
Abstract
Background
As part of the global digital health transformation and Saudi Vision 2030 priorities in chronic disease prevention, understanding public acceptance and preferences for telenutrition services is crucial for developing effective digital nutrition care platforms.
Objectives
This study aimed to adapt, translate, and validate a U.S.-based national telemedicine survey for the Saudi context, to assess adults’ prior use, comfort, willingness, and preferences regarding direct-to-consumer (DTC) telenutrition services.
Methods
A cross-sectional survey was completed by 930 Saudi adults recruited from major urban cities. The survey instrument was adapted, translated, and validated using standard procedures, including internal consistency reliability using Cronbach's alpha coefficient. Descriptive statistics, chi-square tests, binary logistic regression, and two-step cluster analysis.
Results
Among 930 respondents, 61.5% expressed comfort and 54.9% reported willingness to use telenutrition services, increasing to 78.5% when referring to family members. Key predictors of willingness included previous experience with virtual care (OR = 1.52, p < 0.001), comfort with video consultations (OR = 1.39, p < 0.001), and access to personal health records (OR = 1.20, p < 0.041). Willingness was significantly higher among younger adults (18–29 years), employed individuals, and residents of Jeddah. Cluster analysis revealed three segments: digitally engaged and receptive, selective and independent, and supportive but personally hesitant—each characterized by differing levels of comfort and willingness to use DTC telenutrition services. Notably, only 1.3% could identify a telenutrition platform in Saudi Arabia.
Conclusions
These findings underscore the need for culturally tailored, digitally inclusive telenutrition platforms that address sociodemographic differences. Investing in digital health literacy and infrastructure is essential for empowering nutrition care delivery in Saudi Arabia.
Keywords
Introduction
Telehealth in Saudi Arabia has evolved from bridging healthcare gaps in rural areas to becoming a crucial component of the health care system, offering improved accessibility and cost-effective tools.1–6 The Saudi Vision 2030 aims to invest in digital healthcare, but cultural and technical issues still remain. 7 The rising burden of lifestyle-related chronic disease in Saudi Arabia 8 has resulted in the demand for accessible and novel approaches for telenutrition services. Telenutrition delivered by Registered Dietitian Nutritionist (RDN) is defined by the Academy of Nutrition and Dietetics as “The interactive use by an RDN of electronic information and telecommunications technologies to implement the Nutrition Care Process with patients or clients at a remote location, within the provisions of the RDN's state license as applicable,”9,10 has emerged as a viable strategy to expand service reach and continuity. Globally, the COVID-19 pandemic catalyzed widespread adoption of digital health solutions, including in the Arab region, where over 76% of dietitians in Saudi Arabia and across 10 countries turned to telenutrition and social media to sustain patient care during lockdown.11,12 In 2024, a cross-sectional study on Saudi dietitians’ perceptions of telenutrition revealed positive attitudes despite challenges related to limited anthropometric data and technical issues. 13 Saudi Arabia's Vision 2030 framework, which prioritizes health sector digitization, positions telenutrition as a key vehicle for enhancing care access and efficiency. 4 Evidence from randomized controlled trials and systematic reviews support the efficacy of telenutrition interventions in improving weight management, glycemic control, and overall dietary quality, showing comparable or superior outcomes to in-person consultations. 14 Emerging models integrating nutrition into clinical care, such as the plant-based pathways described by Arslan (2024) demonstrate how nutrition interventions can be embedded into routine services through digital and hybrid delivery models, further supporting the relevance of DTC telenutrition within Saudi Arabia's digital health transition. 15 Additionally, Eid et al. (2024) have conducted a telenutrition weight loss program, supported by weekly telemonitoring and monthly telehealth coaching resulted in significant positive outcomes such as weight loss, improvements in stress management, enhanced quality of life, and increase in nutrition knowledge across overweight and obese population.16–23 Despite participants citing life pressures and unmet goals as reasons for dropout, most have reported positive experiences with the program, suggesting that telenutrition, telemonitoring, and telehealth coaching enhance engagement and adherence to the diet. 24 High levels of user satisfaction have also been reported, often attributed to convenience, lower cost, and reduced travel time. 25 A nationwide survey by Welch et al. (2017) explored patient preference for direct-to-consumer (DTC) telemedicine across different provider relationships. The findings showed that patients were significantly more willing to use telemedicine when it involved their own provider, highlighting the importance of trust, continuity of care, and access to personal health records in driving acceptance or remote health services. 26 Yet, the study only examined patient preference for DTC in high income countries, with no nationally representative research examining public perceptions, attitude, and readiness for DTC telenutrition platforms specifically in Saudi Arabia. Understanding how the Saudi community receives and adopts telenutrition is critical to expanding equitable access to nutrition care in a digital era. Few studies have investigated the factors influencing the acceptance of digital health services, highlighting a consistent set of determinants influencing user experience and perception. Almazroi (2022) have reported perceived usefulness, ease of use, privacy, and trust were key predictors of telenutrition acceptance among diabetic patients while these factors have been studied in clinical populations, a lack of population-level insights is observed in Saudi Arabia. 5
The current study seeks to address this gap by adapting, translating, and validating a U.S.-based national telemedicine survey for the Saudi context and for use in telenutrition research. Using a large, demographically stratified sample, we aimed to explore Saudi adults’ perspectives on DTC telenutrition, identify drivers of acceptance, and assess comfort with virtual dietetic consultations. While previous literature5,12,26,27 has explored virtual care adoption generally (e.g. access, usability, and perceived usefulness in broad telehealth contexts), and did not specifically examined population-level readiness, comfort, and willingness for DTC telenutrition in Saudi Arabia. Therefore, our research aimed to answer three primary questions: (1) What are the experiences and perceptions of Saudi adults regarding DTC telenutrition services? (2) Which demographic and experiential factors predict willingness to use virtual nutrition care? and (3) How do attitudinal and behavioral segments differ in their readiness to adopt telenutrition?”
