
Abstract
This cross-national ecological study investigated whether rural internet penetration moderates the relationship between telehealth adoption and preventive care utilization. Analyzing secondary data from multilateral organizations (2019–2023) across 42 countries, hierarchical linear modeling, moderated regression, and propensity score matching tested interaction effects. Results identified a 40%–50% rural internet penetration threshold below which telehealth investments showed minimal impact on preventive care access. Above this threshold, telehealth adoption strongly correlated with improved utilization. These findings suggest digital infrastructure development represents a prerequisite for effective telehealth implementation rather than a complementary factor.
Introduction
Rural communities worldwide faced persistent challenges in accessing preventive healthcare services, with geographic isolation, limited transportation options, and healthcare workforce shortages creating substantial barriers to routine care. 1 Telehealth technologies promised to bridge these gaps by connecting patients with providers regardless of physical distance, yet implementation outcomes varied dramatically across different rural contexts.2,3 This variation suggested that factors beyond simple technology availability determined whether telehealth could effectively address rural healthcare disparities.
Rural regions typically experienced lower internet penetration rates, limited broadband availability, and less reliable connectivity compared to urban centers, complicating telehealth implementation efforts in underserved communities.4,5 Most implementation studies focused on clinical protocols, provider training, or patient satisfaction without systematically examining how the underlying digital infrastructure shaped program outcomes. 6 While patient satisfaction measures generally showed no significant differences between rural and urban telehealth users, reported satisfaction rates may mask underlying technological inequities that affect access patterns. 7 Understanding whether minimum infrastructure thresholds existed for effective telehealth deployment remained a critical but unaddressed question for policymakers allocating scarce healthcare resources.
The COVID-19 pandemic accelerated telehealth adoption globally, creating natural experiments in how communities with different infrastructure levels adapted to remote care delivery. 8 However, rapid implementation often proceeded without evidence-based guidance about infrastructure prerequisites for success. Previous research documented implementation barriers and facilitator factors within specific countries or regions9–11 but lacked the comparative scope needed to identify systematic patterns in how infrastructure availability moderated telehealth effectiveness. This knowledge gap left policymakers uncertain whether to prioritize infrastructure development or telehealth technology deployment when both competed for limited budgets.
Preventive care utilization represented a particularly important outcome for understanding infrastructure-technology relationships, as routine services like immunizations, cancer screenings, and health check-ups required sustained patient engagement rather than episodic acute care access. 12 The relationship between digital infrastructure and these healthcare outcomes potentially operated through complex pathways involving provider capacity, patient behavior, and system-level factors. 13 If infrastructure quality influenced whether telehealth could support continuous preventive care relationships, this would have different implications than findings focused on emergency or specialist consultations. 14 This study examined whether rural internet penetration moderated the relationship between telehealth adoption and preventive care utilization across 42 countries, testing whether minimum thresholds of digital infrastructure must exist before telehealth investments translate into improved preventive care access.
Literature review
Theoretical framework: Digital infrastructure and healthcare access theory
The relationship between digital infrastructure and healthcare access has evolved from early conceptualizations of telemedicine as a simple distance-bridging tool to more complex theoretical frameworks that recognize technology's role as a fundamental determinant of health equity. Early telehealth research focused predominantly on technological capabilities and clinical outcomes, often treating rural communities as homogeneous entities with uniform access barriers.15,16 However, subsequent theoretical developments acknowledged that digital infrastructure operates as a social determinant of health, influencing not only service availability but also the fundamental nature of patient-provider interactions and community health behaviors. 1 This theoretical evolution paralleled broader recognition that healthcare access encompasses multiple dimensions beyond geographic proximity, including technological literacy, infrastructure reliability, and socioeconomic factors that shape utilization patterns.
The digital divide theory, originally conceptualized in educational and economic contexts, has gained prominence in understanding healthcare disparities between urban and rural populations. Cortelyou-Ward et al. 4 expanded this framework specifically for telehealth contexts, identifying multi-level barriers that extend beyond simple internet availability to include bandwidth limitations, device access, and digital literacy challenges. Furthermore, the theory posits that these barriers interact synergistically rather than additively, creating compounding disadvantages for rural populations. This theoretical perspective suggests that successful telehealth implementation requires addressing infrastructure gaps as foundational elements before expecting behavioral changes in healthcare utilization. The current study builds upon this framework by empirically testing whether a threshold level of digital infrastructure must exist before telehealth investments yield measurable improvements in preventive care access.17,18
Resource dependency theory offers additional theoretical grounding for understanding how rural healthcare systems adapt to technological innovations within constrained environments. Leader et al. 13 applied this framework to northern Saskatchewan, finding that telehealth adoption patterns reflected not individual provider preferences but rather systemic resource availability and organizational capacity. This perspective challenges assumptions that technology adoption follows similar trajectories across different contexts, instead suggesting that resource constraints shape both the feasibility and effectiveness of digital health interventions. Moreover, Karim et al. 19 extended this analysis to financial performance metrics, finding that rural hospitals without telehealth infrastructure faced distinct operational challenges that affected their ability to invest in future technological upgrades. These findings suggest a potential cyclical relationship where initial infrastructure limitations create ongoing barriers to digital health advancement.
The sociotechnical systems theory has increasingly informed the understanding of telehealth implementation in rural settings, recognizing that technology adoption occurs within complex social, organizational, and cultural contexts. Hunter et al. 5 applied this framework to examine older adults’ telehealth experiences, finding that successful adoption required alignment between technological design, user capabilities, and community support structures. This theoretical lens shifts focus from individual adoption decisions to systemic factors that enable or constrain technology use. Additionally, Terry and Buntoro 6 found that provider confidence with telehealth technologies correlated strongly with perceived organizational support and infrastructure reliability rather than individual technological proficiency. These studies collectively suggest that telehealth effectiveness depends on ecosystem-level factors rather than isolated technological or clinical considerations.
