
Abstract
Background
Auditory verbal hallucinations (voices) are common in schizophrenia spectrum disorders (SSD), and cause significant distress, making them a critical target in psychotherapeutic interventions. AVATAR therapy, conducted on a two-dimensional computer screen and its adaptation virtual reality-assisted therapy (VRT), using three-dimensional virtual reality (VR), have shown promise. Despite the potential of VRT, research exploring how specific VR characteristics can simulate voices experiences and affect therapy outcome remains scarce. Addressing this gap is key to refining VRT for persistent voices.
Objective
This qualitative substudy of the CHALLENGE trial explored patient perspectives on modified VRT versions (VRT-Emotions, VRT-Environment, and VRT-Whiteboard) and their therapeutic impact, with the aim to inform intervention refinement and development.
Methods
Semistructured interviews were conducted with 15 participants with SSD and persistent voices after undergoing the modified therapies. Data were analyzed within a pragmatist-critical realism orientation, with a hybrid deductive-inductive approach to thematic analysis. Reflexive team dialogues supported analytical rigor.
Results
One overarching theme: A challenging yet transformative therapy, and three subthemes, corresponding to the specific modifications, were generated: Emotional connection with voice, Recognizability builds resistance, and The power of the written word. The modifications were generally perceived to enhance therapeutic experience and effectiveness, albeit participants’ perspectives varied and sometimes contrasted.
Conclusions
Findings suggest that refining VRT for persistent voices may involve improving avatar's facial expressions, tailoring therapy to voice experiences, and using recognizable VR environments with gradual exposure and selective visual tools. While controlled studies are needed to establish efficacy, these insights offer practical guidance for VRT refinement and development.
Keywords
Introduction
Auditory verbal hallucinations (voices) affect approximately 75% of patients with schizophrenia spectrum disorders (SSD). These voices are often critical, threatening, and distressing. 1 Treatment options include medication, 2 psychotherapy, 3 and brain stimulation. 4 However, nearly one-third of patients continue to experience persistent positive symptoms such as voices despite antipsychotic treatment.5–7 Relational approaches, which aim to shift the interpersonal dynamic between patient and voice commonly characterized by feelings of inferiority and powerlessness, have shown promise.8–10 AVATAR therapy 10 exemplifies this approach, allowing patients to dialogue with a computer-generated voice representation to enhance power and control, with evidence supporting its effectiveness.8,10,11 Building on this, virtual reality-assisted therapy (VRT) for persistent voices uses immersive virtual reality (VR) to enable controlled and realistic voice interactions under therapist guidance, with demonstrated efficacy.12,13 Despite the potential of VRT, research on using VR to enhance AVATAR therapy remains scarce, 11 and little is known about which components drive effectiveness.12,14,15 Understanding this is essential for refining and optimizing VRT. To address this gap, this substudy of the CHALLENGE trial13,16 developed an “Experimental Package” of modified VRT versions aimed at optimizing therapeutic experience and effectiveness of VRT for persistent voices. In this context, optimizing therapy refers to enhancing patients’ engagement, sense of relevance, and perceived value of the intervention. By tailoring VRT, this study seeks to better address patient needs and refine a promising treatment. Given the early stages of this field, qualitative methods are particularly useful for capturing patient perspectives and developing knowledge.17,18 A qualitative exploration can illuminate how patients perceive, experience, and engage with the modified VRT versions, allowing exploration and description of nuanced perspectives and identification of VRT components that contribute most to therapeutic benefit. Previous qualitative studies, such as AVATAR1 19 and gameChange, 20 have shaped and refined similar interventions, highlighting the importance of incorporating patient perspectives to improve mental health services and support clinical translation.21,22 Accordingly, this study explored patient perspectives on modified VRT versions and their therapeutic impact, with the aim to inform intervention refinement and development.
