
Abstract
Objective
Pulmonary telerehabilitation (PTR) has emerged as a promising mobile health approach to address post-discharge challenges faced by patients with chronic pulmonary disease (CPD), including limited professional support, physical discomfort, and declining motivation that may compromise adherence and lung function. Challenges exist in traditional hospital-based rehabilitation, constrained by logistics, limited capacity, and accessibility, especially for elderly or mobility-impaired individuals. This study aimed to investigate the feasibility and usability of a novel home-based PTR system (Intelligent Pulmonary Rehabilitation Exercise System (IPRES)), eliciting user experience reported by a cohort of outpatients with relevant respiratory diseases.
Methods
This questionnaire-based, quantitative, single-group pretest–posttest pilot study involved 36 post-discharge CPD patients, predominantly at GOLD stage 3, transitioning from hospital-based to home-based pulmonary rehabilitation
Results
Participants reported high usability, with a mean SUS score of 78.87 ± 6.32. Qualitative feedback indicated that personalized feedback, collaborative goal-setting, and gamified interactions enhanced engagement and motivation, with participants highlighting improved understanding of exercise goals, increased confidence in self-managing rehabilitation, and enjoyment of interactive training tasks.
Conclusion
This pilot study demonstrates that IPRES is feasible and well-received, highlighting usability strengths and engagement factors that can inform future optimization and randomized controlled trials. While medium- and long-term effectiveness requires further evaluation, these findings support the potential of IPRES as a scalable, patient-centered tool for home-based pulmonary rehabilitation.
Keywords
Introduction
Chronic pulmonary diseases (CPDs) comprise a prevalent group of long-term, irreversible health conditions,1,2 with chronic obstructive pulmonary disease (COPD) representing the majority, according to reports by the World Health Organization.3–5 COPD continues to be a leading cause of mortality both globally and in Taiwan.5–7 Given environmental factors such as Taiwan's aging population, high smoking prevalence, and extensive motor vehicle usage, the incidence and healthcare burden associated with pulmonary obstruction are projected to rise significantly.4,8
Patients with CPD often suffer from persistent symptoms such as chronic coughing, sputum production, and exertional breathlessness, which frequently discourage regular exercise participation.9,10 Additionally, impaired respiratory function leads to fatigue and muscle weakness, which, coupled with psychological distress and decreased motivation, significantly hinder adherence to pulmonary rehabilitation (PR) programs. 11 These multifactorial barriers highlight the urgent need for accessible, patient-centered digital interventions that support home-based rehabilitation and promote sustained disease management.12,13
Research indicates that physical exercise enhances pulmonary capacity and psychological well-being in patients with CPD. 14 Stationary cycling is widely used as a low-impact rehabilitation modality, 15 yet such interventions are typically confined to clinical settings due to the need for professional supervision and specialized equipment.16,17 After hospital discharge, patients often lack ergonomic infrastructure and effective home monitoring, undermining consistent and structured exercise, and contributing to poor adherence, recurrent readmissions, and reduced self-management.18,19 Previous studies have shown that home-based PR (HBPR) can achieve comparable safety, exercise capacity, and health-related quality of life (HRQoL) outcomes to center-based programs, often with higher engagement.20,21 However, most prior research focused on stable COPD populations, excluding patients recently discharged after acute exacerbations.
Recent literature highlights a growing trend toward home-based and remote rehabilitation modalities, driven by the demand for accessible, patient-centered care among individuals with CPD.22,23 Despite increasing interest in home-based pulmonary telerehabilitation (PTR), most research has focused on clinical feasibility and physiological outcomes, with limited attention to user-centered factors critical for sustained engagement. These include patient acceptance, health literacy, system usability, motivation, self-efficacy, goal-setting participation, and quality of interaction with digital interfaces—all vital to maintaining adherence and promoting long-term behavioral change.24–26
PTR has demonstrated efficacy comparable to conventional PR in improving patients’ quality of life, while offering advantages in accessibility, continuity of care, and patient engagement—particularly in home-based settings, 27 Clinical studies consistently report positive outcomes such as enhanced exercise capacity, reduced dyspnea, and improved psychosocial well-being, supporting PTR as a viable and scalable alternative to traditional PR programs.28,29
To address these gaps and evaluate usability in CPD patients, this study implemented the Intelligent PR Exercise System (IPRES), a home-based digital health platform. IPRES was designed to support engagement, continuous monitoring, and adaptive exercise guidance during the transition from hospital-based rehabilitation to self-managed home care. A detailed description of the IPRES system design and features is provided in the Methods section under “System Design Overview” of the IPRES platform.
This study aimed to evaluate the usability and user experience of IPRES in facilitating sustainable home-based PTR for patients with CPD. A human-centered usability evaluation assessed user acceptance, system engagement, and perceived effectiveness during the critical transition from supervised hospital care to self-managed rehabilitation. Insights from this study seek to inform the design and implementation of scalable digital rehabilitation solutions that effectively promote patient engagement and adherence in real-world settings.