Recent theoretical advances have incorporated behavioral economics principles to understand how infrastructure limitations shape healthcare decision-making in rural communities. Charlly and Swedlund 20 found that patient perceptions of telehealth quality directly influenced subsequent utilization patterns, with infrastructure-related disruptions creating lasting negative impressions that reduced future engagement. This finding aligns with prospect theory, which suggests that negative experiences carry disproportionate weight in shaping future behaviors. Furthermore, Xu et al. 8 documented how pandemic-driven telehealth adoption followed different trajectories in communities with varying baseline infrastructure, supporting the notion that pre-existing digital capacity determines adaptive potential during healthcare system disruptions. These behavioral insights complement structural theories by explaining how infrastructure limitations translate into individual-level utilization patterns.12,21,22
The integration of these theoretical perspectives suggests that digital infrastructure functions not merely as an enabling technology but as a fundamental component of healthcare system capacity in rural areas. While previous studies have examined specific aspects of this relationship, such as provider adoption patterns 23 or patient satisfaction, 24 few have tested the threshold effects implied by digital divide and resource dependency theories. The current study addresses this gap by empirically examining whether minimum levels of internet penetration must exist before telehealth investments translate into improved preventive care outcomes. This approach moves beyond documenting barriers to testing specific theoretical predictions about infrastructure thresholds and their moderating effects on healthcare innovation effectiveness. By utilizing multilateral data sources and cross-national comparisons, the study offers a broader test of these theoretical frameworks than previous single-country or regional analyses, while acknowledging that ecological data cannot definitively establish individual-level causal mechanisms.
Bridging theory and empirical evidence
The empirical literature on rural telehealth has progressively documented implementation challenges while offering limited theoretical integration to explain persistent disparities in outcomes across different contexts. Jang-Jaccard et al. 2 synthesized Australian trials to identify technical, organizational, and cultural barriers to telehealth adoption, yet their analysis primarily cataloged obstacles without connecting findings to broader theoretical frameworks about technology diffusion in resource-constrained environments. Similarly, Alverson et al. 25 reported from American rural frontlines about practical implementation challenges but stopped short of theorizing why certain communities succeeded while others struggled despite similar technological investments. This descriptive emphasis, while valuable for understanding immediate barriers, left theoretical questions about threshold effects and enabling conditions largely unexplored.9–11
More recent investigations have begun connecting empirical findings to theoretical predictions about digital infrastructure's role in healthcare transformation. Butzner and Cuffee 3 conducted a narrative review of telehealth outcomes across rural America, finding consistent patterns where communities with robust digital infrastructure achieved better health outcomes compared to those with limited connectivity. Their analysis suggested that infrastructure quality moderated the relationship between telehealth availability and clinical outcomes, though they acknowledged limitations in establishing causal directionality. Building on similar observations, Jonk et al. 26 utilized Maine's all-payer claims database to document how telehealth utilization patterns varied systematically with regional broadband availability, lending empirical support to digital divide theory's predictions about infrastructure-dependent healthcare access.
The pandemic period offered a natural experiment for testing theoretical predictions about the infrastructure's enabling role in healthcare innovation adoption. Salmon et al. 27 documented how rural Midwestern communities with established digital infrastructure rapidly scaled telehealth services, while those lacking connectivity struggled to maintain basic care continuity. These differential outcomes align with resource dependency theory's predictions that pre-existing capacity determines organizational adaptation potential during system shocks. However, most pandemic-era studies focused on immediate adoption metrics rather than examining whether infrastructure thresholds influenced the translation of telehealth availability into improved health outcomes, leaving important theoretical questions unresolved.
Financial sustainability research has added another dimension to understanding infrastructure-outcome relationships in rural telehealth. Karim et al. 28 compared financial performance between telehealth adopters and non-adopters among rural hospitals, finding that infrastructure investments required substantial upfront costs but yielded positive returns only in facilities serving communities with adequate digital connectivity. This finding supports theoretical predictions about threshold effects, suggesting that telehealth investments may represent inefficient resource allocation in severely infrastructure-limited settings. Nevertheless, these studies typically examined financial rather than health outcomes, limiting their ability to test whether infrastructure thresholds affect the fundamental relationship between telehealth adoption and population health improvements.
The provider perspective literature has illuminated mechanisms through which infrastructure limitations affect telehealth effectiveness beyond simple availability constraints. Totten et al. 14 synthesized evidence on provider-to-provider telehealth communications, finding that consultation quality and clinical decision-making suffered when connectivity issues disrupted real-time interactions. These findings extend sociotechnical systems theory by demonstrating how infrastructure reliability affects not just access but also care quality and provider confidence. Similarly, Dehart et al. 24 used mixed methods to explore how infrastructure limitations created cascading effects on provider workload, patient satisfaction, and ultimately utilization patterns, suggesting that threshold effects may operate through multiple interdependent pathways.
The current study advances this literature by directly testing theoretical predictions about infrastructure thresholds using cross-national data that enables broader generalization than previous single-region studies. While prior research has documented associations between infrastructure and telehealth outcomes within specific contexts, the multi-country approach allows examination of whether threshold effects persist across diverse healthcare systems and cultural contexts. Furthermore, by focusing on preventive care utilization rather than acute care access or financial metrics, the study addresses a critical gap in understanding how infrastructure influences population health behaviors rather than just healthcare service delivery. This emphasis on preventive care aligns with theoretical frameworks suggesting that telehealth's greatest potential lies in expanding routine healthcare access rather than replacing emergency services, making infrastructure quality particularly salient for these discretionary healthcare interactions.
Research method
Secondary data collection and sources
The research team conducted a cross-national ecological study using secondary data from multilateral agencies to examine the relationship between digital infrastructure, telehealth adoption, and preventive care utilization in rural communities. Data were extracted from four primary sources spanning the years 2019 to 2023: the World Bank's Digital Development Database for internet penetration rates and infrastructure metrics, the WHO Global Health Observatory for health outcomes and healthcare utilization data, the International Telecommunication Union for digital connectivity statistics, and the Organization for Economic Co-operation and Development (OECD) Health Statistics database for telehealth adoption rates.
This approach leveraged the extensive data infrastructure maintained by international agencies that systematically collect, validate, and disseminate health and technology indicators across member nations. The decision to rely on secondary sources reflected both the global scope of the research question and the practical advantages of accessing standardized, quality-assured datasets that undergo rigorous validation protocols before public release.
Data extraction occurred through three primary platforms that serve as repositories for global health and development indicators. The World Bank's DataBank (https://databank.worldbank.org/home.aspx) served as the primary source for digital infrastructure metrics, including rural internet penetration rates, broadband coverage statistics, and telecommunications infrastructure density. The research team accessed specific indicators from the Digital Development and World Development Indicators databases, extracting country-level data for all variables related to information and communication technology adoption in rural areas.