Materials and methods
Study design, settings, and participants
The present study used a nationwide, cross-sectional survey design to assess the Saudi adult population's perspectives, preferences, and comfort with DTC telenutrition services. Recruitment and data collection occurred from May-2025 to September-2025, via an online data collector in the three main cities targeted in the study, to be nationally representative to ensure broad demographic representation. Inclusion criteria included Saudi adults, aged between 18 years or older, who completed an informed digital consent form before starting the survey. Participants were included regardless of health status, technology literacy, or previous exposure to telehealth services, and completed ≥80% of the survey. Participants were excluded if they were younger than 18 years old, reported non-Saudi nationality, did not complete up to 80% of the survey, and declined to provide a digital informed consent. Only responses that met all inclusion criteria and passed quality screening were retained for analysis. Eligible participants were then stratified by gender, age, and geographic representation, covering major cities across Saudi Arabia's western (Jeddah), central (Riyadh), and eastern (Dammam) regions. These cities represent the country's primary urban population hubs and therefore formed the basis of our stratified sampling approach. The study was conducted within the general population targeting adult participants aged 18 and above who provided informed digital consent. The primary analysis set included all participants who met inclusion criteria and completed the full survey (N = 930). To minimize bias, we used stratified sampling across major demographic groups, applied standardized online survey procedures, and implemented data-quality checks to remove incomplete or duplicate responses. This cross-sectional survey was designed and reported in accordance with the STROBE (strengthening the Reporting of Observational Studies in Epidemiology) checklist, which is provided in Supplemental file 1.
Sample size
Sample size determination was estimated based on precision-based calculation, assuming confidence level of 95%, power of 90%, and an expected minimum detectable difference for key outcome (e.g. willingness score on a 5-point Likert scale) of 0.2 points. 26 Accounting for potential non-response and dropout, the target sample size set at 930 participants. This size aligns with methods used in international validation surveys and ensures representativeness for multivariable analysis. A sample of 100 participants were randomly selected for the test-retest reliability analysis over a two-week interval.
Survey instrument adaptation, translation, and validation
The original survey was adapted from a validated U.S.-based national telemedicine survey 26 to reflect the terminology, contextual relevance, and conceptual scope of telenutrition services. The adaptation followed a structured guidelines from Doyon et al. (2023), 28 involving modifications by domains of experts to maintain content validity. The U.S. Telemedicine Survey was selected because it is a validated, nationally used instrument that comprehensively measures telehealth acceptance, comfort, and behavioral intention. No equivalent validated tool for telenutrition existed in Arabic or in the Saudi context at the time, making it the most appropriate foundation for adaptation. Thus, the modified version included additional items targeting Saudi cultural factors, preference for provider characteristics, willingness to pay, family member use, and the digital platforms previously used for virtual health care in Saudi Arabia. Items were grouped into domains reflecting prior experience, willingness, comfort, preferred service attributes, and specialty. The survey instrument was translated to Arabic and validated following the methodology used by Masoud and Mosli (2023). 29 The process followed WHO-recommended cross-cultural adaptation steps. First, an expert panel of bilingual registered dietitians conducted forward translation of the adapted English survey into Arabic, reviewing cultural suitability and domain content. This version was blind back-translated by a separate bilingual translator. Discrepancies were resolved through regular meetings. Content validity was assessed via a panel of five academic experts who rated each item on clarity, simplicity, consistency, and ambiguity using a 4-point scale. Feedback was collected on item consistency, clarity, simplicity, ambiguity according to criteria described, as shown in Table 1. Item-Level Content Validity Index (I-CVI) and Scale-Level CVI (S-CVI) were both 1, indicating full agreement.
Demographics of respondents (N = 930).

Values are expressed as frequencies (n) and percentages (%). Descriptive data were used to summarize categorical variables.
Pretesting and internal consistency reliability
To ensure content clarity and practical usability, a pretesting phase was conducted among 90 participants from diverse demographic, equally distribution among the three main cities. Participants completed the online survey to evaluate item comprehension, flow, and completion time. Feedback was collected from a subsample (30) on item consistency, clarity, simplicity, ambiguity according to criteria described previously. Approximately two weeks after the initial administration, the same individuals were contacted again to complete the survey a second time. Test-retest reliability was then determined by calculating the intraclass correlation coefficient (ICC) between the cumulative scores of responses to comfort, desired attributes, and willingness where it was collected in a 5-point Likert scales to assess the stability of the responses over time. Thus, internal consistency reliability was evaluated using Cronbach's alpha coefficient to determine the degree of inter-item reliability (0.874), which was considered acceptable, as shown in Supplemental file 2. Measures included random stratified sampling by age, gender, and region, data-quality checks for duplicate entries, use of validated items, and pretesting to reduce measurement bias. All participants completed the same online survey using identical question formats and response scales.
Variables and definitions of the adapted and validated Arabic survey for telenutrition assessment
Primary outcome: willingness to use virtual telenutrition (binary yes/no)
Secondary outcomes: comfort score, preference variables
Predictors: age categories, education levels, city, experience with virtual care
Confounders considered: gender, age, marital status, education, employment, income
Cluster variables: comfort, willingness (self), willingness (family); the Adapted and Validated Arabic Survey for Telenutrition Assessment used in this study is provided in Supplemental File 3.
Statistical analysis
Data were analyzed using SPSS (version 27). Descriptive statistics were used to summarize sociodemographic characteristics, prior telenutrition experience, comfort and willingness to use virtual services, and perceived barriers and preferences. Missing data were addressed using multiple imputation with fully conditional specification.
Ordinal variables (comfort and importance ratings) were analyzed as ordered scales, while age and income were categorized into predefined population-based groups. Frequencies and percentages were reported for categorical variables. Associations between categorical variables were examined using chi-square (χ2) tests.
A binary logistic regression model was used to identify predictors of willingness to use virtual nutrition services. Willingness was dichotomized by coding “willing”/“very willing” as 1 and all other responses as 0. All sociodemographic variables (gender, age group, marital status, education, employment status, and city of residence), prior experience, comfort measures, and perceived importance of digital service features were entered initially. Non-significant predictors were removed using the enter method with a retention threshold of p < 0.10 to avoid excluding potentially meaningful variables in exploratory analysis. Model fit was assessed using the Hosmer–Lemeshow test, and explained variance was evaluated using Cox & Snell and Nagelkerke R2 statistics. Model classification accuracy, sensitivity, and specificity were examined at a 0.50 probability cut-off.
A sensitivity analysis was performed by rerunning the model using (1) complete-case data only and (2) alternative probability thresholds (0.40 and 0.60) to assess robustness of effect estimates and classification performance. Predictor variables included ordinal ratings, binary exposures (e.g. prior virtual service use, time constraints), and categorical factors using dummy coding, with “High school/diploma” and “Riyadh” as reference groups. Multicollinearity was assessed using variance inflation factors, all <2, indicating no collinearity concerns. No adjustments for multiple comparisons were applied due to the prespecified predictor set, but results were interpreted cautiously regarding type I error.
