
Abstract
Objectives
Adolescents have been identified as an ideal user group for digital health tools. However, currently, there is limited research exploring applied participatory methods that support adolescents in digital health intervention development across diverse real-world settings. This article introduces the Oky smartphone application, which provides menstrual health support to adolescents around the world and has a unique participatory method for local digital development – Girl-Centred-Design. This study explores three research objectives in relation to Oky's participatory method: (1) exploring how Oky's Girl-Centred-Design method supports meaningful participation with adolescents, (2) identifying Girl-Centred-Design method barriers and enablers and (3) generating Girl-Centred-Design lessons.
Methods
A desk review of 224 documents was conducted, followed by 31 semi-structured qualitative interviews with personnel from six organisations implementing Oky across six countries (Burundi, Kenya, Tanzania, Nepal, Ukraine, and the Philippines). Findings were presented to implementing organisations for validation and were thematically analysed.
Results
Six organisations developed smartphone applications using Oky's Girl-Centred-Design method, which supported meaningful participation in line with the World Health Organisation's definition and Hart's and Lundy's conceptual participation frameworks. Culturally grounded visuals, contents and features were co-created, and participants emerged as influential stakeholders and application ambassadors with new skills and increased confidence. Structural, contextual and cultural enablers and barriers were identified that helped or hindered Oky's Girl-Centred-Design method. Barriers were digital access gaps and cultural taboos. Enablers were peer networks, working with trusted community figures and using familiar spaces. Lessons learned were early-stage and iterative participation with girls and others to sustain participant-driven development throughout the implementation process. Intentional participant skills-building frameworks and further multi-stakeholder collaboration were outlined as future-oriented insights for optimising meaningful participation.
Conclusion
Oky's Girl-Centred-Design is a meaningful participation method for co-creating digital interventions that empowers young people and responds to their needs. Practical and policy implications for future participatory approaches are outlined.
Introduction
Menstruation can impact health outcomes and overall quality of life for menstruators across the world. 1 The ability to manage menstrual health and hygiene (MHH) with dignity and without stigma, as well as access adequate facilities and products, is a human right. 2 However, in communities where menstruation is stigmatised, 3 adolescents in particular are more likely to be uninformed. 4 Knowledge gaps can lead to feelings of shame and confusion 5 as well as unhygienic practices and absenteeism from school and social activities. 6 As a result, there are calls for low-cost, evidence-based, innovative interventions for adolescents that support MHH and menstrual health literacy. 4
The global proliferation of mobile device ownership over the past decade 7 makes digital health interventions increasingly relevant.8,9 As adolescents (aged 10–19) and young people (aged 15–24) are embracing technology globally, 10 they are ideal users for digital health tools.11,12 However, digital divide barriers challenge equality in device access, connectivity and digital literacy, and present major obstacles for digital health tools.13,14 Existing digital interventions highlight varying uptake and engagement, and high dropout rates.15,16 Literature outlines participatory intervention development17–20 and cultural and contextual intervention adaptation21–23 as strategies to address this.
In Implementation Science, participatory methods are promoted for bridging implementers and communities. With a focus on human rights,23–25 social determinants of health, and equity,26–29 participation can inform socio-cultural and contextual developments. 18 The World Health Organisation defines meaningful engagement in public health as the ‘respectful, dignified, and equitable inclusion of individuals with lived experience in a range of processes and activities within an enabling environment where power is transferred to people, valuing lived experience as a form of expertise and applying it to improve health outcomes’. 30
There are also a number of conceptual frameworks and models to guide practitioners and policy makers in participatory action and meaningful engagement. 19 31–37 Hart's ‘Ladder of Youth Participation’ 38 is a hierarchical model that conceptualises youth engagement and agency along an increasingly influential ladder, spanning from manipulation to youth-initiated and youth-directed leadership.
Grounded in the rights of the child, Lundy's ‘Model of Participation’ 39 sets out four domains for meaningful participation: safe, inclusive spaces; hearing children's voices; giving children an audience; and acting upon children's contributions. Often associated with digital initiatives, Human-Centred Design (HCD) methodologies have emerged as an intervention development approach that fosters user empathy and contextual needs through iterative creative processes.40–43 All these approaches make space for intervention user groups to share power through collaboration.44–46
Combining participation with digital health interventions offers an opportunity to develop relevant and appropriate interventions that address power imbalances and inequities in public health and bridge gaps between implementers and users.47–49 This is particularly important in low- and middle-income countries (LMIC) where uneven resource distributions and systemic barriers can affect health access, or where paternalistic interventions marginalise certain communities and limit local ownership.
To date, there are few studies that explore adolescent participation in digital health intervention development across multiple country contexts.12,50 This study contributes by exploring a real-world digital health intervention, the UNICEF-supported “Oky” smartphone application, across diverse LMIC country contexts. Oky is one of the few digital health intervention examples with its own unique co-creation method that encourages and supports systematic participatory development of its digital health tool.
The digital health intervention
Oky is a digital health intervention. It is a smartphone application that sits alongside a portfolio of similarly focused initiatives, including radio and other technology and in-person (non digitalised) interventions, which support the health of adolescent girls. Oky is designed and developed ‘by girls, for girls’ 51 through an inclusive and meaningful participatory co-creation development method to provide accessible, relevant MHH and sexual and reproductive health (SRH) information. Features include an evidence-based MHH and SRH encyclopaedia with age-appropriate ‘girl-friendly language’, 52 a menstrual cycle tracker, personalisable themes and animated avatars and signposts to local health services.
Oky was first co-created through a pilot with 400 adolescent girls in Indonesia and Mongolia, which generated an evidence base upon which Oky's unique Girl-Centred-Design method was established. This pilot generated a number of learnings, upon which the Oky toolkit (Supplemental material 2) was created to guide implementers in other contexts with inclusive Girl-Centred-Design approaches according to context, culture and communities. The Girl-Centred-Design approach stems from HCD and is participatory, to work alongside communities to co-create solutions that address their needs through incorporating their ideas and experiences. 52 These kinds of approaches are said to strengthen relevance, acceptability and equity in health interventions but also require time, resources and sustained investment for implementation, especially in resource-constrained settings.