Methods
Parent study: the CHALLENGE trial
This qualitative substudy is part of the CHALLENGE randomized clinical trial (ClinicalTrials.gov identifier NCT04661163) which investigated the efficacy of VRT compared to supportive counseling for persistent voices in SSD. Inclusion criteria were: 1) age ≥18 years, 2) primary SSD diagnosis (ICD-10, F20-29; excluding F20.6 and F21), 3) voices ≥3 months, 4) outpatient treatment in Denmark, 5) ability to provide informed consent, 6) stable antipsychotic medication for ≥4 weeks, and 7) insufficient response to current or at least two prior antipsychotic treatments. Exclusion criteria were: 1) inability to identify a dominant voice, 2) organic brain disease, 3) substance abuse interfering with treatment, 4) voices in a language not spoken by therapist, 5) language barriers, 6) inability to tolerate assessments, or 7) severely impaired vision. The study found that VRT significantly reduced voice-related symptoms compared to supportive counseling.13,16
Virtual reality-assisted therapy
Virtual reality-assisted therapy rests upon AVATAR therapy 10 and integrates relational, cognitive-behavioral, and compassion-focused elements. The patient creates a visual-auditive representation (an avatar) resembling the most distressing voice, with the therapist's voice transformed to match via software. Sessions involve VR exposure using a head-mounted display and headphones. In initial sessions, the therapist facilitates a dialogue between patient and avatar in VR by speaking as the avatar, using preselected statements, or as a supportive therapist. Therapy follows three phases: 1) strengthening patient power by practicing confronting malevolent and demeaning avatar comments, 2) enhancing patient self-worth as the avatar adopts a more conciliatory stance, and 3) focusing on recovery and future goals. Each 45-min session includes 5–15 min of VR interaction.
Qualitative substudy: the experimental package
This substudy explored three modifications to the VR software applied in the parent study:
VRT-Emotions: The avatar expressed facial emotions (anger, sadness, happiness) to increase realism of VR interaction and address social cognitive deficits prevalent in SSD.
23
Furthermore, these emotional expressions facilitated recognition of changes in the avatar's attitude throughout therapy. VRT-Environment: Patients were gradually exposed to different VR environments, starting with the office environment from the parent study, then a living room, and lastly a bus. These additional environments aimed to enhance real-world applicability and skill transfer.
24
VRT-Whiteboard: A whiteboard in the VR environment displayed statements that the therapist and patient had agreed should be expressed to the avatar. This modification addressed memory impairments in SSD
25
by reducing cognitive load of recalling statements, leaving more focus to confront the avatar.
Sampling
Following the 24-week postbaseline assessment in the parent study, a selected number (n = 15) of participants, randomized to supportive counseling, were invited to participate in this substudy. Consenting participants were randomly assigned (1:1) to receive seven individual sessions of one of three modified VRT versions. Upon therapy completion, participants were invited to an individual interview. Eligibility criteria matched those of the CHALLENGE trial (see “Parent study: the CHALLENGE trial” section). Participants were conveniently sampled based on stable attendance at 12- and 24-week postbaseline assessments and recent completion of 24-week postbaseline assessment in the parent study. Moreover, maximum variation sampling by gender and cognition was applied to capture diverse patient experiences. This combined approach reflects a pragmatist-critical realism orientation, 26 acknowledging practical constraints in the research context, while aiming to capture variation in participants’ perspectives. Given the study's relatively narrow aim and high sample specificity, we estimated that 15 participants (i.e., equals the number of patients invited to try the modified VRT versions), five per modification, would generate sufficient information power to address the study aim. 27
Data collection and generation
Semistructured interview guides were developed for each group (Appendices A-C in Supplemental material), designed to capture both practical information about the modified VRT versions and participants’ experiences with them. They comprised 10 sections: conceptual clarification, introductory questions and motivation, acceptability, feasibility, tolerability, modification, perceived changes/empowerment, usability, security, and debriefing. Interviews featured open-ended questions, with closed-ended subquestions for guidance as needed. Data were collected from 28th August 2022 to 12th September 2023. Eight interviews were conducted at Mental Health Center Copenhagen, five at Aalborg University Hospital, and two online via Microsoft Teams. Only the researcher and the participant were present in the interview situation. Interviews were audio-recorded and therefore field notes were not taken. Interviews lasted 27–65 min and were transcribed verbatim. Transcripts were not returned to participants for comment or correction.