Cluster analysis
To identify distinct participant profiles based on their attitudes and behaviors toward virtual nutrition services, a Two-Step Cluster Analysis was conducted using SPSS version 27. The analysis included three key binary and ordinal variables: comfort with virtual nutrition services, willingness to follow-up virtually for oneself, and willingness for family members to receive virtual follow-up. The two-step method was selected due to its ability to handle both categorical and continuous variables simultaneously and to automatically determine the optimal number of clusters using the Bayesian Information Criterion (BIC). The log-likelihood distance measure was used, and the model was set to identify up to 15 clusters, with automatic model selection based on BIC. Cases with missing values on any of the clustering variables were excluded. The clustering process produced a solution with three distinct clusters. Cluster quality was evaluated using the silhouette measure of cohesion and separation, which yielded a value of 0.5, indicating fair to good quality. Cluster group characteristics were then compared using chi-square tests for categorical variables, with column percentages presented to reflect within-variable distributions across clusters.
Results
Demographic information
A total of 1000 individuals accessed the survey, of whom 950 met eligibility criteria and 20 were excluded (due to incomplete responses, non-Saudi nationality, or failed quality checks), leaving a total of 930 participants who completed the survey and included for analysis. Participant flow diagram is provided in Figure 1. Demographic characteristics for respondents are shown in Table 1. The distribution of gender was balanced with 52.6% men and 47.4% women. The majority were aged between 18 and 44 years (68.2%) and held at least a bachelor's degree (65.2%). Most respondents resided in the three major cities of Riyadh, Jeddah, and Dammam. The distribution of employment status was also balanced with 52.3% employed. The majority of participants had low (<8000 SAR) or middle (8000–14000 SAR) monthly household income (37.7% and 36.6% respectively). Self-rated health was predominantly reported as excellent, very good, or good by participants (31.2%, 29.9%, and 22.6% respectively).

Participant flow chart.
Experience, comfort, and willingness toward telenutrition services
Experience, comfort, and willingness toward telenutrition services is shown in Table 2 and Figure 2. Almost half of the participants had previously tried virtual nutrition services (48.0%) and were currently seeing a dietitian (49.9%). Among those seeing a dietitian, 61.5% reported that the dietitian offered virtual consultations. Among all the responders, only 1.3% were aware of a named virtual nutrition platform. Comfort with virtual services was generally high, with 61.5% indicating they were comfortable or very comfortable using such services, and similar levels were observed for video-based consultations (57.3%). More than half of the participants (54.9%) expressed willingness to follow-up with a dietitian virtually for themselves, while an even greater proportion (78.5%) were willing to arrange virtual care for a family member. Most respondents rated key digital service features as important or very important, including enabling access to medical records (66.1%), prior familiarity with the dietitian (62.5%), and having a dedicated virtual nutrition platform available (66.2%).

Participants’ perceptions of the importance of virtual nutrition service features (n = 930).
Experience, comfort, and willingness toward telenutrition services (N = 930).
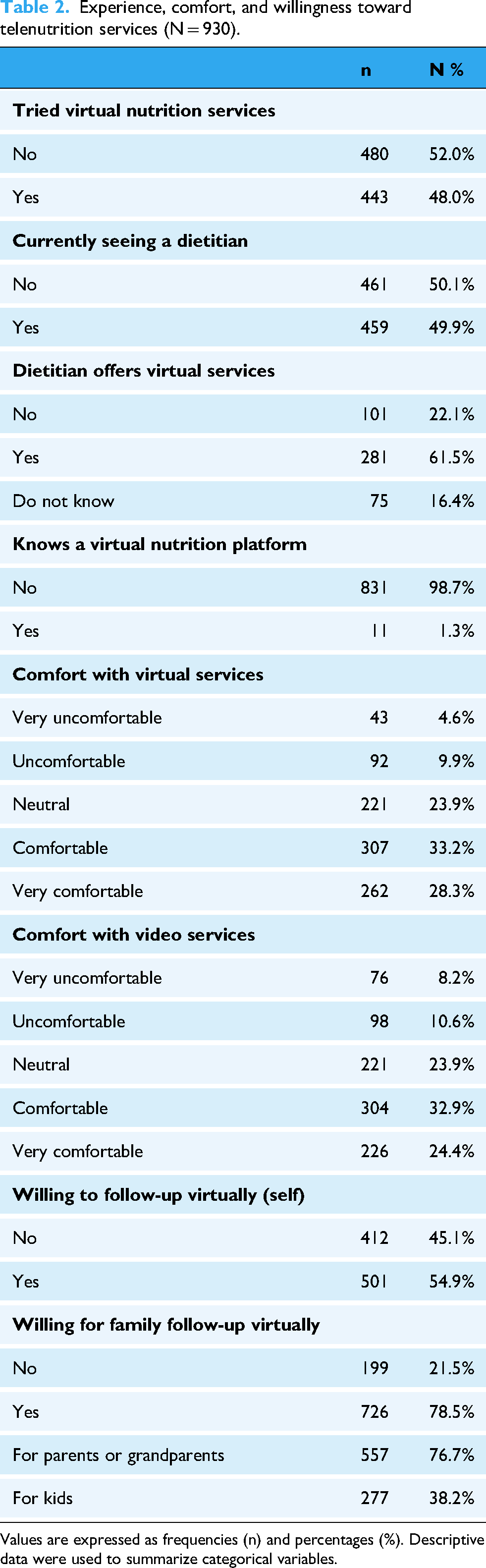
Values are expressed as frequencies (n) and percentages (%). Descriptive data were used to summarize categorical variables.
Participants’ preferences of specialized nutrition counseling for telenutrition services
The preferred uses for telenutrition are shown in Figure 3. More than half of participants (55.8%) selected clinical nutrition consultations for medical conditions as a preferred use of telenutrition. Other commonly preferred services included diet plans for post-bariatric surgery patients (33.8%), individual diet plans for children or infants with allergies or malnutrition (32.8%), and nutrition support for patients using Mounjaro (30.4%). Noting that Mounjaro (tirzepatide) is a dual GIP/GLP-1 receptor agonist delivered as a weekly injection and approved for type 2 diabetes treatment and chronic weight management. Its rapid rise in popularity has contributed to increased public attention toward metabolic health interventions, including virtual nutrition care. Services targeting pregnant or breastfeeding women (29.3%) and laboratory test-linked nutrition recommendations (29.5%) were also frequently selected (Figure 2). Noting that percentages reflect the proportion of participants who selected each service; responses were not mutually exclusive.

