experienced nurses in building trust and providing mentorship. Process described training and rollout strategies, including clarity of program scope, hands on onboarding, and VN specific communication skill development.
The study described the implementation and integration of the VN program into nursing workflows and identified effective practices and challenges faced by bedside and virtual nurses. The findings align with and extend existing literature on telehealth implementation, while also highlighting novel insights specific to VN models.
Recommendations
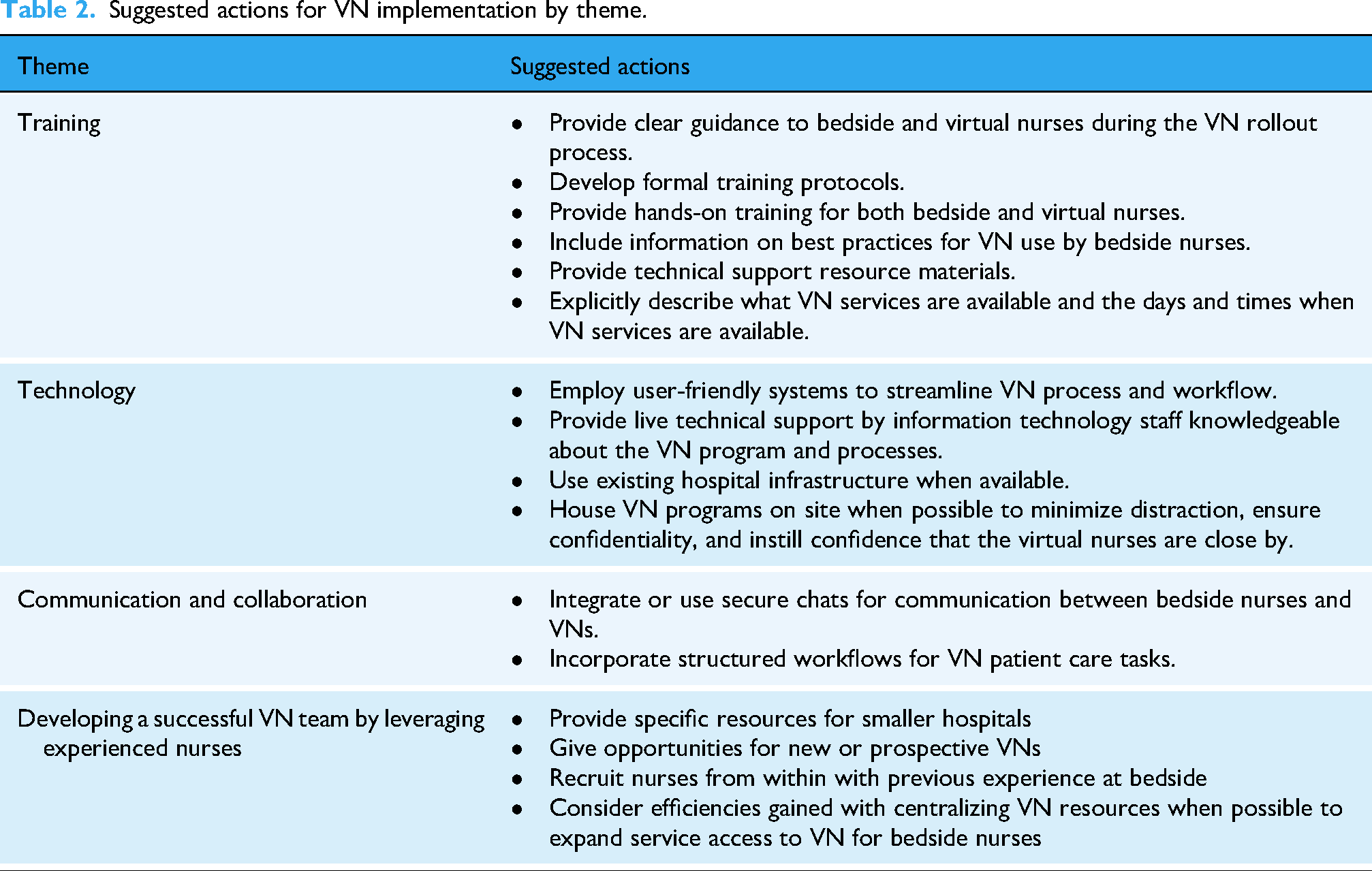
Based on the study findings, a summary of suggested actions for health systems to consider when implementing VN is provided in Table 2.
