
Abstract
Objective
As China faces digitization and aging, despite efforts to improve older adults’ digital health literacy across domains, research lacks examination of the impact of intergenerational back-feeding. This study aims to investigate the effects of intergenerational back-feeding, defined as the transfer of digital knowledge from younger to older generations, on digital health literacy among older adults.
Methods
Semi-structured interviews were conducted with 20 adults aged ≥60 years from three provinces in China. Thematic analysis was guided by the three-stage back-feeding model (access, skills, literacy) and key individual factors (e.g. perceived usefulness and perceived ease of use).
Results
The enhancement of digital health literacy among older adults was shaped by a dynamic interplay between individual factors and intergenerational back-feeding. At the access stage, although younger generations frequently provided digital health devices, interface complexity or a preference for traditional care led some older adults to discontinue use. Skill development was significantly influenced by teaching methods: heuristic and face-to-face guidance improved operational competence, whereas remote, proxy, and directive approaches fostered dependency. At the literacy stage, some younger generations’ risk-averse strategies limited older adults’ autonomy, while only a minority proactively engaged in cross-verifying online health information with offline sources.
Conclusion
This study extended the three-stage back-feeding model to health contexts by incorporating individual factors. These findings confirmed the pivotal role of intergenerational back-feeding in enhancing the digital health literacy of older adults in China. Future efforts should integrate family support with national-level policy implementation, which is significant for advancing healthy aging.
Introduction
By the end of 2024, China's population of older persons aged 60 and above have reached 310 million, which is 22% of the total population, entering a profoundly aging society. 1 In recent years, the World Health Organization has proposed a framework for healthy aging that emphasizes promoting diversity and reducing inequities. While digital technology is transforming healthcare through innovations, such as telemedicine and wearable devices, it also has the potential to exacerbate existing inequalities.2,3 Digital technology is recognized as a pivotal catalyst for health transformation. This is evident in its direct application within health systems, as well as in self-monitoring of health status and behaviors, and indirectly through its impact on social and environmental health determinants. 4 Digital technology has been regarded as a new determinant of health in recent years, solidifying its role as a digital determinant of health.5,6 Central to the digital determinant of health is digital health literacy, defined as the ability to access, evaluate, and apply digital health resources. It is crucial to acknowledge that it has also exerted a direct influence on the healthy autonomy, social participation, and psychological security of older adults. 7 Although the number of older Internet users in China has increased significantly, the overall level of digital health literacy still lags behind the pace of technological development. 8 The low level of digital health literacy results in technology-related dilemmas for older adults, such as difficulty in effectively accessing authoritative health information and the inability to utilize smart health devices for self-management fully.9–11 Furthermore, the advent of the COVID-19 pandemic further exposed systemic vulnerabilities, as limited digital health literacy hindered older adults’ access to remote health services and credible information.12,13
To address this, China has introduced corresponding policies at the national level to promote healthcare and digital health literacy for older adults. For example, the State Council of China has issued relevant documents mandating the integration of smart devices into the care of older adults. 14 In alignment with the national digital inclusion policy, a range of district institutions, including community centers and nursing homes, have implemented training programs aimed at enhancing digital literacy among older adults. 15 However, despite various social programs aimed at fostering digital health literacy among older adults, numerous challenges remain. These challenges encompass the complexities associated with implementing training programs, low participation rates among older adults, and the geographical distance between community institutions and older adults. 16 Therefore, family support has become a key compensatory mechanism and the primary pathway for improving digital health literacy among older adults. 17 The term “family support” refers to the wide range of assistance provided by family members to one another, including financial support, daily care, and emotional support. 18
In the contemporary digital era, younger family members are pivotal in facilitating digital integration in older generations. 19 Specifically, the younger generations (children and grandchildren) are familiar with the Internet and digital technology and pass on their knowledge and skills to the older generations (parents and grandparents). This intergenerational transfer process is referred to in academia as “intergenerational back-feeding” or “digital back-feeding.”20,21 Nevertheless, an obvious distinction emerges when contrasting intergenerational back-feeding with digital mentoring, a practice employed by IT experts and other technical personnel to assist users with specific technical issues. 22 The former approach provides a distinct intergenerational family perspective. Significantly, the family is the main domain in which intergenerational back-feeding occurs. This transfer process offers both technical and emotional support to older adults, underscoring the crucial role of family support in enhancing their self-esteem and promoting healthy lifestyles, including stress management and physical activity.23,24 The concept of intergenerational back-feeding is rooted in Mead's prefigurative culture theory, which posits that technological revolutions invert traditional knowledge transfer (e.g. cultural transmission is predominantly from the older to the younger members of a society). 25 Zhou provided a foundational contextualization of this theoretical framework within the specific sociocultural context of China, defining back-feeding as the transfer of digital skills and cultural cognition from youth to older adults. 26 This transfer was further operationalized into a three-stage model: The first stage was defined as “access back-feeding.” This stage reduced technological thresholds by providing devices such as smartphones and health monitors to solve physical access barriers. The second stage was designated as “skills back-feeding.” This stage involved teaching operational competencies to address cross-functional usage gaps. The third stage was designated as “literacy back-feeding.” This stage involved cultivating critical information evaluation skills to enable knowledge internalization and innovation. 27
Intergenerational back-feeding is prevalent in Chinese families, and China promotes digital health literacy among older adults through smart-care policies. Despite efforts across domains to improve digital health literacy of older adults in China, research remains lacking in the examination of intergenerational back-feeding's impact on this aspect. 20 This study integrates the three-stage back-feeding model within the health context, considering individual factors to systematically analyze the factors influencing intergenerational back-feeding on older adults’ digital health literacy. Through semi-structured interviews, 20 adults aged 60 years and above participated in this study. This study aimed to enhance the digital health literacy of older adults, thereby improving their overall quality of life. This advancement has significant implications for promoting the sustainability of healthy aging in China.
Methods
Study design and setting
This study employed a qualitative descriptive design to explore the impact of intergenerational back-feeding on digital health literacy among older adults, adhering to the Consolidated Criteria for Reporting Qualitative Research guidelines. 28 The design was chosen to explore in depth how participants perceive, experience, and are challenged by learning to use digital health technologies, particularly with the support of younger family members.
This study incorporated individual factors that influence digital health literacy among older adults into the interview outline, including sociodemographic characteristics (gender, age, education, and living arrangements), self-rated health, self-efficacy, perceived usefulness, and perceived ease of use. 29 Self-rated health was assessed by asking participants about their perceptions of their own health. Specifically, they were asked, “How would you describe your current health status?” with response options such as “good,” “fair,” and “poor.” Self-efficacy is defined as the confidence in one's own ability to learn, operate, and troubleshoot digital health technologies. 30 This factor was evaluated based on the measuring general self-efficacy beliefs by asking participants: “If you encounter issues while using digital health devices or services, what do you think about your problem-solving skills?” 31 with response options such as “strong” or “weak.” Perceived usefulness and perceived ease of use were assessed by asking participants about their perceptions of using digital health devices or services. For example, they were asked, “Do you find them useful? Were there any difficulties during use?” 32 In this study, digital health devices were not limited to specialized health monitoring devices (e.g. blood glucose meters, blood pressure monitors, and smart bracelets). It also extends to smart devices such as smartphones and internet-connected televisions that can be used in daily healthcare.