Preferences of specialized nutrition counseling for telenutrition services (N = 930).
Factors associated with choosing telenutrition over traditional nutrition counseling services
Regarding factors influencing the choice of telenutrition over in-person consultations, the most reported barrier was being too busy due to work or study commitments (45.6%). Additional commonly selected barriers included transportation or distance challenges (37.2%), family obligations (34.5%), health-related limitations (34.1%), and financial concerns, such as insurance coverage or high consultation costs 33.7%. Nearly one-third (28.6%) cited scheduling difficulties (Figure 4). Only 20.9% of respondents indicated low motivation or lack of perceived need as a barrier. Noting that percentages reflect the proportion of participants who selected each service; responses were not mutually exclusive.
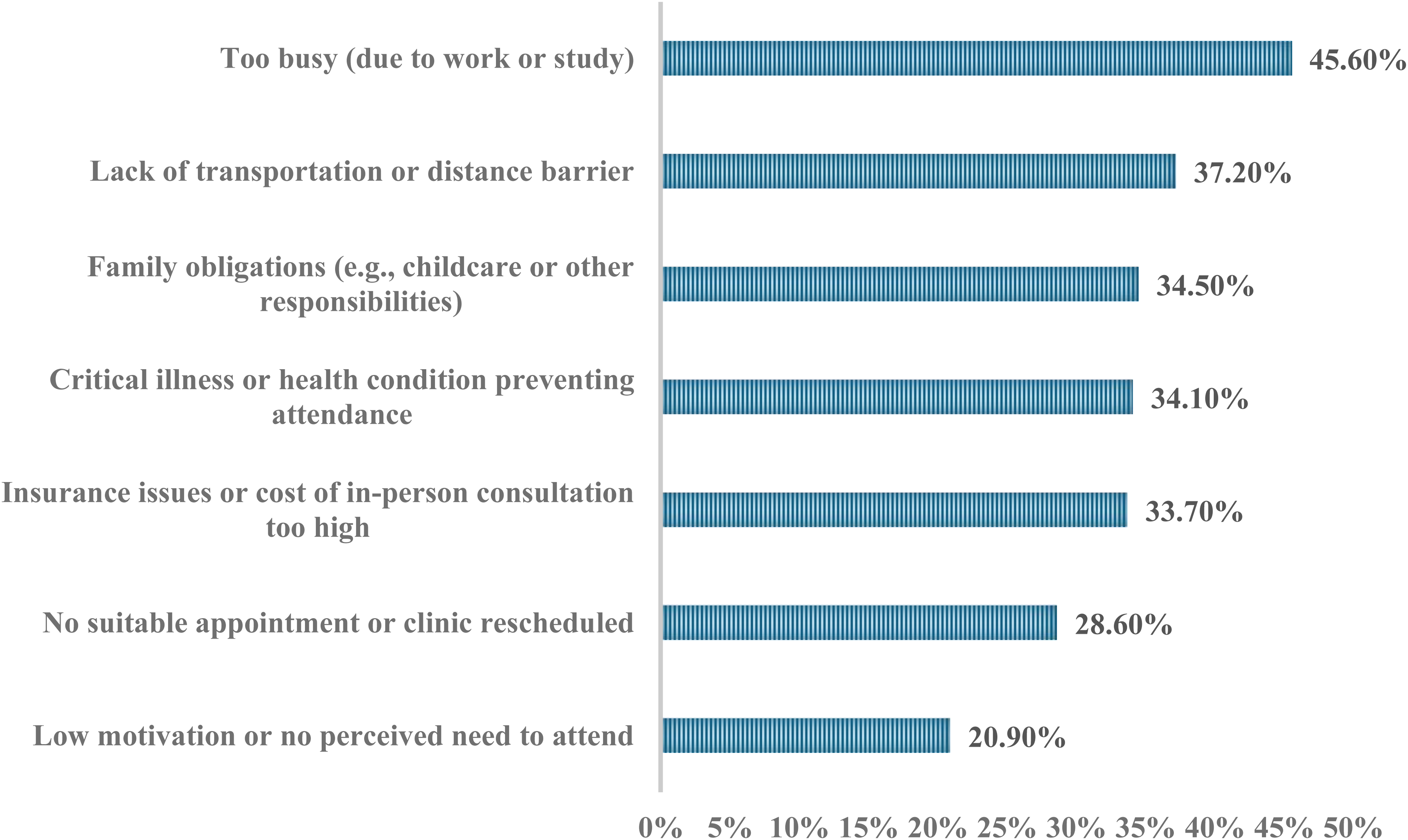
Factors associated with choosing telenutrition over traditional nutrition counseling services (N = 930).
Association between sociodemographic characteristics and willingness to engage in virtual nutrition follow-up
Significant associations were found between willingness to engage in virtual nutrition follow-up and several sociodemographic characteristics. Younger age (χ2 = 40.98, p = 0.006), lower education level (χ2 = 45.05, p = 0.001), being employed (χ2 = 25.38, p < 0.001), and residing in Jeddah (χ2 = 66.23, p < 0.001) were associated with greater willingness to follow-up virtually for their own nutrition service. Similarly, willingness to use virtual follow-up for family was significantly associated with age group, education level, and city of residence (p < 0.05 for all). Gender, marital status, income, and perceived health status were not significantly associated with willingness of using virtual nutrition services (Table 3).
Association between sociodemographic characteristics and willingness to engage in virtual nutrition follow-up (N = 930).

Values are presented as n (%). Percentages represent the proportion of participants within each demographic category who responded “Yes” to willingness for virtual follow-up. Chi-square tests were used to assess associations. Statistically significant results are indicated by p < 0.05 and are shown in bold.