Oky offers several strengths as a digital health tool. As well as being girl-led, Oky is underpinned by design principles that ensure the safeguarding of users and reflect their digital realities. Digital realities refer to the technological infrastructural aspects within real-world environments that enable or challenge digital access and internet connectivity. 53 For example, adolescent girls face more obstacles in accessing and using mobile phones and the internet than their older or male counterparts. Oky uses open-source code, is non-commercialised, and has in-built data privacy and protection measures designed especially for girls. Oky operates completely offline and does not require internet access; it allows multiple users to log in securely on one device; it is designed for compatability with low-end smartphones and older operating systems, and requires little digital memory. As with many digital health tools, Oky requires users to have smartphone access and basic literacy, which can limit accessibility in contexts where this is not the norm. However, Oky has also been designed to help overcome these obstacles through Girl-Centred-Design.
Through a social franchise agreement, based on principles of local ownership, equal partnership, trust and long-term collaboration, 52 ‘Oky Franchise Partners’ (OFP) receive generic Oky software and toolkit resources to develop and implement Oky locally, using Oky's Girl-Centred-Design method (Figure 1), to co-create local applications that users access, use, trust and engage with. 52 This method offers entry points for participatory co-creation approaches, for example, where user insights and co-ideation involve close collaboration with adolescent girls and others in their social circles.

Overview of Oky's Girl-Centred-Design method ©. 52
Objectives
This study aims to explore Oky's Girl-Centred-Design method for developing a smartphone application across diverse contexts. To do this, we set out three research objectives:
Explore how Oky's Girl-Centred-Design method facilitates meaningful participation of targeted user groups of people in application development; Identify barriers and enablers to Oky's Girl-Centred-Design method and Gather lessons learned from OFP's Girl-Centred-Design experiences for optimising participatory health intervention development.
Methods
Study design
This qualitative study explores Oky's application development journey using its Girl-Centred-Design method across six implementation sites in Burundi, Kenya, Tanzania, Nepal, Ukraine, and the Philippines, with six OFP. A desk review and semi-structured interviews were conducted, followed by analysis of findings.
Ethics and consent
We obtained approval from the University of Bremen ethics commission before commencing the study (reference: 2022-26). Individuals from OFP (key informants, KI) provided individual written consent before participating in the study.
Eligibility, sampling, recruitment and onboarding
The eligibility criteria sought OFP from LMIC, that had completed major development activities, had launched their applications (after stage 5 in Figure 1), and were willing and able to commit to the study. According to these criteria, 6 out of 12 OFP were sent a study information sheet between October and November 2023 via email and invited to participate. All six OFP agreed, and introductory sessions were held with KI and the Oky Global team to co-design the study, data collection methods and tools.
Data collection
OFP presented their Oky activities and provided pre-existing project-level documents for desk review, including proposals, reports and monitoring data. Documents were eligible if they related to the research objectives and contributed towards an understanding of what Girl-Centred-Design activities were undertaken by OFP. Following this, individual, semi-structured interviews were held online with KI and recorded via Zoom technology (JB). Interviews were anchored by a topic guide (Supplemental material 5), informed by desk review data and shaped by the individual Oky roles of each KI. The interviews provided an in-depth understanding of how Girl-Centred-Design activities were undertaken. Interviews lasted approximately 90 minutes and were transcribed using Microsoft Word (JB). Identifying characteristics were replaced with generic markers (JB) and subjected to a second review (ML) to ensure accuracy and anonymity.
Data analysis
According to the research objectives, documents underwent a desk review to map out the Girl-Centred-Design activities per OFP (JB and ML). Using the Framework Method, 54 interviews were thematically analysed both deductively and inductively according to the research objectives and relevant emerging themes using Atlas.ti software manual coding features (JB) for two rounds of coding. A second reviewer checked and completed the coding (ML). Findings were summarised per OFP and were presented to the Oky global team and each OFP in group discussions (JB). OFP participants provided feedback and confirmed accuracy to validate the findings.
Reporting was guided by the Social Accountability Reporting for Research Framework (Supplemental material 1) 55 with selected quotes to highlight key findings.
Findings
Application and sample characteristics
Six Oky applications, in Burundi, Kenya, Tanzania, Nepal, Ukraine, and the Philippines, were locally developed using the Girl-Centred-Design method. Activities started between 2021 and 2022, and all applications were live at the point of writing. OFP were non-governmental organisations with varying expertise, including youth, advocacy, rights, technology, health, sociology, gender, education and community engagement. All had long-term experience creating content for adolescents, working with communities, and participatory practices.
The desk review included 224 documents, including project reports and Oky toolkit resources (Supplemental material 2). Thirty-one KI interviews were conducted (Supplemental material 3), and all KI were nationals of their implementing contexts.
Exploring the Girl-Centred-Design method
Girl-Centred-Design activities and stakeholders
Oky's Girl-Centred-Design method, as outlined in the Oky toolkit, was used to consult with 800+ adolescents and young people aged between 10 and 24 years old across the six countries. Girl-Centred-Design activities were conducted through group discussions, interactive workshops, games, application testing and creative activities (Supplemental material 3). Throughout these activities, participants actively co-created content as key collaborators. Participants achieved this through sharing insights into their digital behaviours and health perspectives, including common MHH and SRH questions, beliefs and practices, which co-created contextualised health content. Care was taken to ground content with cultural and contextual relevance and tone for user appeal. Examples of this were framing health content with religious verses, as well as incorporating cultural names and practices into menstrual stories. Some Girl-Centred-Design activities also included educational health messaging that encouraged body positivity and empowerment.
Across the six contexts, in addition to adolescents and young people, a range of multi-disciplinary stakeholders supported Girl-Centred-Design activities (Table 1 and Figure 2). ‘The competencies of the team are a key part of making Oky a success. Though it's a tech project, it involves health, programming, and project management expertise. Oky is just a tool, but the process of developing it with the girls, the active listening of the team, that is not easy. It takes skill, patience, and perseverance, which has to be considered, so it involves a wide range of skills and people from different disciplines’. (KI 22)

Girl-Centred-Design stakeholders across six contexts.