Suggested actions for VN implementation by theme.
Process: training, rollout, and ongoing support
As suggested by our findings, improvements in the initial rollout and training during the implementation process are important when establishing buy-in among bedside nurses. Formal training protocols on the VN process should include how bedside nurses connect patients to VN calls, how to resolve minor issues, and whom to contact in the event of technical issues. These protocols should also include clear communication from the hospital on VN hours of operation, availability, and best practices for use. Bedside nurses also spoke highly of the use of in-person demos and training, particularly for charge nurses who became nurse champions on their units. Nurse champions are key to driving change management, 19 as they can increase utilization and buy-in on their units by other nurses.
Intervention characteristics: technology usability and design
Our interviews highlight the need to develop user-friendly systems that provide a streamlined setup process to facilitate the VN process. These systems should have integrated technology, technical support, and troubleshooting if available. Most of the negative feedback of VN was centered around interactions with the tablet, including the cumbersome setup process and technical issues experienced by both bedside and virtual nurses. Issues with technology have been shown to interfere with nurses’ ability to provide quality care. 20 When possible, use of integrated technology including in-room solutions may streamline the VN process.
Additionally, both bedside and virtual nurses interviewed described not knowing whom to contact in the event of technical issues and reluctance to contact hospital technical support. Nursing staff operate under demanding workloads, and time spent solving technical issues or waiting on technical support may take away from other nursing tasks. 21 Identifying a specific person or department to contact for live technical support may increase nurse confidence in using the technology.
We also recommend that VN programs be housed on-site or near the physical location of the healthcare facility to reduce distractions for virtual nurses and to increase trust in VN among patients and bedside nurses. Lack of trust in telehealth may lead to diminished use of VN services, as distrust has been shown to lead to negative telehealth outcomes. 22 Conversely, patients without technical issues and with no concerns about their privacy have been shown to have a higher degree of trust in their healthcare provider. 23
Workflow integration and communication systems
Nurse workflow integration and nurse communication and collaboration were demonstrated to be crucial components of VN implementation and continued use. Incorporating structured workflows for patient admission and discharge processes could help to delineate responsibilities for completion of patient care tasks. Streamlined VN integration may increase adoption and use by bedside nurses, preventing chaotic nurse workflows that may contribute to nurse burnout. 24 As supported by nurses’ positive perceptions of the secure chat messaging system, we also suggest providing a method for the beside and virtual nurses to communicate patient information quickly and securely, ideally built into their existing EHR interface. Studies have shown improvement in patient care coordination and management between healthcare staff utilizing instant messaging, 25 and integration within an existing interface or platform negates the need for a separate application.
Characteristics of individuals: the role of experienced nurses
Our findings suggest the benefit of staffing the VN team with experienced and passionate nurses who are willing to provide nursing care using the VN model. When not possible to recruit experienced nurses for VN, as may be the case at smaller community hospitals, we recommend providing specific support and resources to build and sustain a VN workforce. This includes providing opportunities for new or prospective virtual nurses to gain experience behind the camera and recruiting nurses from within their hospital with previous experience as a bedside nurse. In addition, staffing models should be considered for rural settings to accommodate virtual nurses located at satellite sites at greater distances from the patient care facility, with26–28 ongoing bi-directional communication between bedside and virtual nurses26,29 and in-person team building26–28 to bridge perceptions that the virtual nurses are too far removed from the facility.
Additionally, utilizing experienced nurses from the health system to fill VN roles may be especially helpful in building trust with patients and bedside nurses. Studies of tele-ICU nurses show increased communication and trust when current or former nurses at that hospital are employed in telehealth roles. 30 One tele-ICU program even set up a program to introduce its telehealth nurses to the bedside nurses to increase rapport and satisfaction, which also had a positive effect on communication, timeliness, and accuracy. 31 It may be beneficial for health systems to have instances where VN staff can go on-site to the patient units to meet bedside nurses and unit managers to build rapport and trust to increase buy-in among unit staff.