Logistic regression model for predicting willingness to use virtual nutrition services
A binary logistic regression was conducted to examine predictors of participants’ willingness to follow-up with virtual nutrition services (Table 4). The model was statistically significant (χ2 = 239.46, p < 0.001) and explained 32% of the variance (Nagelkerke R2 = 0.320). The model demonstrated good fit (Hosmer-Lemeshow p = 0.074) and correctly classified 70.5% of cases with 73.1% sensitivity and 67.3% specificity at the 0.5 probability cut-off. Greater comfort with virtual services (OR = 1.18, 95% CI: 1.02–1.36, p = 0.028) and video services (OR = 1.39, 95% CI: 1.21–1.60, p < 0.001) significantly increased the odds of willingness for virtual follow-up. Similarly, participants who perceived it as important for dietitians to have access to their health records (OR = 1.20, 95% CI: 1.02–1.42, p = 0.027) and to be familiar with the dietitian beforehand (OR = 1.24, 95% CI: 1.05–1.46, p = 0.011) were significantly more likely to express willingness to use virtual nutrition services. Perceived importance of platform availability showed a borderline effect (OR = 1.18, 95% CI: 1.00–1.39, p = 0.056). Being too busy due to work or study (OR = 1.85, 95% CI: 1.34–2.56, p < 0.001) and having previously used virtual nutrition services increased odds of willingness (OR = 1.52, 95% CI: 1.10–2.10, p = 0.011). Compared to participants with a high school diploma, those with a bachelor's degree (OR = 0.68, 95% CI: 0.47–0.97, p = 0.033) and postgraduate education (OR = 0.42, 95% CI: 0.28–0.64, p < 0.001) were significantly less likely to express willingness. Participants residing in Jeddah were more likely to express willing than those in Riyadh (OR = 2.32, 95% CI: 1.57–3.43, p < 0.001).
Logistic regression model for predicting willingness to use virtual nutrition services (N = 930).

Comfort with virtual services and comfort with video services were treated as ordinal variables (1 = very uncomfortable to 5 = very comfortable). Importance ratings were ordinal (1 = not important to 4 = very important). Barriers and prior experience were binary variables (0 = No, 1 = Yes). Education and city of residence were entered as categorical variables using dummy coding, with High school/diploma and Riyadh as reference categories. Hosmer–Lemeshow test was used to assess model fit. Significant p-values <0.05 are shown in bold.
B: regression coefficient; SE: standard error; OR: odds ratio; CI: confidence interval; p: p-value.
Cluster analysis
The two-step cluster analysis identified three distinct participant profiles based on comfort with virtual services and willingness to follow-up virtually (for self and for family) with a silhouette measure of 0.56, indicating fair-to-good quality and interpretability. These variables were all statistically significant differences across clusters (all p < 0.001; Table 5). The clusters were:
Distribution of clustering variables across identified clusters (N = 907).
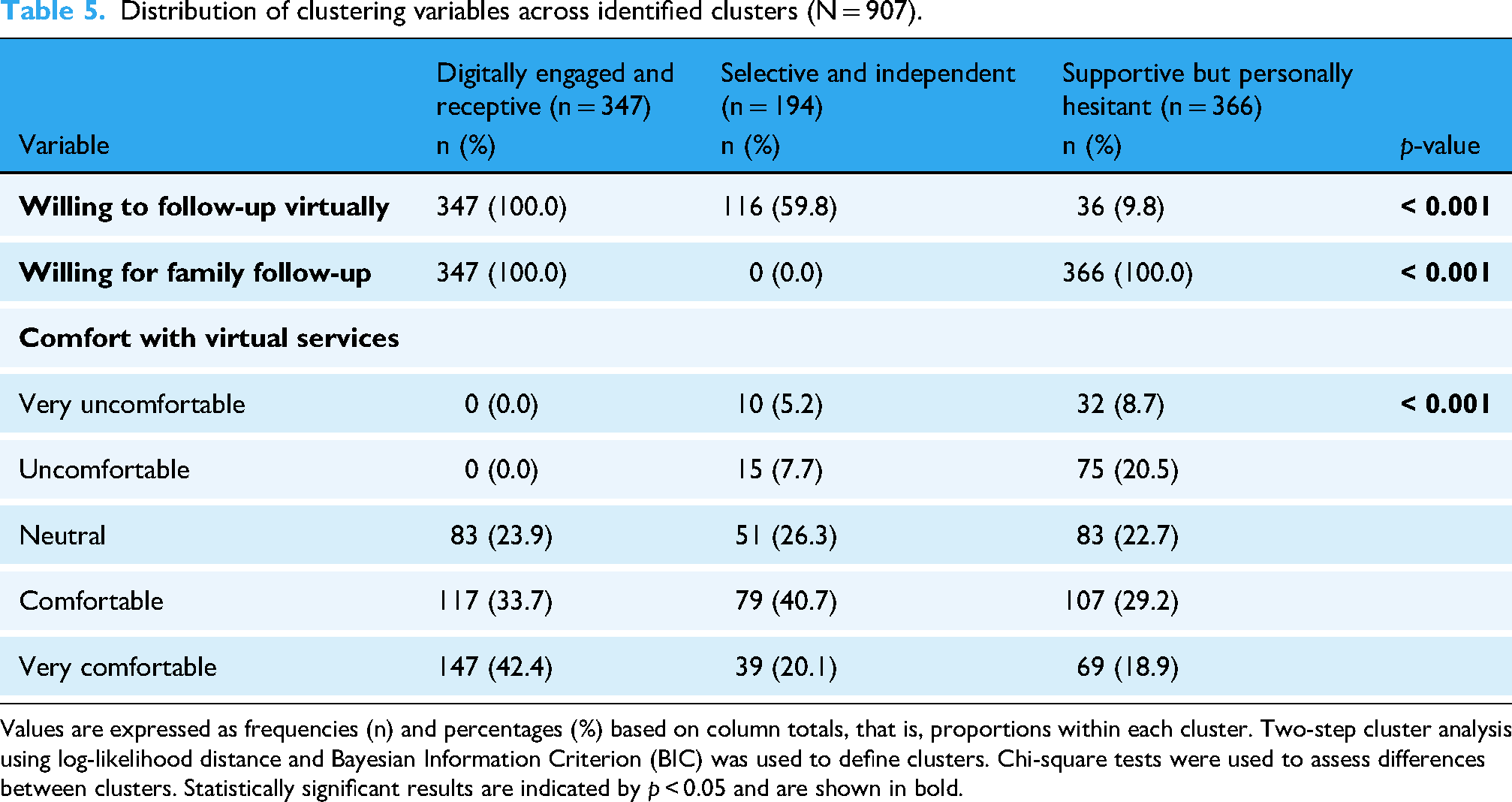
Values are expressed as frequencies (n) and percentages (%) based on column totals, that is, proportions within each cluster. Two-step cluster analysis using log-likelihood distance and Bayesian Information Criterion (BIC) was used to define clusters. Chi-square tests were used to assess differences between clusters. Statistically significant results are indicated by p < 0.05 and are shown in bold.