The selection of these study sites prioritized environments with highly representative samples, which ensured theoretical transferability through maximal diversity. 33 This was achieved by selecting different provinces to capture socioeconomic and digital disparities in China. Jiangsu province has a mature digital health infrastructure and high Internet penetration, enabling the observation of advanced digital health literacy development. 34 Gansu province provides a critical comparative context as a developing region in which national policy interventions actively improve digital accessibility. 35 Therefore, the provinces of Jiangsu and Gansu were the main research sites for this study. Furthermore, Jilin Province, characterized by its moderate level of economic development and Internet penetration rate, was selected as an additional sample site in this study.34–36
Participants
Guided by grounded theory, 37 the theoretical purposive samplings were employed. Following the age criteria stipulated by Chinese law on the protection of older adults’ rights and interests, 38 this study purposively selected a sample of 20 individuals aged 60 years and above, comprising 10 females and 10 males. Other inclusion criteria included (1) possession of a good status of cognitive ability, (2) capability to engage in interviews conducted in Mandarin, and (3) residence in environments equipped with basic digital health infrastructure. All participants were invited to take part voluntarily, and no relationship was established prior to the commencement of the study. The number of participants was chosen based on the principle of achieving information saturation during the interviews. This research approach has been grounded in previous qualitative studies. 39
Data collection
Data were collected through semi-structured interviews using a guide that was developed based on the study's theoretical framework (see Supplementary Material 1). The guide was piloted with three older adults to assess question clarity and comprehension, and subsequently refined through consultations with gerontology experts.
Four interviewers, comprising both undergraduate and postgraduate students, conducted the interviews. All had received prior training in qualitative research methods and social fieldwork procedures. Participants were interviewed face-to-face in familiar sites such as local parks or community centers, with each interview lasting between 30 and 40 minutes. All interviews were audio-recorded using smartphones to ensure data accuracy and reliability.
Thematic saturation was methodically assessed throughout the data collection process. After 18 interviews, the analysis indicated that no new themes were emerging. To rigorously confirm that saturation was achieved, two additional interviews were conducted. These final interviews served to refine and solidify the boundaries of the existing themes, with no new interpretations, contexts, or dimensions identified. Therefore, the data obtained in this study reached saturation, consistent with established qualitative research standards. 39
Data analysis
This study employed a combined inductive and deductive thematic analysis approach, strictly adhering to Braun and Clarke's six-phase framework for analysis. 40 Initially, the analysis was used a deductive approach, guided by (1) the three-stage back-feeding model, 27 which pre-defined the overarching themes of access, skills, and literacy back-feeding; (2) Mead's prefigurative culture theory, 25 which directed this study's attention to dynamics of knowledge reversal and intergenerational relationships; (3) the technology acceptance model and relevant research results,32,41 which pre-defined individual factors including in the interview guide, such as “self-rated health,” “perceived usefulness,” and “perceived ease of use.” In parallel, an inductive analysis was conducted on the data to capture emergent themes. The primary data analysis was performed by J.S., a senior master's student in sociology with formal training in qualitative research methods. This process involved three complete cycles of reading, sorting, and coding the transcripts, which initially generated 44 distinct codes. The analysis was then critically reviewed by L.Y., a postdoctoral researcher in gerontology and medical health. In this peer debriefing process, L.Y. challenged interpretations, suggested alternative groupings, and audited the consistency of the coding framework.
The analytical rigor was ensured through three rounds of reflective discussion and reconciliation between the codes. First, the researchers compared the initial 44 codes. Discussions focused on reconciling differing code labels, consolidating overlapping concepts, and explicitly tagging each code as either deductive or inductive in origin. Second, the focus shifted to grouping codes into meaningful sub-themes and refining their definitions. A key development in this stage was the conceptual evolution of an inductive code from “learning cognition” to the more robust and theoretically grounded construct of “self-efficacy.” Third, the final discussion centered on the overarching thematic structure. To enhance conceptual clarity and align with the core theoretical model, the “individual factors” were maintained as a distinct theme, while the “intergenerational back-feeding” factors were divided into the three discrete, deductive-informed stages of access, skills, and literacy. This process culminated in the final framework of three main themes and 12 sub-themes. Any disagreements in coding or thematic construction were resolved through consensus-reaching discussions between the two authors. In cases where consensus could not be immediately reached, the codes and supporting transcripts were revisited jointly until an agreement was achieved.
A complete codebook detailing all themes, their origins (deductive or inductive), their definitions, and illustrative quotations is available in Supplementary Material 1. As noted in the Data Collection section, thematic saturation was confirmed after 20 interviews. The analytical process ensured that the identified themes comprehensively represented the participants’ experiences.
Ethics
This study was approved by the Research Ethics Committee of Nanjing University of Posts and Telecommunications (Approval No. IRB-2022KYNCS003). All participants provided written informed consent after receiving detailed explanations of the study purpose, procedures, risks, and benefits.
Results
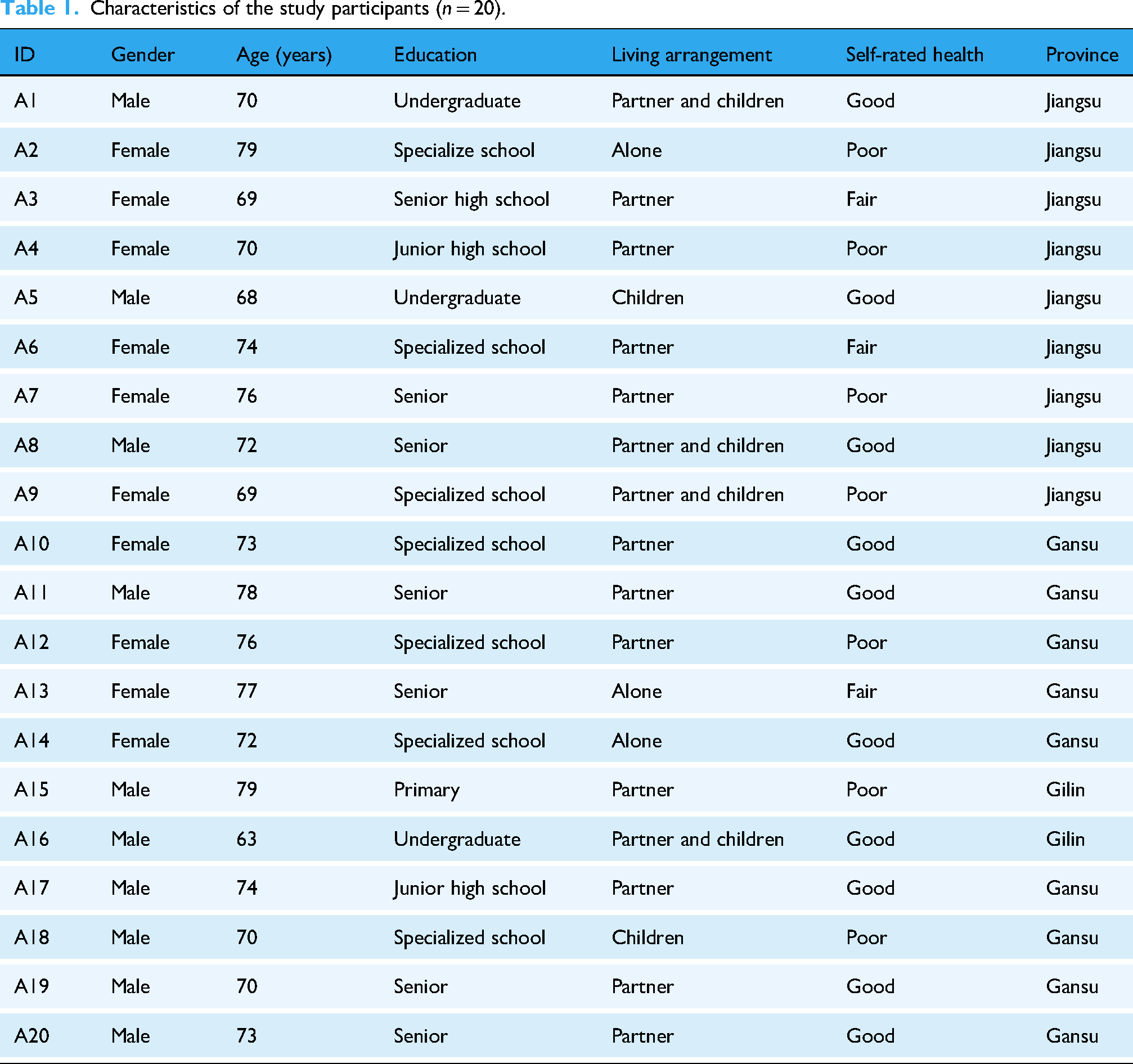
In this study, 20 older adults were interviewed (10 females and 10 males), with an age range of 63–79 years. Their educational backgrounds included primary school, junior high school, senior high school, specialized school, and undergraduate. Six lived with their partners and children, 11 lived with their partners only, and three lived alone. Table 1 describes the characteristics of the participants.
