
Abstract
Objectives
With the advancement of digital technologies, digital health-supported physical activity has attracted considerable attention for its potential to enhance cognitive function in older adults. To systematically review the research progress and trends in this field, this study utilized CiteSpace 6.3 R2 for bibliometric analysis of relevant literature.
Methods
Publications were retrieved from the Web of Science Core Collection and Scopus databases, and after screening and merging, a total of 201 publications were included for analysis. CiteSpace 6.3 R2 was used to conduct bibliometric analysis from dimensions such as keyword, country, and institution.
Results
The annual publication counts showed an overall increasing trend, with Frontiers in Aging Neuroscience having the highest number of publications, and the coverage of the two databases being partially overlapping yet complementary. Co-occurrence analysis revealed that the United States, Harvard Medical School, and Eling D. De Bruin were the most active at the national, institutional, and author levels. In terms of co-citation analysis, Frontiers in Aging Neuroscience, “Unknown,” and Ying-Yi Liao (2019) had the highest citation frequencies across journals, authors, and references. High co-occurrence keywords included “virtual reality,” “older adults,” and “exercise.” Keyword clustering revealed major clusters such as “rct,” “multiple sclerosis,” and “digital health,” with recent burst keywords including “age,” “care,” “digital health,” and “physical exercise.”
Conclusion
Research in this field is rapidly advancing, showing a clear trend toward multidisciplinary integration. Collaboration networks have formed across regions, institutions, and authors, but remain relatively fragmented. Core journals, influential authors, and highly cited publications have collectively shaped the foundational knowledge base of the field. Recent studies have focused on integration models and collaborative mechanisms between digital health technologies and physical activity. Future research should emphasize interdisciplinary and international collaboration, prioritizing the development of personalized, real-world-oriented digital health interventions to enhance the quality of life for older adults.
Keywords
Introduction
Cognitive function encompasses a suite of higher-order mental processes involved in knowledge acquisition, information processing, and reasoning-based decision-making in humans. Rather than being a single ability, it represents a complex system arising from the interplay among multiple subdomains, including perception, memory, attention, language, and executive function. 1 Collectively, these processes enable learning, adaptation, and social interaction in everyday life. Cognitive performance naturally declines with advancing age. While the modest decline is considered a normative feature of aging, reductions that exceed this expected range may progress to mild cognitive impairment (MCI) or neurodegenerative disorders such as Alzheimer's disease. 2 Cognitive deterioration not only compromises information-processing efficiency and the execution of daily activities but also precipitates emotional disturbances, social withdrawal, and loss of independence, thereby markedly diminishing quality of life and social functioning. 3 Among older adults, this decline significantly increases dependency and care needs, posing a major public health concern.
A substantial body of research suggests that regular physical activity can help delay cognitive decline and promote cognitive health.4–6 In 2018, the World Health Organization (WHO) published the Global Action Plan on Physical Activity 2018–2030, which aims to reduce the global proportion of adults engaging in insufficient physical activity by 15% by 2030 7 ; however, the most recent surveillance data (2024) reveal that the proportion of adults aged ≥ 60 years who are insufficiently active continues to rise. 8 Insufficient physical activity is recognized as a major public health challenge worldwide, contributing to the burden of non-communicable diseases and premature mortality. 9 The global healthcare costs attributable to physical inactivity are estimated to exceed 50 billion USD annually, of which approximately 30 billion USD are borne by the public sector. 10 In addition to well-documented associations with cardiovascular disease, type 2 diabetes, and depression, insufficient physical activity has been linked to accelerated cognitive decline and an increased risk of dementia. 11 These multifaceted health and economic consequences highlight the urgency of scaling up effective and accessible interventions to increase physical activity among older adults.
The rapid evolution of digital health technologies presents novel opportunities for promoting physical activity among older adults. Wearable sensors, mobile health (mHealth) applications, and virtual–reality-based exergaming transcend temporal and spatial barriers, delivering personalized, readily accessible, and sustainable exercise interventions. These innovations could help close the current gap between observed activity levels and the WHO targets, thereby laying a practical foundation for the broader and more effective promotion of physical activity. 12
Digital health, as a collective term for the application of digital technologies in healthcare, encompasses electronic health and mobile health and extends to areas such as big data, genomics, and artificial intelligence. 13 Physical activity based on these technologies has advantages over traditional methods in terms of integration, personalization, and compliance. 14 Specifically, digital health-based physical activity involves the real-time monitoring, data analysis, and immediate feedback of individual exercise using wearable sensors, mobile applications, virtual or augmented reality, or artificial intelligence. At its core, this novel approach focuses on enhancing the effectiveness and sustainability of physical activity through data-driven and precision management, thereby improving health, delaying functional decline, preventing chronic diseases, and supporting disease recovery.
In recent years, research on digital health-based physical activity and cognitive function in older adults has been steadily increasing. Systematic reviews indicate that eHealth interventions can increase physical activity time, energy expenditure, and step counts in older adults, supporting their inclusion in practice guidelines. 15 Wearable-based interventions are generally acceptable to this population and yield small but significant physical activity gains, suggesting scalability for population-level health promotion. 16 Specifically at the level of cognitive function, reviews and meta-analyses report that digital or home-based physical activity programs can improve cognitive performance, and that exergame-based training produces measurable benefits in global cognition—particularly among individuals with MCI or dementia—with longer training durations associated with greater effects.17,18 Moreover, digital technologies enable continuous, objective monitoring of habitual PA patterns, facilitating precision assessment and tailored behavior modification in dementia and MCI populations. 19 However, there remains a lack of systematic reviews and quantitative integration in this area, which to some extent hinders a comprehensive understanding of overall development trends and research frontiers. Therefore, a systematic approach is needed to thoroughly analyze the existing literature. Bibliometric analysis is a widely recognized method for identifying research focus, examining knowledge structures, and mapping the field's evolutionary trajectory. 20 By integrating publication statistics, co-occurrence analysis, co-citation analysis, and keyword distribution, bibliometric analysis enables a comprehensive synthesis of existing research and reveals the knowledge base as well as future research directions.
This study employed CiteSpace (version 6.3.R2) to conduct a bibliometric analysis of the scholarly literature on digital health-based physical activity and cognitive function in older adults. Specifically: (1) annual publication counts, journal sources, and database sources were quantified to reveal developmental trends in the field; (2) multi-level collaboration networks—across regions, institutions, and authors—were constructed to systematically examine global research linkages; (3) journal, author, and reference co-citation networks were analyzed to map the field's intellectual foundation; (4) keyword co-occurrence, clustering, and burst analyses were conducted to identify research focus, thematic structures, and emerging trends; and (5) these findings were integrated to develop an overarching knowledge framework, synthesize primary research focus, and outline directions for future inquiry.
Material and methods
This study followed the “Preliminary guideline for reporting bibliometric reviews of the biomedical literature (BIBLIO)” (Supplementary Material 1) for its writing. 21
Data collection
This study employed the Web of Science Core Collection (WoSCC) and Scopus databases as primary data sources for the bibliometric analysis. Both databases offer broad, multidisciplinary coverage across the natural sciences, medical and health sciences, engineering, and technology, and are widely recognized worldwide as the most comprehensive bibliometric data sources.22,23 They also provide structured cited-reference metadata required for citation-dependent analyses (e.g., co-citation). Given the inherently multidisciplinary scope of our topic, spanning sport science, computer science, and neuroscience, we selected multidisciplinary sources to ensure comprehensive and comparable coverage. In contrast, PubMed focuses on the life and biomedical sciences, provides limited coverage of computer science and sport science, and does not provide the cited-reference metadata needed to build robust citation networks.24,25 Including PubMed would therefore risk introducing disciplinary bias and limiting the feasibility and reproducibility of our citation-based analyses. Consistent with current practice in bibliometrics, where most studies use WoSCC or Scopus and an increasing number adopt a dual-database design,26,27 we therefore employ a dual-database approach (WoSCC and Scopus) to balance coverage, data quality, and methodological fit.
The quality of a literature search strategy plays a critical role in determining the effectiveness of bibliometric analysis. Drawing on prior studies and recognizing that major databases implement different rules for stemming/lemmatization and phrase handling, we balanced precision and recall by uniformly using quoted exact matches (“word”) and explicitly enumerating common lexical variants to reduce the risk of missed records.28,29 In this study, the search strategy was initially developed by the research team through internal discussions to form a preliminary plan and was subsequently refined through two rounds of peer review before finalization (Supplementary Material 2). The strategy was structured around four core themes: (1) digital health (e.g., digital health, wearable devices, virtual reality, etc.); (2) physical activity (e.g., exercise, physical activity, sports, etc.); (3) older adults (e.g., older adults, elderly, seniors, etc.); and (4) cognitive function (e.g., cognitive function, memory, executive function, etc.). Boolean operators were used to combine the key terms to ensure the search was both systematic and comprehensive. Given the continuous evolution of the concept of “digital health” alongside the rapid development of the Internet and information technology since the early 21st century, 30 the search timeframe was set from 2000 to 2024 to ensure comprehensive coverage of relevant literature.
