
Abstract
Introduction
Health systems globally face challenges, including geographical barriers, and inadequate health workers. Telemedicine has turned up as a potential solution to bridge these gaps, relying on technology to enhance healthcare accessibility and improve the quality of health services. A relatively unexplored area in Ghana, the adoption of telemedicine in healthcare delivery has great potential to address health inequalities in the country. We explored the implementation of telemedicine using the Hub and Spokes model.
Methodology
A qualitative case study was conducted among 15 health professionals working at the telemedicine unit in the Hohoe Municipality. Face-to-face in-depth interviews were used in collecting data, which were analyzed thematically using Atlas.ti.
Results
Telemedicine has significantly improved healthcare accessibility by bridging geographical gaps and improving service delivery. The hub has effectively supported the spokes leading to improved patient satisfaction, reduced mortality, and stillbirth rates. However, challenges such as communication barriers (network issues, one-way communication), and logistical constraints (lack of transportation systems, telephones, and funds to buy airtime for calls) militated against effective delivery of services. Despite these challenges, telemedicine holds significant opportunities for improving healthcare delivery by ensuring timely referrals, bridging knowledge gap between practitioners, and enhancing overall service quality and efficiency.
Discussion
Integrating telemedicine into routine patient care in the Hohoe Municipality has proven beneficial in addressing healthcare inequalities. Telemedicine has enhanced the quality of healthcare and increased accessibility for remote areas by applying HSM. This highlights telemedicine as an important strategy towards achieving universal health coverage (SDG 3.8) by 2030.
Keywords
Background
Telemedicine (TM) is a quickly evolving technology used by global healthcare systems to provide health services through electronic information. TM delivers healthcare services over distance, which offers an opportunity to improve clinical management and expand service coverage, especially in remote areas. 1 TM is now more practical due to technological improvements and increased accessibility to information technology. 2 The field of healthcare has witnessed a transformative phenomenon with the introduction of TM, a technology-driven approach that holds the promise of overcoming geographical barriers and enhancing healthcare accessibility. 3 Remaining true to its roots in the Greek word “tele,” referring to distance, 4 TM focuses on the delivery of healthcare services by healthcare professionals providing services from a distance using information and communication technologies for the exchange of valid and correct information. 5
Accessibility to healthcare remains a global challenge; half (50%) of the population is unable to access primary healthcare services, with 800 million people spending over 10% of their budget on healthcare services. 6 In Sub-Saharan Africa (SSA), healthcare access is very low, approximately 42.6% of people have access to healthcare care which has increased the mortality and morbidity rate of diseases. 7
In Ghana, 1.9% of rural communities have access to a private or public hospital, leaving a majority of the population without access to healthcare. 8 Many factors contribute to this challenge, but the most common one is geographical barriers. 9
TM was first introduced in 2011 and integrated in 2016 into the healthcare system to address the challenges of health inequalities and improve the quality of health services 10 and serve as a cornerstone of achieving universal healthcare by bridging the gaps in the Ghanaians’ healthcare system, such as inadequate health professionals, financial constraints, geographical barriers, and inadequate health facilities. The idea of TM is not new but has been evolving for a long time and aims to reduce health inequities, enhance the health status of people living in remote areas through shorter patient travel times, reduce healthcare costs, and provide access to doctors and specialists.3,11,12
According to the Hub and Spokes model (HSM), basic services are supplied at secondary locations while essential resources are centralized at a single location where specialized services may be offered. 13 The model's layout produces a healthcare network with a better-resourced main site that serves outlying sites and offers essential basic services. A lot of TM systems are implemented as a HSM, with hospitals serving as the hub and other facilities like assisted living facilities serving as the spokes. 14 HSM is more likely to be advantageous in low- and middle-income countries where diseases are becoming more prevalent as a result of urbanization and changing demography. Since poor infrastructure is a major issue in these areas, the spokes can benefit from the knowledge and highly skilled labor of the rich in resource hubs to deliver improved services. 13
As a developing country, Ghana typically lacks the infrastructure and adequate labor which significantly reduces the cost of providing high-quality healthcare, particularly in remote areas.
15
To address these healthcare gaps, TM has emerged as a strategic framework for extending specialized services to remote and underserved areas by the application of HSM
Materials and methods
Our study adopted the consolidated criteria for reporting qualitative research (COREQ).
Settings
Our study was conducted in 15 health facilities, one regional hospital (Hub), a hospital, eight health centers, and five Community-based Health Planning and Services (CHPS) compounds serving as the spokes in the Hohoe Municipality. The Volta Regional Hospital (VRH) serving as a hub, was formerly known as Hohoe Municipal Hospital, is a secondary facility that serves a population of about 114,472, of which males constitute 47.9% and the remaining females. 16 The Hospital started on April 5, 1935 and was officially inaugurated by the late Dr Kwame Nkrumah on December 21, 1952. Currently, it has a staff strength of over 316 with a bed capacity of 178 and serves as the referral point for very ill patients from other clinics and hospitals within and outside the Municipality. The geographical location of Hohoe Municipality and the various facilities in the HSM are shown in Figure 1.