Participatory stakeholders across six contexts.
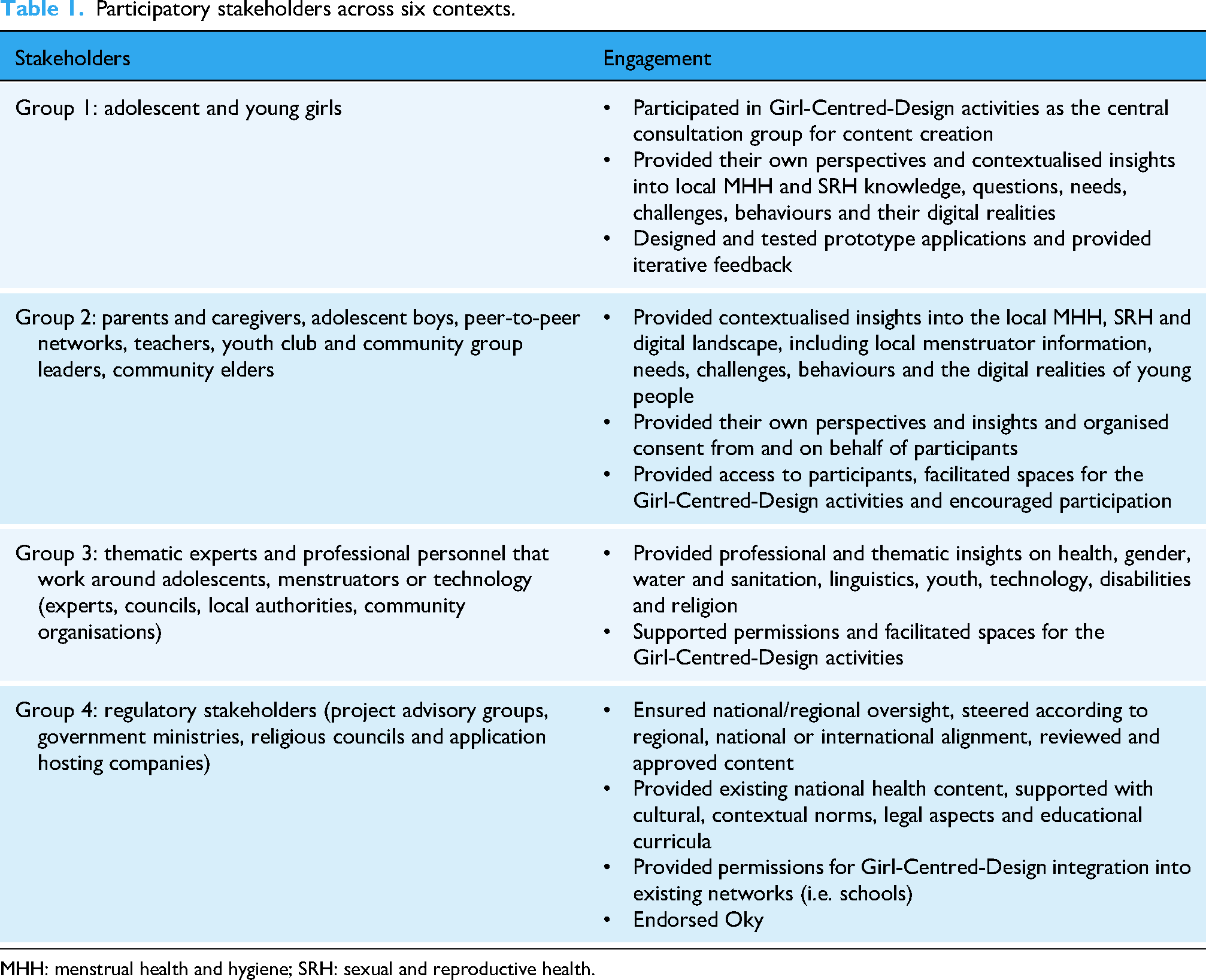
MHH: menstrual health and hygiene; SRH: sexual and reproductive health.
Girl-Centred-Design outputs
Four main application development areas (outputs) were co-created across the six implementation sites (Table 2). These were (1) MHH and SRH content, (2) language, (3) visuals, and (4) local health services information. Inclusion features, including for girls with disabilities, cut across these developments (Supplemental material 6).
Main co-created outputs across the six applications.