Characteristics of the study participants (n = 20).
The thematic analysis finally developed a comprehensive framework consisting of four main themes and 12 sub-themes. It detailed the complex interplay between individual factors and intergenerational back-feeding in shaping older adults’ digital health literacy (Table 2).
Overview of themes and subthemes (four main themes, 12 sub-themes).

Analysis of the factors influencing intergenerational back-feeding on digital health literacy of participants revealed several key findings. All 20 participants contributed to discussions on perceived ease of use, communication medium access, and back-feeding content, establishing these as central concerns. However, only six participants reported actual ownership of dedicated digital health devices, indicating a notable gap between device access and functional adoption. Meanwhile, sub-themes such as self-rated health and perceived usefulness engaged the majority of participants, reflecting their widespread relevance. Notably, several sub-themes demonstrated substantial analytical significance despite lower participant numbers. Age perception, discussed by only two participants, generated seven distinct statements offering deep insights into this psychological barrier. Similarly, digital health device access and back-feeding manners provided rich, nuanced data for understanding implementation challenges. The complete distribution of participants mentioned for each theme is detailed in Table 3.
Frequency of statements and the number of participants mentioning each theme.

Individual factors
Age perception
Age perception was determined by inferences based on how participants talked about their ages during the interviews. While only two of the 20 participants explicitly expressed a sense of age misalignment with digital health technologies, their accounts revealed a profound influence on technology adoption. These participants consistently viewed themselves as beyond the target demographic, which led to a clear pattern of technological disengagement. This manifested as a self-imposed exclusion, with one participant stating, “I think such tools are more suitable for younger adults” (A6), or a complete dismissal of relevance, as another asserted, “I’m so old, how could I manage those things?” (A15). Despite its limited explicit mention, this perception fundamentally hindered their willingness to accept and use digital health devices provided by younger generations, underscoring its role as a meaningful, qualitative barrier in the context of intergenerational back-feeding.
Self-rated health
In this study, self-rated health significantly influenced how older adults engaged with digital health technologies. Among the 16 participants who discussed this theme (Table 4), three distinct patterns emerged based on their perceptions of health. Eight participants with good self-rated health proactively used digital tools for prevention and monitoring. For instance, in addition to reading books, participants used TVs, smartphones, and other digital devices to access health information, as well as smart health devices to monitor their health. Those with fair self-rated health recognized technology's value but cited skill limitations, with one wishing for “smartphone tutoring classes” (A13). Some participants with poor self-rated health demonstrated the most targeted use of technology. Specific health challenges, including osteoporosis and hypertension, motivated this active engagement with digital health technology even when their digital skills were limited.
Thematic distribution of self-rated health.
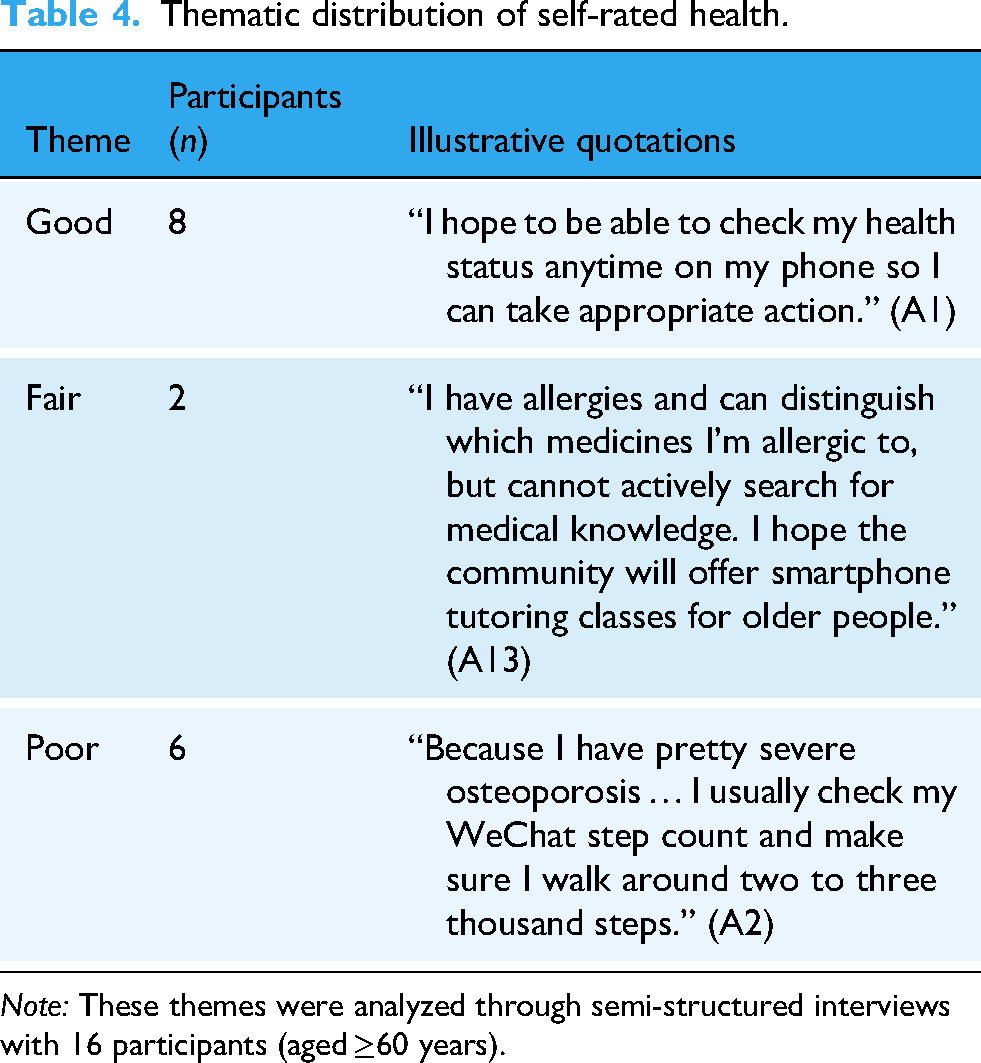
Note: These themes were analyzed through semi-structured interviews with 16 participants (aged ≥60 years).
