
Abstract
Objective
This review examines how virtual communities support patients with lung cancer, focusing on their effectiveness in improving emotional wellbeing and treatment adherence, and addressing challenges like misinformation and privacy.
Methods
A scoping review was conducted using PubMed, CNKI, and Web of Science. Inclusion criteria included patients with lung cancer aged ≥18, virtual community interventions, and original research in Chinese or English. Studies were screened and appraised independently.
Results
Nineteen studies (2015–2024) showed that apps and websites were key platforms, offering information, emotional support, and social interaction. These communities reduced anxiety, improved treatment compliance, but did not affect survival rates. Misinformation and privacy were concerns.
Conclusions
Virtual communities significantly benefit patients with lung cancer psychologically and socially, but not in survival. Future research should address diversity, longitudinal designs, and platform optimization to reduce risks.
Introduction
Lung cancer remains a formidable malignancy, profoundly affecting patients both physically and psychologically. 1 The complexity of its management is exacerbated by the multifaceted challenges patients face, including not only physical symptoms but also psychological distress, social isolation, and lifestyle disruptions. 2 Conventional clinical approaches often struggle to adequately address this broad spectrum of needs.
In response to these limitations, virtual communities of practice have emerged as an innovative and supportive model in the digital era.3,4 These platforms allow patients to access reliable medical information, share personal experiences, and form supportive networks, thereby helping to alleviate the disease-related emotional and physical burdens. 5 By facilitating peer support and timely information exchange, these communities play an increasingly important role in comprehensive lung cancer care.
Beyond emotional and social support, virtual communities also serve as effective platforms for health education. 6 Through multimedia and interactive tools, patients can better understand their disease, treatment options, and necessary lifestyle adjustments. This tailored approach improves both comprehension and retention of health knowledge, 7 enabling patients to participate more actively in their treatment decisions.
Such functions align closely with the principles of supportive care, which aims to address the physical, emotional, social, spiritual, and informational needs of patients throughout their illness trajectory. 8 An interdisciplinary effort—spearheaded by oncology teams and supplemented by palliative care, social work, rehabilitation, psycho-oncology, and integrative medicine—is essential to deliver this multidimensional support.
The review
Design
The review will be conducted in accordance with the methodological framework developed by Arksey and O’Malley, 9 which encompasses the following five key components: (1) clarification of the research question; (2) execution of a search for relevant research literature; (3) screening of literature pertinent to the research question; (4) presentation of data through graphical means to illustrate the findings; and (5) an extensive scoping review, followed by the collation and summary of research findings, and ultimately, the preparation of a report that conforms to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. Details can be found in Supplemental Appendix S1.
Search methods
Systematic search databases, including PubMed, CNKI, Wanfang, CBM, CINAHL, JBI, Cochrane Library, Medline, Embase, ScienceDirect, Web of Science, and PsycINFO. Refer to Supplemental Appendix S2 for specific retrieval. The search was conducted by combining Mesh and terms, and the search time was from January 2013 to December 2024. The complete search strategy link has been uploaded to PROSPERO, please refer to Supplemental Appendix S3 for details.
For this review, four research questions were asked: Q1: What are the current trends in the adoption and technological evolution of virtual communities for patients with lung cancer? Q2: Which digital platforms are used to host virtual communities for patients with lung cancer? Q3: What are the functions of virtual communities? Q4: What are the psychological, social, and clinical benefits of virtual community engagement for patients with lung cancer?
Inclusion and exclusion criteria
Inclusion criteria:
The subjects were patients with lung cancer, aged ≥18 years old, and the treatment method and stage were not limited; Related content of virtual community, such as the specific form, function, implementation approach and outcome evaluation of virtual community; The type of literature is original research; and Published in Chinese or English.
Exclusion criteria:
Low-quality literature; Incomplete data, incomplete information, or unable to obtain the full text of the literature; and Republished or updated literature.
Study selection
The literature retrieved was imported into Note Express (version 3.9.0) to eliminate duplicate publications. Following the established inclusion and exclusion criteria, two researchers skilled in evidence-based nursing practices independently undertook an initial literature screening based on titles and abstracts. Subsequently, a full-text review of the selected articles was performed for more detailed re-screening. To ensure the rigor and consistency of the screening process, any uncertainties or disagreements regarding the inclusion of specific literature were resolved through a structured deliberation process involving a third investigator. This process included re-evaluating the literature against the predefined criteria and engaging in consensus-driven discussions to reach a final decision. This approach guarantees a thorough and transparent screening process, ensuring the reliability and accuracy of the study selection.