Data analysis
Data were analyzed within a pragmatist-critical realism orientation. 26 From a pragmatic perspective, the goal was to produce practical findings to inform intervention refinement and development, while a critical realist stance supported exploration of new insights. Accordingly, a hybrid deductive-inductive thematic analysis 28 was employed to integrate rationale-driven themes, while remaining open to generating new ones. It was an iterative process involving the following steps: 1) Familiarization: Transcripts were familiarized. 2) Coding: The analysis was initiated deductively, informed by the rationales underpinning the modifications (see “Qualitative substudy: the experimental package” section). A codebook with predefined codes included in the interview guides was developed, ensuring that relevant extracts were coded (Table 1). Interviews were coded separately within each modification. However, after coding all interviews, patterns across the modified VRT versions became evident. Therefore, a more inductive analysis process began in line with the method's iterative nature. Interviews were recoded with a data-driven approach, coding extracts independently of the preexisting coding frame. This hybrid approach combined two contrasting philosophical methods of reasoning. While the predefined codes, based on the study's objective and the interview questions, called for a top-down, rationale-driven analytical process, the inductive component allowed for openness to insights derived from participants’ experiences with the modified VRT versions. 3) Generating initial themes: Deductive and inductively generated codes were collated to generate themes. 4) Reviewing themes: Themes were reviewed for consistency with coded extracts and entire dataset. 5) Defining and naming themes: Themes were defined and named. 6) Writing up: The narrative for each theme was written.
Overview of predefined codes used in the thematic analysis.

Researcher reflexivity
Interviews were conducted by GJ (MSc, Researcher, F), who had no prior relationship with participants or study involvement. Coding and analysis were carried out by KR (MSc, Researcher, F), uninvolved in study planning and interview guides development. Both were experienced in qualitative methods applied to mental health research. Aligning with our pragmatic-critical realism orientation, we acknowledge that subjectivity is an inherent part of qualitative research. 29 As the study was conducted within a research unit focused on VRT, the researchers’ professional backgrounds and familiarity with the field may have influenced data collection, analysis, and interpretation. Furthermore, the hybrid deductive-inductive approach meant that existing theoretical knowledge of VRT and SSD informed the initial deductive coding, while remaining open to novel insights emerging from data when coding inductively. Reflexive team dialogues helped balance these methods of reasoning, ensuring that interpretations were both theoretically informed and empirically grounded. Participants did not provide feedback on the findings.
Ethical declaration
The CHALLENGE trial was approved by the Committee on Health Research Ethics of the Capital Region of Denmark (Project-ID: H-19086621, obtained 10th March 2020) and the Danish Data Protection Agency. This substudy, included in the approved protocol, required no separate approval. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. All participants provided written informed consent before study initiation and were informed that withdrawal would not affect treatment. Written informed consent was also obtained for audio-recording of the interviews. Participants were assured of confidential, anonymized data handling, with pseudonyms used in participant quotations.
We used the COREQ checklist to ensure adherence to the COREQ reporting criteria. 30
Results
The final sample comprised 15 participants (8 female; mean age = 35.9 years, SD = 12.4), with 86.6% diagnosed with schizophrenia (F20) by clinical staff at their standard treatment facility. On average, participants had experienced voices for 15.9 years (SD = 9.5). One participant, although not recruited through the CHALLENGE trial, fulfilled its eligibility criteria. This participant, along with six others whose 24-week postbaseline assessments were not conducted recently, were reassessed using the Psychotic Symptom Rating Scales, Auditory Hallucinations subscale and Delusions subscale, 31 the Scale for Assessment of Positive Symptoms, 32 the Voice Power Differential Scale, 33 and the Personal and Social Performance Scale. 34 Baseline demographic and clinical characteristics are presented in Table 2. Analysis of variance and chi-square tests revealed no significant group differences. All participants consented to and completed posttherapy interview.