Conceptually, the platform integrates an ergonomically designed cycling interface, wearable physiological sensors, and a tablet-based interactive module to provide personalized feedback and gamified training experiences. Collaborative goal-setting features reinforce self-efficacy and support long-term adherence, while the system aligns with hospital-derived assessments to ensure continuity of care. These human-centered design principles optimize IPRES for real-world home deployment and advance the broader adoption of sustainable, patient-centered digital PR models.
Methods
Study design and implementation
This study primarily aimed to enhance the implementation of PTR by identifying and addressing key barriers to sustained patient engagement. Acknowledging that adherence depends on daily routines and autonomy, the IPRES was developed within a human-centered design framework. The system specifically supports patients’ transition from structured, hospital-based rehabilitation to flexible, self-directed home care.
This study was conducted at the Respiratory Therapy Unit of Chang Gung Memorial Hospital and employed a primarily quantitative design. Usability was assessed using the System Usability Scale (SUS), a validated 10-item questionnaire. In addition, participants were invited to provide brief open-ended feedback on their experiences with the program and use of the IPRES; these comments were summarized descriptively to contextualize questionnaire findings rather than subjected to formal qualitative analysis. Due to the difficulty of recruitment and screening, participant enrollment extended over a three-year period (2021–2024).
A user-centered, single-group pretest–posttest design was employed to evaluate the feasibility and user experience of the IPRES platform. Usability was assessed primarily with the SUS, complemented by structured questionnaires covering engagement, motivation, behavioral intention, clarity of exercise goals, sense of autonomy, emotional responses, and willingness to sustain self-managed rehabilitation. In addition, participants provided brief open-ended feedback to contextualize questionnaire findings. Comparisons with prior conventional rehabilitation experiences were performed to identify facilitators and barriers to long-term adherence and to determine whether IPRES's human-centered features could support behavioral change and sustained participation in home-based PR.
Recruitment and study procedure
Two weeks prior to hospital discharge, participants were introduced to the IPRES and provided written informed consent before study enrollment (IRB approval number: 202200070B0). Participants received anonymized identifiers, and all personal data were encrypted and stored in a secure cloud environment accessible only to authorized clinical staff in compliance with IRB requirements.
A total of 36 participants, aged 42–85 years, diagnosed with CPD were recruited. They were recruited from a tertiary hospital affiliated with Chang Gung Medical College based on physician evaluation and clinical recommendation. COPD severity was classified according to GOLD stages 1–4 based on spirometry, providing important clinical context as varying degrees of obstruction may influence exercise tolerance, system usability, and adherence to rehabilitation. Most participants were GOLD stage 3, often hospitalized due to acute pulmonary exacerbations with severe dyspnea. Following inpatient treatment and stabilization, these patients were identified by physicians as requiring close monitoring and individualized exercise prescriptions to support continued home-based rehabilitation. All participants had completed an eight-week hospital-based conventional PR program before enrollment, ensuring comparable clinical stabilization and rehabilitation experience. 30
Intervention overview
This study targeted high-risk, post-discharge CPD patients, predominantly GOLD stage 3, transitioning from hospital-based conventional PR to a home-based telerehabilitation program using the IPRES. Under physician-directed assessment, individualized and adaptive exercise programs were prescribed, accompanied by continuous physiological monitoring, enabling evaluation of feasibility, usability, and adherence in a population underrepresented in prior home-based PR (HBPR) research.
During the introductory sessions, participants engaged in individualized lower-limb pedaling exercises using the recumbent bicycle component of IPRES. Each session was supported by a scenic virtual interface displayed on a tablet application to enhance immersion and motivation. Real-time physiological monitoring—including heart rate and oxygen saturation—was conducted via a wearable pulse oximeter to ensure safety and support adaptive exercise progression.