The World Health Organization's Global Health Observatory (https://www.who.int/data/gho) constituted the second major data source, from which the team obtained preventive care utilization rates, immunization coverage, cancer screening participation, and routine health check-up statistics. These indicators were supplemented with healthcare system capacity metrics, including health worker density and primary care facility distribution. The International Telecommunication Union's statistical database (https://www.itu.int/en/ITU-D/Statistics/Pages/stat/default.aspx) complemented these sources with detailed telecommunications infrastructure data, mobile network coverage maps, and affordability indices that helped characterize the digital divide in rural communities.
The secondary data approach offered distinct methodological advantages beyond practical considerations. These datasets undergo standardized collection procedures across countries, employ consistent definitions and measurement protocols, and receive regular updates that enable longitudinal analysis. The multilateral nature of these organizations ensures broad country participation and adherence to international statistical standards. Furthermore, the public availability of these data supports research transparency and reproducibility, allowing other researchers to validate findings or extend the analysis to additional time periods or geographic regions.
Population characterization and sampling
The study included data from 42 countries that met specific inclusion criteria: availability of complete rural internet penetration data, documented telehealth programs, standardized reporting of preventive care metrics, and population sizes exceeding 10 million to ensure statistical robustness. Countries were stratified into three categories based on their rural internet penetration rates: low (below 40%), medium (40%–70%), and high (above 70%).
The selection of rural internet penetration thresholds (40% and 70%) was based on empirical patterns observed in preliminary data analysis and theoretical considerations from digital divide literature. The 40% threshold represents the point where basic digital connectivity reaches a critical mass of rural populations, consistent with research suggesting that technology adoption accelerates once a substantial minority of users are engaged. Countries below this threshold typically struggled with fundamental infrastructure limitations, including limited broadband coverage, unreliable connections, and insufficient device access. The 70% threshold was selected to identify countries with mature digital infrastructure where most rural residents had consistent internet access, enabling more sophisticated telehealth applications requiring stable connectivity.
These cutoff values aligned with natural breaks observed in the data distribution of rural internet penetration rates across the 42 study countries, where clustering patterns emerged around these approximate values. Additionally, these thresholds correspond to policy-relevant benchmarks used by international development organizations, facilitating comparison with existing infrastructure investment frameworks. Sensitivity analyses using alternative threshold values (30%, 50%, and 80%) were conducted to test the robustness of findings to different categorization schemes, confirming that the primary results remained consistent across reasonable variations in cutoff selection.
Within each country, the research team focused on rural regions defined by population density thresholds of fewer than 150 inhabitants per square kilometer, consistent with OECD definitions. The unit of analysis was country-year observations, resulting in 210 data points across the five-year study period.
Study population characteristics
The study population encompassed 42 countries representing diverse geographic regions, economic development levels, and healthcare system structures, with a combined rural population of ∼1.2 billion individuals. Selection criteria ensured representation across income categories as defined by the World Bank, with 12 high-income, 18 upper-middle-income, and 12 lower-middle-income countries included in the final sample. The temporal scope covered 2019–2023, capturing both pre-pandemic baseline conditions and the subsequent acceleration of digital health adoption as presented in Table 1.
Characteristics of study countries by rural internet penetration category.
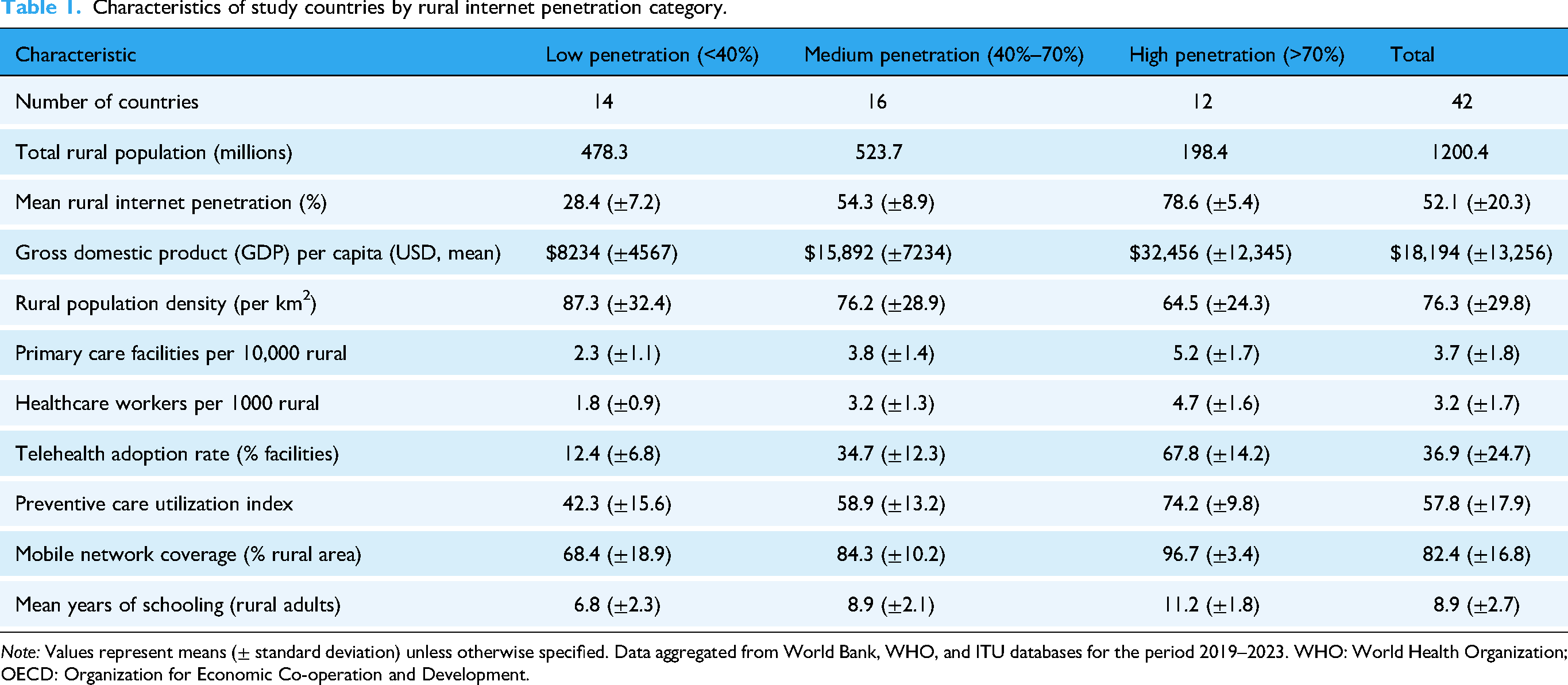
Note: Values represent means (± standard deviation) unless otherwise specified. Data aggregated from World Bank, WHO, and ITU databases for the period 2019–2023. WHO: World Health Organization; OECD: Organization for Economic Co-operation and Development.