Baseline demographic and clinical characteristics.

Notes. *Data missing for one participant in the VRT-Whiteboard group on age, duration of hearing voices, SAPS summary (global) score, and VPDS total score. **Set to be significant at ≤ 0.05. Data are mean (SD) or n (%).
The Psychotic Symptom Rating Scales, Auditory Hallucinations subscale (PSYRATS-AH), bThe Psychotic Symptom Rating Scales, Delusions subscale (PSYRATS-D), cThe Scale for Assessment of Positive Symptoms (SAPS), dThe Voice Power Differential Scale (VPDS), eThe Personal and Social Performance Scale (PSP).
Thematic analysis
Table 3 presents the inductively generated codes, developed during data analysis and used across groups. Based on the findings from the thematic analysis, one overarching theme was constructed to reflect participants’ perspectives and experiences across the modified VRT versions, along with three subthemes corresponding to each modification.
Overview of inductively generated codes, overarching theme, and subthemes.
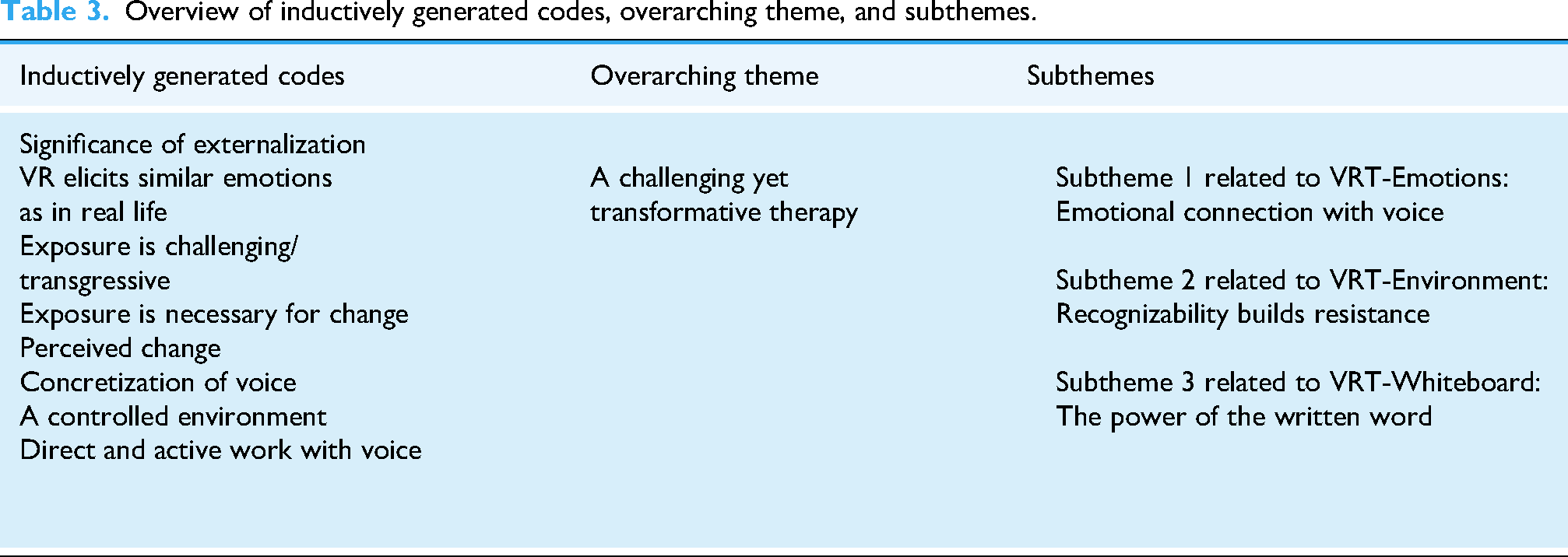
Overarching theme: a challenging yet transformative therapy
Across the modified VRT versions, therapy was characterized as challenging and transgressive, especially in the initial sessions. Participants experienced practicing confrontation with their voice in naturalistic VR settings not only as anxiety-provoking but also as enhancing therapeutic value: “It was very challenging to sit in front of the avatar we created and simply to see it… but it was cool, and it moved something in me, which gave me a motivation to do more of it.” (Adam) “[I]t became a bit more real… Meaning that what we do in VR, uh, affects a bit more… and that's good because, I mean, I become more overwhelmed by it, but it's also when I become overwhelmed that I can work with it (…) the more real it becomes and the more overwhelmed I become, the more it can be related to my reality… so, I get some tools that I can actually use outside VR as well.” (Sarah) “It was also knowing that if I confront the voice in here, then it can’t harm me. It doesn’t start yelling at me… It's the therapist who controls it.” (Julie) “This made sense because it was like: ‘okay, the voice says this in these situations, and what do I do then?’” (Caroline)
Subtheme 1 related to VRT-emotions: emotional connection with voice
When asked about ability to recognize facial emotions, some participants reported no such impairments in real life. However, participants found it difficult to recognize the avatar's facial emotions, and none identified all the emotions the avatar could express (anger, sadness, happiness). Happiness was most recognized; only one noticed sadness. In accordance with this, participants suggested improving the VR software for clearer facial expressions. For example, one participant believed that if the avatar needed a darker skin color to resemblance the voice, then more shades of black would ease recognition of its facial emotions. Despite these challenges, participants felt more understood and validated when the avatar responded to their statements with corresponding facial emotions: “I think it was really nice that it [the avatar] could react to what was being said, so it wasn’t totally cold (…) Sometimes words can be a bit empty because people sometimes just say what's expected… so, I mean, it made what it said feel a bit more believable.” (Caroline)