Quality appraisal
The methodological quality of included studies underwent independent evaluation by two reviewers (XBZ and LZ), employing Joan Kennelly's 10 established criteria for overall assessment (Supplemental Appendix S4). For randomized controlled trials (RCTs), the Quality Checklist for RCTs and Observational Studies was applied; qualitative studies were assessed using the Guidelines to Evaluate the “Quality and Evidence” of Qualitative Studies to examine methodological consistency and alignment between conclusions and data analysis. Discrepancies between reviewers were resolved through discussion or consultation with a third reviewer (YYL). RCTs scoring below 15 were classified as poor quality, those scoring 15 to 19 as medium quality, and those scoring above 19 as high quality. Detailed methodological quality assessment criteria are provided in Supplemental Appendix S5.
Data extraction and charting
Data Extraction Data were extracted using Microsoft Excel 2016. Two researchers independently performed the data extraction, which was then integrated by a third researcher. The information extracted included the author's name, publication year, country, study design, treatment type, cancer classification, sample size, virtual community platform, intervention timing, intervention duration, application environment, evaluation time, outcome measurements, and outcomes.
Results
Characteristics of studies
The study in question aggregates 19 articles (Figure 1) that investigate the engagement of patients with lung cancer with virtual communities over a 9-year period, from 2015 to 2024. The research methodologies include 12 RCTs, 1 one-arm intervention studies and 6 qualitative studies. The patient population consists of individuals diagnosed with lung cancer, which includes the two main subtypes: non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC). The sample sizes for these studies extend from a minimum of 19 to a maximum of 200 participants, with the studies conducted across China, Germany, the United Kingdom, Italy, Korea, America, and Canada.

Flowchart of study selection process.
Based on the general characteristics of the 19 included studies, Figure 2 illustrates a noticeable upward trend since 2015 in the number of publications focusing on the use of virtual communities among patients with lung cancer. A significant proportion of these studies was conducted in China, and the primary setting in which these virtual communities are utilized is the patient's home.
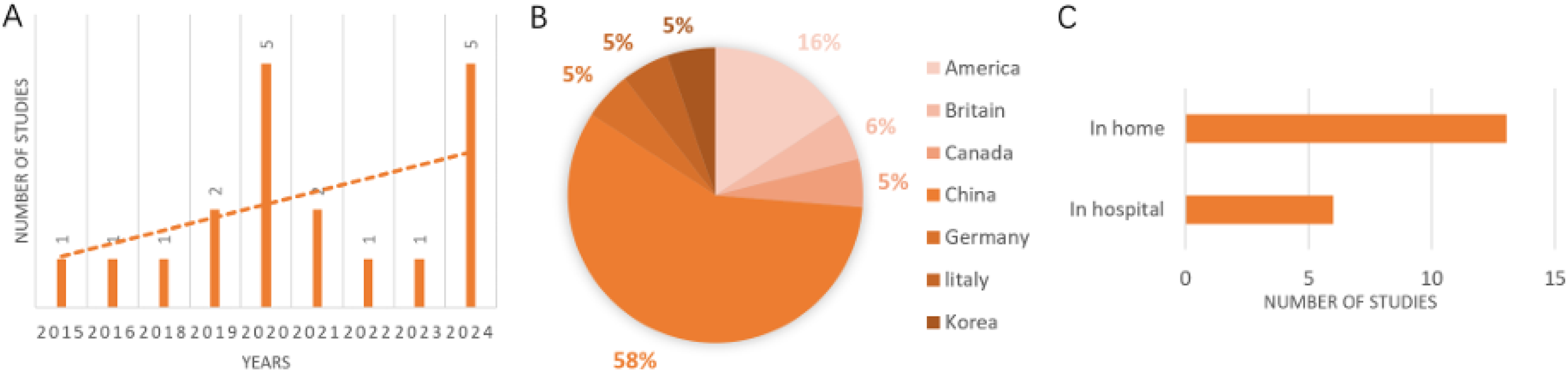
General feature composition diagram. (A) Bar chart of virtual community research trends; (B) study the national pie chart; and (C) application environment bar chart.