Self-efficacy
The study identified self-efficacy as a pivotal factor in older adults’ engagement with digital health technologies. Among 14 participants who discussed this theme (Table 5), four participants with strong self-efficacy expressed confidence in their ability to acquire new digital health skills. As one participant noted, “Now that I’m retired and have more time on my hands, I find that I grasp quickly when taught” (A16), reflecting a proactive approach to learning often connected to retirement activities. In contrast, 10 participants reported substantial learning difficulties, primarily due to age-related cognitive decline. While some expressed limited interest in using digital devices, stating “we have little interest in using our smartphones” (A4), other participants were motivated to learn to avoid becoming a burden on their children, with one participant expressing, “I wish I could go to one (e.g. smartphone learning classes), I do not want to bother my son” (A7).
Thematic distribution of self-efficacy.
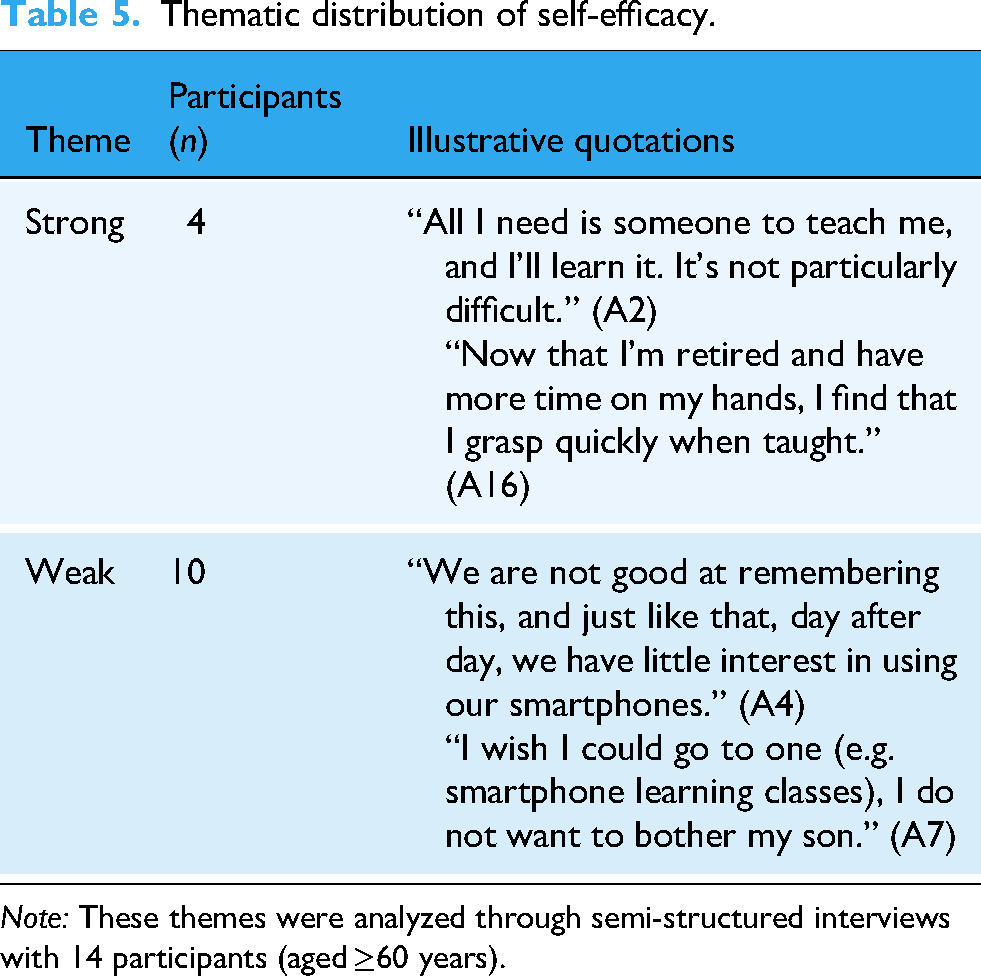
Note: These themes were analyzed through semi-structured interviews with 14 participants (aged ≥60 years).
Perceived usefulness
In this study, perceived usefulness emerged as a significant theme during the interviews, revealing three distinct patterns among the 16 participants who discussed this theme (Table 6). Eight participants demonstrating active engagement recognized clear benefits in digital health devices, with one noting, “This blood pressure meter and blood glucose meter are really quite convenient” (A3). Those showing passive engagement acknowledged potential benefits but remained skeptical, as expressed by one who stated, “I don’t find it very reliable, so I don’t use it often” (A7). Meanwhile, six participants in disengagement completely dismissed the technology's value, preferring a traditional alternative. For example, one participant mentioned, “Modern devices are overly advanced. Our feature phones are far more convenient” (A18). In this study, “feature phones” refer to mobile devices with only basic functionalities, such as texting and telephoning.
Thematic distribution of perceived usefulness.