Data screening
After implementing the search strategy, a total of 1587 publications were retrieved from the WoSCC and 5621 publications from Scopus. An automated initial screening was then conducted within each database to exclude non-peer-reviewed or informal publications, such as conference papers, preprints, and editorials, resulting in 1421 publications in WoSCC and 4926 publications in Scopus. Non-English publications were subsequently removed, leaving 1395 and 4840 publications in the respective databases. A further evaluation was performed based on publication type, research topic, source reliability, and document completeness (Supplementary Material 3). This stage involved two researchers independently reviewing all retrieved publications, with any disagreements resolved by a third researcher to reach consensus. Following this screening process, 132 publications from WoSCC and 136 publications from Scopus were retained.
Before merging the datasets, the relevant information was standardized to address formatting differences between the two databases. This process included correcting author names containing special symbols or garbled characters, unifying the formatting of country/region information for the same country, and standardizing institutional names by simplifying multi-level affiliations to their primary institution. The standardized datasets were then imported into CiteSpace for merging, during which 67 duplicate publications were removed. Ultimately, 201 publications were retained for analysis. Figure 1 illustrates the overall screening procedure. This final sample size satisfies the minimum threshold typically required for robust bibliometric analysis.31–33
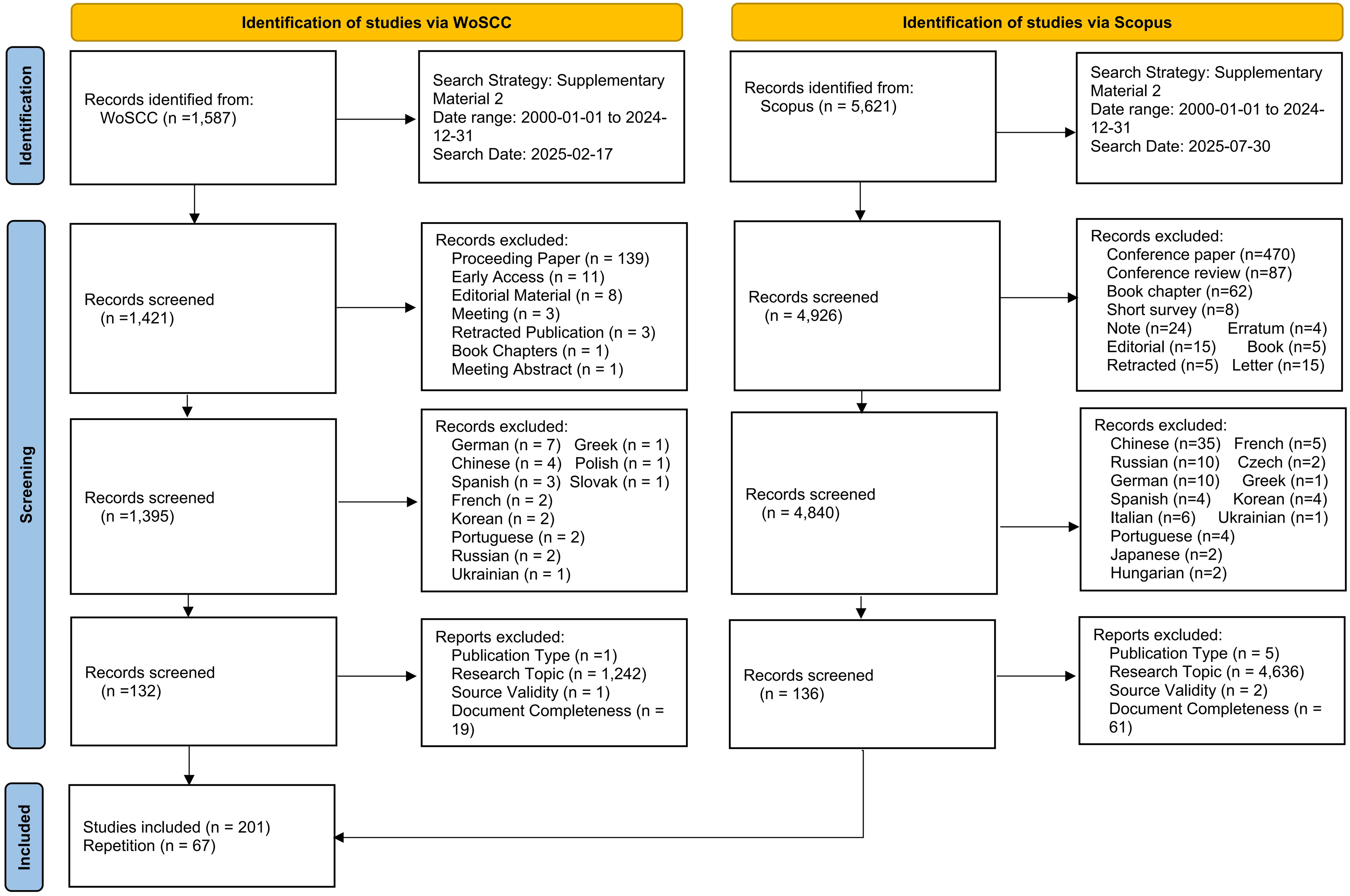
Flow diagram of publication screening process.
Analysis methods and tools
This study employed CiteSpace (version 6.3 R2) to perform the bibliometric analyses. Owing to its capacity for visualizing results, algorithmic objectivity, and systematic analytical framework, CiteSpace has become a widely adopted platform in bibliometric scholarship. The software enables a comprehensive depiction of the intellectual landscape and temporal evolution of a given research domain. 34 Moreover, its automated workflows enhance analytical efficiency, minimize subjective bias, and improve the methodological rigor and interpretability of the resulting findings. 35
The specific software parameter settings for the analysis are as follows: the time slice ranges from January 2000 to December 2024, with a slice interval of 1 year; node selection criterion adopts the g-index (k = 25); node types include author, institution, country, keyword, and reference; all other parameters are kept at their default values.
Results
Publication statistics
Publication counts by annual
The annual number of publications provides a straightforward indicator of scholarly interest in this research area. As shown in Figure 2, the overall trajectory is upward, with only minor fluctuations from year to year. From 2011 to 2017, the annual publication count remained in the single digits, reflecting modest growth. It first exceeded ten in 2018 (16 publications) and has since consistently remained in double digits, with peaks observed in 2021 and 2024, underscoring the field's sustained growth and increasing academic prominence.

Annual number of publications (2011–2024).
Publication counts by journal
Publications in this field are published in 113 journals. Table 1 lists the top five journals ranked by publication counts, with a total of 40 publications—19.90% of the total output—indicating a certain degree of concentration in research dissemination. Among them, Frontiers in Aging Neuroscience ranks first with 12 publications (5.97%), while each of the other four journals has seven publications (3.48%). Additionally, all five journals are indexed in both WoSCC and Scopus, and most have relatively high JIF and CiteScore values, ranking in the Q1 quartile, except for BMC Geriatrics, which is ranked in Q2 based on its CiteScore.
Top five journals by publication counts.

Note: JIF values are from Journal Citation Reports 2024, and CiteScore values are from Scopus 2024. Quartile refers to the highest quartile ranking among the journal's subject categories.
Publication counts by database search
As shown in Figure 3, a total of 201 publications were retrieved, of which 67 were indexed in both databases, accounting for approximately one-third of the total. Scopus exclusively retrieved 69 publications (50.7% of its total), while WoSCC exclusively retrieved 65 publications (49.2% of its total).

Number of publications in Scopus and WoSCC databases.
Co-occurrence relations
Country/region co-occurrence
The country/region co-occurrence map comprises 45 nodes and 128 edges (Figure 4), illustrating the collaborative network structure among different countries/regions. Table 2 presents the top five countries based on collaborative publication counts, with representation from the Americas, Asia, and Europe. The United States ranks first as the most active country in collaboration, with 49 co-authored publications and an intermediary centrality of 0.44. China follows with 26 publications and a centrality of 0.01. Among the remaining countries, Italy (21 publications), South Korea (19 publications), and Brazil (15 publications) show notable research activity, with Italy also exhibiting a relatively high centrality of 0.14.