One participant, who only experienced the voice auditorily without visual perception, found the facial expressions unhelpful. In contrast, participants who experienced their voice both auditorily and visually found the facial emotions enriching as they resembled how they perceived their voice. However, one participant, who experienced the voice as a shadow without facial features, not only described the facial emotions as “weird” and “unfamiliar” initially but also explained: “The fact that you could feel that there was, you know, that it could show emotions, it was actually a bit… like it had weaknesses or something like that… so, I didn’t feel like I was the only one who was weak.” (Daniel)
Subtheme 2 related to VRT-environment: recognizability builds resistance
Participants described the office environment as unfamiliar from their everyday voice experiences but found the living room and bus environment recognizable as they commonly experienced their voice in such settings. Participants expressed that the recognizability made the therapy more relevant and improved transfer of skills acquired in VR to real life situations, including grocery stores and supportive housing residences. Especially the bus environment was emphasized as recognizable, due to its association with real-life distressing voice experiences. Therefore, participants stressed the importance of gradual exposure to the different VR environments, and some noted the significance of gradual exposure in enhancing therapeutic process: “We moved on to the bus which I was nervous about, but I actually experienced that with the progress I had made in VR, I felt quite comfortable with it. (…) So I, myself, asked the voice to come closer and that was such an awesome feeling… to feel so on top of things and confident. After having built it up through both office- and living room-environment to be like ‘come closer, it's fine.’” (Sarah) “In the end, I managed to tell the voice that I didn’t think it was speaking very nicely to me… I think the room we were in, the living room, made me dare to say it to the voice. It felt more like a conversation you could have with any other person… that definitely worked really well for me. The thing about making the voice just like any other person.” (Rebecca)
Subtheme 3 related to VRT-whiteboard: the power of the written word
Participants highlighted the whiteboard as a useful and helpful tool, reinforcing their sense of authority in therapy. It supported recall of statements to express to the avatar and guided their responses to the malevolent and demeaning avatar: “I wouldn’t have been able to remember what I was supposed to say to the voice… especially because having to say no so firmly is not, uh, it's very unnatural for me (…) It has been really good for me that it was on the whiteboard. I can’t think that way on my own.” (Julie) “It [the whiteboard] made me calm so that I was able to confront the voice (…) I’m almost certain that I wouldn’t have been able to say it with the same confidence, if I hadn’t seen it in writing.” (Adam) “You get anxious when you see it [the avatar] and at the same time, you’re also reminded, that you must confront it when it's written on the whiteboard (…) You’re reminded that you have to say no.” (Julie)
Discussion
The objective of this study was to explore patient perspectives on modified VRT versions and their therapeutic impact, with the aim to inform intervention refinement and development. Overall, the findings suggest that participants experienced positive changes in their relationship with and appraisal of the voice following therapy, although the changes were of varied degree. Participants experienced the modifications as evoking emotional responses similar to real life voice experiences, which was highlighted as crucial for change. Some described improvements in voice-related symptoms posttherapy, while all explained acquiring new strategies for interacting with their voice. These findings mirror previous studies demonstrating symptom