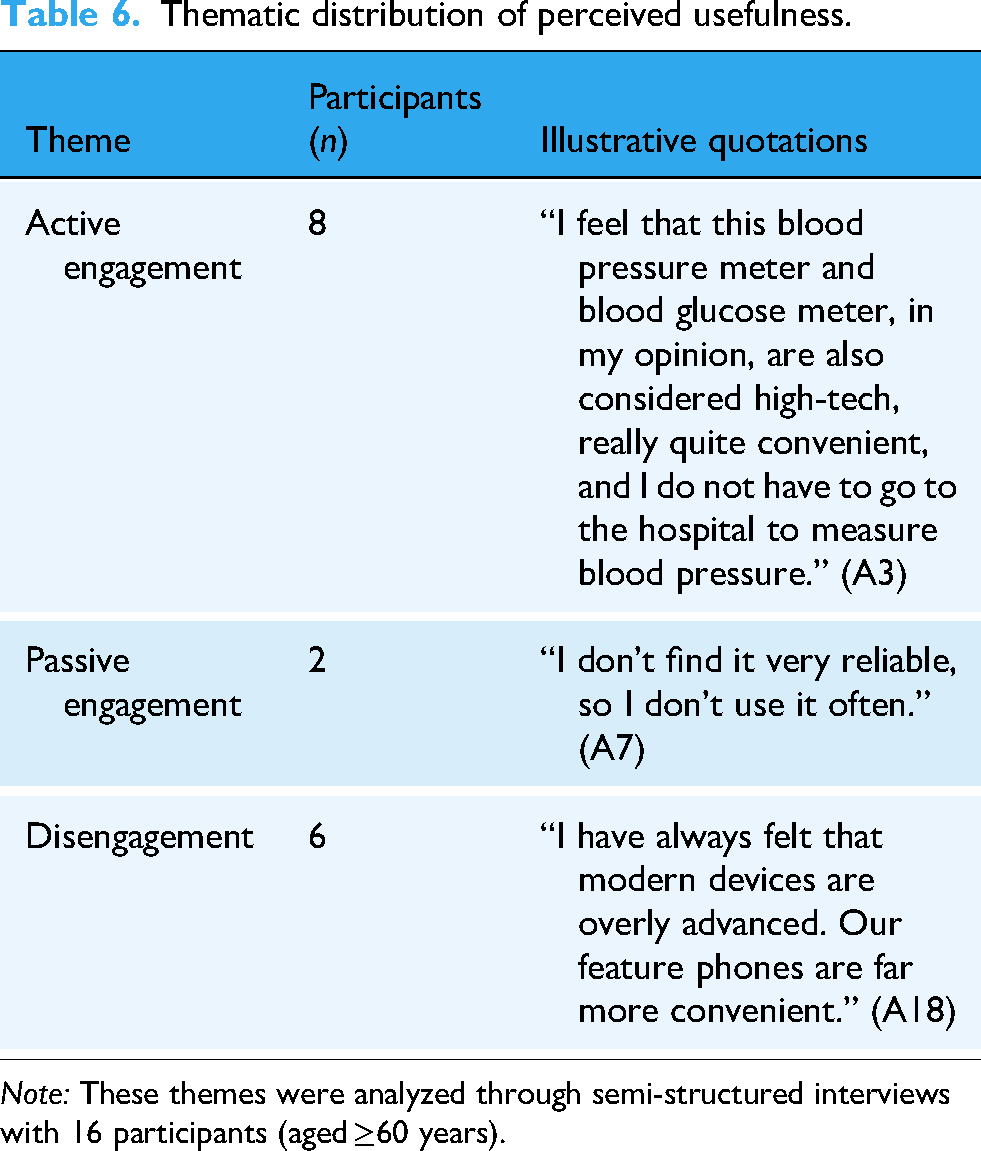
Note: These themes were analyzed through semi-structured interviews with 16 participants (aged ≥60 years).
Perceived ease of use
In this study, perceived ease of use emerged as a critical determinant in older adults’ adoption of digital health technologies, with 20 participants revealing three distinct engagement patterns based on their operational experiences (Table 7). Six participants demonstrated active engagement, navigating technological challenges with varying strategies. While one found the using and operating process straightforward, others acknowledged difficulties but persisted, as evidenced by “I find it difficult, but I’m learning little by little” (A12). Notably, even interested participants encountered barriers, with one expressing hesitation: “I don’t dare to use them due to concerns about improper operation” (A5). Another six participants showed passive engagement, mastering only basic functions and using these devices less frequently. The majority of participants completely disengaged, citing interface complexity and accessibility issues: “These devices have rather complex designs and can be hard on the eyes to use” (A18).
Thematic distribution of perceived ease of use.

Note: These themes were analyzed through semi-structured interviews with 20 participants (aged ≥60 years).
Access back-feeding
Communication medium access
The study revealed that the acquisition of communication devices among older adults was predominantly facilitated by younger generations, with 20 participants demonstrating distinct usage devices preference (Table 8). Thirteen participants expressed a preference for smartphones, which they perceived as more beneficial compared to feature phones. However, seven participants continued to use their feature phones, despite owning smartphones purchased by the younger generations. As a result, the smartphones remained unused.
Thematic distribution of communication medium access.
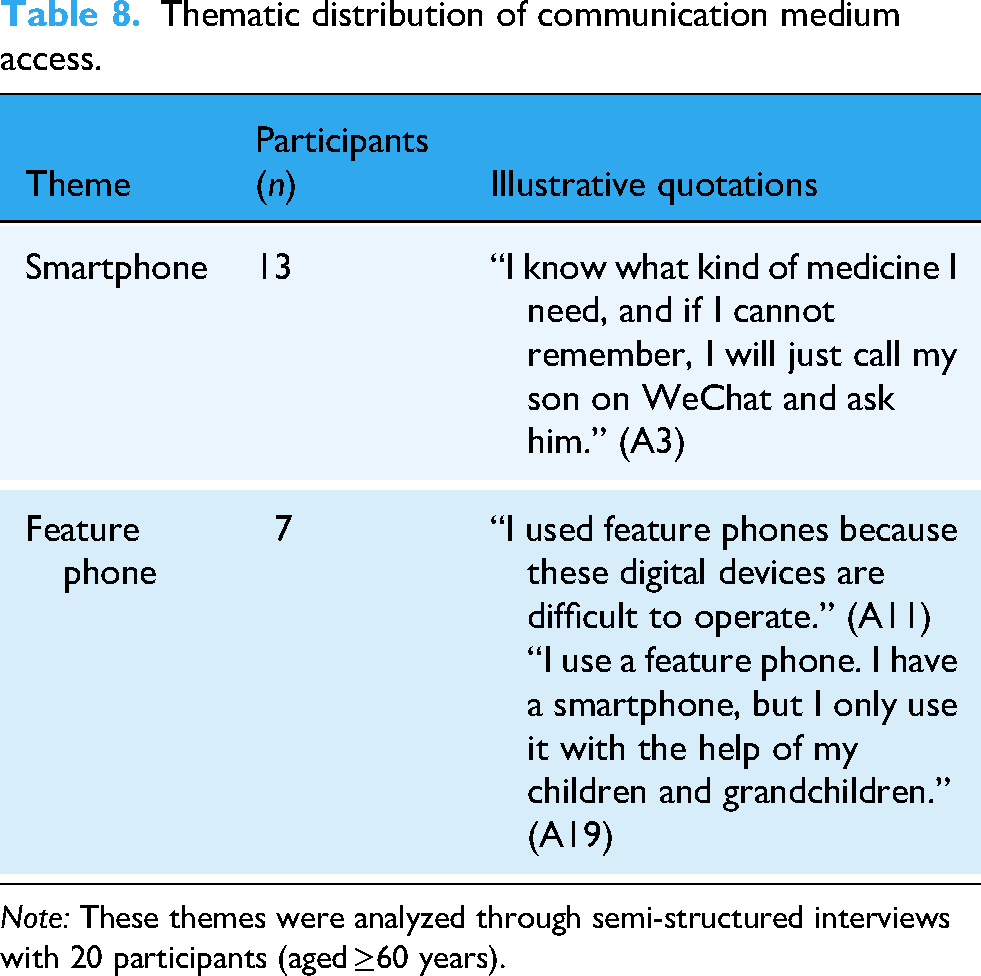
Note: These themes were analyzed through semi-structured interviews with 20 participants (aged ≥60 years).
Digital health device access
In addition to smartphones, six participants were given dedicated health-monitoring devices by younger generations, which enabled continuous physiological tracking (Table 9). Specialized digital health devices respond to specific health needs among these participants, particularly in the management of chronic conditions.
Thematic distribution of digital health device access.

Note: These themes were analyzed through semi-structured interviews with six participants (aged ≥60 years).