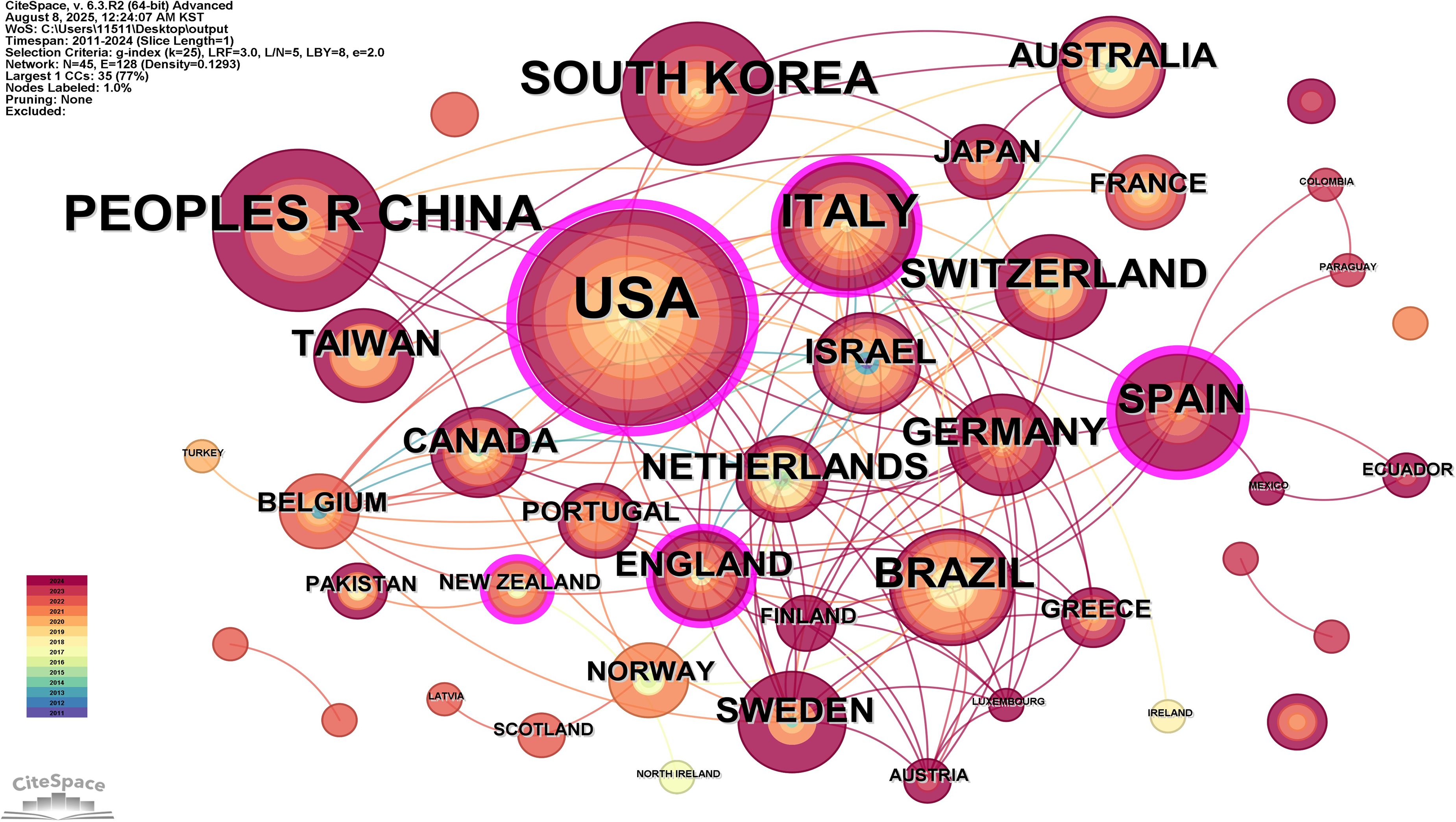
Country/region co-occurrence map.
Top five countries/regions by collaborative publication counts.

Institutional co-occurrence
The institutional co-occurrence map consists of 225 nodes and 328 edges (Figure 5), effectively visualizing the collaboration network among research institutions. Table 3 lists the top five institutions in terms of collaborative publication counts. The institution with the highest number of collaborative publications is the Harvard Medical School, with a total of 7. Close behind are the Karolinska Institutet and Tel Aviv University, each with six collaborative publications. The Swiss Federal Institute of Technology has five collaborative publications, while the remaining six institutions each have 4. In terms of intermediary centrality, Harvard Medical School has the highest value at 0.07, followed by Tel Aviv University and Monash University, each with a value of 0.06, which are relatively higher than those of other institutions.

Institutional co-occurrence map.
Top five institutions by collaborative publication counts.
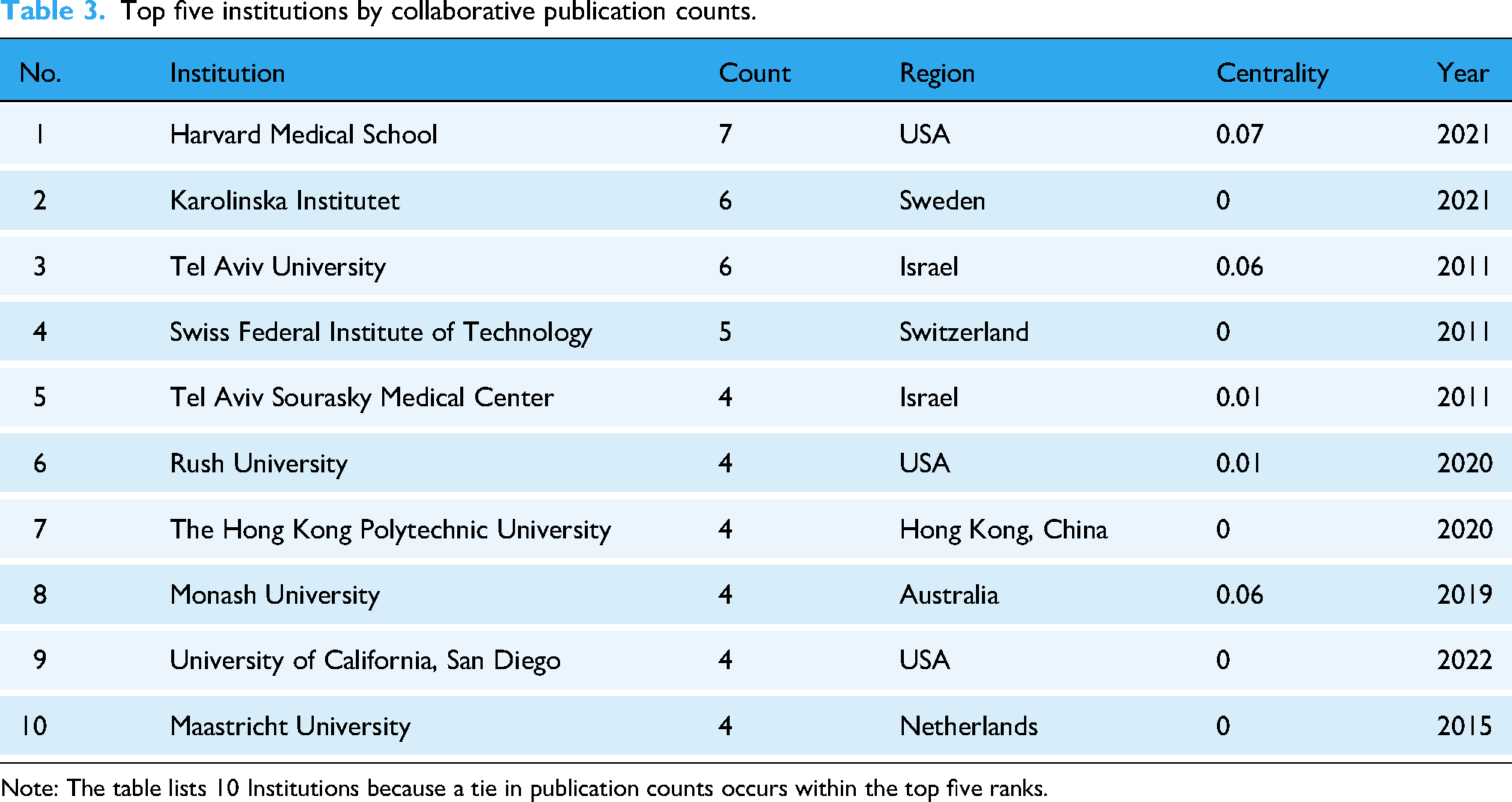
Note: The table lists 10 Institutions because a tie in publication counts occurs within the top five ranks.
Author co-occurrence
The author co-occurrence map consists of 283 nodes and 506 edges (Figure 6). Table 4 lists the top five authors in terms of collaborative publication counts. Eling D. De Bruin ranks first with eight collaborative publications, making him the most active collaborative author in the field. Renato Sobral Monteiro-Junior follows in second place with five collaborative publications. The other four authors have all collaborated on four publications each. It is worth noting that the intermediary centrality of these authors is 0, indicating that they do not occupy a central position connecting different research groups within the collaborative network.