Quality assessment
Among the RCTs, one study was classified as “good” and the remaining 12 as “fair” in methodological quality. Additionally, four studies were designated “High value” and two “Fair value.” The overall quality of the included literature was deemed acceptable, with no studies excluded based on these standards. Detailed assessment criteria are provided in Supplemental Appendix S6.
Virtual community platform
This study details the primary platforms and application contexts of virtual communities utilized by patients with lung cancer, as summarized in Table 1.
Virtual community platform.
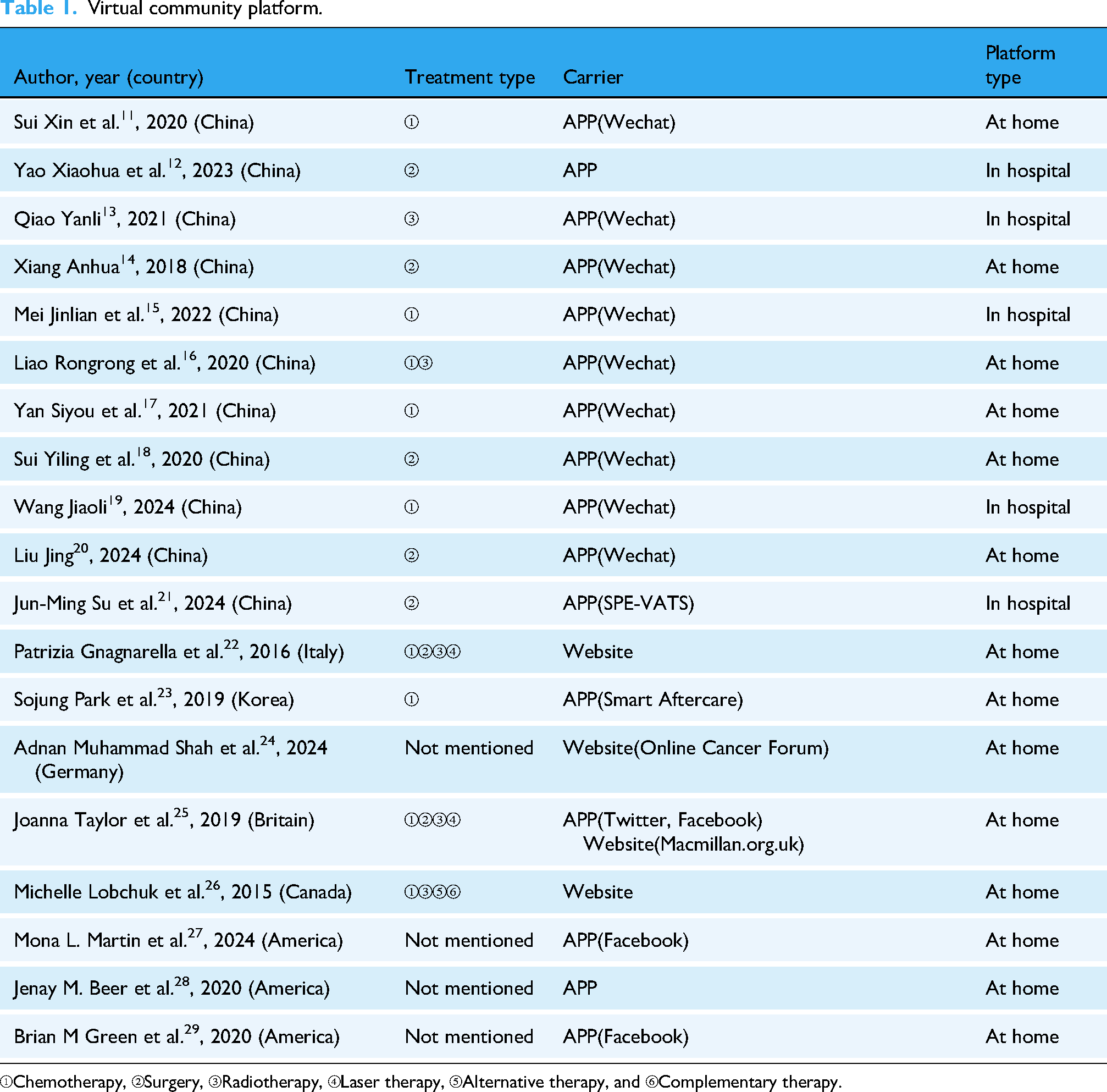
①Chemotherapy, ②Surgery, ③Radiotherapy, ④Laser therapy, ⑤Alternative therapy, and ⑥Complementary therapy.