Furthermore, this study revealed that the healthcare benefits of digital devices become effective when they are incorporated into household activities, such as family co-learning through television and smartphones to gain health knowledge. My partner and I both have hypertension, and he also has a small brain infarction. Therefore, children often teach us how to alleviate our chronic diseases. We usually watch TV or learn about it on our smartphones. (A4)
Skills back-feeding
Back-feeding content
This study found that the skills back-feeding content among the 20 participants was categorized into several major themes: understanding health information, monitoring personal health, diagnosing and treating diseases, and purchasing medicines online. As detailed in Table 10, understanding health information represented the most commonly taught category. Monitoring personal health followed, with participants learning to use digital health devices such as blood pressure monitors under family guidance. More advanced competencies, including diagnosing and treating diseases and purchasing medicines online, were taught to fewer participants.
Thematic distribution of skills back-feeding content.

Note: These themes were analyzed through semi-structured interviews with 20 participants (aged ≥60 years).
Back-feeding means
Among the 12 participants who reported specific teaching methods, face-to-face and remote back-feeding were equally prevalent, yet demonstrated markedly different outcomes (Table 11). Face-to-face interaction proved more effective for developing operational competence, as it enabled immediate feedback and hands-on guidance. As one participant noted, “I usually wait for my son to get home from work and ask him about it” (A5). However, this approach risked fostering dependency, evidenced by cases where family members directly operated digital devices for older adults. In contrast, remote back-feeding presented substantial challenges due to interface complexity and fragmented communication. The results suggested that participants would prefer to wait for their children or grandchildren to come home so that they can provide face-to-face support, rather than offering remote assistance in real time.
Thematic distribution of skills back-feeding means.
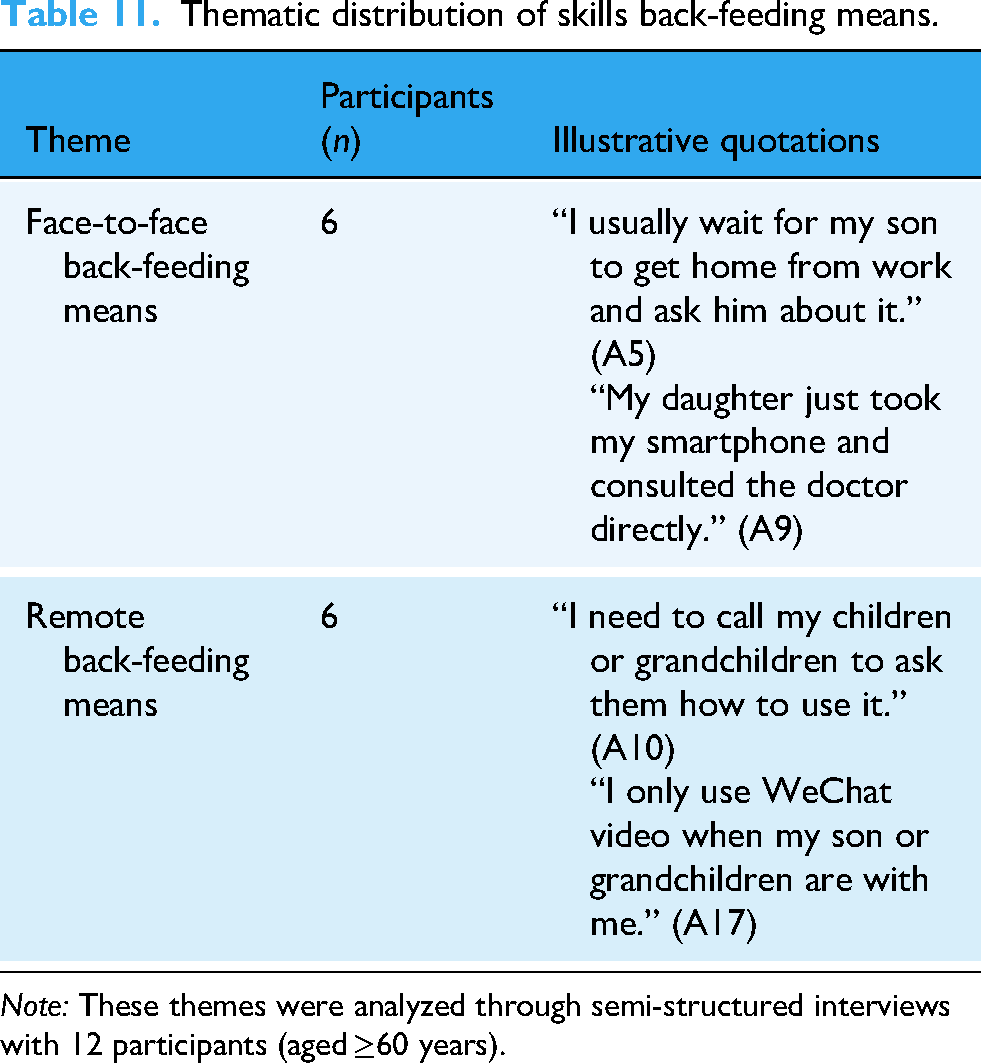
Note: These themes were analyzed through semi-structured interviews with 12 participants (aged ≥60 years).
Back-feeding manners
Among 11 participants reporting instructional methods, three distinct teaching manners emerged with varying levels of effectiveness (Table 12). Four participants primarily accessed digital health services through proxy back-feeding methods of the younger generations. It is characterized by younger generations taking on all tasks for older generations, such as directly assisting participants with offline hospital registration. Five participants experienced directive back-feeding, following the younger generations’ instructions without exercising independent judgment. Only two participants engaged in heuristic back-feeding, exhibiting high autonomy by independently learning and utilizing digital health tools with minimal guidance.
Thematic distribution of skills back-feeding manners.

Note: These themes were analyzed through semi-structured interviews with 11 participants (aged ≥60 years).
Literacy back-feeding
Trust and risk management in online health information
These results revealed that how younger generations employ distinct strategies to manage participants’ online health risks is shaped by their assessment of the older generation's digital judgment capabilities. As detailed in Table 13, younger generations adopted trust-based guidance with seven participants, providing regular risk reminders while trusting their basic discernment. One participant noted, “My son and daughter-in-law have both advised me, so I take certain precautions” (A1). Conversely, with five participants, younger generations implemented restrictive strategies, selectively withholding sensitive functions due to skepticism about their evaluation abilities. For instance, one of the participants mentioned, “My children are afraid that I will be deceived … So I have not been taught to buy health care products online” (A7).
Thematic distribution of trust and risk management in online health information.

Note: These themes were analyzed through semi-structured interviews with 12 participants (aged ≥60 years).
Online health information search and evaluation
In this study, younger generations employed different aspects to cultivate participants’ digital health literacy, focusing specifically on developing information search and evaluation competencies. As shown in Table 14, younger family members actively guided six participants in information-seeking practices, directing them to reliable sources and demonstrating search techniques. This guidance often involved sharing selected content, as one participant described: “I also look through the health information my daughter sends me” (A16). Simultaneously, seven participants received coaching in credibility assessment, learning to cross-verify online information through multiple channels. As one participant's description: “Usually watch from TV … and also screen health knowledge by asking the neighbor's doctor related health questions” (A14).
Thematic distribution of online health information search and evaluation.

Note: These themes were analyzed through semi-structured interviews with 13 participants (aged ≥60 years).