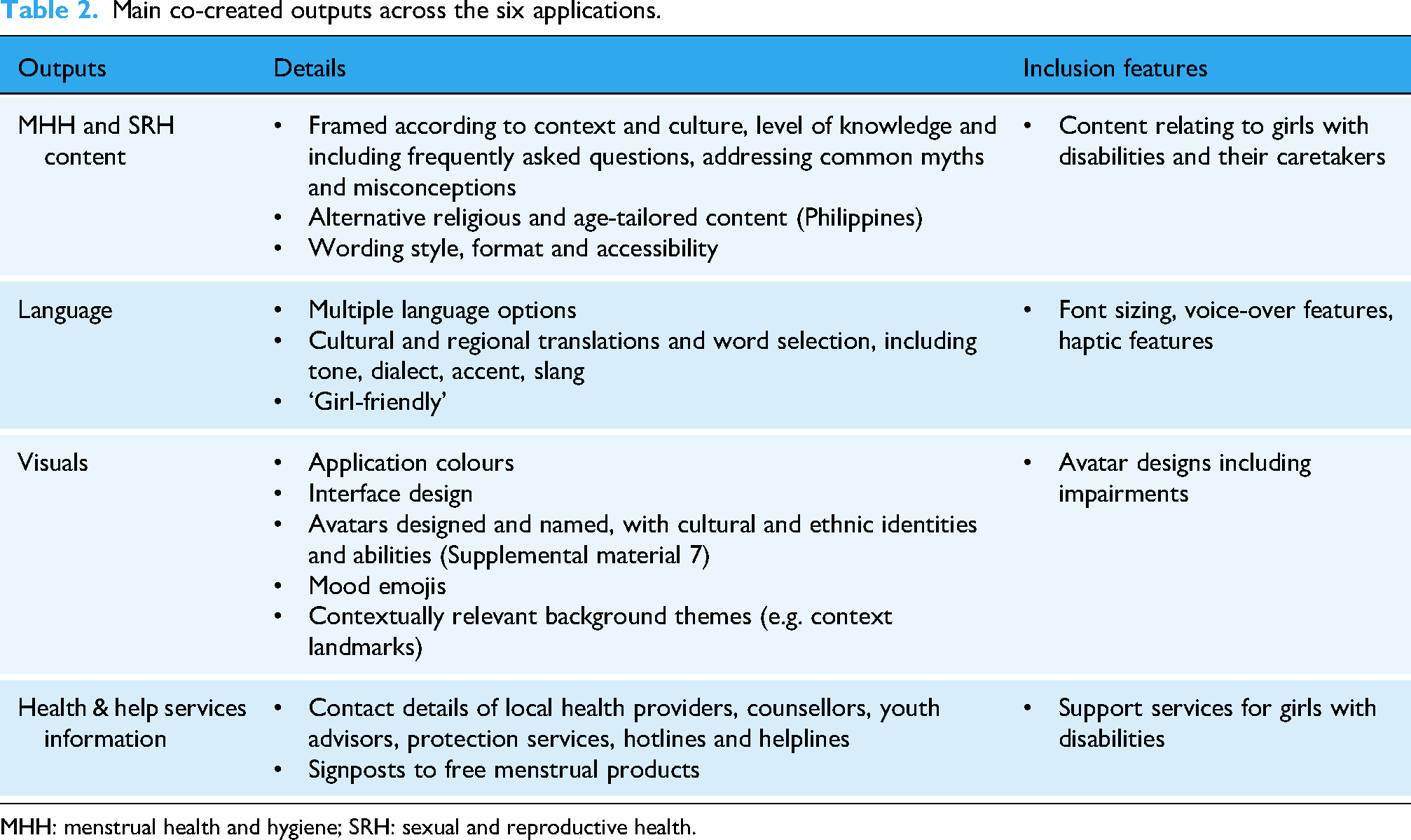
MHH: menstrual health and hygiene; SRH: sexual and reproductive health.
Girl-Centred-Design reflections
OFP reported that they found the toolkit resources helpful for developing Oky according to its Girl-Centred-Design method and maintaining child-centredness throughout. This was complemented with cross-context learning exchanges between OFP and the Oky Global team, which fostered collaboration.
OFP identified through Girl-Centred-Design activities that adolescents and young people were rarely consulted for their opinions. Instead, parents, caregivers and authority figures tended to make decisions for them. As such, OFP perceived that participants found Oky's Girl-Centred-Design method to be an exciting and interesting opportunity to contribute their ideas. The extent and depth of participant feedback highlighted to OFP the value of co-creation approaches with adolescents and young people. ‘Every day new apps are developed, but it's not about the tech, it's about those processes that support children and especially vulnerable children. Oky is an enabler, a space that facilitates lasting safeguarding and makes sure that the girls have their concerns and issues, such as menstrual health and all the other aspects, addressed’. (KI 18)
OFP observed a cultural shift between Oky's Girl-Centred-Design method and more traditional, top-down and expert-driven health approaches. The Girl-Centred-Design method was considered more intensive, more interactive and more collaborative, spanning multiple implementation stages. ‘The Girl-Centred-Design processes are more of a cultural shift to working with the community rather than giving them what we think they’ll need. Overall, this works to shift that dominant structure, and tip the scales in the favour of the community, and I think that's what we need for more equitable futures’. (KI 18)
Girl-Centred-Design was reported as relevant and practical for meaningfully engaging with young people to understand their needs and co-create Oky content. This method was credited for bridging the knowledge gap between adolescent girls and OFP, and there was a growing sense of participant ownership towards Oky. ‘I think the process was very important in terms of developing ownership and making sure that it's not just something that comes from donors. There's a saying when it comes to bringing things in, “This is only for Mzungu”, meaning that “this product is one of those white people things”. So, I think it's very important to make something of our own…’ (KI 16)
Girl-Centred-Design barriers and enablers
There were a number of structural, cultural and contextual barriers and enablers that hindered or helped the Girl-Centred-Design, outlined in Figure 3.

Barriers and enablers to Oky's Girl-Centred-Design method across six contexts.
Structural barriers and enablers
As part of the Girl-Centred-Design activities, participants were introduced to the global Oky application as a template to develop from. In five of the implementing contexts, limited digital device access amongst participants challenged this activity. This barrier was particularly felt by less economically well-off participants and those in rural, coastal and island communities. Addressing this, one OFP provided devices to participants during Girl-Centred-Design activities for hands-on Oky access, but some participants were unfamiliar with digital devices and digital terminology. One OFP limited their participant recruitment only to urban areas on the assumption that participants in these areas would be more likely to have digital access. OFP also expanded their non-digital Girl-Centred-Design activities such as drawing, discussions and storytelling.
Some OFP had not raised the full funding amount recommended by UNICEF to localise Oky, which limited some iterative Girl-Centred-Design activities and the integration of certain features. For example, the Nepalese OFP were keen to integrate their national calendar into Oky's menstrual tracking feature. However, a lack of funds prohibited this development at that time.