Cluster 1: Digitally Engaged and Receptive (n = 347):
All participants included in this cluster were willing to follow-up virtually for themselves and their family. A high proportion of them were either comfortable or very comfortable with virtual nutrition services (76.1%).
Cluster 2: Selective and Independent (n = 194):
The majority of participants in this cluster (59.8%) were willing to follow-up for themselves but none for their family. Their comfort with virtual services was generally moderate, with the majority of them (66.4%) rating themselves as neutral or comfortable.
Cluster 3: Supportive but Personally Hesitant (n = 366):
The majority of participants in this cluster (91.2%) were not willing to follow-up for themselves but all of them were willing for family follow-up. The majority of them were reported discomfort or neutrality with virtual nutrition services (52.4%). These differences across clusters were statistically significant (all p < 0.001), indicating meaningful segmentation in readiness and attitude toward telenutrition.
Demographics and experience, comfort, and willingness toward telenutrition services among the three different clusters
Cluster membership was significantly associated with key sociodemographic variables including age group (χ2 = 39.37, p < 0.001), education level (χ2 = 44.86, p < 0.001), employment status (χ2 = 10.62, p = 0.005), marital status (χ2 = 17.04, p = 0.009), city of residence (χ2 = 90.76, p < 0.001), and current health status (χ2 = 44.53, p < 0.001) (Table 6). A total number of 907 were included in this analysis based on complete response across all targeted variables. In addition, the clusters differed significantly in prior experience with virtual nutrition services, comfort with video services, perceived importance of digital features (e.g. platform availability, access to health records), and various in-person service barriers (all p < 0.05; Table 7).
The Digitally Engaged and Receptive group were more likely to be younger (38.0% aged 18–29 and less than 25% were over 45 years), employed (57.5%), hold a bachelor's degree (41.5%) and to have an excellent (40.3%) or very good (28.8%) health. The majority of them expressed comfort with video-based services (66.8%), had previous experience with virtual nutrition services (56.2%), and were currently seeing a dietitian (55.1%). Common reasons for considering virtual services included being too busy (54.5%) and facing transportation barriers (44.1%). The Selective and Independent group were slightly older (around 30% were over 45 years) with a higher proportion residing in Jeddah (54.1%). They showed a slightly lower level of comfort with virtual services as 40.7% reported feeling comfortable and 20.1% very comfortable. They also had a slightly lower engagement with virtual care, with nearly half having prior experience (49.7%) and 54.2% currently seeing a dietitian. Their main reason for considering virtual care was being too busy (55.5%) followed by cost or insurance-related barriers (40.8%). The Supportive but Personally Hesitant group tended to be older, with around 40% over the age of 45, around the third of them were divorced or widowed and more than half were unemployed (54.3%). This group also had the highest proportion of postgraduate qualifications (32.2%) and the lowest rates of current engagement with virtual services as only 39.5% had tried virtual care. The common reasons to consider virtual nutrition care among them were transportation (33.8%) and cost (36.0%).
Participant demographics by cluster (n = 907).

Values are expressed as frequencies (n) and percentages (%) based on column totals, that is, proportions within each cluster. Chi-square tests were used to assess differences between clusters. Statistically significant results are indicated by p < 0.05 and are shown in bold.
Telenutrition preferences and experiences by cluster (n = 907).
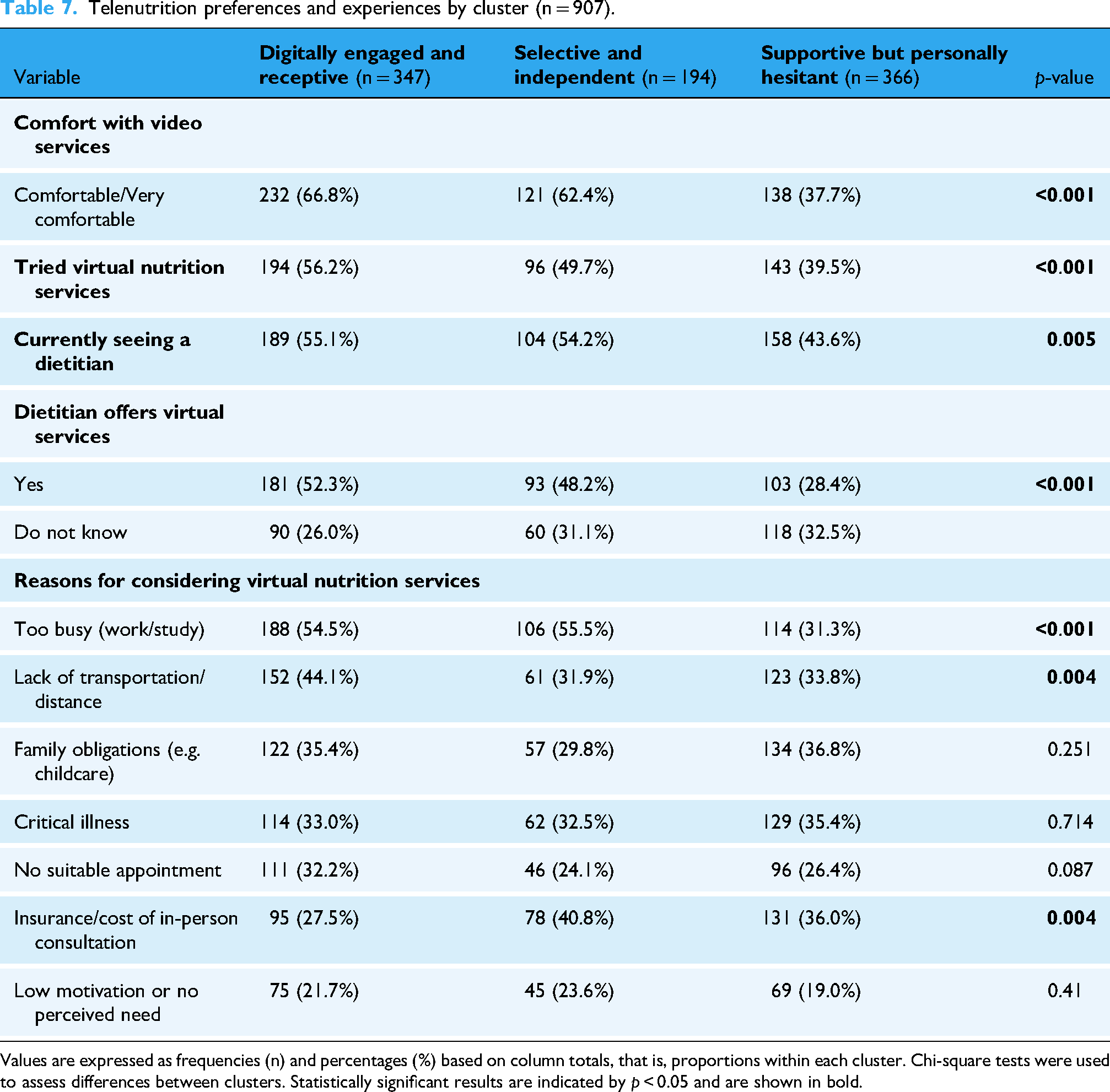
Values are expressed as frequencies (n) and percentages (%) based on column totals, that is, proportions within each cluster. Chi-square tests were used to assess differences between clusters. Statistically significant results are indicated by p < 0.05 and are shown in bold.