Virtual community functions
Functions of virtual communities, as derived from screening results, are presented in Table 2.
Virtual community function.

Virtual community effectiveness
The effectiveness of virtual communities is summarized in Tables 3 and 4.
Clinical effectiveness of virtual communities.

P1: experimental group; P2: control group; A: rehabilitation knowledge cognition; B: compliance; C: adverse reactions; D: early postoperative time out of bed; E: thoracic drainage retention time; F: urinary catheter retention time; G: length of stay; H: negative emotion; I: self-management efficacy; J: satisfaction; K: quality of life; L: cancer fatigue; M: mental resilience; N: nutritional status; NSCLC: non-small cell lung cancer; O: rehospitalization time; P: treatment cost; Q: loss of follow-up rate; R: survival situation; RCT: randomized controlled trial; S: pain; T: 6MWT.
Psychosocial and supportive benefits of virtual communities.

Tips: P3: Total posts.
NSCLC: non-small cell lung cancer; RCT: randomized controlled trial; PANAS: Positive and Negative Affect Scale; SUPPH: Strategies Used by People to Promote Health; SPE-VATS: scenario-based PE web app for lung tumor patients undergoing VATS; PFS: Piper Fatigue Scale; SAS: Self-Rating Anxiety Scale; 6MWD: 6-min walking distance; SDS: Self-Raring Depression Scale.
Virtual communities function as a critical conduit for patient support, primarily mediated through two modalities: mobile applications and web-based health forums. Each platform offers distinct advantages, facilitating convenient access to information, support, and interactive engagement for patients.
Apps: Mobile applications, particularly those integrated with social platforms like WeChat, have been widely adopted in several studies.11–21 These apps offer convenience and accessibility, allowing patients to obtain information, support, and engage in interactions at any time and from anywhere. The mobility and user-friendly interface of apps make them a popular choice for patients seeking real-time engagement with their virtual community.
Websites: Studies22–25 have utilized online forums and cancer-specific websites as platforms for virtual communities. These websites often provide a wealth of resources, professional guidance, and a space for patients to seek support and share experiences. The static nature of websites can be advantageous for hosting comprehensive information and facilitating in-depth discussions that may not be as easily managed within a mobile app environment.
Building on these structural foundations, the analysis shows virtual communities offer patients with lung cancer a multifaceted support system addressing diverse needs. All 19 studies reported patients using these platforms for disease-related information acquisition, with 17 specifically focusing on treatment information. Beyond information, 15 studies documented emotional support (e.g. emotional catharsis), and nearly half (9 studies) noted access to psychological counseling. Social connection was prominent: 16 studies described patients forming peer ties and 11 documented online activities strengthening networks. Additionally, 9 studies identified patients utilizing resources for treatment decisions and symptom management, enhancing self-care. Though less common, a minority (6 studies) indicated some patients utilized platforms for advocacy—combating discrimination, promoting equity, and raising awareness.
These functional benefits correspond to positive clinical impacts, as evidenced across multiple studies. The clinical impact of virtual communities on patients with lung cancer is summarized below.
Psychologically, engagement in these platforms is associated with reductions in anxiety, depression, and negative emotions, alongside improvements in self-management efficacy.11,13 Furthermore, involvement in such communities supports greater adherence to treatment regimens,11,17 which remains critical for successful long-term disease management. Collectively, these contributions lead to meaningful improvements in overall quality of life,14,15,22,26 including reduced complication rates and mitigation of the adverse mental states often related to chemotherapy.