In four contexts, regulatory stakeholders (governments, application hosting companies, advisory groups and councils) acted as both an enabler and a barrier to Oky's Girl-Centred-Design method. In the Philippines, government partners supported Oky with a memorandum to work through the schools’ system, enabling Girl-Centred-Design activities to scale. In other contexts, they supported and endorsed Oky activities with other organisations, giving it their seal of approval. However, in some settings, they also challenged Oky's Girl-Centred-Design method, where they found certain topics to be problematic, including content related to puberty (considered vulgar), family planning (considered age-inappropriate), homosexuality (outside legal frameworks), COVID-19 (contentious) and LGBTQ+ (religiously, culturally and legally unaligned). Here, OFP reduced or removed some co-created content prior to application approval. ‘I think it is very important for the government to be more open minded and focus more on what their people say they need, rather than what they want Oky to be. Because at the end of the day, we are working for the people… if we don’t include certain information, and people continue to make risky health decisions, we'll just end up having the same problems every day. So, it is important to continue advocating and engaging with the government, so they align with us, in inspiring social behavioural change within our communities whilst also inspiring change in our policies and decision makers’. (KI 01)
This process reduced the responsiveness of Oky's Girl-Centred-Design method to iteratively respond to participants’ evolving needs. OFP addressed regulator comments where possible: For example, the Philippines OFP integrated age-bracketed content, overcoming the issue of age-inappropriate content.
Cultural barriers and enablers
In four contexts, MHH and SRH were taboo in certain communities, which challenged open discussions on these topics. Adjustments were made, including gathering permissions from community elders and leaders, particularly in indigenous groups, prior to participation with young people. From this, trusted figures, such as teachers and indigenous and religious leaders, encouraged their communities to engage. They supported culturally sensitive Girl-Centred-Design activities by, for example, starting with a prayer, drawing upon local cultural practices to discuss menstrual health challenges and using locally accepted menstrual terms in discussions.
Further, working within and through community-based structures and systems, such as school networks, youth and social clubs, community health teams and peer-to-peer programmes, was a considerable Girl-Centred-Design enabler. As well as providing familiar and accessible physical spaces for Girl-Centred-Design activities, this approach provided access to and enabled insights from a broad range of participants. Furthermore, direct participants cascaded information to peers, widening participation into broader communities. In addition to face-to-face and peer-to-peer activities, a number of remote participatory formats, including social media, SMS, WhatsApp groups, toll-free phone lines and in-app surveys, were used. These platforms supported iterative Girl-Centred-Design across implementation stages, which preserved the girl-centredness throughout, including during ongoing testing in real time. ‘Society keeps changing, the communities we serve keep evolving so localisation is never over, it's never complete, so we need to continue to find solid mechanisms that keep engagement alive and keep channels of communication open and honest, so we can maintain trust, credibility and relevance. We have to keep listening and we have to be prepared to change and continue to grow. Anything other than that becomes stale, out of date and obsolete’. (KI 17)
Participants held OFP to account for realising their ideas within the applications. As participants saw their ideas coming to life within the application, KIs observed that they increasingly developed a sense of ownership and leadership over the application. Major aspects that fostered participant ownership were trusted facilitators who created safe participatory spaces and offered iterative opportunities to participate in co-creation activities. Participant ownership manifested as continuing use of the application outside of the participatory spaces, as well as championing the application with their peers, carrying out their own peer participatory practices to gather additional ideas for further co-creation activities. ‘Having the peer network is such a great help, because it's people they're familiar with, it's people they talk to regularly and feel that they can talk to about these topics, because they’re peers so they’re not scared to raise it as they might be with their parents or teachers…they go and have conversations with members of their communities and their peers and then come to us with the feedback’. (KI 06)
Contextual barriers
The war in Ukraine and the COVID-19 pandemic in Kenya changed the implementation of Oky's Girl-Centred-Design activities. During periods of movement restrictions, in-person Girl-Centred-Design activities were transferred and adapted to online forums, including WhatsApp, SMS and Zoom. This shift supported the continuance of Girl-Centred-Design activities under these conditions; however, it did introduce some new challenges. Intermittent connectivity, power cuts, the low-tech nature of some participants’ phones, or lack of device access caused delays, interrupted the activities, and excluded unconnected participants. When movement restrictions eased, broader in-person activities resumed and enabled wider participation. The Ukrainian OFP responded to the contextual changes by integrating crisis-related Oky content into their application, supporting users with menstrual product advice in disrupted markets as well as mental health support.
Girl-Centred-Design lessons learned
A number of participation, collaboration and implementation lessons were learned by the OFPs, from the Girl-Centred-Design experiences, outlined in Figure 4.

OFP's lessons learned across the Girl-Centred-Design experiences.
Participation lessons
The inclusive nature of Oky's Girl-Centred-Design method was challenged at some points by COVID-19 restrictions through the transference of Girl-Centred-Design activities online. In addition, the Nepalese OFP limited their recruitment strategies in consideration of the limited digital access factors in rural areas. The OFP reflected that integrating a more diverse participant base may make their applications more widely appealing in the future.
Empathetic facilitators, particularly women, played an important role in connecting with young girls through shared menstrual experiences. OFP recognised facilitator-participant power dynamics and used the Girl-Centred-Design method to balance these, working with participants as equals. Communicating the aims of the Girl-Centred-Design to participants was outlined as important for setting their expectations of their role in Oky's development. Interactive games and energisers were organised with participants in small groups, using informal, inclusive language which kept them engaged, particularly when discussing sensitive topics. The depth of Girl-Centred-Design activities required time and flexibility, which was set according to participants’ needs and across a number of participatory channels supporting participant ownership throughout the process. ‘After developing it [Oky] according to their feedback, the ownership seemed to change hands, the girls took [the development of Oky] up and began to own it and run it in a way. It's like the girls are our managers, they tell us what to do, and we do it. They are the new CEOs!’ (KI 17)
Implementation lessons
KI observed that participants developed communication, technology, health and leadership skills during Girl-Centred-Design activities. Further, the KI emphasised that the diversity of disciplines and skills involved in supporting and facilitating Girl-Centred-Design activities was an integral component of a digital health intervention. This included a strong technical team with knowledge of digital safeguarding as well as a range of skills to bring the participants’ ideas to life. The importance of close collaborations between technical personnel and Girl-Centred-Design facilitators remained central throughout to ensure the co-creations remained girl-centred. This was underpinned by adequate and flexible funding and time to meet the iterative pace and direction of the Girl-Centred-Design activities and support personnel.