reduction and increased empowerment following VRT.12–14,35,36 Therapy was experienced as challenging, echoing previous studies that highlight strong emotional reactions to VRT or AVATAR therapy.12,14,19 While aligning with general effects of exposure therapies, 37 these reactions underscore the importance of a sensitive approach during the first therapy phase. Furthermore, participants perceived therapy as enhancing ability to act and exercise control in the relationship with their voice, suggesting that the modified VRT versions improved self-efficacy by fostering agency. 38 For participants in the VRT-Whiteboard group, the whiteboard supported authority by serving as a cognitive anchor and aiding memory recall. Improved memory performance has been linked to enhanced self-efficacy, 39 which may explain their increased confidence and ability to confront their voice. However, the whiteboard had mixed effects; it both increased emotional tension for one participant and reduced anxiety for another, reflecting the nuanced experiences participants had with this tool. Thus, it can function as both a stressor and a coping mechanism, depending on individual responses.
In the VRT-Emotions group, challenges with recognizing the avatar's facial emotions may relate to emotion perception deficits often observed in SSD, particularly regarding negative facial emotions. 40 While this implies need for improvement, the facial emotions still facilitated emotional engagement and offered new ways of relating to the voice. Additionally, social responsiveness fosters emotional connection and understanding in human–human interactions.41,42 This supports the assumption that human-like social cues in virtual agents make individuals respond to them as they would to humans, 43 consequently making the avatar's social capabilities crucial for therapy effectiveness. Furthermore, the perceived usability and applicability of the modification appeared to be associated with how participants perceived their voice in real life. Voice characterization, including physical voice features, has been shown to predict behavioral engagement with the avatar 44 and it may limit AVATAR therapy effectiveness if patients experience voices with no physical characterization. 45 In this regard, a key finding in this study was that the avatar's facial emotions enabled engagement with a voice perceived without facial features in real life, offering access to previously absent aspects of the voice experience. This indicates a potential to optimize therapeutic experience and outcomes for patients with purely auditory voices. Participants in the VRT-Environment group believed that recognizable VR environments helped transfer therapeutic gains to real life. This may stem from greater sense of presence through recognizability, essential for transferring learned therapy skills to everyday life.20,24,46 While previous studies have demonstrated efficacy of VRT in reducing voice-related symptoms and distress using generic environments,12,14 this finding indicate that VR environments resembling real life settings, where voices are distressing, offer additional therapeutic benefits.20,47 Gradual exposure to different VR environments supported resistance development, highlighting how VR promotes habituation and threat reevaluation by allowing controlled exposure. 48 While some participants benefitted from a relaxed setting, others valued more challenging ones. In the VRT-Whiteboard group, the whiteboard's effectiveness was believed to depend on memory impairment, reflecting a dual nature of the tool where it can be experienced as both supportive and potentially intrusive. These findings stress the importance of tailored VRT.