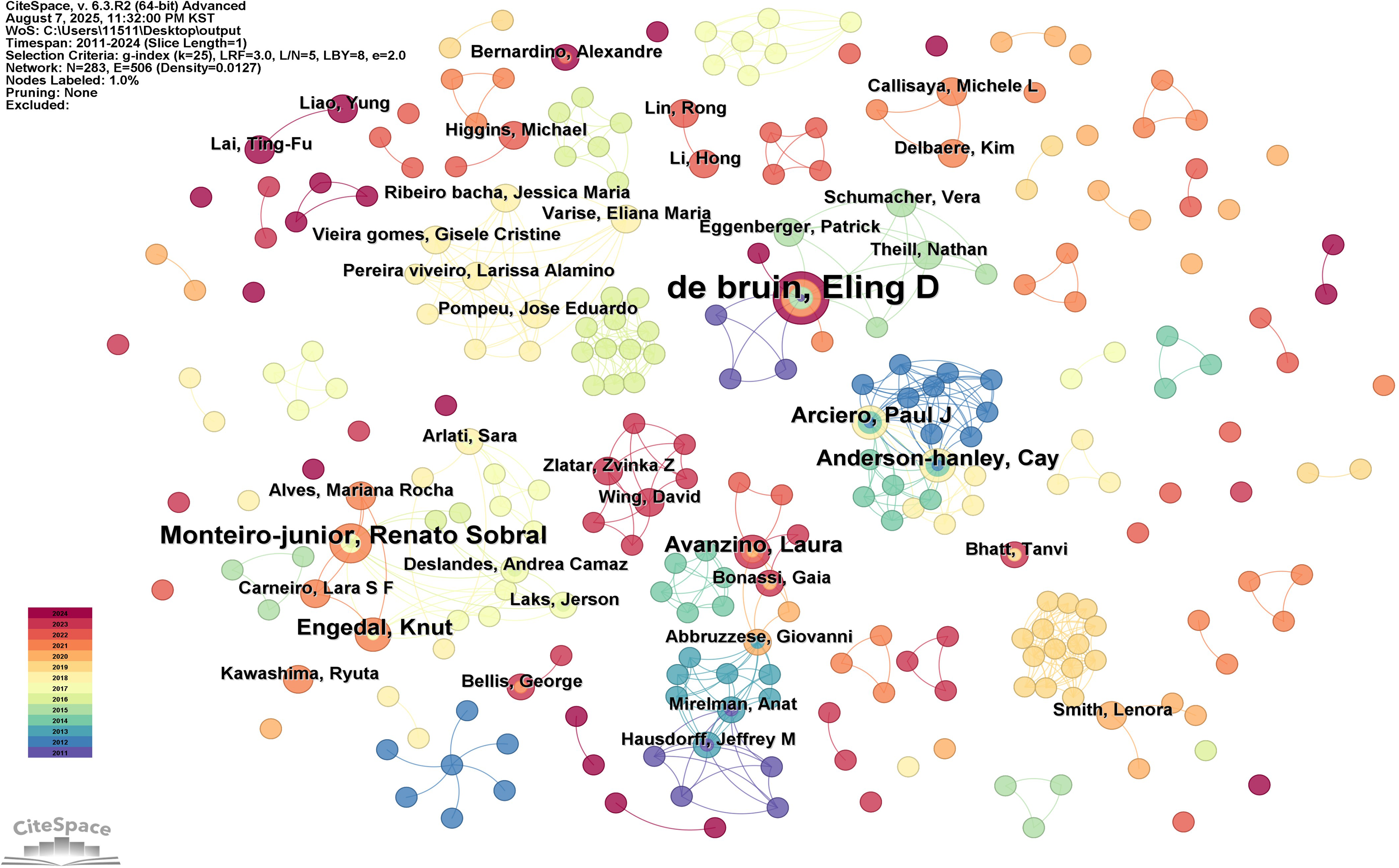
Author co-occurrence map.
Top five authors by collaborative publication counts.
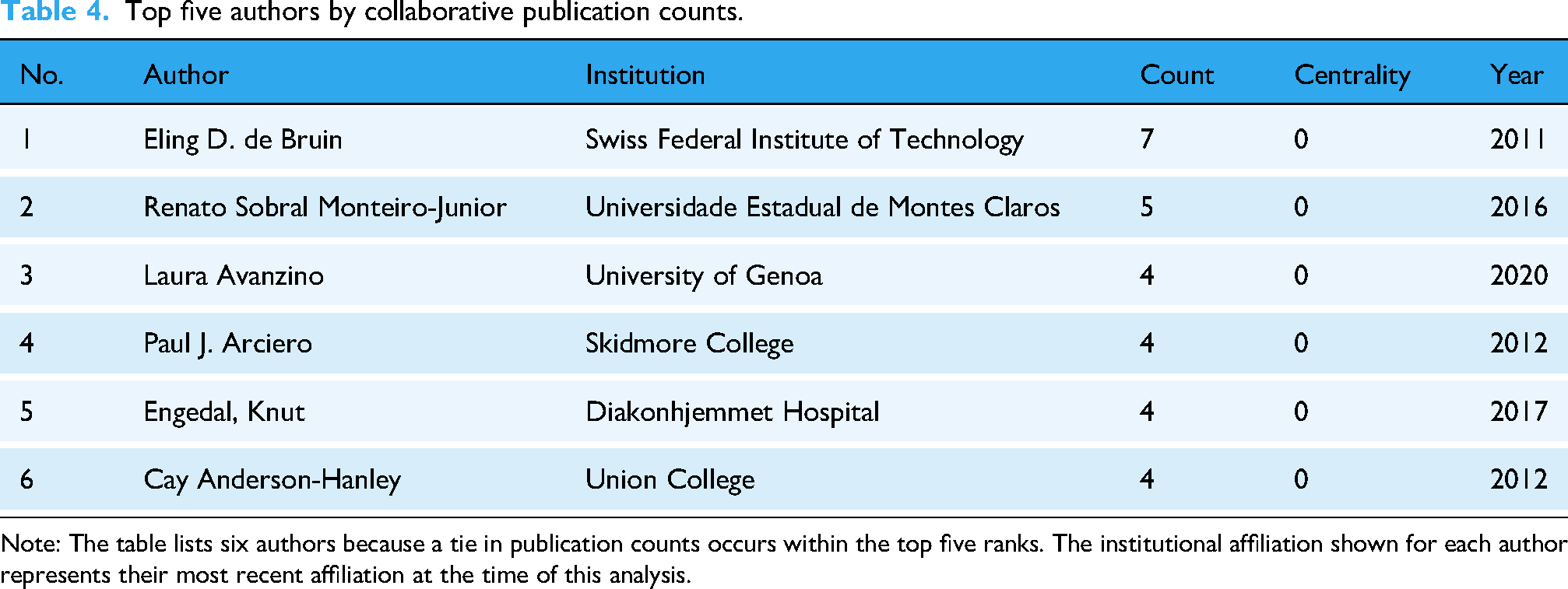
Note: The table lists six authors because a tie in publication counts occurs within the top five ranks. The institutional affiliation shown for each author represents their most recent affiliation at the time of this analysis.
Co-citation relations
Journal co-citation
Figure 7 displays the co-citation network of journals, revealing eight main clusters comprising a total of 354 nodes and 2888 edges. Table 5 lists the top five most frequently co-cited journals. Frontiers in Aging Neuroscience and Journal of the American Geriatrics Society each have 96 co-citations, ranking jointly first, followed closely by PLOS ONE with 94 co-citations. BMC Geriatrics has the highest intermediary centrality (0.06) among the listed journals. Most of these journals are in Q1quartile, with BMC Geriatrics being the only one in Q2 according to its CiteScore quartile ranking.