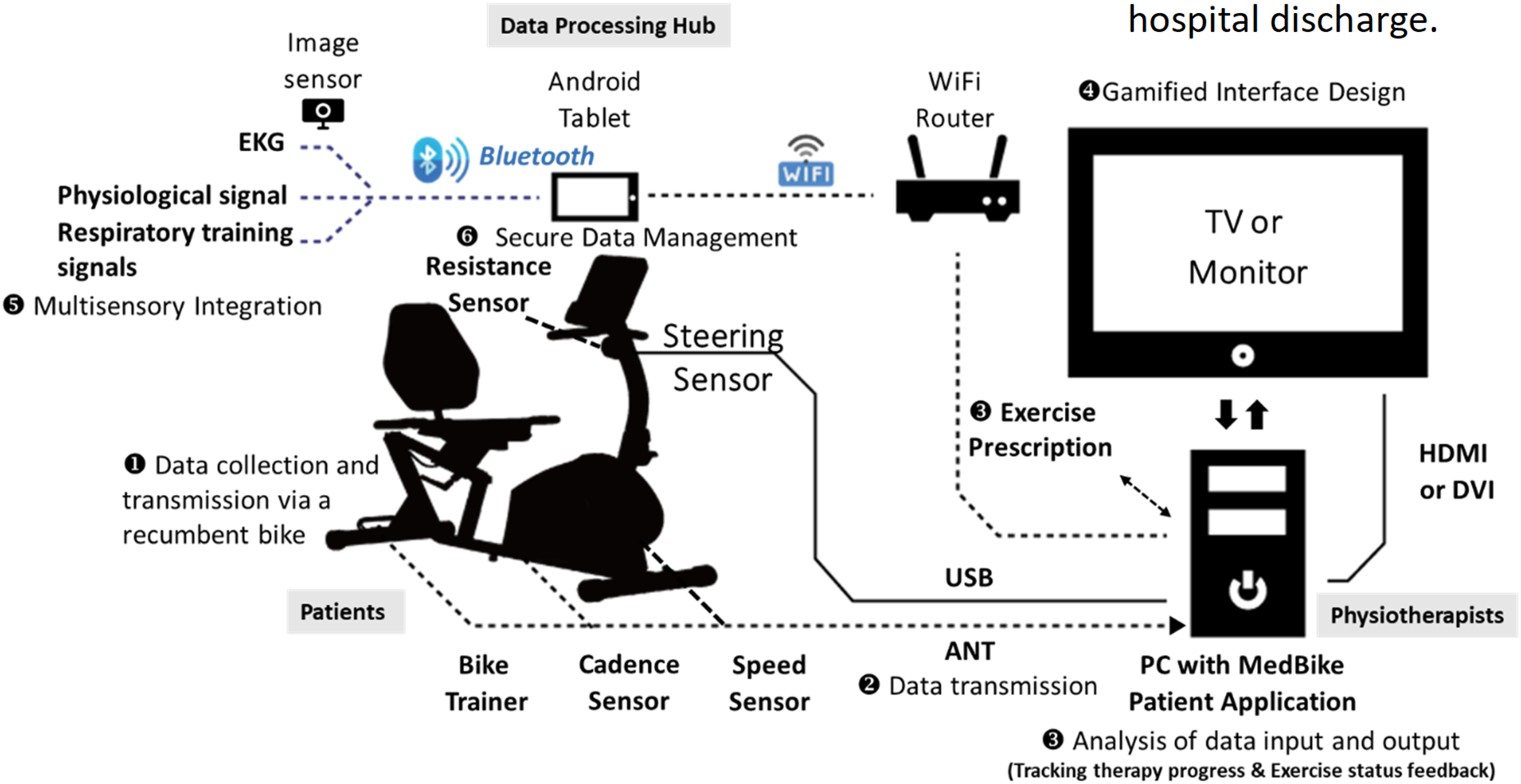
As illustrated in Figure 1, IPRES provides an integrated home-based intervention comprising an ergonomically designed recumbent bicycle with adjustable resistance, a tablet-based telehealth interface featuring gamified rehabilitation tasks, wearable sensors for real-time physiological monitoring, and a cloud-based portal for clinician oversight. The system delivers personalized training goals based on hospital-derived assessments and embeds interactive gaming elements, real-time biofeedback, and visual progress tracking to enhance motivation, strengthen self-efficacy, and facilitate shared goal setting. These human-centered features address common barriers to adherence in traditional rehabilitation by promoting sustained engagement and autonomous participation.

Real-time data exchange framework of the Intelligent Pulmonary Rehabilitation Exercise System (IPRES).
System design overview of the IPRES platform
Overview
The IPRES was developed as a comprehensive home-based digital health platform to support telerehabilitation for patients with CPD (Figure 1). The system was designed to facilitate the transition from hospital-based supervision to self-managed rehabilitation at home, addressing barriers such as physical discomfort, low motivation, and limited self-monitoring. This study focused on evaluating usability, patient receptiveness, and overall user experience, with the goal of informing scalable, patient-centered PTR solutions.
Hardware components
Ergonomic recumbent bicycle: Adjustable features minimize fall risk and accommodate diverse anthropometrics, providing a safe and comfortable exercise interface for elderly or mobility-impaired patients. Wearable sensors: Wireless physiological sensors continuously monitor heart rate, peripheral oxygen saturation (SpO₂), and blood pressure, transmitting data via Bluetooth Low Energy (BLE) to the tablet interface for real-time feedback. Software architecture
Tablet-based application (Android OS): Delivers gamified rehabilitation modules with interactive challenges and real-time visual feedback. Cloud-based backend: Provides secure data storage, management, real-time analytics, clinician dashboards, and automated alerts for abnormal physiological readings or low compliance. Integration with hospital assessments: Exercise prescriptions and goals are aligned with inpatient evaluations to ensure clinical continuity. AI-driven personalization
Adaptive algorithms: Continuous physiological and behavioral data are analyzed using machine learning to dynamically adjust exercise prescriptions. FITT-based personalization: Exercise programs follow the FITT principles (Frequency, Intensity, Time, and Type) and are refined in real time based on patient performance and physiological response. Human-centered features. IPRES incorporates core interactive features designed to enhance patient engagement and support home-based rehabilitation (Figures 2 and 3).