Further reflecting the global relevance of these platforms, user interaction patterns within virtual communities exhibit distinct regional variations. German forums demonstrated a pronounced focus on hospice care, underscoring a specific demand for end-of-life support. 24 In the United Kingdom, the functionality of these platforms varied considerably: dedicated forums and groups served as venues for both emotional and informational support, whereas Twitter was utilized predominantly for information dissemination, amid perceptions of an overall deficit in lung cancer-specific resources. 25 By contrast, online forums in North America—including those in Canada and the United States—fostered highly supportive environments that facilitated the sharing of emotional experiences and advanced efforts in lung cancer advocacy. 23 27–29
Discussion
The integration of virtual communities as a support source for patients with lung cancer reflects their increasing role in the daily lives of individuals managing the disease, especially in home-based care settings, underscoring the growing importance of these platforms in providing continuously accessible supportive care beyond clinical environments. This phenomenon can be attributed to the widespread use of social media platforms, notably applications like WeChat,30,31 which facilitate the exchange of information and emotional support among patients. Within these digital spaces, individuals are afforded the opportunity to acquire knowledge, disseminate their treatment experiences, and obtain psychological solace, all within the confines of their home care setting. This model caters to the demand for accessible information and home-based care, while also embodying the spirit of communal support. In the realm of medicine, virtual communities manifest as both applications and websites, each boasting distinct benefits and constraints. For instance, image visualization tools on iOS devices have gained favor among physicians for their ease of use and real-time capabilities. 32 Conversely, websites offer patients a forum for discussion, enriched by a plethora of resources and engaging interactive features. 33
This study integrated 19 articles demonstrating that virtual lung cancer communities confer multifaceted benefits in NSCLC management. Critical appraisal, particularly of the numerous RCTs,11–22 provides robust evidence for efficacy under controlled conditions. Consistent RCT findings reveal that virtual community interventions significantly reduce adverse treatment reactions, 11 shorten hospital stays, 12 enhance treatment compliance,11,14 alleviate anxiety and depression, 13 15–19,21,22 and improve quality of life.14–19,21,23 Replication across independent trials minimizes chance findings and underscores virtual communities as effective supportive interventions. Concurrently, qualitative studies24–29 elucidate mechanisms, illustrating how virtual communities create safe spaces for emotional sharing, 26 facilitate peer information exchange,25,27,29 and foster empowerment and community.28,29 This mixed-methods evidence base thus establishes not only virtual community efficacy but also its mechanisms and beneficiary populations.
Moreover, virtual communities demonstrate stage-specific value across the lung cancer care trajectory. At diagnosis, they mitigate uncertainty and enhance self-advocacy through shared experiences and encouragement.24,27 During active treatment, they provide real-time side-effect management support, improve adherence, and promote adaptability via professional guidance and peer interaction.12,13,17 In rehabilitation, they sustain healthy behaviors, enhance nutritional knowledge and practices,20,22 and support psychological adjustment. 16 For advanced-stage and palliative patients, as well as caregivers, virtual communities deliver critical emotional solace, practical nursing guidance, and reduce isolatio,24,26,29 exemplified by caregiver testimonials 29 : “I am caring for my husband who is in advanced stages. It is coming more apparent that he will lose the battle due to respiratory issues…Reading your entries reminds me that others have gone before me as caregivers for this disease that these issues.” While evidence indicates improvements in quality of life, compliance, and social connectedness, 18 their impact on survival remains limited. 18 Outcomes vary, with only modest behavioral changes, 27 differential anxiety reduction—particularly among women and highly educated patients 21 —and persistent resource support gaps relative to other malignancies. 25 These mixed results underscore the imperative for further research to optimize virtual community design, enhance generalizability beyond Chinese populations, and maximize tangible benefits in NSCLC management.
Virtual communities offer numerous benefits, yet they confront significant challenges. The dissemination of accurate information is paramount. Unsubstantiated content, such as personal anecdotes or alternative therapies, may mislead patients and adversely affect their health. 25 The proliferation of unverified medical information poses a particular challenge, as laypersons often struggle to discern what is reliable, potentially leading to misguided medical decisions. 34 Privacy and security are of utmost importance. When individuals share sensitive health data, inadequate handling can result in privacy violations, harassment, and fraud. 26 Robust community regulations and explicit privacy protocols are essential to safeguard personal information. Negative emotions within virtual communities can also detrimental to the mental health of their members. Although it is normal for communities to experience periods of despair or fear, excessive negativity can foster a sense of anxiety and depression among participants. 26 Striking a balance between emotional support and positive interactions is critical for fostering a healthy virtual community.
Limitations
This review is constrained to studies published in Chinese and English, potentially omitting insights from other linguistic domains and compromising the generalizability of the results. Subsequent research ought to broaden its linguistic scope to encapsulate a more inclusive array of global perspectives. It is crucial to acknowledge that the preponderance of included studies were observational, which constrains our capacity to infer causal links between virtual communities and patient outcomes. The indications of benefits, such as enhanced access to information and social support, should be approached with prudence, given the intrinsic limitations of observational data. Future inquiries should give precedence to longitudinal or experimental designs with controls to more stringently evaluate causality and fortify the empirical foundation.