Strengths and limitations
The qualitative design provided valuable insights into patients’ subjective experiences beyond the reach of quantitative methods.17,18 Another strength is that all 15 participants undergoing the modified VRT versions completed the posttherapy interview, ensuring comprehensive representation. However, lack of sampling on ethnicity may restrict diversity of findings, and the qualitative approach limits establishing causality between modifications and perceived changes. Furthermore, the two online interviews may raise concern about data quality. It has been argued that physical presence is necessary for emotional connection between researcher–participant, 49 while other studies show that technology-mediated interviews can yield data of equal or higher quality, particularly for sensitive topics.50,51
Although multiple coders can enhance reliability, 18 only one researcher performed the data coding. To mitigate this, the analysis was initially deductively rationale-driven, followed by an inductive approach, to reduce selective interpretation. 18 Nonetheless, the absence of lived experience involvement remains a limitation, as such involvement strengthens research through development of more applicable interventions and deepened data analysis.22,52
Conclusions and implications
The findings suggest that the modified VRT versions have potential to enhance therapeutic experience and effectiveness, albeit further development is needed. Understanding the perspectives of individuals who disengage from treatment is crucial for optimizing interventions, but this was not possible in current study as all participants completed therapy. Since qualitative methods preclude establishing causal relationships, efficacy studies are warranted to assess the modifications’ impact on therapy outcomes. Future research should also involve VRT-trained therapists for refinement and development. Furthermore, findings revealed that VRT was experienced as challenging yet also empowering. This tension merits further investigation as it may reflect a Goldilocks principle, referring to optimal use of therapy techniques: sufficient to promote therapeutic change without hindering progress or causing adverse effects. 53 Such investigations could also inform application and refinement of VRT. In line with our reflexive stance, we acknowledge that our interpretations were shaped by the researchers’ professional backgrounds and familiarity with VRT, which may have influenced conclusions. While the study provides qualitative insights on participants’ therapy experiences, its contribution is applied, offering valuable clinical and VR technical knowledge that inform the application and further development of VRT for persistent voices (see Box 1). The team is now discussing how to integrate these adaptations, with therapists assessing their relevance for each patient.
Considerations regarding application and future development of VRT

Supplemental Material
sj-docx-1-dhj-10.1177_20552076251411033 - Supplemental material for Patient perspectives on modified virtual reality-assisted therapy for persistent auditory verbal hallucinations: A qualitative substudy of the CHALLENGE randomized clinical trial
Supplemental material, sj-docx-1-dhj-10.1177_20552076251411033 for Patient perspectives on modified virtual reality-assisted therapy for persistent auditory verbal hallucinations: A qualitative substudy of the CHALLENGE randomized clinical trial by Katrine Rasmussen, Ditte Lammers Vernal, Lise Sandvig Mariegaard, Gry Jørgensen, Fatime Zeka, Lisa Charlotte Smith, Merete Nordentoft, Julie Midtgaard and Louise Birkedal Glenthøj in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251411033 - Supplemental material for Patient perspectives on modified virtual reality-assisted therapy for persistent auditory verbal hallucinations: A qualitative substudy of the CHALLENGE randomized clinical trial
Supplemental material, sj-docx-2-dhj-10.1177_20552076251411033 for Patient perspectives on modified virtual reality-assisted therapy for persistent auditory verbal hallucinations: A qualitative substudy of the CHALLENGE randomized clinical trial by Katrine Rasmussen, Ditte Lammers Vernal, Lise Sandvig Mariegaard, Gry Jørgensen, Fatime Zeka, Lisa Charlotte Smith, Merete Nordentoft, Julie Midtgaard and Louise Birkedal Glenthøj in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251411033 - Supplemental material for Patient perspectives on modified virtual reality-assisted therapy for persistent auditory verbal hallucinations: A qualitative substudy of the CHALLENGE randomized clinical trial