Gamification: Interactive challenges, scenic environments, and progress tracking foster engagement and enjoyment. Real-time biofeedback: Enhances bodily awareness and safety through continuous performance monitoring. Collaborative goal-setting: Supports communication between patients and providers, strengthening self-efficacy and promoting long-term adherence. Social connectivity: Online community features provide peer interaction and emotional support, contributing to sustained behavior change. Data security and privacy
Participants were assigned anonymized identifiers, and informed consent explicitly addressed AI operations and data use. All data were encrypted in transit (TLS 1.2) and at rest, stored in a cloud environment compliant with IRB and HIPAA standards. Role-based access control limited data access to authorized clinicians, and regular audits ensured confidentiality and integrity. Operational workflow. Figure 4 illustrates the operational workflow of the IPRES platform. Participants followed a structured protocol consisting of initial screening, baseline assessments, and scheduled home-based training sessions. Post-intervention, usability and engagement were compared with prior conventional rehabilitation experiences to identify facilitators and barriers to adherence. Automated FITT-based prescription. Continuous physiological data (e.g. heart rate, SpO₂, and workload) are analyzed by AI/ML algorithms to dynamically generate and refine individualized exercise prescriptions following the FITT principles. Rule-based safeguards ensure safe adjustments despite missing or noisy sensor data, thereby enhancing both personalization and safety. Real-time data synchronization. Exercise and monitoring data are uploaded to a secure cloud portal, enabling clinicians to review progress and provide timely feedback. Closed-loop feedback. Physiological and behavioral indicators are integrated into a bidirectional adaptive framework. The system autonomously adjusts exercise parameters while clinicians can intervene remotely, supporting sustained participation and long-term behavioral change. Gamified rehabilitation interface. A tablet application provides interactive cycling tasks with real-time feedback, designed to sustain motivation and enjoyment. Multisensory physiological monitoring. Wearable sensors continuously track SpO₂, heart rate, and exercise workload. Data processing techniques mitigate signal noise to preserve the reliability of feedback, with clinical safeguards ensuring safe home use. Secure and visualized data management. Encrypted cloud storage and infographic dashboards facilitate shared decision-making and empower patients to track their progress.

Home-use simulation setup integrating a gamified interface, wireless biosensors, and adjustable resistance cycling.

Interactive interface design integrating real-time biofeedback to foster bodily awareness and progress tracking.
Operation workflow of the Intelligent Pulmonary Rehabilitation Exercise System (IPRES).
Together, these features establish IPRES as a practical and patient-centered digital health solution, designed to enhance engagement, promote adherence, and ensure continuity of PR beyond hospital discharge.
Usability testing protocol
This study employed a structured usability evaluation to assess not only the technical performance, safety, and environmental compatibility of the IPRES, but also to examine how its design influences patients’ perceptions of conventional rehabilitation and promotes long-term engagement and health-related behaviors. The IPRES evaluation protocol consisted of the following components:
Observational analysis of system operation to assess technical stability, physical safety, and environmental suitability, ensuring alignment with the functional needs and limitations of patients with CPD. Usability assessment of telehealth tablets and wearable devices, focusing on intuitiveness, ease of setup, and reliability during unsupervised use—factors critical for fostering user confidence and autonomy in home-based settings. Patient-reported outcomes collected through structured surveys to evaluate acceptance, comfort, and satisfaction with the IPRES-based rehabilitation experience. These responses were used to compare perceptions of traditional versus digital rehabilitation, with particular attention to shifts in motivation, goal clarity, and willingness to sustain self-directed rehabilitation—key indicators of engagement and potential behavior change.
Statistical analysis
To evaluate the feasibility and usability of the IPRES as a therapeutic intervention, quantitative assessments were conducted using two validated instruments: the SUS and the Post-Study System Usability Questionnaire (PSSUQ).31,32 These tools were chosen for their reliability in capturing user experience across digital health interventions.
Usability was conceptualized through three core dimensions:
Effectiveness—the extent to which users were able to complete intended tasks successfully. Efficiency—the resources (e.g., time, cognitive effort) required to complete those tasks. Satisfaction—users’ subjective evaluation of the system's overall usability and their experience during use.
Reliability analysis demonstrated good internal consistency for the SUS scores, with a Cronbach's alpha of 0.721. The observed mean SUS score was compared against the widely accepted benchmark of 68, as established by Sauro (2018), to provide context for the usability outcomes. The SUS, a standardized 10-item instrument comprising five positively and five negatively worded statements, yields scores ranging from 0 to 100 and is commonly used to evaluate perceived usability across digital systems. This comparison provides a reference point to assess whether user perceptions of IPRES usability meet, exceed, or fall short of normative expectations in human–computer interaction research.
To evaluate the feasibility and usability of the IPRES as a therapeutic intervention, quantitative assessments were conducted using two validated instruments: the SUS and the PSSUQ, both widely recognized for measuring system usability and user acceptance. Usability was conceptualized along three core dimensions: effectiveness, efficiency, and satisfaction.