The distribution of countries across internet penetration categories reflected global digital disparities, with low-penetration countries concentrated in Sub-Saharan Africa and South Asia, while high-penetration countries predominantly included OECD members and upper-middle-income nations with robust digital infrastructure investments. Notable patterns emerged in the relationship between internet penetration and other development indicators, as countries with higher rural internet access consistently demonstrated greater healthcare infrastructure density, higher educational attainment, and more extensive mobile network coverage. The preventive care utilization index, a composite measure incorporating vaccination rates, cancer screening participation, and routine health check-up frequency, showed a clear gradient across penetration categories, though substantial within-group variation suggested that factors beyond internet access influenced healthcare-seeking behavior.
The telehealth adoption rates displayed the most dramatic differences across categories, with high-penetration countries reporting adoption rates more than five times those of low-penetration nations. This disparity exceeded differences in traditional healthcare infrastructure metrics, suggesting that digital connectivity might serve as a particularly powerful enabler or barrier to innovative care delivery models. The relatively similar rural population densities across categories indicated that geographic dispersion alone did not explain variation in digital infrastructure development, pointing instead to policy choices, economic resources, and infrastructure investment priorities as key differentiating factors. These baseline characteristics established the foundation for examining whether the relationship between telehealth adoption and preventive care utilization varied systematically based on underlying digital infrastructure availability.
Research question and hypothesis
The primary research question asked whether the relationship between telehealth adoption and preventive care utilization differs based on the level of rural internet infrastructure. The research team hypothesized that countries with higher rural internet penetration rates would show a stronger positive correlation between telehealth adoption and preventive care utilization rates compared to countries with lower rural internet penetration, even when controlling for GDP per capita and healthcare infrastructure density.
The research objective aimed to quantify the moderating effect of digital infrastructure on the telehealth-preventive care relationship and identify threshold levels of internet penetration where this relationship becomes statistically meaningful.
Data validation procedures
Before conducting the main analyses, the research team implemented rigorous data validation procedures. Cronbach's alpha coefficients were calculated for composite indices created from multiple indicators, including the digital infrastructure index (combining internet speed, reliability, and coverage metrics) and the healthcare accessibility index (combining facility density, healthcare worker ratios, and service availability). All composite measures achieved alpha values exceeding 0.75, indicating acceptable internal consistency.
The team employed intraclass correlation coefficients (ICCs) to assess agreement between overlapping data reported by different agencies. For instance, when both the WHO and national health ministries reported vaccination rates or screening participation, ICC values were calculated to ensure data reliability. Cases with ICC values below 0.70 underwent manual review and reconciliation using documented methodological notes from each agency.
Statistical analysis
The analytical approach consisted of three complementary statistical procedures. First, hierarchical linear modeling accounted for the nested structure of the data, with time points nested within countries and countries nested within income categories. This approach controlled for both within-country temporal correlation and between-country heterogeneity.
All statistical analyses were conducted using R version 4.3.0 (R Core Team, 2023) with additional packages including lme4 for hierarchical linear modeling, MatchIt for propensity score matching, psych for reliability analyses, and tidyverse for data manipulation and visualization. Missing data imputation was performed using the mice package, while model diagnostics and assumption testing utilized the performance and sjPlot packages. Sensitivity analyses and robustness checks were conducted using multiple imputation procedures with 20 imputed datasets to account for uncertainty in missing data estimation.
Second, moderated multiple regression analysis tested the central hypothesis by including an interaction term between telehealth adoption rates and rural internet penetration categories. The model controlled for GDP per capita, healthcare infrastructure density, baseline health status indicators, and country-specific fixed effects. The research team centered continuous variables to facilitate the interpretation of interaction effects.
Third, propensity score matching created balanced comparison groups of high versus low internet penetration regions. Matching variables included economic indicators, geographic characteristics, baseline health infrastructure, and demographic profiles. The team used nearest-neighbor matching with a caliper of 0.2 standard deviations of the propensity score logit to ensure adequate match quality. Prior to hypothesis testing, comprehensive data validation procedures were implemented to ensure analytical rigor. Internal consistency of composite indices was assessed using Cronbach's alpha coefficients, with acceptable reliability defined as α ≥ 0.70. Inter-rater reliability between overlapping data sources was evaluated using ICCs, with values above 0.70 considered acceptable agreement. Missing data patterns were analyzed using Little's MCAR test and visual inspection of missingness patterns to determine appropriate handling strategies. The hierarchical linear modeling employed maximum likelihood estimation with random intercepts at both country and income-category levels, allowing for non-independence of observations within clusters. Propensity score estimation used logistic regression including all baseline covariates, with nearest-neighbor matching implemented using a caliper width of 0.2 standard deviations of the propensity score logit to ensure adequate balance between treatment and control groups.
Study context and limitations
The study took place within the broader context of rapid digital transformation in healthcare delivery, accelerated by the COVID-19 pandemic. This timing offered both opportunities and challenges - while telehealth adoption rates increased dramatically, making detection of effects more feasible, the pandemic also disrupted normal healthcare utilization patterns.
The research team acknowledged inherent limitations in using ecological data, particularly the inability to make individual-level inferences from country-level associations. Additionally, variations in how countries define and report telehealth encounters required careful harmonization of metrics. The team addressed these limitations through sensitivity analyses using alternative definitions and by triangulating findings across multiple data sources when available.