Discussion
This study creatively applied the three-stage model to the health context, uncovering key issues that differ from those in non-health domains. 27 Most importantly, the integrated framework (Figure 1) in this study demonstrates the dynamic interaction between individual factors and intergenerational back-feeding at different stages. In the context of China's digital transformation and an aging population, improving the digital health literacy of older adults is vital for sustainable aging in place. Nevertheless, obstacles such as challenging implementation and low participation rates hinder the technology's potential. 16 This study confirms that intergenerational back-feeding has emerged as a crucial mechanism for enhancing digital health literacy among older adults, which is significant for promoting healthy aging in China. Additionally, these findings support the view that combining user competence with external support is crucial for effective use of digital health technology. This study highlights the importance of family support in fostering digital health literacy. 9

The findings revealed that enhancing digital health literacy among older adults depends not only on individual factors such as age perception, self-rated health, self-efficacy, perceived usefulness, and perceived ease of use, but is also significantly linked to the three stages of intergenerational back-feeding: access, skills, and literacy. In the access stage, back-feeding is categorized into communication medium access and digital health device access. In the skill stage, back-feeding is divided into back-feeding content, back-feeding means, and back-feeding manners. In the literacy stage, back-feeding is classified into trust and risk management in online health information and online health information search and evaluation. The process is illustrated in Figure 1, which shows how intergenerational back-feeding gradually influences older adults’ digital health literacy through different back-feeding stages. It also shows how individual factors interact with intergenerational back-feeding to influence older adults’ digital health literacy.
Complexity of individual factors: dynamic balance between self-perception and health needs
This study indicated that advancing age is often perceived as a natural barrier among older adults, which aligns with research on their experiences with digital healthcare platforms. 42 However, this study also discovered that older adults’ biological age exerted a divergent influence on their perceived age. This finding suggested that older adults’ perceptions of age influence their willingness to utilize digital technology. A key finding of this study is that older adults across all self-rated health statuses (e.g. good, fair, and poor) demonstrated willingness to engage with digital health technologies. This suggests that perceived health status itself does not deter adoption, but rather shapes the nature and motivation for use. Specifically, those with good health engaged in proactive monitoring and prevention, whereas those with poor health focused on managing specific conditions such as osteoporosis or hypertension. This pattern aligns with prior research indicating that health risk perceptions are a significant driver of technology adoption. 43 The variation in use motivation underscores the importance of tailoring digital health interventions to older adults’ specific health perceptions and needs, rather than treating them as an undifferentiated group.
Meanwhile, this study revealed that the self-efficacy of older adults has various influences on their digital health literacy. Participants with strong self-efficacy were willing to acknowledge their digital skill limitations and displayed active skill-learning behaviors. This finding is consistent with systematic reviews identifying self-efficacy as a pivotal component in e-health literacy interventions for older adults. 44 This proactive learning phenomenon can be attributed to their underlying confidence in their ability to learn, which reduces the anxiety and fear associated with acquiring digital skills, thereby fostering enhanced digital health literacy. Participants who exhibited weak self-efficacy ascribed their difficulties to irreversible age-related decline, which resulted in avoidance behavior toward digital health devices. Notably, a minority of participants expressed a willingness to acquire skills, driven by a sense of intergenerational responsibility to avoid falling behind younger generations. This highlights that motivational factors embedded within family relationships can potentially initiate engagement, even in the presence of initial low self-efficacy. This emphasises the complex interplay between individual characteristics and social context in the acquisition of digital health literacy.
In addition, this study further explores the complex relationship between perceived usefulness and perceived ease of use by identifying three distinct engagement patterns: active engagement, passive engagement, and disengagement. Interestingly, while most participants recognized the potential benefits of digital health devices for health management, many ultimately exhibited passive engagement or disengagement due to usability issues. This contradiction between acknowledged usefulness and actual engagement patterns highlights both the promise and limitations of existing digital health technologies. This finding aligns with current research suggesting that technology design needs optimization for older adults’ cognitive abilities and physical limitations. 45
This study revealed how gender, educational background, and living arrangements distinctly shape older adults’ engagement with intergenerational back-feeding and digital health literacy development. Regarding gender differences, female participants demonstrated a complex dual attitude toward health technology adoption. While they often expressed stronger motivation to learn digital skills to avoid burdening their children, this sense of responsibility coexisted with heightened self-doubt about their technological capabilities. This finding challenges the simplistic characterization of “technophobia” among older female adults. Instead, it suggests a more nuanced interplay between intergenerational responsibility and confidence barriers, which requires targeted support strategies. 46 Second, the educational level of older adults influences the progression of their intergenerational back-feeding stage. The participants in higher education may consistently advance to the literacy back-feeding stage. Conversely, most participants with a high school education or below predominantly remained at the skills back-feeding stage, focusing on basic operations. This educational disparity highlights the need for differentiated teaching approaches that accommodate varying literacy levels in digital health interventions. Third, older adults’ living arrangements influence the sustainability of their participation in intergenerational back-feeding. The participants living alone exhibited a reduced propensity to engage in intergenerational back-feeding, attributable to geographic isolation and the absence of timely access to skill support. 47 Interestingly, these participants demonstrated a preference for community-based support systems over family assistance. This suggests that, to ensure comprehensive digital inclusion for all older adults, regardless of their living arrangements, it is essential to supplement family efforts with formal community resources.
The influence of intergenerational back-feeding: a phased impact
The findings of this study indicate that intergenerational back-feeding exhibits variability across different stages, and its influence on the digital health literacy of older adults is characterized by a progressive, stage-by-stage process.
Access back-feeding: first steps in digital health technology engagement
This study revealed that most participants possessed both smartphones and feature phones, with many asserting a preference for the latter. This finding aligns with research indicating the need to prioritize device accessibility within the context of digital inclusion. 9 However, the study stated that device access does not necessarily equate to practical use. A more comprehensive exploration is required to understand older adults’ willingness to utilize such devices and the role of younger generations in enhancing their skills. For example, some participants returned to traditional care owing to functional redundancy (e.g. the complex interface of the smart bracelet), corroborating earlier studies that emphasized the need to simplify technology to accommodate older users. 48
In terms of digital health device access, the findings revealed two main pathways: (1) some participants were provided with specialized health devices, such as blood glucose meters and smart bracelets, by the younger generations. These devices effectively meet older adults’ specific clinical needs, which significantly affect their intention to continue using such devices. 49 (2) The use of smart devices, such as smart televisions and smartphones, to acquire health knowledge represents an innovative approach. This phenomenon can be explained by their integration into family activities, which lowers the barriers to digital health technology engagement for older adults, even without specialized health devices. Currently, no studies have reached this conclusion, so it remains to be confirmed.
Although the acquisition of digital health devices by the younger generations may facilitate self-health monitoring in older adults, they face challenges in accepting new devices and knowledge. Age perception discrepancy and weak self-efficacy may reduce older adults’ willingness to use digital health devices, avoid back-feeding behaviors, and hinder digital health literacy improvement. Therefore, achieving real access to digital health technology relies not only on physical accessibility but also on enhancing the psychological willingness of older adults to utilize it. To further enhance the digital health literacy of older adults, the sustainable use of this technology depends on subsequent skill support, underscoring the limitations of back-feeding from access.