Crucially, these usability outcomes were interpreted in the context of patient engagement, recognizing that positive user experiences—characterized by successful task completion, minimal effort, and high satisfaction—are linked to increased motivation, improved adherence to rehabilitation protocols, and greater patient autonomy. Thus, this evaluation aimed not only to assess technical performance but also to determine whether IPRES empowers patients to actively manage their recovery.
Descriptive statistics summarized SUS and PSSUQ scores, while exploratory analyses examined usage patterns and identified potential usability barriers that might affect long-term adherence and system adoption.
To complement these standardized measures, a custom 5-point Likert-scale questionnaire was developed to capture participants’ subjective experiences with IPRES in greater detail. Responses ranged from 1 (strongly disagree) to 5 (strongly agree), with 3 indicating neutrality.
This supplementary questionnaire targeted practical aspects of user interaction and personal engagement with the IPRES platform, focusing on three key domains:
Physical comfort and usability, including seat adjustability, ease of interacting with the touchscreen and pulse oximeter, and clarity of information displayed on the tablet interface. Interface comprehension and clarity, emphasizing users’ ability to understand exercise instructions and navigate the gamified rehabilitation tasks. Overall user experience, covering satisfaction, perceived usefulness, motivation to continue training, and willingness to incorporate the system into long-term self-managed rehabilitation.
Statistical analyses were performed using IBM SPSS Statistics version 25. A single-group pretest–posttest design enabled evaluation of both initial user impressions and changes in usability and engagement over time. All assessments were conducted using standardized, structured questionnaires with pre-defined response options, indicating a fully quantitative approach without qualitative or freeform components.
Results
A total of 36 patients diagnosed with CPD were enrolled in the study. Results focus on behavioral engagement, usability, and self-management to assess the feasibility of home-based PTR. Usability was primarily evaluated using the SUS, a validated 10-item questionnaire with predefined response options. In addition, participants were invited to provide brief open-ended feedback regarding their experiences with the PR program and use of the IPRES. These narrative comments were summarized descriptively rather than subjected to formal qualitative analysis. Baseline demographic and clinical characteristics of the cohort—including medical history, comorbidities, and recent hospitalization details—are summarized in Table 1. These data offer important context for interpreting the usability outcomes and patient-reported experiences.
Characteristics of the participants (n = 36).

Phase 1: Initial ergonomic feasibility evaluation
Participants performed baseline exercise sessions in a simulated home-use environment while trained evaluators observed physical comfort, interface accessibility, and task completion using a structured checklist. Notes were documented to provide a comprehensive assessment of user-system interaction and identify potential usability challenges.
Participants <160 cm experienced limited pedal reach, and minor seat adjustments improved comfort and performance, supporting engagement. System feasibility was further evaluated post-discharge, focusing on operational performance, clarity of instructions, and participant acceptance.
Some participants reported reduced motivation during home use, often linked to system latency and session duration, highlighting the importance of timely feedback. Stable internet connectivity was essential for real-time data logging; interruptions affected confidence and perceived control.
The dual-screen setup increased cognitive load, particularly for older adults with mild visual or digital literacy limitations, suggesting a need for consolidated, intuitive visual feedback.
Overall, usability challenges related to interface complexity, ergonomics, and technological accessibility directly influenced engagement and adherence. These observations informed iterative refinements to enhance the IPRES platform's capacity for sustained home-based rehabilitation and support positive health behavior change.
Phase 2: Formal usability testing
Following Phase 1, formal usability testing was conducted with 36 post-discharge CPD patients at the Respiratory Therapy Department of Chang Gung Memorial Hospital. Participants completed the IPRES intervention and provided feedback via the SUS and an adapted version of the PSSUQ. Responses were recorded on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree).
The mean SUS score was 78.87 ± 6.32, reflecting participants’ high perceived usability, ease of use, and acceptance of the system (Figure 5). Qualitative feedback highlighted areas for refinement, including device ergonomics, interface clarity, and session pacing, providing actionable insights to enhance sustained engagement and home-based PR adherence.

Mean SUS scores for IPRES and their standard deviation among participants (n = 36).
Beyond technical usability, several questionnaire items specifically targeted the impact of the IPRES platform on patient engagement, including motivation to continue rehabilitation, clarity of rehabilitation goals, perceived autonomy, and willingness to adhere to the program after discharge. Responses to these engagement-related measures were consistently positive, indicating that the system's gamified interface, real-time feedback, and personalized goal-setting features effectively enhanced user involvement and intrinsic motivation.
Participant perceptions of usability and engagement
Participants provided feedback on usability and engagement using structured questionnaires, including Likert-scale items. Overall, participants reported favorable perceptions across key usability dimensions, including system acceptance, comprehension, and overall satisfaction. Specifically, 77.8% of respondents indicated a greater willingness to use the IPRES platform compared with conventional PR methods, 83.3% expressed confidence in learning to operate the system with minimal effort, and 91.7% rated the system as easy to use. Additionally, 75% reported confidence in using the system independently, indicating readiness for self-managed home rehabilitation.