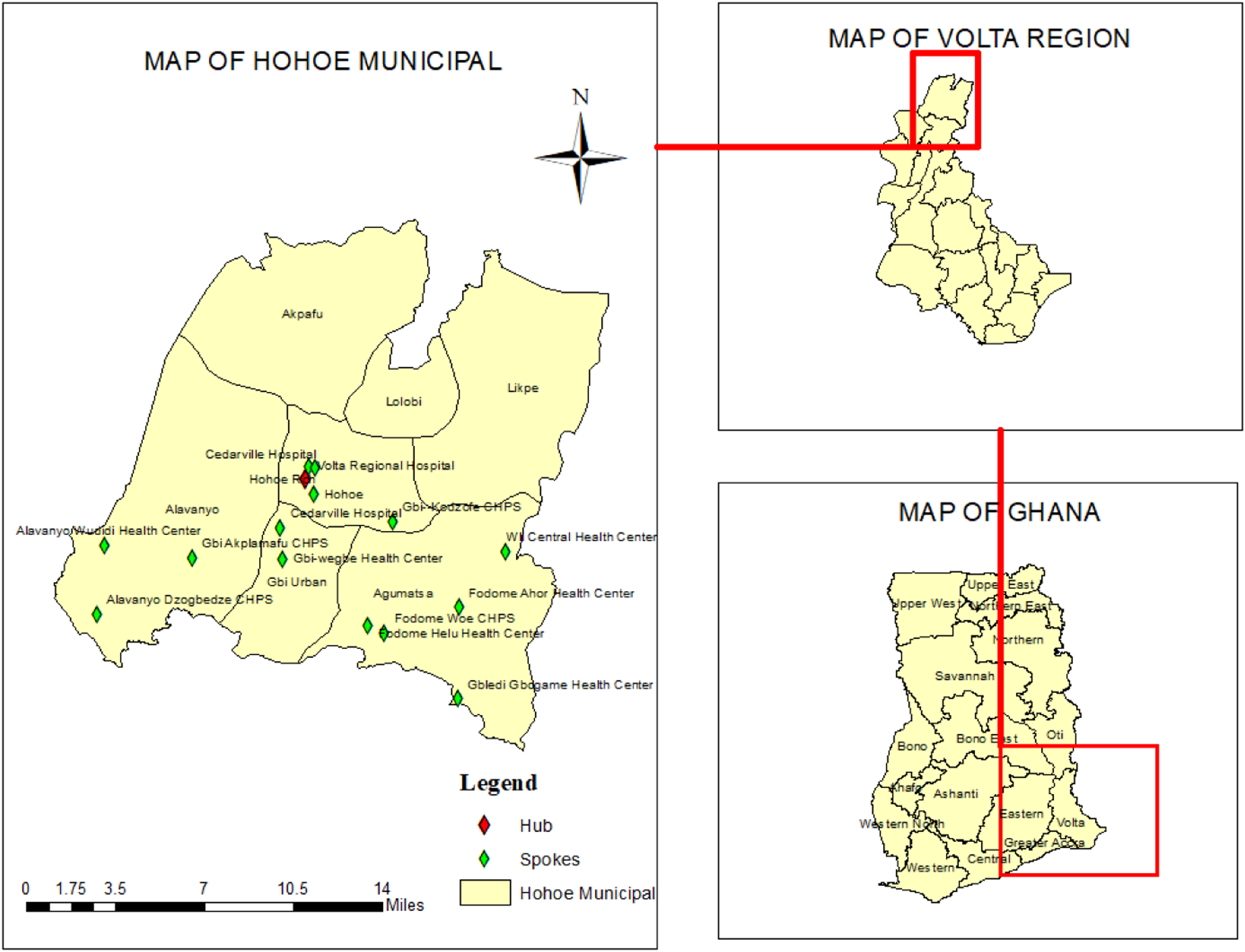
Map of Hohoe Municipality.
Study design
Our study employed an exploratory qualitative design to explore the implementation of TM, focusing on its contribution, challenges, and potential benefits. Qualitative exploratory design helped in gaining an in-depth understanding 17 of healthcare personnel's experiences on the contribution of the Teleconsultation Centre (TCC) in extending healthcare to remote areas, challenges, and opportunities for sustainable integration of TM.
Theoretical issues
HSM is frequently used in the healthcare system to address issues by providing specialized treatments to rural or remote areas. The concept of HSM has no single originator; instead, it has been adopted by several groups and legislators. The healthcare system has also adopted and modified it to find effective ways to deliver complete and easily accessible healthcare. HSM was pioneered in the airport industry in 1952, but it was introduced in 1920 by Dr Bertrand Dawson of the Royal Army Medical Corps in the field of medicine. 18 HSM is a design strategy that organizes service delivery into a network. It has a central hub, which is a primary facility offering a complete range of services, connected to several smaller spokes, which are secondary locations providing more limited and routine services. Most TM systems are implemented in this model, with hospitals serving as the hub and other assisted facilities serving as the spokes. 18 HSM has been applied to link weak peripheral settings to a hub with abundant resources, thereby enriching such settings. 13 The model allows people in rural areas to access advanced therapies while receiving primary care locally, thereby reducing geographical barriers and addressing health inequalities. It also improves coordination and communication between various healthcare delivery levels and encourages effective provider collaboration and referral systems. The approach has been used in TM, remote patient care, and disease management initiatives, among other healthcare contexts.