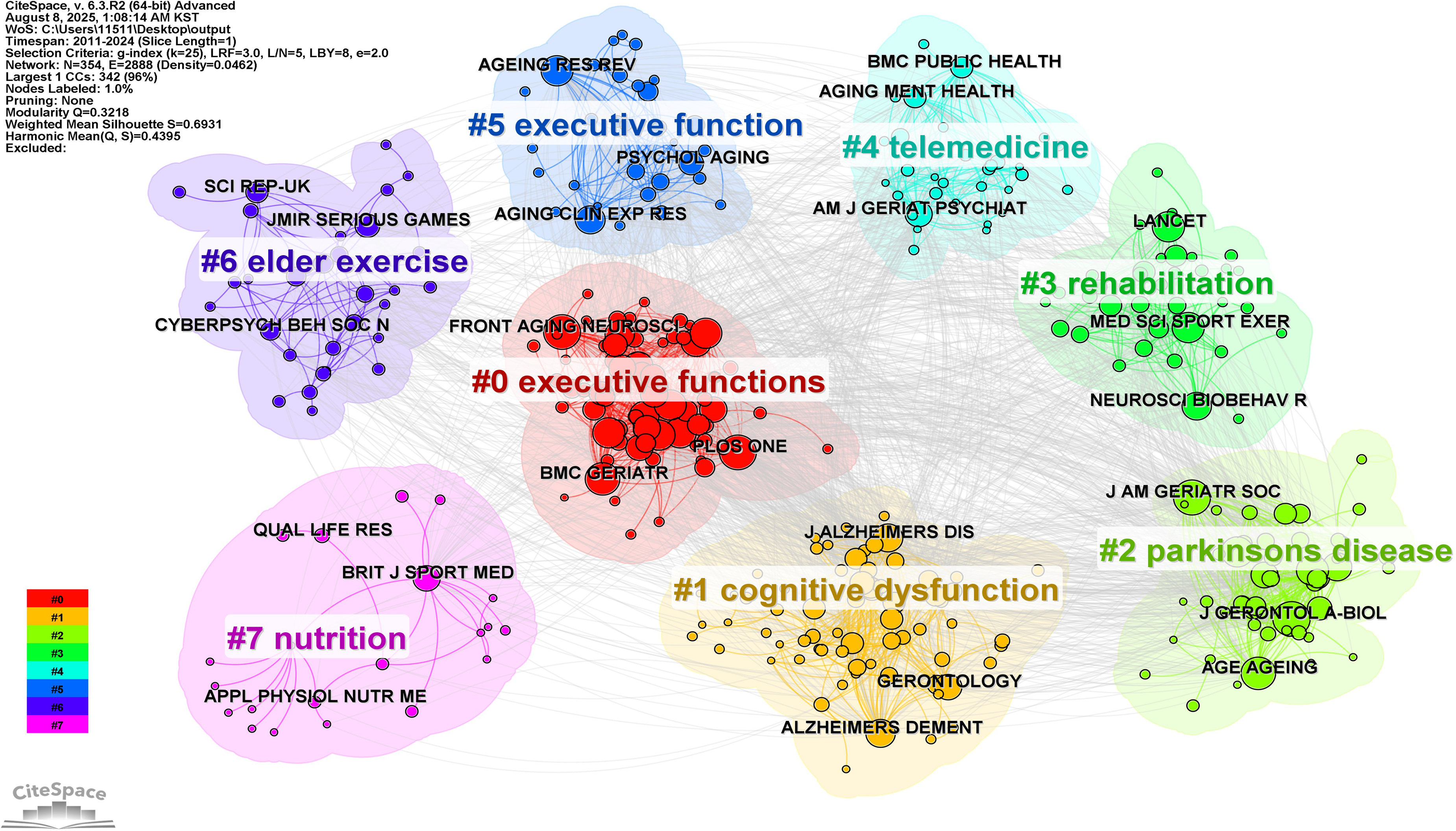
Journal co-cited map.
Top five journals by co-cited frequency.
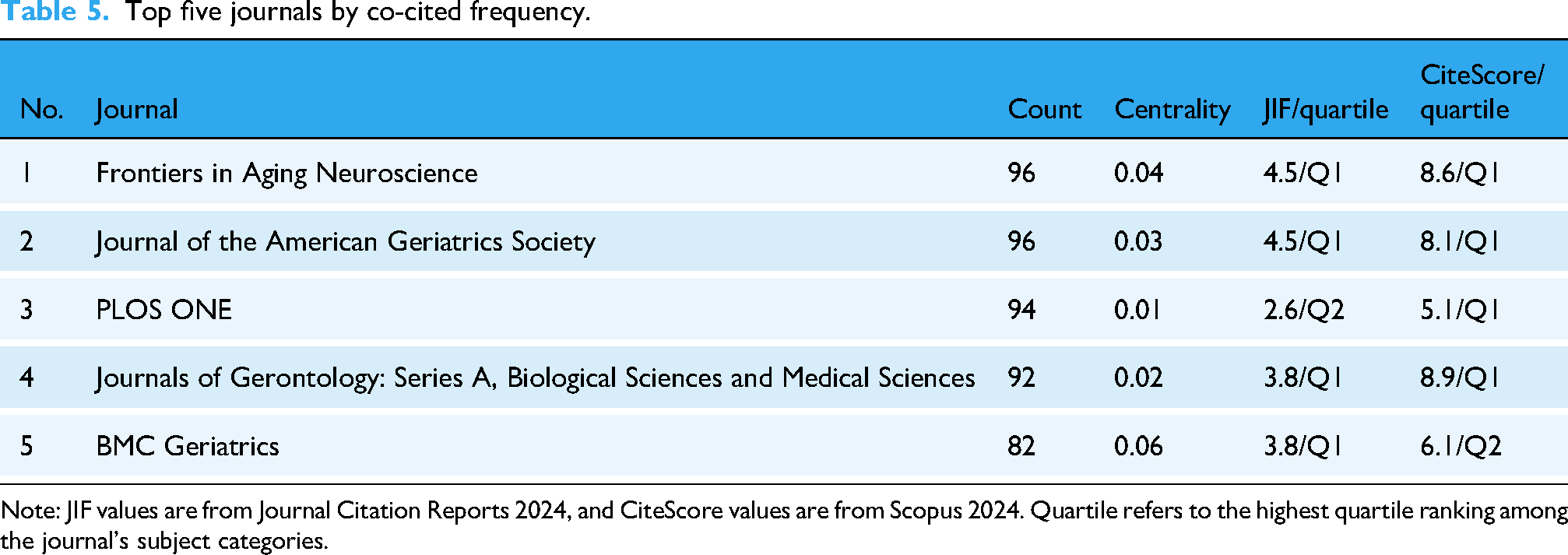
Note: JIF values are from Journal Citation Reports 2024, and CiteScore values are from Scopus 2024. Quartile refers to the highest quartile ranking among the journal's subject categories.
Author co-citation
Figure 8 displays the co-citation network of authors, revealing 14 main clusters comprising a total of 466 nodes and 2111 edges. Table 6 lists the top five most frequently co-cited authors. The “Unknown” node has the highest number of co-citations (n = 73) and intermediary centrality of 0.1. Among the identified authors, Cay Anderson-Hanley and Ying-Yi Liao have the highest number of co-citations (n = 39), with Cay Anderson-Hanley exhibiting the highest intermediary centrality (0.19), indicating a prominent bridging role within the network. Ziad S. Nasreddine and Mirelman Anat follow, with 34 and 29 co-citations and intermediary centrality values of 0.06 and 0.13.

Author co-cited map.
Top five authors by co-cited frequency.

Reference co-citation
Figure 9 displays the co-citation network of references, revealing 12 main clusters comprising a total of 448 nodes and 1742 edges. Table 7 lists the top five most frequently co-cited references. Ying-Yi Liao's two publications (DOI: 10.3389/fnagi.2019.00162; DOI: 10.23736/S1973-9087.19.05899-4) rank first and second, with co-citation frequencies of 22 and 21, respectively. Emma Stanmore (2017) (DOI: 10.1016/j.neubiorev.2017.04.011) and Anat Mirelman (2016) (DOI: 10.1016/S0140-6736(16)31325-3) follow closely, each with 17 co-citations. Notably, these two publications exhibit the highest (0.10) and lowest (0.00) intermediary centrality values.

Reference co-cited map.
Top five references by co-cited frequency

Keyword distribution
Keyword co-occurrence
Table 8 displays the top 10 keywords by co-occurrence frequency. “Virtual reality” has the highest frequency (n = 87) and an intermediary centrality of 0.04. “Older adults” (n = 78) and “exercise” (n = 53) rank second and third, reflecting the central focus on target populations and intervention strategies. Although “physical activity” (n = 47) ranks fourth in frequency, its relatively high intermediary centrality (0.14) suggests a significant bridging role across topics. Similarly, “balance” (n = 41, centrality = 0.11) and “Alzheimer's disease” (n = 32, centrality = 0.12) also demonstrate notable connecting functions within the network. Notably, lower-frequency terms such as “risk” (n = 27, centrality = 0.05) and “impairment” (n = 27, centrality = 0.07) contribute to thematic diversity despite their smaller occurrence counts.
Top 10 keywords by co-occurrence frequency.

Keyword clustering
Figure 10 presents the keyword co-occurrence timeline, revealing a total of eight clusters. The earliest clusters, emerging in 2011, include Cluster #1 (“multiple sclerosis”), Cluster #3 (“gait”), and Cluster #4 (“aerobic exercise”). Cluster #2 (“digital health”), Cluster #5 (“cognitive decline”), and Cluster #6 (“accidental falls”) appeared in 2012, while Cluster #0 (“rct”) and Cluster #7 (“mobile health”) began to gradually take shape around 2013–2014. Regarding the activity periods of each cluster, Cluster #4 became inactive after 2020, whereas Clusters #2, #3, and #6 remained active until 2023. The remaining clusters continue to be active, indicating the long-term evolution and ongoing development of research themes in this field.

Keyword cluster timeline.
Keyword bursts
Figure 11 displays the top 25 keywords with the highest burst strength. The results indicate that “executive function” had the highest burst strength (4.57). This is followed by “falls” (strength 2.59) and “stroke” (strength 2.47). In terms of duration, “attention” (2011–2020), “executive function” (2011–2019), and “dual tasking” (2011–2018) rank as the top three. Notably, “age,” “care,” “digital health,” and “physical exercise” remain in a state of ongoing burst, highlighting their continued relevance in current research.

Keyword burst.