Minor usability challenges were reported, including perceived operational complexity (5.6%), belief that prior experience was necessary (36.1%), dissatisfaction with system design (11.1%), inconvenience during use (8.3%), and concerns regarding the time required for familiarization (25%). These quantitative findings are summarized in Table 2.
Participants’ responses to the System Usability Scale (SUS) for the Intelligent Pulmonary Rehabilitation Exercise System (IPRES) (n = 36).

Note:
1. SUS is a 10-item Likert scale (1–5); items 2, 4, 6, 8, 10 are reverse-coded.
2. SUS scores range from 0 to 100; higher scores indicate greater usability.
3. Mean SUS score = 78.87 ± 6.32, indicating above-average usability.
All participants completed the questionnaire; percentages are rounded.
Overall, the structured questionnaire results indicate that the IPRES platform achieved high usability and supported key aspects of patient engagement, including motivation, perceived control, and intention to maintain exercise behaviors after discharge. Areas identified for improvement, such as interface clarity and ergonomic adjustments, provide guidance for future iterations of the platform.
Overall, participants reported positive perceptions of the IPRES in terms of acceptance, usability, clarity, and functional coherence, as demonstrated by high agreement rates on key evaluation items. Specifically, 77.8% of participants expressed willingness to frequently use the IPRES platform, compared to only 33% who were willing to continue hospital-based rehabilitation. Moreover, 69.4% disagreed that extensive learning was necessary, indicating a relatively low cognitive load. A majority of users (91.7%) found the system easy to operate, while 83.3% agreed that its features were well integrated. Additionally, 75% of participants felt confident in independently using the system. These findings suggest that IPRES effectively mitigates psychological and technical barriers, thereby promoting increased patient autonomy and motivation. Collectively, these user responses highlight a strong readiness to engage in rehabilitation activities, emphasizing the system's potential to enhance patient engagement across cognitive, emotional, and behavioral domains.
A minority of participants reported certain limitations with the IPRES. Specifically, 5.6% perceived the system as overly complex to operate, compared to 39% who found the hospital-based rehabilitation process somewhat complicated. Additionally, 36.1% felt that professional or experienced assistance was necessary when using IPRES, which is lower than the 56% reporting similar needs during conventional rehabilitation. Regarding design coherence, 11.1% expressed dissatisfaction with the system's integration, whereas 36% voiced similar concerns about the organization of hospital rehabilitation. Moreover, 8.3% found IPRES cumbersome, in contrast to 58% who experienced conventional rehabilitation as somewhat troublesome. Finally, while 25% reported that IPRES involved a significant learning curve, a greater proportion (39%) indicated needing to acquire substantial knowledge or skills for hospital-based training. Collectively, these comparative results indicate that despite areas requiring improvement, the IPRES imposes substantially fewer operational and cognitive barriers than traditional rehabilitation methods. This reduction in complexity and reliance on professional support may lower barriers to patient participation and enhance engagement, particularly for individuals with limited prior rehabilitation experience.
Participants’ positive evaluations of the IPRES were largely attributed to its well-integrated and user-friendly interface. Specifically, 83.3% agreed that the system's functions were well organized, compared to only 42% expressing similar satisfaction with the structure of conventional hospital-based rehabilitation routines. The interface also enhanced clarity and responsiveness; 52.8% of participants confirmed the presence of clear error feedback, and 66.7% reported being able to independently identify and correct mistakes, whereas only 25% felt similarly capable in the traditional hospital setting. These design features appear to reduce cognitive and procedural barriers that commonly impede patient engagement. Supporting this, 91.7% found the IPRES easy to use, and 63.9% considered it functionally comprehensive, suggesting that a well-structured, self-guided interface may empower patients to engage more actively and confidently in their rehabilitation.
Beyond functional performance, the IPRES elicited a notably more positive emotional response from users compared to their previous experiences with traditional hospital-based rehabilitation. Specifically, 83.4% of participants reported feeling happy, and 80.6% felt entertained while using IPRES, whereas many characterized conventional rehabilitation as less engaging and often monotonous. Rather than viewing IPRES solely as a clinical intervention, participants perceived it as an enjoyable and motivating activity. These emotional benefits likely contributed to enhanced motivation and greater willingness to participate, closely aligning with core aspects of patient engagement. Nonetheless, despite these favorable impressions, 63.9% of users acknowledged that the interface design could be further improved, highlighting the importance of continued user-centered development to optimize usability and maintain sustained patient engagement (see Table 3).
Results of the Post-Study System Usability Questionnaire (PSSUQ) for the Intelligent Pulmonary Rehabilitation Exercise System (IPRES) (n = 36).

Note: Percentages may not total 100 due to rounding.