Collaboration lessons
Leveraging community support underpinned the Girl-Centred-Design with trust and credibility and led to greater local understanding and acceptance. This was particularly prominent in the Philippines, where early engagement with government stakeholders supported the integration of Oky Girl-Centred-Design activities within the national school system across the country. Peer-to-peer mechanisms were considered highly beneficial for connecting hard-to-reach communities and including unconnected and out-of-school adolescents, and overcoming barriers related to sensitive topics. This channel was reported as ideal for gaining honest feedback. Integrating Oky within similar projects and like-minded organisations was also outlined as a mechanism to share resources and sustain Girl-Centred-Design activities as contexts and users evolved. Parents and caregivers were outlined as a group for greater future collaboration, as a strategy to increase digital access through device sharing.
The Oky Burundi launch event showcased how girl-led advocacy amplified girls’ voices directly to power when a girl-led discussion panel enabled regulatory stakeholders to hear directly from girls regarding their MHH and SRH experiences. This, alongside early and proactive engagement with regulatory authorities, was considered helpful for advocating for Oky's Girl-Centred-Design method. ‘Politics and policies have shaped Oky. That is key because myths and misconceptions are often based on community beliefs and community practices are mostly shaped by the policies that we have. So, policy and advocacy around menstrual health and hygiene make Oky and the whole conversation on menstrual health and hygiene quite active’. (KI 17)
Discussion
Summary of key findings
Our study explored how Oky's Girl-Centred-Design methodology supported meaningful participation, in line with WHO and other conceptual participatory frameworks, with adolescent girls and others, across diverse settings to develop Oky from the implementation perspective. We identified structural, cultural and contextual Girl-Centred-Design enablers, including working through peer networks and school systems, as well as barriers, including limited funding and digital access.
We also identified participation, implementation and collaboration lessons to optimise participatory practices, including allowing participants to set the pace and collaborating with a broad set of participants, from the early project stages and throughout. Exploration of our findings contributes towards broader discussions for developing and enhancing public health intervention relevance through meaningful participation.
Interpretation of findings
The Girl-Centred-Design method supported participants to take ownership of the iterative co-creation processes and develop local versions of Oky. As a result of participatory Girl-Centred-Design activities, local Oky applications were developed with grounded co-created content and features.
Considering our findings in relation to theoretical conceptions of meaningful engagement and participation with young people supports their interpretation: In line with WHO's meaningful engagement definition, 30 Oky's Girl-Centred-Design method broadly created the environment for respectful, dignified and equitable inclusion of individuals. The OFP facilitated the participatory activities to gather the lived experience of participants in relation to their menstrual health and social challenges, knowledge gaps and misconceptions. The diversity of online and offline Girl-Centred-Design activities, as supported by the Oky toolkit resources, provided a range of processes and activities within an enabling environment where power was seen to change hands between facilitators and participants, with some participants taking leadership roles, and many building skills and confidence along the way. As a result, Oky was co-created using the learnings from the Girl-Centred-Design activities, transferring the grounded experiences of participants and their lived experience as a form of expertise that developed into the content and features within the Oky applications. This resulted in six smartphone applications that are live today, supporting hundreds of thousands of users to improve their menstrual health.
Comparing our findings with conceptual participatory models further indicates the meaningfulness of Oky's Girl-Centred-Design activities. The Girl-Centred-Design implementation sits within the upper rungs of Hart's Ladder, 38 around rung six, which conceptualises adult-initiated actions with shared decision making with young people. However, as youth ownership and leadership increased, participants took greater influence, Girl-Centred-Design implementation moved up to the highest rung of the ladder, with youth-initiated and youth-directed action. Considering our findings through the lens of Lundy's domains, 39 we identified a range of safe and inclusive spaces for Girl-Centred-Design activities (space domain), in which young people were supported to express themselves through a variety of formats (voice domain). Young people, as the central participant group, were influential stakeholders (influence domain), with their ideas leading local application development (audience domain). These findings reflect a growing body of public health research that outlines how community collaboration can bridge the intervention-community gap and set the stage for participant-led development.56–61
Oky's Girl-Centred-Design method was outlined as a cultural shift, in favour of young people and their communities.62,63 Amauchi et al. 64 refer to decolonising epistemologies and feminist and gender research paradigms for challenging hierarchical knowledge-making systems and addressing social and gender inequalities for equitable futures. 64 We found that in general, adolescent girls were an often overlooked participatory group. However, Girl-Centred-Design disrupted this norm, and the co-creations indicated they were a highly valuable collaboration group. This challenges top-down approaches that assume that experts know better than young people regarding their health and social realities. As such, our study found that Oky's Girl-Centred-Design method aligns with gender, feminist and decolonising lenses in shifting towards community leadership for more equitable and inclusive power sharing. 50 64–66
Our study identified that there were challenges to the Girl-Centred-Design method in the form of structural, cultural and contextual barriers that required flexibility to navigate. In particular, regulatory restrictions underscored tensions between high-level decision-making and participant-led approaches, which meant some co-created content was reduced or removed in line with child safeguarding requirements. This highlights friction within Lundy's influence and audience domains 39 where our findings suggest that participants’ power to enact change was reduced at this point in time. These challenge aligns with broader literature,67,68 which illustrates the power of politics to shape health inequities, underscoring the importance of advocacy for participatory and co-creative approaches. UNICEF has seen examples of cases where co-created content that regulatory stakeholders wanted to remove was reinstated, where regulatory stakeholders changed their minds based on hearing the voices of girls, highlighting the power of the Girl-Centred-Design method.