Supplemental material, sj-docx-3-dhj-10.1177_20552076251411033 for Patient perspectives on modified virtual reality-assisted therapy for persistent auditory verbal hallucinations: A qualitative substudy of the CHALLENGE randomized clinical trial by Katrine Rasmussen, Ditte Lammers Vernal, Lise Sandvig Mariegaard, Gry Jørgensen, Fatime Zeka, Lisa Charlotte Smith, Merete Nordentoft, Julie Midtgaard and Louise Birkedal Glenthøj in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076251411033 - Supplemental material for Patient perspectives on modified virtual reality-assisted therapy for persistent auditory verbal hallucinations: A qualitative substudy of the CHALLENGE randomized clinical trial
Supplemental material, sj-docx-4-dhj-10.1177_20552076251411033 for Patient perspectives on modified virtual reality-assisted therapy for persistent auditory verbal hallucinations: A qualitative substudy of the CHALLENGE randomized clinical trial by Katrine Rasmussen, Ditte Lammers Vernal, Lise Sandvig Mariegaard, Gry Jørgensen, Fatime Zeka, Lisa Charlotte Smith, Merete Nordentoft, Julie Midtgaard and Louise Birkedal Glenthøj in DIGITAL HEALTH
Supplemental Material
sj-pdf-5-dhj-10.1177_20552076251411033 - Supplemental material for Patient perspectives on modified virtual reality-assisted therapy for persistent auditory verbal hallucinations: A qualitative substudy of the CHALLENGE randomized clinical trial
Supplemental material, sj-pdf-5-dhj-10.1177_20552076251411033 for Patient perspectives on modified virtual reality-assisted therapy for persistent auditory verbal hallucinations: A qualitative substudy of the CHALLENGE randomized clinical trial by Katrine Rasmussen, Ditte Lammers Vernal, Lise Sandvig Mariegaard, Gry Jørgensen, Fatime Zeka, Lisa Charlotte Smith, Merete Nordentoft, Julie Midtgaard and Louise Birkedal Glenthøj in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank the participants who took part in the study. The authors also thank Emma Slebsager Riis and Katja Skovgaard Bang for conducting the therapy in the Experimental Package.
ORCID iDs
Ethical considerations
The CHALLENGE trial was approved by the Committee on Health Research Ethics of the Capital Region of Denmark (Project-ID: H-19086621, obtained 10th March 2020) and the Danish Data Protection Agency. This substudy, included in the approved protocol, required no separate approval. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. We used the COREQ checklist to ensure adherence to the COREQ reporting criteria. 30
Consent to participate
All participants provided informed consent and were informed that withdrawal would not affect treatment. Informed consent was also obtained for audio-recording. Participants were assured of confidential, anonymized data handling, with pseudonyms used in participant quotations.
Contributorship
KR: Conceptualization, methodology, formal analysis, writing – original draft preparation, writing – review and editing, and project administration. DLV: Conceptualization, investigation, and writing – review and editing. LSM: Conceptualization, investigation, and writing – review and editing. GJ: Conceptualization, methodology, investigation, and writing – review and editing. FZ: Investigation and writing – review and editing. LCS: Conceptualization, methodology, formal analysis, and writing – review and editing. MN: Conceptualization, writing – review and editing, and funding acquisition. JM: Conceptualization, methodology, formal analysis, writing – original draft preparation, writing – review and editing, supervision, and project administration. LBG: Conceptualization, methodology, writing – original draft preparation, writing – review and editing, supervision, project administration, and funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Innovation Fund Denmark (grant number 8088-00023B Grand Solution) and the Independent Research Fund Denmark (grant number 2096-00012B).
Declaration of conflicting interests
DLV, LSM, and LBG have received compensation from Heka VR for teaching VRT to clinicians in other research projects in Denmark and abroad. Further, DLV and LBG are currently involved in other research collaborations with Heka VR.
Data availability
Data are available upon reasonable request. All relevant data are included in the article. Raw data are stored on a secure server.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.