Discussion
This study advances the field of PTR by demonstrating the feasibility and strong usability of the IPRES in facilitating home-based care for patients with CPD. Unlike prior HBPR studies,20,33 which primarily targeted stable COPD populations and focused on therapeutic outcomes, our study focused on high-risk, post-discharge patients, predominantly GOLD 3, integrating physician-directed assessment with AI-driven, adaptive exercise prescriptions.
The ergonomic, user-centered design of IPRES effectively addresses common barriers to long-term adherence, such as physical discomfort, motivational challenges, and lack of real-time feedback. Automated personalized exercise prescriptions based on FITT principles, multisensory biofeedback, and gamification were observed to enhance autonomy, self-efficacy, and sustained participation during the study period, aligning with prior evidence that individualized programs and remote supervision enhance behavioral engagement and self-management. However, conclusions regarding medium- or long-term adherence, safety, or clinical effectiveness cannot be drawn from this pilot study.
Cloud-based closed-loop monitoring and machine learning algorithms enable clinicians to remotely tailor interventions based on continuous physiological and behavioral data, extending usability and engagement capabilities beyond prior studies that offered limited individualized monitoring. While AI-driven personalization shows promise for supporting behavioral change, the current study only assessed short-term interaction and immediate user experience. Future research employing longitudinal study designs is necessary to determine whether these adaptive strategies can sustain long-term participation and translate into clinical benefits.
Our findings underscore strong usability, with a mean SUS score of 78.87 (SD = 6.32), reflecting high user acceptance, ease of use, and satisfaction—indicating that IPRES is feasible and well-received in a short-term home-based setting. Minor improvements, including stable connectivity and optimized bike ergonomics, remain essential.
Compared with previous HBPR reviews, our study demonstrates short-term feasibility in a higher-risk population recently hospitalized for acute exacerbations, addressing engagement, real-time monitoring, and individualized exercise prescription within the study period. However, these results cannot be generalized to long-term adherence, safety, or clinical effectiveness. The observed usability outcomes underscore the potential of user-centered design and AI-assisted home-based rehabilitation, but further longitudinal studies are required to assess sustained engagement and health-related impacts.
Collectively, these findings underscore the critical role of user-centered design in promoting patient engagement, as observed in the short-term evaluation, which may influence adherence in a home-based setting but does not directly measure long-term outcomes. Unlike prior studies focusing primarily on therapeutic efficacy, our study emphasizes the PTR experience from the patient's perspective, highlighting system usability, user acceptance, and patient comprehension. These observations were captured primarily via structured questionnaires (e.g. SUS), providing a quantitative, patient-centered evaluation that differentiates our approach from earlier investigations. For instance, Holland et al. developed a remote HBPR system tested on eight COPD patients (mean age 66) with moderate lung impairment, concentrating mainly on clinical outcomes such as exercise capacity and health-related quality of life, with limited focus on usability or patient experience. In contrast, our study systematically examines short-term user interaction, emotional responses, and willingness to engage, without inferring medium- or long-term clinical effectiveness. 34
The IPRES demonstrates the feasibility, safety, and strong usability of HBPR for high-risk, post-discharge CPD patients, with a mean SUS score of 78.87 (SD = 6.32) and high overall satisfaction. Consistent with prior systematic reviews,20,34 short-term observations suggest that HBPR can achieve engagement levels comparable to center-based programs (73%–98% session attendance), although long-term adherence and clinical efficacy were not assessed in this study. Unlike earlier studies that focused primarily on stable COPD populations or limited individualized monitoring, 35 IPRES integrates physician-directed assessment, AI-driven adaptive prescriptions, real-time biofeedback, and gamification, thereby tailoring interventions to evolving patient needs and addressing common barriers such as ergonomic challenges and digital literacy.
Beyond clinical efficacy, this study emphasizes the patient experience in PTR, highlighting usability, acceptance, and comprehension as assessed through structured questionnaires as critical determinants of short-term engagement. Our comprehensive satisfaction survey revealed high acceptance while identifying areas for refinement, such as network stability and ergonomic optimization. Compared with previous research, which focused mainly on exercise capacity and HRQoL,36,37 our study systematically examined short-term user interaction, emotional responses, and willingness to engage, without inferring medium- or long-term rehabilitation success, underscoring the pivotal role of patient-centered design in ensuring long-term rehabilitation success.
Telerehabilitation provides advantages over conventional hospital-based rehabilitation, including accessibility, reduced travel burden, and potential cost savings. 38 User-centered elements such as real-time feedback, gamification, and social support may enhance short-term motivation and engagement, which are important for potential adherence, although long-term outcomes were not assessed in this study. 39 The IPRES exemplifies this approach by integrating individualized exercise prescriptions with physiological monitoring and psychological, social, and behavioral support. Participants reported high satisfaction and usability, though areas for improvement were noted. From a human factors perspective, the limited adjustability of the stationary bike caused discomfort in upper and lower limbs, while the dual-display setup—with small fonts and split attention between a virtual environment and physiological data—hampered comprehension and focus. These findings underscore the need for adjustable, ergonomically designed equipment and integrated, intuitive interfaces. Addressing such challenges is important to optimize short-term usability and support self-managed PR within the scope evaluated.