Limited resources were outlined in our study. Traditional funding arrangements rely on pre-determined timelines, objectives and output frameworks.69,70 Considering these structures in relation to HCD methods, which do not always have set objectives and outputs and instead rely on creative processes, highlights tensions. A key strength of HCD methods lies in their adaptive ability to respond iteratively to contextual factors and participant requirements,71–73 and Oky's Girl-Centred-Design method also works in this way, but was limited by traditional funding parameters in some contexts. We echo Youth Participatory Action Research (YPAR) literature, which calls for flexible, long-term funding for collaborative activities that reflect the interests and needs of both implementers and communities for meaningful power-sharing.74–77
Digital tools can widen access to health information; however, without digital access, health inequalities can increase. 78 Our study highlighted digital access as a structural barrier to digital health tools, which is a major aspect of the Digital Divide.13,14,79 This disproportionately affects LMIC contexts, particularly along age, gender and socio-economic lines. In participatory spaces, access is associated with managing power, and participatory practices have the potential to disempower participants if power and social dynamics are not addressed. 80 This issue was identified in COVID-19 times, where participatory activities were transferred online, excluding unconnected groups, or where non-urban groups were excluded from participatory recruitment.
These aspects limit the diversity of participants and their value when excluded from participatory spaces. However, our study found the flexibility of Oky's Girl-Centred-Design method helpful in addressing some barriers through offering alternative formats, including non-digitalised activities, adjusting the pace and involving others. We stress the adaptability of the Girl-Centred-Design method in responding to contextual challenges and participant needs through localised approaches and note that the overall Oky portfolio also incorporates various non-digital elements, allowing for additional flexibility.
Public health literature emphasises that social determinants of health play a greater role in our lives than genetics or healthcare access. 81 This was reflected in our findings, where MHH stigma, myths and misinformation impacted menstrual and social norms and practices. We found collaboration with trusted community leaders and gatekeepers bridged gaps between OFP and participants, 82 and framed MHH and SRH content sensitively to address real challenges faced by adolescents and young people. The importance of cultural developments that resemble communities has been highlighted in other research for generating relevant interventions.83–85 This was true in our study, where activities centred around real-life and relevant issues engaged participants during Girl-Centred-Design and facilitated local Oky developments that responded to these real-life challenges.
Our findings suggest several early lessons for optimising participatory public health intervention development. Inclusive, early and diverse participation, including those in hard-to-reach areas and the unconnected, and with high-level decision-makers, was at the heart of our findings. 57 86–90 This supported Girl-Centred-Design trust, credibility and acceptance, throughout the development processes and beyond, which is echoed in other inclusion research. 91 Further, we revealed the importance of flexible, iterative and interdisciplinary approaches, underpinned by adequate resources. These aspects align with HCD and YPAR principles of adaptability, 92 which are particularly relevant for dynamic contexts and creative processes. 93 Some aspects of these findings would benefit from further development, and thus, this article provides a starting point for this.
Throughout our findings, the theme of ownership emerged. Ownership was conceptualised as participants taking greater and increasingly influential roles in the development processes and holding OFP to account regarding carrying out their co-creation wishes. This was linked with intervention sustainability through proactive, ongoing girl-led and peer-to-peer action. These themes reflect the highest points of Hart's ladder 38 and the ethos of youth leadership within YPAR. 75
Implications
As adolescence is a key developmental period for young people to establish healthy habits and important skills,94,95 expanding existing participant skill-building activities from Oky initiatives into Girl-Centred-Design activities could emphasise participation benefits, provide mutual benefit, and foster youth-led sustainability and intervention ownership for long-term Oky evolutions.
Assessing co-created public health interventions includes both processes and outcomes. 19 The addition of a girl-led participatory assessment could validate Girl-Centred-Design methods from the participant perspective and identify future opportunities for youth-led, ongoing development influence, such as scalability. Future participatory health interventions should consider how they can proactively plan for disruptions, such as pandemics or movement restrictions, by integrating flexible participatory and hybrid methods that ensure inclusion. Policy-focused implications from our study suggest early engagement and advocacy with regulators and coalitions with like-minded stakeholders 96 could mitigate participatory constraints and advocate for health rights.
Strengths and limitations
Exploring Oky's Girl-Centred-Design method from the perspective of OFP across six real-world LMIC and humanitarian contexts adds to the potential transferability of our findings to other similar country contexts where digital health tools are being considered. However, the context and organisational differences across the OFP, with varying budgets, donor requirements and team structures, as well as the number of interviews and varied desk review documents, limited standardisation across the implementation contexts studied, which introduces variability. This may mean that the findings of this study are not universally generalisable. However, the site-specific Oky developments illustrate the flexibility of Oky's Girl-Centred-Design approach to respond to diverse cultural, regulatory and structural conditions. As such, this article provides patterns and lessons that may be transferable to other similar contexts. This study focused on LMIC contexts, many of which have acute health disparities, and so further exploration of participatory digital health tools, including for other health issues, in these regions offers particular value.
The semi-structured nature of the interviews enabled exploration of the diverse roles and experiences of the Girl-Centred Design facilitators. Interviews took place remotely (online) by one interviewer, using the English language, without being present during Girl-Centred-Design participation. This approach may have inadvertently missed implied KI sentiments. Whilst validation sessions occurred with OFP, there are limitations to this approach.
This study did not include Girl-Centred-Design participants or other stakeholders, and rather focused on the perspectives of OFP as the Girl-Centred Design facilitators. Considering the highly interdisciplinary nature of Girl-Centred-Design approaches, this singular perspective may perpetuate inherent biases. Future research should be inclusive of Girl-Centred-Design participants and other stakeholders to capture and explore the participatory experience from their perspective.
Conclusion
Our study found Oky's Girl-Centred-Design method a valuable and feasible approach for facilitating meaningful participation with adolescent and young stakeholders who co-created digital health applications in diverse settings. Particularly, this supported the co-creation of contextually grounded digital health content whilst generating local intervention ownership and strengthening participants’ confidence and leadership skills. Key barriers in terms of digital access gaps, regulatory restrictions on sensitive topics and limited resources persisted. Key enablers were the strength and breadth of peer networks, trusted facilitators, participatory community spaces and the flexibility of the participatory method, including hybrid and non-digital approaches.
Our study highlights lessons for future participatory digital health development. Meaningful participation is a cultural shift in intervention development. It takes time, energy, resources and flexibility. To support this, inclusive and early participation that iterates along the development journey and beyond can build trust, credibility and relevance. Flexibility in participatory approaches supports inclusiveness and responsiveness in dynamic, real-world settings.