Skills back-feeding: from “intergenerational dependency” to the possibility of “self-discovery”
This study showed that the skills back-feeding content among 20 participants was categorized into four major themes: understanding health information, monitoring personal health, diagnosing and treating diseases, and purchasing medicines online. The younger generations equipped older adults with devices (e.g. blood glucose meters and smart bracelets) and operational training, initially aligning digital health tools with smart care needs. 50 Nevertheless, this study identified that skills back-feeding was predominantly confined to data reading, with a notable deficiency in the comprehensive interpretation of health data. This pattern aligns with the “instrumentalization of technology” observed in digital health platform studies, wherein the device is perceived as a passive recording tool rather than an active instrument for health management. 42 Furthermore, a minority of participants utilized telemedicine functions, such as online consultations and medication purchases, corroborating the evidence that remote healthcare enhances convenience. 51 This study additionally elucidates the distinctive influence of intergenerational back-feeding, highlighting the importance of family as a key component of social support. In particular, the younger generations mitigate older adults’ anxiety regarding the trustworthiness of online health services through technological guidance.
Simultaneously, this study identified that the efficacy of back-feeding varied among the younger generations’ back-feeding means for older adults. Face-to-face means was more effective than remote coaching in enhancing competency, corroborating findings that contextualized training optimizes technology adoption. 51 Besides, the study results showed that back-feeding manners were differentiated between proxy, directive, and heuristic manners. The prevalence of proxy back-feeding aligns with the concept of “technology dependence,” leading to a loss of autonomy, as described in previous studies.21,52 This phenomenon is characterized by a diminished capacity of older adults to engage in active learning, potentially hindering their progression to subsequent stages of back-feeding behavior. Consequently, this may impede the effective promotion of digital health literacy. Notably, this study found that face-to-face back-feeding is usually linked to proxy back-feeding, which strongly promotes older adults’ dependency on family support. Conversely, heuristic back-feeding promoted independent problem solving among older adults, innovatively complementing the assumptions of unidirectional intergenerational knowledge transfer. 42
Furthermore, this study suggested that the development of digital health literacy in older adults during skills back-feeding was influenced by their self-efficacy, perceived usefulness, and perceived ease of use. First, participants with strong self-efficacy were more likely to benefit from heuristic back-feeding manners, progressing more readily to autonomous use. In contrast, those with weak self-efficacy often remained dependent on proxy or directive support from younger generations, creating a cyclical pattern in which a lack of practice further undermined confidence. This study highlights the critical role of self-efficacy as both an outcome and an enabler in the intergenerational back-feeding process, suggesting that targeted interventions to build older adults’ digital confidence may be necessary to break dependency cycles and foster sustainable digital health literacy. Second, following the acquisition of skills from the younger generations, some participants reported enhanced satisfaction with existing online health devices, resulting in increased utilization of these devices. Conversely, some participants struggled to adapt to digital health products. Despite the younger generations’ repeated efforts to reinforce their skills, participants could not use the products effectively. This leads to a negative attitude that ultimately hinders the improvement of digital health literacy. These disparities underscore the need for “aging-adaptive” policy reforms and family interventions. 50
Literacy back-feeding: health information trust and critical evaluation development
During the literacy back-feeding stage, older adults’ digital health literacy spans a wide array of competencies, ranging from the practical application of skills to the critical evaluation of information. At this stage, the younger generations prioritize enhancing the capacity of older adults to search for and discern health information online. Literacy back-feeding can empower older adults to develop greater self-confidence in complex digital environments, thereby enhancing their ability to manage their health.
This study found that most participants exhibited “passive reception” or “half-belief” toward online health information, aligning with studies linking information overload to anxiety. 53 Concurrently, two different strategies emerged concerning the younger generations’ evaluations based on participants’ ability to identify health information. Trust-based guidance fostered collaborative risk management through shared verification, while restrictive teaching created significant limitations in digital health skill acquisition. In other words, younger generations may lack a comprehensive understanding of older adults’ online health information needs. Consequently, specific health application skills are selectively taught, which diminishes the digital health literacy of older adults. Notably, while younger generations actively facilitated older adults’ digital health literacy through reliable source recommendation and verification techniques, a few participants demonstrated significant agency in integrating these digital skills with established offline practices (e.g. referring to health books and consulting doctors offline). This aligns with calls for multimodal health service integration, 54 offering novel insights into digital-age health literacy dynamics.
Limitations and future work
This study had several limitations. First, our sample included a higher proportion of older adults with higher educational levels than the general population. These findings may not apply to subgroups with lower levels of education. Future studies should include more participants from vulnerable groups (e.g. rural and illiterate older adults) to validate the mechanisms identified in this study. Second, the semi-structured interviews for intergenerational back-feeding in this study did not form a two-way dialogue between the young and old generations. Future studies can further enrich the interview subjects to explore how family support is an important influencing factor for older adults. Third, this study focused on the influence of intergenerational back-feeding on older adults’ digital health literacy. Although the participants were selected from different provinces based on economic development and Internet penetration, this study did not consider macro factors, such as digital infrastructure and medical resources. Future research can establish a comprehensive analytical framework.
Conclusion
This study confirmed the pivotal role of intergenerational back-feeding in enhancing the digital health literacy of older adults in China. As digital health technologies become integral to elderly care in China, intergenerational back-feeding remains insufficient to improve digital health literacy without adequate policy implementation. Future efforts should integrate intergenerational back-feeding with national policy and district-level implementation, which is significant for advancing healthy aging. The government should establish public digital health centers in accessible locations to facilitate low-cost access to digital health devices for older adults. Activity centers for senior citizens and social welfare institutions should collaborate with the family members (such as children or grandchildren) of older adults to provide training in digital health technologies. These measures will help implement China's smart care policies by addressing gaps between national policies and local realities, ensuring the successful and sustainable integration of digital health technology for older adults.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251411034 - Supplemental material for Understanding the factors influencing intergenerational back-feeding on digital health literacy of Chinese older adults: Qualitative interview study
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251411034 for Understanding the factors influencing intergenerational back-feeding on digital health literacy of Chinese older adults: Qualitative interview study by Jiachen Sun and Lu Yang in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251411034 - Supplemental material for Understanding the factors influencing intergenerational back-feeding on digital health literacy of Chinese older adults: Qualitative interview study
Supplemental material, sj-docx-2-dhj-10.1177_20552076251411034 for Understanding the factors influencing intergenerational back-feeding on digital health literacy of Chinese older adults: Qualitative interview study by Jiachen Sun and Lu Yang in DIGITAL HEALTH
Footnotes
Ethics considerations
This study was approved by the Research Ethics Committee of Nanjing University of Posts and Telecommunications (Approval No. IRB-2022KYNCS003). All participants provided written informed consent after receiving detailed explanations of the study's purpose, procedures, risks, and benefits. The transcripts were anonymized by replacing identifiable information with coded IDs (e.g. A1-A20) and removing personal details from the transcribed text. The raw interview data and coded thematic material were securely stored in a password-protected file, accessible only to the research team.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Social Science Fund of China under Grant number 21BRK019.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Although the participants provided written informed consent for the interview material to be used for academic research, the sensitive nature of the health narratives required that the data be kept confidential. Therefore, the data supporting this study cannot be shared.
Declaration of generative AI and AI-assisted technologies in the writing process
During the preparation of this work, the authors used ChatGPT in order to improve language. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.