Discussion
Knowledge framework
The research results indicate that after more than 10 years of development, the research field of digital health-based physical activity and cognitive function in older adults has gradually formed a diverse and continuously evolving knowledge system. Establishing a comprehensive and intuitive knowledge framework is crucial to help researchers quickly and accurately grasp the core content of this field. This will significantly enhance a systematic understanding of the field and support more efficient and precise future research and innovative practices. Figure 12 presents the knowledge framework of digital health–based physical activity and cognitive function in older adults.

Knowledge framework of digital health-based physical activity and cognitive function in older adults.
The annual publication count in this research field show an upward trend, reflecting the increasing attention from the academic community to this research area. Particularly during the COVID-19 pandemic, the accelerated application of digital health technologies in the health care of older adults has significantly propelled related research, as evidenced by the sharp increase in publications in 2020. 36 The distribution of journals also demonstrates a multidisciplinary integration, with leading journals focusing on neuroscience, geriatrics, public health, and digital health. Most of these journals are in the Q1 quartile, indicating that high-quality publications have a strong attraction for research outcomes in this field, showing that their academic value has been widely recognized. From the analysis of publication counts by database searches, it is evident that the two databases have complementary strengths, and relying on a single database may lead to substantial omissions of relevant literature, potentially introducing retrieval bias. Therefore, the combined use of multiple databases is essential to ensure comprehensive coverage and to enhance the robustness of bibliometric analyses in this field.
Collaboration network analysis reveals that the United States occupies a central hub position, with high intermediary centrality, indicating its leading role in global research collaboration. Although China ranks highly in terms of publication output, its lower centrality suggests that international collaboration remains relatively limited and concentrated. On the other hand, countries like Italy and Brazil, despite having moderate research outputs, serve as bridging entities that connect research efforts from different regions due to their higher centrality. A temporal dimension further uncovers the evolution of the collaboration landscape, showing that the United States were actively engaged in international collaboration as early as 2011, while China rapidly emerged after 2019, with the involvement of emerging countries accelerating the expansion of the collaboration network.
At the institutional level, the field has established a sizable international collaboration network; however, its overall network density remains limited, with core institutions concentrated in a few countries and regions. Notably, Harvard Medical School, Tel Aviv University, and Monash University occupy central positions within the network, playing pivotal roles in resource integration and knowledge dissemination. Such a “core–periphery” structure can enhance research efficiency, yet it may also lead to unequal resource allocation and restrict the participation of peripheral institutions. 37 Several high-output institutions, such as Karolinska Institutet, the Swiss Federal Institute of Technology, and the Hong Kong Polytechnic University, maintain considerable influence in the field but appear to operate within relatively closed collaborative circles, with insufficient cross-regional engagement. Strengthening connections between these institutions from diverse regions and disciplinary backgrounds may foster greater research diversity and stimulate innovation.
At the author level, prolific researchers, while producing a considerable number of collaborative papers, generally exhibit zero centrality, suggesting that collaborations are mainly limited to local teams with low global connectivity. Authors like Eling D. de Bruin, although prolific, have limited centrality, indicating a tendency towards fixed partner collaborations. In conclusion, international collaboration in this field spans multiple countries; however, the overall network remains relatively fragmented. This underscores the importance of fostering deeper collaboration across countries, institutions, and research teams to establish a more cohesive and interconnected global research network.
In the co-citation analysis, highly co-cited journals are predominantly distributed across the fields of geriatrics, neuroscience, public health, and general medicine, with the majority ranked in the Q1 quartile. Their frequent occurrence in co-citation analysis indicates that research in this field extensively draws upon and references high-quality scholarly research outputs, thereby providing a solid knowledge base for subsequent studies. The clustering map reveals a tightly connected core knowledge group centered on research related to executive functions, which extends outward into applied domains such as rehabilitation, physical activity, and nutrition, forming a dense network of scholarly connections. This structure also reflects a clear trend toward interdisciplinary integration, incorporating public health, sports science, nutrition, and digital technology into the research framework, thereby promoting a transition from a single-disease perspective to a comprehensive health management model.
At the author level, highly co-cited authors such as Cay Anderson-Hanley, Ying-Yi Liao, Ziad S. Nasreddine, and Mirelman Anat have made significant contributions in areas including digital interventions, cognitive assessment tool development, and multi-task training.38–41 Their work not only holds substantial influence within their respective domains but also plays a pivotal role in cross-disciplinary knowledge integration. The clustering results reveal that core author groups are densely distributed around themes such as “meta-analysis,” “mild cognitive impairment,” and “dementia,” extending into physical activity domains like “postural balance,” “falls,” and “dancing,” as well as digital technology applications such as “wii-fit nintendo” and “active video game,” reflecting a pronounced trend toward interdisciplinary convergence. Notably, the “Unknown” node exhibited the highest frequency, primarily due to missing or inconsistent author information in reference metadata during database indexing. 42 Variations in name abbreviations, punctuation, and ordering, as well as incomplete metadata for conference abstracts, short communications, and non-English publications, can lead to matching failures. 43 This underscores the direct impact of database indexing quality on analytical outcomes and highlights the need for future research to prioritize metadata quality assessment and careful data source selection to enhance the accuracy of co-citation analyses.
At the reference level, highly co-cited reference encompasses a range of study designs, including randomized controlled trials, meta-analyses, and systematic reviews. Two studies by Liao et al. were the most frequently co-cited, providing a systematic examination of virtual reality–based cognitive and physical training interventions for improving cognitive function in older adults,39,44 thereby laying both the theoretical and empirical foundations for the application of digital technologies in aging research. The meta-analysis by Stanmore et al. synthesized evidence on the effects of exergaming interventions from an evidence-based perspective, 45 with its relatively high intermediary centrality underscoring its role as a pivotal link connecting diverse research themes. Mirelman et al. highlighted the potential of VR-based dual-task training to reduce fall risk, 40 while Lauenroth et al.analyzed the effects of combined physical and cognitive dual-task interventions from a neurophysiological perspective, 46 providing experimental evidence for subsequent mechanistic investigations. The clustering map reveals a tightly connected knowledge group centered on meta-analytic research, extending outward into subfields such as virtual reality, serious games, postural balance, and information technology, thus constructing an interdisciplinary knowledge network.
Keyword co-occurrence, clustering, and burst analyses collectively trace the evolutionary trajectory of the research field over the past decade. Broadly, the focus has shifted from a singular emphasis on “physical activity improving cognition” to a more multidimensional integrative model linking “digital health–physical activity–cognition–quality of life.” The co-occurrence network reveals that intervention modalities (e.g., exercise, virtual reality, physical activity) and target populations (e.g., older adults) constitute central thematic intersections. In addition, terms like “balance,” “dementia,” and “Alzheimer's disease” are positioned at critical nodes within the network, indicating that digital health–based physical activity interventions address not only cognitive enhancement but also the preservation of physical function and the prevention of neurodegenerative conditions.47,48
The temporal evolution of keyword clustering clearly illustrates the progressive development of research themes over time. During the early phase (2011–2012), studies primarily concentrated on “cognitive impairment,” “cognitive function, “ and “aerobic exercise,” often comparing digital health-based physical activity interventions with traditional exercise approaches.38,49 During the mid-term period (2013–2017), research expanded to include interactive and compound modalities, such as “exergames” and “dual-task training.”50,51 From 2018 onward, high-frequency keywords such as “augmented reality” and “information technology” emerged, indicating the increasing integration of digital tools into intervention execution, assessment, and long-term monitoring.52,53
The burst analysis reveals that “executive function” exhibits the highest burst intensity, underscoring that enhancing executive function is a primary objective of digital health–driven physical activity interventions.54,55 “falls” and “stroke” followed closely, indicating that these events are frequently adopted as key functional and health outcome measures in evaluating intervention efficacy.56,57 In terms of burst duration, “attention,” “executive function,” and “dual tasking” maintained prominence over multiple years, highlighting their sustained research value as critical cognitive processes and training strategies. 58 Meanwhile, keywords such as “age,” “care,” “digital health,” and “physical exercise” remain in an ongoing burst state, reflecting a shift in research from singular functional improvement toward broader, integrated goals encompassing elder care, health promotion, and quality-of-life enhancement.59,60
Research focus
Through a comprehensive analysis of publication statistics, co-occurrence relationships, co-citation relations, and keyword distribution, this study delineates the developmental trajectory and emerging research frontiers in the field of digital health-based physical activity and cognitive function in older adults. The prominence of keywords such as “executive function,” “virtual reality,” “aerobic exercise,” and “rehabilitation” underscores the research emphasis on the integration modality of digital health with physical activity and its synergistic mechanisms.
The integration modality of digital health and physical activity can be categorized into four progressive levels: basic monitoring, feedback-driven, interactive engagement, and intelligent intervention. With continuous technological advancements, these systems are evolving from simple data collection and feedback mechanisms toward multimodal, personalized, and intelligent closed-loop intervention frameworks.