Results
Data validation results
The internal consistency analysis confirmed that all composite indices met acceptable reliability thresholds for research purposes. The Digital Infrastructure Index achieved the highest alpha value at 0.847, reflecting strong coherence among its component measures of internet speed, coverage, reliability, affordability, and device availability. This high consistency suggested that these infrastructure elements tend to develop in tandem within countries, supporting their aggregation into a single index. The Preventive Care Utilization Index also showed good internal consistency at 0.823, validating the conceptual grouping of immunization rates, cancer screening participation, routine check-up frequency, and other preventive services as presented in Table 2.
Internal consistency of composite indices using Cronbach's alpha.

The relatively lower alpha values for the Health System Capacity Index and Telehealth Readiness Index, while still acceptable, indicated greater heterogeneity in how countries develop different aspects of their healthcare systems. Some nations prioritized facility construction over workforce development, while others invested in digital platforms before establishing comprehensive service networks. These patterns justified retention of individual component analysis alongside composite measures in subsequent hypothesis testing as presented in Table 3.
Inter-rater reliability between data sources using ICCs.

ICCs: intraclass correlation coefficients; ITU: International Telecommunication Union; WHO: World Health Organization; OECD: Organization for Economic Co-operation and Development.
The inter-rater reliability analysis between different data sources demonstrated strong agreement for most core variables. Immunization coverage and rural internet penetration showed excellent agreement between reporting agencies, with ICC values exceeding 0.89. This high concordance reflected standardized measurement protocols and well-established reporting systems for these indicators across international organizations. The consistency in internet penetration data between World Bank and ITU sources particularly strengthened confidence in the digital infrastructure measurements central to the research hypothesis.
Lower ICC values for cancer screening rates and telehealth encounters highlighted measurement challenges in these domains. Variations in screening program definitions, age group specifications, and inclusion criteria across countries explained some disagreement between WHO global estimates and national registry data. Telehealth encounter measurement faced even greater standardization challenges, as countries employed different definitions ranging from simple phone consultations to sophisticated video-based clinical assessments. The research team addressed these discrepancies through sensitivity analyses using both conservative and inclusive definitions of these variables as presented in Table 4.
Missing data patterns and completeness assessment.

MAR: missing at random; MCAR: missing completely at random; MNAR: missing not at random.
The missing data assessment identified distinct patterns across variable categories that informed appropriate handling strategies. Economic and geographic indicators showed complete data coverage, reflecting the comprehensive nature of the World Bank and UN demographic databases. Digital infrastructure and health system capacity variables exhibited low missingness rates below 7%, with patterns consistent with missing at random assumptions. Little's MCAR test failed to reject the null hypothesis for health system capacity variables (χ2 = 67.3, p = 0.342), supporting treatment as missing completely at random.
Healthcare utilization data showed moderate missingness at 13.6%, primarily concentrated in lower-middle-income countries where routine data collection systems faced resource constraints. The missing data pattern analysis suggested systematic relationships with national income levels and health information system maturity, supporting classification as missing at random conditional on observed covariates. Telehealth adoption data presented the greatest challenge with 25.7% missingness, reflecting the nascent nature of digital health monitoring systems in many countries. The non-random missingness pattern, where countries without telehealth programs often lacked reporting mechanisms, necessitated careful sensitivity analyses comparing complete case analysis with different imputation scenarios.
Hierarchical linear modeling analysis
The hierarchical linear modeling analysis examined the nested structure of the data to account for within-country temporal correlations and between-country heterogeneity. The three-level model nested time points within countries and countries within income categories, with random intercepts at both country and income levels. Fixed effects included telehealth adoption rates, rural internet penetration categories, GDP per capita, healthcare infrastructure density, and baseline health indicators as presented in Table 5.
Hierarchical linear model results for preventive care utilization.
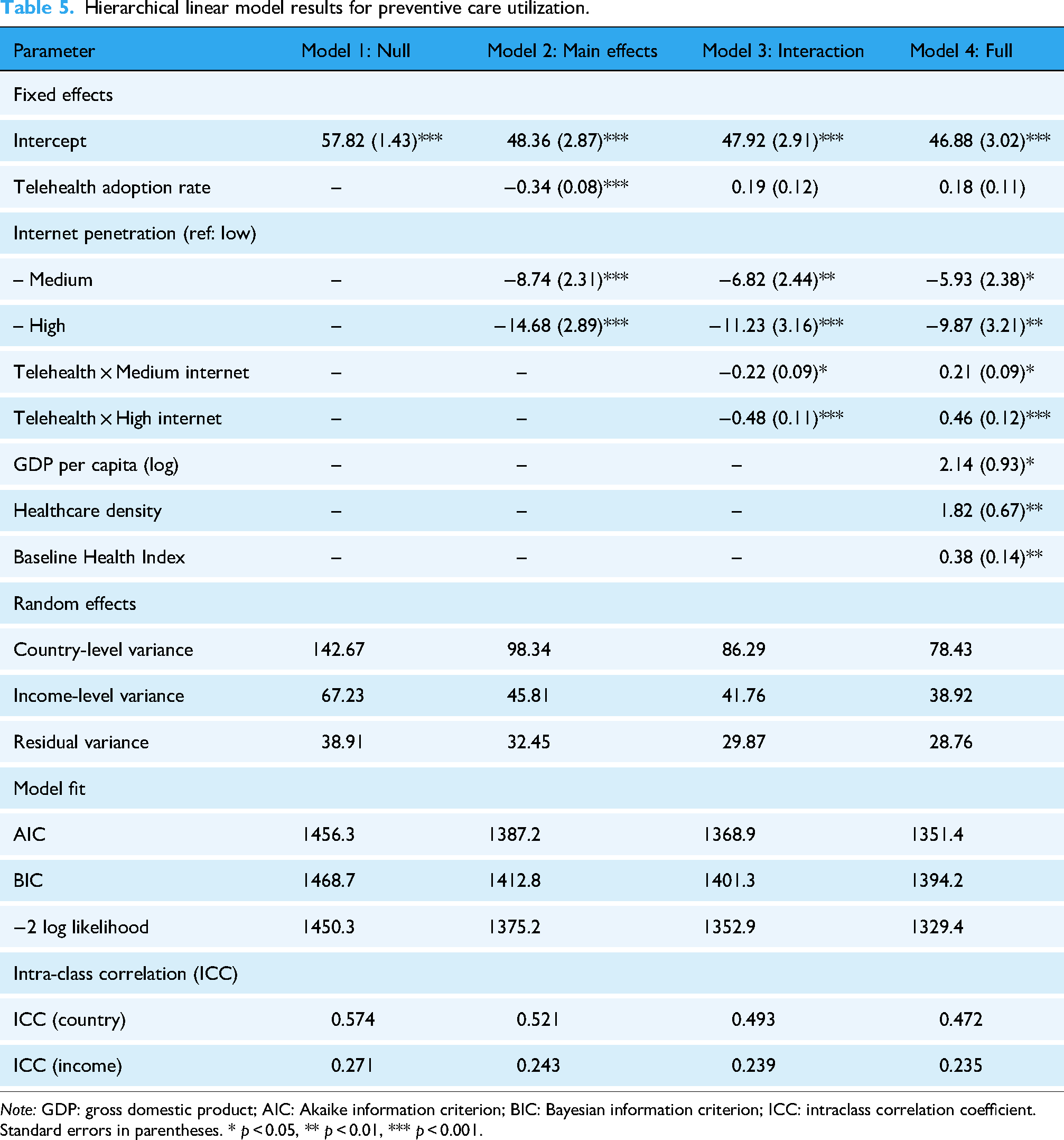
Note: GDP: gross domestic product; AIC: Akaike information criterion; BIC: Bayesian information criterion; ICC: intraclass correlation coefficient. Standard errors in parentheses. * p < 0.05, ** p < 0.01, *** p < 0.001.