Discussion
This nationally representative survey provided a critical insight into previous experience, comfort, willingness, and preference of using DTC telenutrition services among Saudi population. One of the most significant findings is the relatively high receptiveness to virtual dietetic care, with more than half of the participants indicating comfort and willingness to engage in nutrition care services and follow-up via digital platforms. The significance of these results aligns with Saudi Arabia's broader health transformation to digital health under Vision 2030 and its implications for improving access to nutrition services in Saudi Arabia. 7 Using the same survey tool, Welch et al. (2017) findings showed that 52% of the U.S population were also willing and 53% were comfortable seeing their own provider via telemedicine. 26 Our study has confirmed similar logistical enables such as access to personal medical record and having the same dietitian significantly increased willingness to use telenutrition. The analysis of comfort to use telenutrition showed that both general and video-based virtual care are considered strong facilitators of user experience in digital health engagement. These findings agree with previous studies that emphasized on trust and convenience as key determinants of digital health adoption and confirm relevance within the Saudi culture.3,5,26 While our study did not specifically quantify previous telehealth usage, the relatively high levels of comfort and willingness suggest increase normalization of virtual dietetic care. In contrast, Welch et al. (2017) reported very low utilization (3.5%), reflecting the early-stage exposure of the U.S at that time prior to COVID-19 periods. Indeed, COVID-19 pandemic has introduced telehealth showing a significant increase in telehealth adoption among dietitians, with 78% providing virtual care compared to 37% pre-pandemic. 30 Studies have shown that most patients were comfortable with different virtual care platforms, including phone and video consultations, with higher comfort with phone consultations in comparison to video call consultation, which is also seen in our previous pilot study. 13 This may be due to culture impact and lack of awareness. Previous studies have shown effective virtual nutrition care interventions in several specialties such as obese, 18 cardiac rehabilitation, 27 oncology, 31 liver, 32 renal, 33 cardiovascular and diabetic patients. 34 In the present study, participant preferences for specialized virtual services were explored, with 55% favoring clinical nutrition care and 20–33% indicating interest in bariatric, pediatric, and pregnancy related support. Whereas in our previous pilot study carried on dietitians, most of referrals for telenutrition services (n = 35; 32.4%) were covering referrals for weight loss/weight maintenance. 13 Thus, it is crucial that telenutrition platforms accommodate participants’ preference for specialized virtual services, even if they differ from commonly practiced approaches.
Understanding participants demographics of virtual care users is crucial to address barriers and challenges in order to develop and/or improve digital nutrition services accessibility.30,35 In 2021, it was revealed that older adults and rural residents are less likely to use video-base telehealth care services. 36 Additionally, low-income individuals and those with poor health also reported lower comfort levels with virtual care. 37 Current findings confirmed variations in responses across demographic groups, where younger individuals, who are employed and living in Jeddah were more likely to adopt virtual nutrition care, whereas higher education levels, particularly postgraduates were associated with lower willingness. This inverse relationship may reflect those with age, high expectations and awareness of clinical standards and data security, which requires further investigations. In comparison to Welch et al. (2017), no significant associations were seen among highly educated populations, 26 whereas other studies were aligned with the present outcomes, showing that older adults showed low readiness due to lack of resources and training. 38 Yet, rural communities demonstrated varying degree of readiness for telehealth implementation due to factors associated with awareness influencing success, 39 urban residence and internet accessibility. 40 In our study, drivers to adopt telenutrition services, were identified as work/study constraints (45.6%), transport difficulties (37.2%), and family or health obligations (34%). These findings reinforce the unitality of DTC nutrition care services in improving accessibility for mobility limited populations.
A cluster analysis was further conducted in the present study, which clarified the segmentation of users. Cluster 1 (n = 347) was the largest group and was identified as the “Digitally Engaged and Receptive” cluster, which represents a key demographic for scaling telenutrition services due to their high readiness and engagement. Cluster 2 (n = 194) was identified as the “Selective but Personally Hesitant” group, characterized largely by older and less educated individuals. Cluster 3 (n = 366) was identified as the “Supportive but Personally Hesitant” group. Although open to virtual care for family members, they showed reluctance to use it for themselves and may benefit from targeted awareness efforts and gradual exposure to telehealth tools. In alignment with our cluster analysis, a 2016 study reported that overall motivation and attitudes toward telemedicine, particularly among older adults and their caregivers were unsatisfactory 41 ; however, clustering approaches were not conducted in Welch et al.'s study. 26 These findings add depth into understanding user segmentation, reinforcing the importance of customizing telenutrition strategies to patient subgroups. Thus, patient motivation to adopt telenutrition services is a crucial factor for a successful implementation of virtual nutrition care services. In the year 2024, Eid et al. confirmed that combining monthly health coaching and weekly telemonitoring to telenutrition weight loss programs, have shown higher retention, responsiveness, and less dropouts in comparison to those following only virtual care service. 24 Indeed, integrating virtual nutrition care process 2 demonstrated an improvement in service accessibility and patients’ motivation. The most powerful component was integrating health coaching sessions and weekly monitoring through cloud-based platforms for sustainable dietary improvements and enhanced patient follow-up.18,42 Yet, only 1.3% of participants identified a specific virtual nutrition platform, suggesting that entrepreneurs and policymakers should tailor their strategies not only by age or education, but also by users’ motivational profile and specialized services. Digital behavioral assessments, such as those applied by Arslan et al. in esports populations highlight the potential for telenutrition platforms to monitor niche eating patterns like night eating or compulsive food behaviors, which could be applied to the clusters identified in our analysis. 43
Our findings highlight an opportunity for the Saudi Ministry of Health to integrate structured telenutrition services into primary healthcare pathways through Sehhaty and other digital platforms, accompanied by national awareness campaigns to increase recognition and uptake. To our knowledge, this is the first study to adapt, translate and validate a U.S.-based national telemedicine survey specifically for the Saudi context, focusing on DTC telenutrition. A large, demographically stratified sample was investigated, where novel insights into Saudi adults’ perspectives on telenutrition, including acceptance drivers and comfort with virtual dietetic care offering a uniquely detailed analysis of demographics trends and motivational segmentation that was not previously explored in the literature. In addition, the nature of the study design limits our findings, where cross-sectional and self-reported data may have exhibited bias and causalities, in particularly with questions related to comfort and willingness. Because sampling captured major regions and demographic strata, findings are generalizable to urban Saudi adults, but rural populations may be underrepresented. Future approaches must take into account food insecurity and limited access to healthy foods, which have been shown to influence sustainable eating behaviors and readiness for remote nutrition services.44,45 Incorporating equity-based determinants may help explain variations in comfort and willingness observed across demographic groups. This study focused on demographic predictors, but additional factors such as personality traits and social influence have been shown to influence digital health adoption. These constructs should be considered in future Saudi-specific models to guide targeted policy and awareness strategies.