Professional nursing staff primarily operated the IPRES during hospitalization, contributing to high usability scores and rapid error correction. Post-discharge, patients and caregivers must assume greater autonomy, emphasizing the importance of intuitive system design that supports independent use. Simplified operation, clear feedback, and caregiver-friendly features are critical for maintaining short-term engagement and user satisfaction and ensuring continuity of care, while medium- and long-term adherence and effectiveness remain to be established in future studies, particularly in contrast to hospital-based programs with continuous clinical supervision.
Study strengths and limitations
Strengths of this study include direct comparison of user experiences between conventional hospital-based and home-based PR. Limitations include the single-group design, modest sample size, evaluation conducted primarily during hospitalization, potential bias from personalized support during assessments, and participants’ physical limitations affecting independent use. Although IPRES incorporates a closed-loop adaptive framework, this study did not systematically quantify latency, error rates, or robustness of real-time adjustments. The absence of a control group and comparison with other treatment modalities further limits generalizability. Future research should assess unsupervised home use over extended periods, in real-world settings, and leverage longitudinal multimodal data to refine AI-driven personalization, validate algorithmic decisions, and optimize patient-centered outcomes. Additionally, adequately powered randomized controlled trials with appropriate blinding are needed to evaluate longer-term safety, efficacy, and adherence.
Beyond technical and usability considerations, ethical compliance, patient trust, and system scalability are critical for AI-assisted home-based rehabilitation. All participants’ data were anonymized, encrypted, and stored in controlled cloud environments, compliant with IRB and HIPAA regulations, while access was restricted to authorized clinical personnel. The transparent implementation of decision-tree models and RL, coupled with clear communication about data use, likely contributed to participant confidence. Additionally, IPRES's modular cloud-based architecture and remote monitoring capabilities have the potential for scalability and integration with electronic health records, as well as short-term resource optimization observed in this pilot study. Future research should investigate how algorithm transparency, privacy assurances, regulatory compliance, and operational feasibility influence patient engagement, sustained use, and medium- to long-term implementation across healthcare systems.
The primary objective of this study was to evaluate IPRES's impact on patient behavior, usability, and self-management using structured, questionnaire-based assessments (primarily the SUS), rather than direct clinical outcomes. While the current study focused on usability and behavior-driven engagement, the medium- and long-term clinical efficacy—including lung function, exercise tolerance, and symptom control—remains to be investigated in future studies. Integration of continuous physiological and behavioral data through adaptive algorithms may enable future research to explore potential correlations between engagement patterns and clinical improvements, but such outcomes were beyond the scope of the present pilot investigation.
Conclusion
In this pilot study of 36 participants, we evaluated the usability and patient experience of a home-based PTR platform (IPRES). Participants reported high levels of usability, engagement, and satisfaction with the gamified interface and monitoring features. The platform integrates personalized exercise protocols while supporting patient autonomy and accessibility. Although clinical efficacy and long-term behavioral outcomes were not assessed, the findings suggest that IPRES may have potential as a scalable solution for home-based PR and warrant further evaluation in larger, longitudinal studies.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251393295 - Supplemental material for Design of an AI-driven home-based pulmonary telerehabilitation system to enhance patient engagement
Supplemental material, sj-docx-1-dhj-10.1177_20552076251393295 for Design of an AI-driven home-based pulmonary telerehabilitation system to enhance patient engagement by Shih-Ying Chien, Han-Chung Hu and Winston Tseng in DIGITAL HEALTH
Footnotes
Acknowledgements
We express our gratitude to all participants in this project for their generous contribution of time, sharing of usage experiences, and insights, which greatly enriched this study. Furthermore, we extend our special thanks to the Respiratory Therapy Department at Chang Gung Memorial Hospital for their clinical support throughout this research endeavor.
Ethical approval
This study was approved by the Research Ethics Committee of Chang Gung Medical Foundation (Institutional Review Board, IRB No. 202200070B0).
Consent to participate
All participants provided written informed consent prior to enrollment in the study.
Authors’ contributions
SY Chien contributed to the study design, data analysis, and manuscript drafting. HC Hu was responsible for site coordination and patient referrals and provided recommendations for testing procedures. Winston Tseng assisted with manuscript revision and provided suggestions from the perspectives of community health and home care.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Science and Technology Council (grant numbers 111-2222-E-182-02-MY2, 113-2221-E-182-057, and 114-2221-E-182-048).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets utilized in the present study are not publicly accessible due to the need to safeguard participants’ personal data. However, interested parties may obtain access to the datasets by contacting the corresponding author and making a reasonable request.
Clinical trial registration
Not applicable.
Additional notes on study execution
All usability testing was conducted using structured, pre-defined questionnaires, including the System Usability Scale (SUS) and complementary engagement surveys. No qualitative interviews or free-form responses were collected, and therefore no thematic analysis was performed. The evaluation report summarized quantitative questionnaire results only, providing insights into usability, engagement, and motivation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.