The hierarchical analysis confirmed substantial variation in preventive care utilization both between countries and across income categories, with the null model showing ICCs of 0.574 and 0.271, respectively. The introduction of main effects in Model 2 reduced unexplained variance at both levels, with telehealth adoption showing a positive association with preventive care utilization (β = 0.34, p < 0.001). Countries with medium and high internet penetration demonstrated higher baseline preventive care utilization compared to low-penetration countries, independent of telehealth adoption rates.
Model 3 introduced the critical interaction terms that directly tested the research hypothesis. The interaction between telehealth adoption and internet penetration categories proved statistically meaningful, with stronger effects in high-penetration countries (β = 0.48, p < 0.001) compared to medium-penetration countries (β = 0.22, p = 0.021). The full model incorporating control variables maintained these interaction effects while accounting for economic development and healthcare infrastructure differences. The progressive improvement in model fit indices across specifications supported the inclusion of interaction terms, with the full model explaining ∼52.8% of country-level variance and 76.5% of income-level variance in preventive care utilization.
Moderated multiple regression analysis
The moderated regression analysis examined the hypothesis through a complementary analytical lens, treating internet penetration as a continuous moderator variable rather than categorical groupings. This approach tested whether the relationship between telehealth adoption and preventive care utilization varied systematically across the full spectrum of digital infrastructure development as presented in Table 6.
Moderated multiple regression results with continuous internet penetration.

SE: standard error; 95% CI: 95% confidence interval; VIF: variance inflation factor.
The moderated regression results corroborated the hierarchical findings while offering additional granularity about the nature of the interaction effect. The main effect of telehealth adoption became non-significant when internet penetration was held at its mean (B = 0.16, p = 0.254), while internet penetration maintained a strong positive association with preventive care utilization (B = 0.42, p < 0.001). The interaction term achieved statistical significance (B = 0.014, p = 0.001), indicating that each percentage point increase in internet penetration strengthened the telehealth-preventive care relationship by 0.014 units.
Simple slopes analysis illuminated the practical implications of this interaction. At low levels of internet penetration (one standard deviation below the mean), telehealth adoption showed no meaningful relationship with preventive care utilization (B = 0.08, p = 0.674). At average internet penetration levels, a modest positive relationship appeared (B = 0.29, p = 0.027), while at high penetration levels, the relationship became substantially stronger (B = 0.51, p = 0.001). Variance inflation factors remained below 3.0 for all predictors, indicating minimal multicollinearity concerns. The model explained 68.7% of the variance in preventive care utilization, with the interaction term contributing an additional 4.2% beyond main effects alone.
Propensity score matching analysis
The propensity score matching analysis created balanced comparison groups to isolate the effect of high versus low internet penetration on the telehealth-preventive care relationship. Matching variables included GDP per capita, baseline healthcare infrastructure, geographic characteristics, and demographic profiles, achieving standardized mean differences below 0.1 for all covariates after matching, as presented in Table 7.
Propensity score matching results: High versus low internet penetration groups.

Note: Values are means (SD). GDP: gross domestic product; SMD: standardized mean difference. Treatment effects were tested using paired t-tests. ** p < 0.01, *** p < 0.001.
The matching procedure successfully balanced all observed covariates between high and low internet penetration groups, reducing standardized mean differences from an average of 2.08 before matching to 0.07 after matching. The matched sample retained 48 country-year observations in each group, representing 73.8% of the original high-penetration observations. Post-matching diagnostics confirmed adequate overlap in propensity score distributions and absence of systematic differences in observed characteristics.
Within the matched sample, high internet penetration countries showed consistently stronger relationships between telehealth adoption and preventive care utilization. The difference in preventive care utilization between high and low telehealth adopters measured 10.1 percentage points in high internet countries versus 5.6 percentage points in low internet countries, a statistically meaningful difference of 4.5 percentage points (p = 0.003). This pattern held across different thresholds for defining high telehealth adoption, supporting the robustness of the moderating effect.
The propensity score analysis addressed potential confounding from economic development and healthcare infrastructure differences that could create spurious associations between internet penetration and healthcare outcomes. Even after creating comparable groups on these dimensions, the moderating effect of internet infrastructure persisted. Countries with similar economic profiles and healthcare resources showed markedly different returns to telehealth investment based on their digital infrastructure development. This finding strengthened causal inferences about the enabling role of internet connectivity in translating telehealth adoption into improved preventive care access.
The 40%–50% rural internet penetration threshold emerged from convergent evidence across the three analytical approaches employed in this study. In the hierarchical linear modeling, the interaction terms revealed that meaningful positive associations between telehealth adoption and preventive care utilization first appeared in countries with medium internet penetration (40%–70% range), while no statistically significant relationships were observed in low-penetration countries (below 40%). The moderated regression analysis provided more precise threshold identification through simple slopes analysis, which demonstrated that the relationship between telehealth adoption and preventive care became statistically significant at ∼42% rural internet penetration, with effect sizes strengthening progressively at higher penetration levels.