Conclusion
Online communities have demonstrated considerable promise in aiding patients with lung cancer by offering access to information, emotional support, opportunities for social engagement, assistance with treatment decisions, and advocacy for their rights and interests. While these platforms enhance treatment adherence and social interaction, their impact on survival rates remains limited, and challenges such as misinformation, privacy concerns, and negative emotional dynamics persist. Current research is constrained by linguistic limitations and a reliance on observational studies, highlighting the need for more rigorous, longitudinal investigations. Addressing these gaps can help optimize virtual communities to provide safer, more effective, and inclusive support for patients globally.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251395985 - Supplemental material for Virtual communities for patients with lung cancer: A scoping review of support types, effectiveness, and emerging challenges
Supplemental material, sj-docx-1-dhj-10.1177_20552076251395985 for Virtual communities for patients with lung cancer: A scoping review of support types, effectiveness, and emerging challenges by Benxiang Zhu, Le Zhang, Dongmei Mao, Yuanyuan Luo, Zhihui Yang, Jingxia Miao and Lili Zhang in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251395985 - Supplemental material for Virtual communities for patients with lung cancer: A scoping review of support types, effectiveness, and emerging challenges
Supplemental material, sj-docx-2-dhj-10.1177_20552076251395985 for Virtual communities for patients with lung cancer: A scoping review of support types, effectiveness, and emerging challenges by Benxiang Zhu, Le Zhang, Dongmei Mao, Yuanyuan Luo, Zhihui Yang, Jingxia Miao and Lili Zhang in DIGITAL HEALTH
Supplemental Material
sj-pdf-3-dhj-10.1177_20552076251395985 - Supplemental material for Virtual communities for patients with lung cancer: A scoping review of support types, effectiveness, and emerging challenges
Supplemental material, sj-pdf-3-dhj-10.1177_20552076251395985 for Virtual communities for patients with lung cancer: A scoping review of support types, effectiveness, and emerging challenges by Benxiang Zhu, Le Zhang, Dongmei Mao, Yuanyuan Luo, Zhihui Yang, Jingxia Miao and Lili Zhang in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076251395985 - Supplemental material for Virtual communities for patients with lung cancer: A scoping review of support types, effectiveness, and emerging challenges
Supplemental material, sj-docx-4-dhj-10.1177_20552076251395985 for Virtual communities for patients with lung cancer: A scoping review of support types, effectiveness, and emerging challenges by Benxiang Zhu, Le Zhang, Dongmei Mao, Yuanyuan Luo, Zhihui Yang, Jingxia Miao and Lili Zhang in DIGITAL HEALTH
Supplemental Material
sj-docx-5-dhj-10.1177_20552076251395985 - Supplemental material for Virtual communities for patients with lung cancer: A scoping review of support types, effectiveness, and emerging challenges
Supplemental material, sj-docx-5-dhj-10.1177_20552076251395985 for Virtual communities for patients with lung cancer: A scoping review of support types, effectiveness, and emerging challenges by Benxiang Zhu, Le Zhang, Dongmei Mao, Yuanyuan Luo, Zhihui Yang, Jingxia Miao and Lili Zhang in DIGITAL HEALTH
Supplemental Material
sj-docx-6-dhj-10.1177_20552076251395985 - Supplemental material for Virtual communities for patients with lung cancer: A scoping review of support types, effectiveness, and emerging challenges
Supplemental material, sj-docx-6-dhj-10.1177_20552076251395985 for Virtual communities for patients with lung cancer: A scoping review of support types, effectiveness, and emerging challenges by Benxiang Zhu, Le Zhang, Dongmei Mao, Yuanyuan Luo, Zhihui Yang, Jingxia Miao and Lili Zhang in DIGITAL HEALTH
Footnotes
Ethics approval
A scoping review not involves human subjects, human material, human tissues or human data. Therefore, the approval of an ethics committee was not necessary.
Contributorship
BXZ was involved in writing original draft, resources, and data curation; LZ in writing review & editing, resources, and data curation; DMM, YYL, and ZHY in resources and data curation; JXM in methodology; and LLZ in supervision, methodology, and funding acquisition. BXZ, LZ, and DMM completed the literature search and screening. BXZ completed the manuscript. JXM and YYL were responsible for contacting practice agencies; ZHY and LLZ conceptualized and designed the study. All authors critically reviewed the manuscript and approved the final manuscript. BXZ and LZ contributed equally to this work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant number 72374097).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.