As the most fundamental and indispensable component, the monitoring layer performs essential functions such as data collection, behavioral recording, and the perception of individual states. With the widespread adoption of wearable devices and mobile health (mHealth) technologies, the real-time and continuous tracking of older adults’ health behaviors has significantly enhanced the precision and scientific rigor of interventions. For example, one study utilized mHealth wearable devices to monitor participants’ heart rates in real-time, helping them maintain moderate-to-vigorous physical activity (MVPA) during daily exercise, thereby improving both the quality and efficiency of physical activity. 61 Another study combined wearable physiological sensors with mobile monitoring systems to dynamically track stress levels during exercise and cognitive training, proposing an online stress perception and feedback architecture that supported personalized interventions and informed the development of intelligent decision support systems (DSS). 62
Furthermore, smartphone-based applications capable of accurately recording physical activity data have already been widely applied among older adults. 63 Further investigations have integrated such applications with smart wristbands to monitor physical activity and dietary behaviors using multimodal data streams, enabling comprehensive digital tracking and integration of behavioral information. 64 Notably, the monitoring layer now encompasses not only objective sensor data but also subjective self-reports, reflecting a transition in digital health from simple “perception and recording” to more dynamic “evaluation and feedback.” The value of the monitoring layer lies not only in its technological capabilities but also in its foundational role in enabling individualized feedback, constructing personal profiles, and facilitating subsequent interaction and intelligent interventions. As such, it marks a pivotal starting point in the evolution from passive data acquisition to active system response in digital health systems.
The feedback-driven layer functions as a critical bridge between passive monitoring and active intervention. Rather than merely collecting behavioral or physiological data, this layer employs real-time feedback mechanisms to facilitate users’ awareness of their current status and prompt dynamic behavioral adjustments, thereby improving both adherence and intervention effectiveness. For instance, tele-exergame systems offer enhanced visual feedback and remote real-time supervision during exercise, fostering user engagement and a sense of control through a “perception–feedback–adjustment” closed-loop, which improves the continuity and interactivity of interventions and exemplifies the transition from monitoring to motivational feedback. 42 In mHealth interventions targeting autonomous physical activity among older adults, systems are designed not only for real-time heart rate monitoring but also for delivering Just-in-Time (JIT) feedback based on heart rate zones. 61 These systems actively guide users to maintain exercise intensity within the MVPA range, promoting goal-oriented self-regulation. Thus, the system evolves from a passive data collector to an active behavioral regulator that intervenes in real-time during the performance of individual behaviors.
Notably, the VITAAL exergame system utilizes virtual reality platforms coupled with interactive feedback mechanisms to deliver visual guidance and task-specific immediate feedback for older adults with limited mobility. This assists participants in correcting their movements and adjusting rhythms during dynamic training, thereby enhancing both movement quality and user engagement. Embedding feedback into the training process reinforces the behavioral-response connection, serving as a representative example of the feedback-driven layer in digital health applications. 65 Overall, the feedback-driven layer not only facilitates information transmission but also enhances user responsiveness and behavioral goal orientation through the “state recognition–behavioral adjustment–positive reinforcement” pathway. This establishes a critical foundation for implementing subsequent personalized and intelligent intervention layers.
The interactive engagement layer marks a pivotal phase in the transition from passive acceptance of interventions to active user participation and bidirectional interaction. This layer emphasizes deep engagement between technological systems and users, fostering active involvement, multimodal feedback, and seamless integration into daily routines and social contexts among older adults, thereby enhancing the acceptability, enjoyment, and sustainability of interventions. Studies have implemented AI-driven dynamic difficulty adjustment mechanisms in mobile applications by developing serious games infused with entertainment elements tailored to older adults with diverse cognitive levels. 66 These systems significantly boost user motivation and immersive experience, reducing attrition rates. Similarly, the “Quartier Agil” project—grounded in community participation—encourages older adults to engage in smartphone-based, physical, and cognitive training under the supervision of a coach while also autonomously organizing or participating in cognitive stimulation activities (e.g., task-oriented games) via a mobile app. 67 In addition to maintaining physical and cognitive functioning, the intervention fosters digital literacy, social connectedness, and a sense of community belonging. In a recent mHealth trial, interactive engagement was fostered through WhatsApp group support, Samsung Health–based activity tracking with real-time feedback, frequent e-contacts, and brisk walking in familiar community settings, thereby enhancing participation and adherence among older adults with cognitive frailty. 63
Moreover, the COGNIMO platform integrates augmented reality (AR) with home-based dual-task training, offering older users immersive cognitive-motor interactions. 68 Participants engage in tasks that combine physical movement and cognitive processing, with training frequency positively associated with cognitive improvements, indicating high user adherence and engagement. This approach exemplifies the integration of virtual environments into self-directed training, further deepening the convergence of digital technology and health behavior within the interactive engagement layer. Collectively, this layer advances beyond simple user participation by incorporating personal perception, social interaction, motivational incentives, and adaptive system design. It lays a robust foundation for the evolution toward intelligent, autonomous interventions in the next phase of digital health development.
The core of the intelligent intervention layer lies in utilizing multimodal sensing systems and intelligent feedback mechanisms to enable real-time monitoring of individual status, generate personalized intervention pathways, and dynamically adjust strategies. This supports the development of a closed-loop health management system with adaptive capabilities tailored to the needs of older adults. For example, the “Farming” serious game platform incorporates AI-driven personalization tools—such as dynamic difficulty adjustment and relative scoring algorithms—to adapt the intensity of physical and cognitive tasks based on real-time user performance.66,69 These mechanisms significantly enhance the entertainment value and user engagement of the system, thereby improving adherence and demonstrating the real-world feasibility of intelligent technologies in elderly care.
In addition, recent research has integrated AI speakers, radar sensors, and personalized fitness applications to create innovative care service platforms. 70 These systems provide tailored intervention plans based on baseline functional assessments and support the simultaneous optimization of physical activity and cognitive stimulation under intelligent guidance. The integration of multimodal sensing, personalized recommendations, and closed-loop feedback highlights the potential for scalable and effective digital interventions targeting older adults, particularly those living alone. Overall, the intelligent intervention layer transcends the static nature of traditional exercise programs by combining real-time feedback, individualized tailoring, and adaptive decision-making, offering a more precise, responsive, and sustainable digital solution for geriatric health promotion.
The deep integration of digital health with physical activity holds substantial promise for enhancing cognitive health in older adults, with synergistic mechanisms likely operating through multiple physiological and cognitive pathways.
Firstly, the neuroplasticity mechanism is further supported. Among various digital physical activity approaches, virtual reality–augmented cognitive-motor training interventions (VRCMTIs) have shown particular promise for individuals with MCI. Compared to traditional exercise, VRCMTIs—such as virtual cycling—yield greater cognitive improvements, likely due to the enhanced cognitive stimulation and complex neural activation that result from simultaneous engagement in physical and cognitive tasks. 38
During VRCMTI sessions, older adults integrate multimodal sensory inputs (visual, auditory, tactile) to complete demanding tasks in immersive environments. This process engages key executive functions—including task switching, decision-making, and temporal regulation—activating widespread neural networks. As task complexity increases, the dynamic coordination of multiple cognitive systems promotes cognitive transfer and neural reorganization, thereby reinforcing neuroplasticity. 71 Moreover, exergames, including virtual reality–based exercise (VRE), can offer benefits comparable to traditional exercise while adding cognitive engagement through dual-task demands. Interacting with immersive environments requires working memory, planning, inhibitory control, and decision-making, leading to heightened cognitive and sensory stimulation. This stimulation can promote brain adaptations mediated by neurotrophic factors such as BDNF, GDNF, IGF-1, FGF-2, and VEGF, which support neuroplastic processes including neurogenesis, synaptogenesis, and angiogenesis. 72
In addition, exergaming has been linked to the reactivation of prefrontal neurotransmitter systems, particularly cholinergic and dopaminergic pathways, enhancing synaptic plasticity and neural signal efficiency. These neurochemical and structural changes may delay neurodegeneration and sustain cognitive gains. 73 Collectively, these findings highlight that neuroplasticity plays a primary role in mediating the impact of digital health–enabled physical activity interventions on cognitive function.
Secondly, cognitive–sensory integration has emerged as a key mechanism underlying the cognitive benefits of digital health interventions. Compared to traditional physical activity, approaches incorporating augmented reality, interactive technologies, and multimodal feedback offer enriched cognitive stimulation by engaging individuals in simultaneous motor and sensory-cognitive tasks. During such interventions, older adults must process real-time visual, auditory, and tactile information while executing complex functions such as action path planning, rhythm coordination, and sequence control. These integrated demands enhance sustained attention, sensory integration, and executive control.74,75
Evidence suggests that these interventions activate distributed neural networks—particularly in the frontal and parietal cortices and sensorimotor integration regions—by prompting continuous adaptation of motor behavior and cognitive strategies. This neural engagement improves spatial perception, response inhibition, and attentional regulation. 47
In summary, digital health interventions leveraging cognitive–sensory integration pathways extend the cognitive enhancement potential of physical activity by fostering neuroplasticity and reinforcing higher-order cognitive functions. These findings offer a novel theoretical framework for addressing age-related cognitive decline.