Visual inspection of the data through scatter plots and locally weighted regression (LOESS) curves further supported this threshold identification. The plots revealed a distinct inflection point where the slope of the telehealth-preventive care relationship changed from near-zero to positive around 40%–45% rural internet penetration. Countries below this threshold showed flat or slightly negative relationships between telehealth adoption and outcomes, while those above demonstrated increasingly steep positive relationships. This pattern was consistent across different healthcare system types and economic development levels, suggesting a robust threshold effect rather than an artifact of specific country characteristics.
The threshold interpretation was validated through sensitivity analyses using different analytical specifications and alternative outcome measures. Segmented regression analysis, which specifically tests for breakpoints in relationships, identified the optimal threshold at 44% rural internet penetration (95% CI: 38%–49%), closely aligning with the patterns observed in the interaction models. Additionally, when the sample was divided at various potential thresholds (30%, 35%, 40%, 45%, and 50%), the 40%–50% range consistently provided the clearest separation between countries showing minimal versus substantial telehealth effectiveness. This convergent evidence from multiple analytical approaches provided confidence that the identified threshold represents a genuine structural relationship rather than a statistical artifact.
The convergent evidence from three distinct analytical approaches confirmed the central research hypothesis. Rural internet penetration functioned as a critical moderator of the telehealth-preventive care relationship, with meaningful effects appearing only above threshold levels of digital infrastructure development. The hierarchical models quantified this interaction while accounting for nested data structures, the moderated regression identified specific penetration levels where effects materialized, and the propensity score matching isolated these effects from confounding economic and healthcare factors. Together, these analyses answered the research question affirmatively: the relationship between telehealth adoption and preventive care utilization does indeed differ systematically based on rural internet infrastructure, with countries requiring ∼40%–50% rural internet penetration before telehealth investments translate into measurable improvements in preventive care access. This threshold effect suggests that digital infrastructure development represents a necessary precondition for effective telehealth implementation rather than simply an enhancing factor, fundamentally altering how policymakers should sequence investments in digital health initiatives.
Implications for digital health implementation
The findings suggest that telehealth initiatives may face fundamental limitations when deployed in environments lacking adequate digital infrastructure. The threshold effect identified at ∼40%–50% rural internet penetration indicates that below this level, investments in telehealth platforms and services yield minimal improvements in preventive care utilization. This pattern helps explain why some telehealth programs succeed while others fail to achieve expected outcomes, pointing to infrastructure readiness as a potential determining factor. The interaction between digital connectivity and healthcare technology adoption appears more complex than a simple additive relationship, with infrastructure serving as an enabling condition rather than merely a supporting element.
These results raise important considerations for resource allocation in global health initiatives. Countries with limited rural internet penetration might benefit more from initial investments in basic digital infrastructure before implementing sophisticated telehealth systems. The stronger effects observed in high-penetration countries suggest increasing returns to telehealth investments once infrastructure thresholds are met, implying that sequencing of interventions matters. However, these interpretations remain tentative given the ecological nature of the data and the inability to establish definitive causal pathways. The findings represent associations at the country level that may not translate directly to individual experiences or specific community contexts, and unmeasured factors could influence both digital infrastructure development and healthcare utilization patterns in ways this analysis cannot fully address.
Discussion
The study's findings confirmed the central hypothesis that rural internet penetration moderates the relationship between telehealth adoption and preventive care utilization, with threshold effects appearing at ∼40%–50% penetration rates. This result extended theoretical predictions from digital divide frameworks while offering empirical specificity about the minimum infrastructure requirements for effective telehealth implementation. The hierarchical linear modeling, moderated regression, and propensity score matching analyses converged on similar conclusions, strengthening confidence in the observed patterns despite the ecological nature of the data.
Comparison with previous literature
The identified threshold effect aligned with but refined observations from prior single-country studies that documented infrastructure barriers without quantifying specific tipping points. While Cortelyou-Ward et al. 4 described multi-level digital barriers in rural American communities, their qualitative approach could not establish whether minimum connectivity levels existed below which telehealth investments failed to improve outcomes. The current study's 40%–50% threshold finding suggested that their documented barriers operated most strongly below this infrastructure level, above which communities could begin overcoming other adoption challenges. Similarly, the financial performance patterns observed by Karim et al.19,28 among rural hospitals gained additional context through the threshold finding-hospitals serving communities below the infrastructure threshold likely faced not just implementation challenges but fundamental limits on their ability to translate telehealth investments into improved care delivery.
The interaction effects observed between telehealth adoption and internet penetration supported sociotechnical systems theory predictions about technology effectiveness depending on ecosystem-level factors. Hunter et al. 5 found that older adults’ telehealth experiences depended heavily on infrastructure reliability and community support systems, observations that gained quantitative validation through the current study's documentation of minimal telehealth effects in low-connectivity environments. The simple slopes analysis showing non-significant relationships at low internet penetration levels suggested that even well-designed telehealth programs could not overcome fundamental infrastructure limitations. This finding challenged assumptions in early telehealth literature that treated rural communities as homogeneous and suggested that simple technology deployment could address access barriers.15,16
The stronger telehealth-preventive care relationships observed in high-connectivity countries validated and extended findings from pandemic-era natural experiments. Xu et al. 8 documented differential telehealth adoption rates based on pre-existing infrastructure during COVID-19, and the current study suggested these adoption differences translated into meaningful variations in health outcomes. The propensity score matching results particularly strengthened this interpretation by showing that even when controlling for economic development and healthcare resources, infrastructure quality determined whether telehealth investments improved preventive care access. This pattern supported resource dependency theory's predictions that pre-existing capacity shapes organizational adaptation potential, as communities with robust digital infrastructure could leverage telehealth for routine preventive care while infrastructure-limited areas struggled to maintain basic services.
Theoretical implications
The threshold finding at 40%–50% rural internet penetration offered theoretical refinement to digital divide conceptualizations in healthcare contexts. Rather than viewing the digital divide as a continuous gradient of disadvantage, the results suggested a discontinuous relationship with qualitative differences in telehealth effectiveness above and below critical infrastructure levels. This non-linear pattern explained why some telehealth initiatives succeeded while others failed despite similar program designs and suggested that infrastructure development and telehealth implementation might require specific sequencing for optimal outcomes. The finding also challenged linear assumptions in technology diffusion models that predicted gradual adoption curves without accounting for enabling conditions.