Interestingly, current approaches are exploring integrating artificial intelligence (AI) in telenutrition platforms. Giasanti (2024) provided a high level overview of the digital health evolution, identifying AI, mobile apps, and virtual reality (VR) as transformative tools, but digital literacy still remains a significant barrier. 46 In alignment with these findings, Zhang's bibliometric review of 2860 studies on machine learning and telemedicine showed that ChatGPT's emergence in 2023 signaling caused a significant shift towards generative AI in telehealth. 47 Focusing on the nutrition context, recent studies by Sosa et al. 48 and O’Hara et al. 49 highlighted AI's strong performance in dietary assessment, particularly with image recognition and meal planning. Sosa's scoping review confirmed that AI applications target dietary analysis, with emerging interest in malnutrition and obesity management. Yet, O’Hara's evaluation of ChatGPT-4 exposed significant accuracy limitations, in particularly with nutrient estimation and portion size recognition, where human dietitians input is a necessity. Recent work by Arslan (2024) emphasizes the growing role of AI conversational agents, such as ChatGPT, in nutrition counseling and public information delivery. Integrating these tools within virtual nutrition platforms may enhance engagement but requires careful evaluation of accuracy, safety, and cultural relevance. 50 At the time of data collection, Saudi Arabia did not have widely known, dedicated DTC telenutrition platforms. Most virtual nutrition consultations were offered through general telehealth applications such as Sehhaty or through independent dietitians using private digital channels such as Zoom. Because these services are not branded as specialized telenutrition platforms, users may not remember or associate them with a specific name. This likely explains why fewer than 2% of participants could identify a named platform despite nearly half reporting prior experience with virtual nutrition services. Therefore, longitudinal and intervention studies are recommended to track the adoption and effectiveness of newly developed platforms on long-term behavior change and health outcomes, including verification of the sustained influence of specific sociodemographic predictors on telenutrition engagement.
Conclusions
In conclusion, this nationwide study provides the first population-level evidence on Saudi adults’ awareness, comfort, and willingness to engage with DTC telenutrition. Despite high digital penetration in the Kingdom, a substantial proportion of participants demonstrated low awareness of existing virtual nutrition services, and fewer than 2% were able to name a specific platform. Willingness to use telenutrition was shaped primarily by age, prior virtual-care experience, employment status, and perceptions of convenience and accessibility, underscoring the need for tailored outreach strategies. These findings highlight important demographic and behavioral mechanisms that can guide early-stage market positioning and inform national implementation priorities. Given Saudi Arabia's ongoing digital health transformation, telenutrition platforms, particularly when integrated with AI-enabled tools, which represent promising avenues to expand access to dietetic care, enhance patient engagement, and address growing nutrition-related health challenges. Strategic investments in public awareness campaigns, integration into existing national digital platforms (e.g. Sehhaty), and capacity-building initiatives for dietitians will be essential to enhance adoption and equitable use. Continued research, including longitudinal and intervention studies, is recommended to validate the long-term behavioral and health impacts of telenutrition and to track the evolving influence of sociodemographic predictors on engagement over time.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076261419237 - Supplemental material for Digital health adoption in nutrition care: A national cross-sectional, Arabic-validated survey and cluster analysis of patient experience and willingness to use telenutrition in Saudi Arabia
Supplemental material, sj-pdf-1-dhj-10.1177_20552076261419237 for Digital health adoption in nutrition care: A national cross-sectional, Arabic-validated survey and cluster analysis of patient experience and willingness to use telenutrition in Saudi Arabia by Noura MS Eid in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076261419237 - Supplemental material for Digital health adoption in nutrition care: A national cross-sectional, Arabic-validated survey and cluster analysis of patient experience and willingness to use telenutrition in Saudi Arabia
Supplemental material, sj-pdf-2-dhj-10.1177_20552076261419237 for Digital health adoption in nutrition care: A national cross-sectional, Arabic-validated survey and cluster analysis of patient experience and willingness to use telenutrition in Saudi Arabia by Noura MS Eid in DIGITAL HEALTH
Footnotes
Abbreviations
The following abbreviations are used in this manuscript:
Acknowledgements
The author acknowledges DSR with thanks for technical and financial support.
Ethical approval
Ethical approval and participants consent was carried in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of The Research Ethics Committee (REC) at the Unit of Biomedical Ethics, Faculty of Medicine at King Abdul-Aziz University, Jeddah, Saudi Arabia (NCBE Registration No: Reference No 195-25). Date: Sunday, May 11, 2025.
Informed consent
Informed consent was obtained from all subjects involved in this study.
Author contribution
Noura MS Eid: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing—original draft preparation, writing—review and editing. Noura MS Eid has read and agreed to the published version of the manuscript.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Deanship of Scientific Research (DSR) at King Abdulaziz University, Jeddah, Saudi Arabia under grant no. (IPP: 110-290-2025). The author, therefore, acknowledge with thanks DSR for technical and financial support.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data presented in this study are available upon reasonable request from the corresponding author at ooaeid2@kau.edu.sa.
Guarantor
Noura M.S. Eid is the guarantor of this work and accepts full responsibility for the integrity of the data, the accuracy of the analysis, and the content of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.