Our findings contribute to the digital public health evidence base and the theory of participatory development and localisation, through specifying opportunities for and barriers to participatory implementation research. Future research should broaden stakeholder inclusion and explore new validation approaches for participatory development, including intervention implementation sustainability and scalability as outcomes.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251393398 - Supplemental material for Participatory co-creation of a smartphone application using Girl-Centred-Design to support adolescent girls’ health: Barriers, enablers and lessons learned across six countries
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251393398 for Participatory co-creation of a smartphone application using Girl-Centred-Design to support adolescent girls’ health: Barriers, enablers and lessons learned across six countries by Jennifer Benson, Meret Lakeberg, Tegan Palmer, Tilman Brand and Hajo Zeeb in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076251393398 - Supplemental material for Participatory co-creation of a smartphone application using Girl-Centred-Design to support adolescent girls’ health: Barriers, enablers and lessons learned across six countries
Supplemental material, sj-pdf-2-dhj-10.1177_20552076251393398 for Participatory co-creation of a smartphone application using Girl-Centred-Design to support adolescent girls’ health: Barriers, enablers and lessons learned across six countries by Jennifer Benson, Meret Lakeberg, Tegan Palmer, Tilman Brand and Hajo Zeeb in DIGITAL HEALTH
Supplemental Material
sj-pdf-3-dhj-10.1177_20552076251393398 - Supplemental material for Participatory co-creation of a smartphone application using Girl-Centred-Design to support adolescent girls’ health: Barriers, enablers and lessons learned across six countries
Supplemental material, sj-pdf-3-dhj-10.1177_20552076251393398 for Participatory co-creation of a smartphone application using Girl-Centred-Design to support adolescent girls’ health: Barriers, enablers and lessons learned across six countries by Jennifer Benson, Meret Lakeberg, Tegan Palmer, Tilman Brand and Hajo Zeeb in DIGITAL HEALTH
Supplemental Material
sj-pdf-4-dhj-10.1177_20552076251393398 - Supplemental material for Participatory co-creation of a smartphone application using Girl-Centred-Design to support adolescent girls’ health: Barriers, enablers and lessons learned across six countries
Supplemental material, sj-pdf-4-dhj-10.1177_20552076251393398 for Participatory co-creation of a smartphone application using Girl-Centred-Design to support adolescent girls’ health: Barriers, enablers and lessons learned across six countries by Jennifer Benson, Meret Lakeberg, Tegan Palmer, Tilman Brand and Hajo Zeeb in DIGITAL HEALTH
Supplemental Material
sj-pdf-5-dhj-10.1177_20552076251393398 - Supplemental material for Participatory co-creation of a smartphone application using Girl-Centred-Design to support adolescent girls’ health: Barriers, enablers and lessons learned across six countries
Supplemental material, sj-pdf-5-dhj-10.1177_20552076251393398 for Participatory co-creation of a smartphone application using Girl-Centred-Design to support adolescent girls’ health: Barriers, enablers and lessons learned across six countries by Jennifer Benson, Meret Lakeberg, Tegan Palmer, Tilman Brand and Hajo Zeeb in DIGITAL HEALTH
Supplemental Material
sj-pdf-6-dhj-10.1177_20552076251393398 - Supplemental material for Participatory co-creation of a smartphone application using Girl-Centred-Design to support adolescent girls’ health: Barriers, enablers and lessons learned across six countries
Supplemental material, sj-pdf-6-dhj-10.1177_20552076251393398 for Participatory co-creation of a smartphone application using Girl-Centred-Design to support adolescent girls’ health: Barriers, enablers and lessons learned across six countries by Jennifer Benson, Meret Lakeberg, Tegan Palmer, Tilman Brand and Hajo Zeeb in DIGITAL HEALTH
Supplemental Material
sj-pdf-7-dhj-10.1177_20552076251393398 - Supplemental material for Participatory co-creation of a smartphone application using Girl-Centred-Design to support adolescent girls’ health: Barriers, enablers and lessons learned across six countries
Supplemental material, sj-pdf-7-dhj-10.1177_20552076251393398 for Participatory co-creation of a smartphone application using Girl-Centred-Design to support adolescent girls’ health: Barriers, enablers and lessons learned across six countries by Jennifer Benson, Meret Lakeberg, Tegan Palmer, Tilman Brand and Hajo Zeeb in DIGITAL HEALTH
Footnotes
Abbreviations
Acknowledgements
Special thanks go to the six Oky Franchise Partners, NFCC, NGO Girls, SaCoDé, Plan International Pilipinas Foundation Inc., LVCT Health and Tai Tanzania for their collaboration in this study, and to the Oky Global team at UNICEF for supporting this study. Thanks also to Jon Perkins for setting the Oky stakeholder figure (![]() ) and the Oky toolkit resources figure (Supplemental material 2).
) and the Oky toolkit resources figure (Supplemental material 2).
Ethical approval
Received from the University of Bremen Ethics Committee on 8th December 2022, reference: 2022-26).
Consent to participate
All key informants provided written informed consent prior to participating in this study.
Consent for publication
Oky figures are published with permission from the Oky Global team at UNICEF.
Contributorship
All authors (JB, ML, TP, TB and HZ) have made substantial contributions to the conception and JB, TP, TB and HZ were involved in design of the work; JB and ML in the acquisition, analysis and interpretation of data; JB drafted the work and JB, TP, TB and HZ substantively and critically revised it, and JB, ML, TP, TB and HZ approved the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted with financial support from the University of Bremen for publication costs and the Leibniz Institute for Prevention Research and Epidemiology – BIPS for the authors’ time. The funding organisations had no role in the design of the study, data collection, analysis, interpretation, or writing of the manuscript.
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Tegan Palmer is a consultant for UNICEF's Oky Core Team. She was not involved in data collection or analysis.
Guarantor
XXX
Data availability
In line with the agreement made with key informants, the data for this study is not made available.
Some KI quotes have been edited for grammatical and brevity purposes.
Authors’ information
Please see Supplemental materials 4: Reflexivity statement for author details.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.