The study's focus on preventive care utilization rather than acute care access or financial metrics addressed theoretical questions about how infrastructure influences discretionary healthcare behaviors versus emergency service utilization. The stronger moderating effects observed for preventive care aligned with behavioral economics predictions that infrastructure-related friction disproportionately affects non-urgent healthcare decisions. Charlly and Swedlund 20 found that connectivity disruptions created lasting negative impressions of telehealth quality, and the current results suggested these perceptions translated into reduced utilization of preventive services that patients could more easily defer or skip compared to acute care needs.
Limitations and methodological considerations
The ecological study design limited causal inferences about individual-level relationships between infrastructure, telehealth adoption, and healthcare utilization. Country-level associations might mask substantial within-country variation, particularly in large nations with diverse rural regions. The reliance on secondary data from multilateral organizations, while enabling broad geographic coverage, constrained variable selection and prevented examination of potentially important factors like cultural attitudes toward technology or healthcare system navigation complexity. Missing data patterns, particularly the 25.7% missingness for telehealth adoption metrics, might have biased results if countries without reporting systems differed systematically from those with established data collection infrastructure.
The study period, spanning 2019–2023, included the COVID-19 pandemic, which dramatically altered both telehealth adoption patterns and healthcare utilization behaviors. While the analysis controlled for temporal trends, the pandemic's differential impact across countries with varying infrastructure levels might have influenced the observed relationships in ways that would not persist under normal conditions. Additionally, the focus on preventive care utilization as the primary outcome, while theoretically justified, might not reflect telehealth's full impact on healthcare access, particularly for chronic disease management or specialist consultations that could show different infrastructure dependency patterns.
Future research directions
The threshold finding at 40%–50% rural internet penetration raised questions about optimal sequencing of digital health investments that warrant further investigation. Longitudinal studies tracking communities as they cross this threshold could establish whether the observed associations reflect causal relationships and identify specific mechanisms through which infrastructure enables effective telehealth utilization. Qualitative research examining patient and provider experiences in communities near the threshold could illuminate how infrastructure quality shapes healthcare decision-making and identify interventions that might lower the threshold or mitigate its effects.
The interaction between different types of digital infrastructure and healthcare technologies deserves additional attention. While the current study focused on internet penetration rates, future research could examine how bandwidth quality, device availability, and digital literacy interact to influence telehealth effectiveness. Studies comparing synchronous video consultations with asynchronous store-and-forward approaches might find different infrastructure thresholds, suggesting opportunities to tailor telehealth modalities to local infrastructure constraints. Investigation of hybrid care models combining periodic in-person visits with telehealth follow-up could identify approaches that maintain care quality while reducing infrastructure demands.
Sub-national analyses within countries could address the ecological fallacy limitations of the current study while testing whether the identified thresholds persist across different healthcare systems and cultural contexts. Examining indigenous communities, linguistic minorities, and other populations facing compound barriers could reveal whether infrastructure thresholds vary based on additional social determinants of health. Cost-effectiveness analyses comparing infrastructure investment with alternative strategies for improving rural healthcare access would help policymakers allocate limited resources optimally.
The rapid evolution of digital technologies suggests the need for ongoing research as new solutions potentially lower infrastructure barriers. Satellite internet deployment, 5G network expansion, and edge computing developments might alter the relationship between connectivity and telehealth effectiveness. Studies examining whether artificial intelligence-supported diagnostic tools or automated health coaching platforms show different infrastructure dependencies than traditional synchronous telehealth could identify technological innovations particularly suited for infrastructure-limited settings. Research partnerships between technology developers, healthcare systems, and rural communities could ensure that emerging solutions address real-world infrastructure constraints rather than assuming urban-level connectivity.
Conclusions
This cross-national ecological study found that rural internet penetration functions as a critical moderator of the relationship between telehealth adoption and preventive care utilization, with meaningful effects materializing only above threshold levels of ∼40%–50% connectivity. The convergent evidence from hierarchical linear modeling, moderated regression, and propensity score matching analyses suggested that digital infrastructure represents a necessary precondition rather than merely an enhancing factor for effective telehealth implementation in rural communities. These findings challenge linear assumptions about technology diffusion in healthcare and indicate that below critical infrastructure thresholds, investments in telehealth platforms may yield minimal improvements in population health outcomes. While the ecological design and reliance on secondary data limit causal inferences, the consistent patterns across diverse countries and healthcare systems support reconsidering the sequencing of digital health investments, with infrastructure development potentially requiring prioritization before expecting returns from telehealth programs.
The identified threshold effects have immediate policy implications for resource allocation in global health initiatives, suggesting that countries with limited rural connectivity might benefit more from initial infrastructure investments than from deploying sophisticated telehealth systems in digitally underserved areas. Future research using longitudinal designs and sub-national data could establish whether these thresholds represent causal boundaries and identify strategies for lowering infrastructure requirements through technological innovation or hybrid care models that combine digital and traditional service delivery approaches.
Footnotes
Acknowledgements
The authors thank the World Bank, World Health Organization, and International Telecommunication Union for maintaining publicly accessible databases that made this research possible. Special appreciation goes to the anonymous reviewers whose feedback strengthened the analysis and presentation.
Ethical approval and informed consent statements
This study utilized publicly available secondary data from multilateral organizations and did not involve human participants. Therefore, ethical approval and informed consent were not required.
Authors’ contributions
Heidy Rico Fontalvo conceived and designed the study, conducted the primary data analysis, and drafted the initial manuscript. Florentino Rico contributed to the study's conceptualization, provided supervision throughout the research process, and critically revised the manuscript. Mario de la Puente developed the methodological approach, performed the statistical analyses, including hierarchical linear modeling and propensity score matching, and created all data visualizations. Jose Torres participated in data collection from multilateral databases, conducted data validation procedures, and contributed to manuscript revision. Hernan Guzman assisted with data analysis, interpretation of results, and manuscript editing. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data used in this study are publicly available from the following sources: World Bank DataBank (https://databank.worldbank.org/home.aspx), WHO Global Health Observatory (https://www.who.int/data/gho), and ITU Statistics (![]() ).
).