Thirdly, emotion and motivation regulation mechanisms play a critical role in the effectiveness of digital health interventions. Regular physical activity enhances emotional well-being in older adults by increasing neurotrophic factors, and improving blood flow to the frontal and hippocampal regions, thereby contributing to cognitive resilience. 76 Integrating virtual reality technology into interventions further amplifies these effects by providing immersive environments and real-time feedback, which increase emotional engagement and adherence—key factors often lacking in cognitively impaired older adults. 39
Immersive virtual reality environments have been shown to enhance user engagement, increase acceptability, and improve enjoyment, factors that are associated with increased activation in dopaminergic and cholinergic pathways.77–79 These neuromodulatory systems are known to support cognitive processes such as attention and working memory. However, the precise relationship between user motivation and neurophysiological activation remains complex and may involve bidirectional or indirect mechanisms. Additionally, exergaming elements such as goal-setting, adaptive challenges, and immediate rewards have been found to promote emotional regulation and sustained user participation.80,81 These features may establish a positive feedback loop among motivation, emotional experience, and cognitive enhancement, which could help explain the broader and more enduring benefits of digital interventions compared to traditional approaches. 82
Future research characteristics
In the research field of physical activity and cognitive function among older adults within the context of digital health, future developments are anticipated to emphasize interdisciplinary integration. Geriatrics and public health will continue to provide foundational data on the physical and mental health status of aging populations, informing the design of interventions. Neuroscience and cognitive science will further elucidate mechanisms such as neuroplasticity and neural network reorganization, identifying potential biological targets through which physical activity improves cognition. Meanwhile, disciplines such as computer science, artificial intelligence, and data science will support real-time monitoring, adaptive algorithms, and personalized feedback systems. Human-computer interaction and design research will enhance usability by tailoring digital interfaces to meet the needs of older adults. Behavioral science, sports science, and psychology will contribute motivational frameworks and evidence-based training principles to support personalized and sustainable engagement in physical activity. Rehabilitation and biomedical engineering will drive the adoption of multimodal sensors and virtual reality technologies in home-based applications, enhancing ecological validity. As digital interventions scale to community and policy levels, health economics will assess cost-effectiveness, while ethics and legal research will ensure data privacy and user rights.
Future research in this field is also expected to follow a more multidimensional and in-depth trajectory through multi-level collaborations. At the national level, regional integration and global coordination will advance in parallel. East Asian countries (e.g., China, Japan, and South Korea) may collaborate in the development of wearable devices, mobile health platforms, and multi-center clinical trials. At the same time, Europe and the Americas will contribute complementary strengths in AI algorithms and neuroimaging, facilitating the cross-regional application of digital health technologies. At the institutional level, industry-academia-research-medical collaborations will be further strengthened. Enterprises will drive technological innovation and product delivery, universities will contribute interdisciplinary knowledge and training, research institutes will optimize algorithms and explore mechanistic pathways, and medical institutions will provide clinical validation and real-world data. At the author level, cross-institutional, cross-regional, and interdisciplinary collaborations—enabled by cloud platforms and open-source tools—will become increasingly normalized, forming integrated teams across fields such as sports science, neuroscience, data science, and behavioral psychology.
Moreover, future research will present several emerging characteristics. First, research will increasingly emphasize not only cognitive performance but also functional outcomes such as emotional well-being, social interaction, and self-directed behavior. Second, there will be a stronger focus on personalization, with interventions tailored to differences in age, health status, lifestyle, and care needs, thereby enhancing precision and relevance. Third, intervention contexts will shift from controlled laboratory environments to real-world settings, such as home-based rehabilitation, community services, and telehealth platforms. This transition will enhance accessibility and sustainability, aligning digital health solutions with long-term care systems. Lastly, research methodologies will increasingly adopt mixed-methods and participatory approaches, combining quantitative outcome evaluations with qualitative user feedback. This evolution will promote a human-centered research paradigm in which older adults serve not merely as study subjects but as active participants in the design and refinement of interventions.
Strengths and limitations
This study has the following strengths. Through a multi-perspective analysis, encompassing publication statistics, co-occurrence relationships, co-citation relationships, and keyword distribution, we provide a comprehensive depiction of the field's structural features and temporal evolution; on this basis, we propose a preliminary knowledge framework that clarifies the current state of research and provides a reference for future research. Methodologically, a dual-database design (WoSCC and Scopus) provides complementary, multidisciplinary coverage, reduces single-source bias. The workflow adheres to the BIBLIO reporting guideline, the search strategy underwent peer review and is reported verbatim, and data selection was performed by two independent reviewers with third-party adjudication for discrepancies. Before merging datasets, we harmonized metadata, standardizing author, institution, and country names, and we applied de-duplication based on DOI, title, author, and year, thereby enhancing data quality, auditability, and reproducibility.
This study has several limitations. First, although the WoSCC and Scopus are widely regarded as the two most comprehensive sources for bibliometric analysis, records indexed exclusively in other databases may have been missed, potentially affecting the overall comprehensiveness of the analysis. To mitigate this risk, we adopted a dual-database design, documented the full queries and limits, and reported cross-database overlap and complementarity. Second, only English-language publications were included, potentially introducing language bias by excluding regionally significant or practically valuable non-English literature. Future work will include publications in multiple languages, with standardized screening and translation where necessary. Third, despite peer review of the search strategy, all keywords were searched as quoted exact matches (“word”) in the databases, which may render topic coverage imperfect; to reduce this risk, we enumerated common variants (e.g., singular/plural, hyphenated/non-hyphenated, acronym/full term). Fourth, bibliometric analysis primarily maps the current state and trends of a field and does not directly assess the methodological quality, study design rigor, or reliability of individual articles. As a partial mitigation, we restricted the dataset to peer-reviewed journal articles and excluded preprints, editorials, and conference papers; future work should integrate bibliometric findings with systematic reviews to achieve a more comprehensive understanding of the field.
Conclusion
Research on digital health-based physical activity and cognitive function in older adults is rapidly developing and demonstrates multidisciplinary characteristics. Forming an international collaboration framework with the United States at its core and broad participation from other countries, yet the overall network remains relatively fragmented, with cross-regional and cross-institutional collaborations requiring further development. Co-citation analysis reveals a solid knowledge base, built upon contributions from core journals, key authors, and highly impactful publications. The research focus lies in exploring the integration modalities of digital health with physical activity, ranging from basic monitoring and feedback-driven approaches to interactive and intelligent interventions, and their synergistic effects on cognitive function through mechanisms such as neuroplasticity enhancement, cognitive–sensory integration, and emotion–motivation regulation. Future directions emphasize the integration of geriatrics, neuroscience, computer science, and sports science, along with other disciplines, to promote personalized rehabilitation, real-world applicability, and quality of life improvements, advancing toward a human-centered and intelligent research paradigm.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251395534 - Supplemental material for Digital health-based physical activity and cognitive function in older adults: A bibliometric analysis
Supplemental material, sj-docx-1-dhj-10.1177_20552076251395534 for Digital health-based physical activity and cognitive function in older adults: A bibliometric analysis by Qifeng Han, Wenbo Ma, Zhenping Jiang, Yulin Sun, Liang Chen and Qian Sun in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251395534 - Supplemental material for Digital health-based physical activity and cognitive function in older adults: A bibliometric analysis
Supplemental material, sj-docx-2-dhj-10.1177_20552076251395534 for Digital health-based physical activity and cognitive function in older adults: A bibliometric analysis by Qifeng Han, Wenbo Ma, Zhenping Jiang, Yulin Sun, Liang Chen and Qian Sun in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251395534 - Supplemental material for Digital health-based physical activity and cognitive function in older adults: A bibliometric analysis
Supplemental material, sj-docx-3-dhj-10.1177_20552076251395534 for Digital health-based physical activity and cognitive function in older adults: A bibliometric analysis by Qifeng Han, Wenbo Ma, Zhenping Jiang, Yulin Sun, Liang Chen and Qian Sun in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to thank the researchers in the field of Digital Health-Based Physical Activity and Cognitive Function in Older Adults, whose publications have made significant contributions to this analysis. The authors also express their gratitude to the developers of the CiteSpace software, whose visualization tools enabled us to present our findings more effectively.
Contributorship
Qifeng Han: writing—original draft preparation, conceptualization, data curation, and software. Wenbo Ma: writing—original draft preparation, methodology, and data curation. Zhenping Jiang: writing—original draft preparation, formal analysis, and data curation. Yulin Sun: writing—original draft preparation, visualization, and formal analysis. Liang Chen: writing—review and editing, conceptualization, and supervision. Qian Sun: writing—review and editing, conceptualization, and supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used in this study were obtained from the WoSCC. The datasets generated and analyzed during the study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.