Limitations
Our study has some limitations. The interview participants may not fully reflect the full spectrum of VN implementation practices within this health system. There may have been selection bias in the list of potential participants the Virtual Care Center provided to the study team for screening, with the potential for the recommended individuals to be more engaged in or positive about VN. Additionally, this study was limited to one hospital at a health system using one modality of VN. Additional research is needed to determine the extent to which experiences represented in this study align with experiences in other health systems. Furthermore, comparisons of different types of VN programs, such as tele-ICU and VN rounding, are needed as those formats may present different implementation challenges.
In our interviews, we utilized an open and exploratory approach. Some challenges or recommendations may have been excluded by participants. Although perhaps not comprehensive, our findings provide a foundation for future examination of VN implementation across settings and programs. Furthermore, our findings provide insights for health systems leaders that could be used to guide decisions about how best to initiate a VN program and support their nursing staff operating within a VN program.
Conclusions
This study identified the challenges and recommendations for VN implementation among stakeholders of a VN program in a hospital system in the southeastern United States. Our findings refine CFIR for telehealth-enabled VN by showing that adoption hinges on “digital workability” (e.g., reliable devices, low setup burden), and they extend CFIR by highlighting “digital workflow coupling” through EHR-embedded secure chat plus message load effects, alongside experienced nurse capital and telepresence execution as core determinants of uptake. The actionable recommendations produced based on the challenges and facilitators identified, with regard to the required infrastructure and tools to develop VN programs, staffing needs and support, communication systems, and protocols and collaboration strategies for successful VN implementation, can support health systems to navigate the complexities of VN implementation. Future research on VN should build on our findings, including exploring how VN affects patient and organizational outcomes, bedside and virtual nurse satisfaction, and long-term sustainability for VN programs.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261425406 - Supplemental material for Virtual nursing implementation and workflow integration: A qualitative study of challenges and effective strategies
Supplemental material, sj-docx-1-dhj-10.1177_20552076261425406 for Virtual nursing implementation and workflow integration: A qualitative study of challenges and effective strategies by Jennifer Morelli, Callie Rockey-Bartlett, Christopher M. Shea, Barbara S. Edson and Saif Khairat in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076261425406 - Supplemental material for Virtual nursing implementation and workflow integration: A qualitative study of challenges and effective strategies
Supplemental material, sj-docx-2-dhj-10.1177_20552076261425406 for Virtual nursing implementation and workflow integration: A qualitative study of challenges and effective strategies by Jennifer Morelli, Callie Rockey-Bartlett, Christopher M. Shea, Barbara S. Edson and Saif Khairat in DIGITAL HEALTH
Footnotes
Acknowledgments
The study team would like to thank Ariana Avila and Sharita Thomas for their assistance on this project. We would also like to thank the nurses and members of leadership who participated in interviews.
Ethical considerations
The Institutional Review Board at the University of North Carolina at Chapel Hill reviewed and approved this study on March 26, 2025 (Study No. 23-2580, Reference ID 468520) with a determination of not human subjects research and a written informed consent waiver.
Consent to participate
All participants interviewed for this study were provided with informed consent and verbally consented to participate.
Author contributions
Jennifer Morelli: conceptualization, data curation, formal analysis, investigation, software, supervision, validation, visualization, writing–original draft, and writing–review and editing. Callie Rockey-Bartlett: data curation, formal analysis, validation, writing–original draft, and writing–review and editing. Christopher M. Shea: conceptualization, methodology, resources, software, validation, and writing–original draft. Barbara S. Edson: conceptualization, resources, supervision, and writing–original draft. Saif Khairat: conceptualization, formal analysis, funding acquisition, methodology, resources, supervision, validation, writing–original draft, and writing–review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Health Resources and Services Administration (HRSA) (Grant 6 U3GRH40003-01-01) and the National Center for Advancing Translational Sciences of the National Institutes of Health (NIH) under Award Number RC2TR004380 and the UNC School of Nursing. The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of HRSA or NIH, nor does mention of department or agency names imply endorsement by the U.S. Government. UNC School of Nursing, and supported by the National Institute Of Nursing Research of the National Institutes of Health under Award Number R01NR021711.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data sets presented in this article are not readily available as they are part of ongoing data analysis. Requests to access the data sets may be directed to Saif Khairat.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.