In Hohoe Municipality, the model connects 14 healthcare facilities at lower levels (spokes) to the main central unit (TCC-Volta Regional Hospital, Hohoe), which serves as the Hub. VRH is equipped with the necessary resources: specialists, well-trained nurses, midwives, and doctors. Through HSM, services are rendered via TM to support the spokes. Health professionals at lower-level facilities contact the TCC by phone to receive guidance and support in managing cases beyond their capacity. The VRH (Hub) ensures that adequate and necessary services are provided to any of the spokes that call in through the TM platform. It also serves as a referral system and prevents unnecessary referrals. Patients receive services such as obstetric care, management of minute acute conditions, and other medical consultations through the platform. This model not only provides service to patients but also enhances the skills of the health personnel at the spokes. As shown in Figure 2, the conceptual framework illustrates the HSM in the Hohoe Municipality.
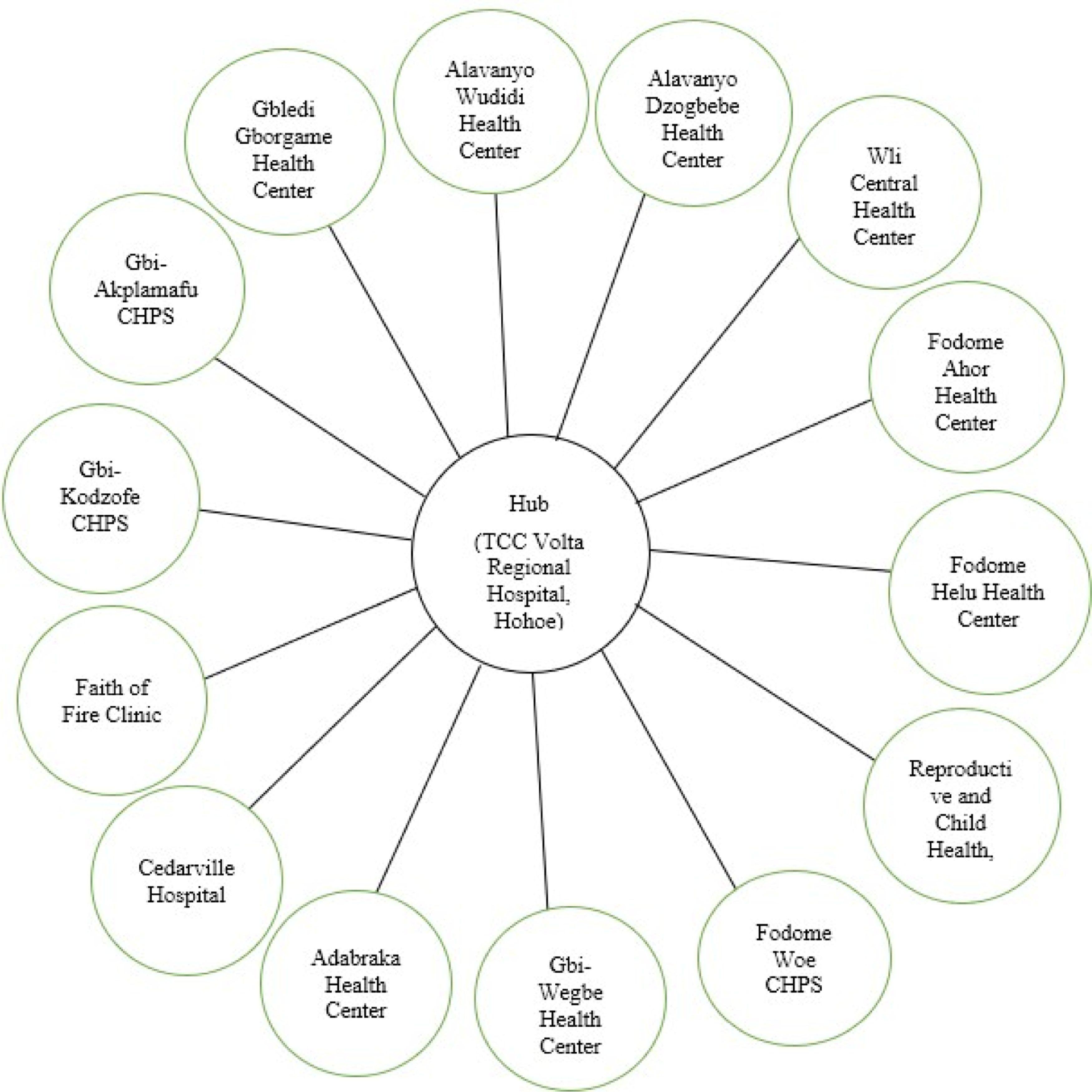
Hub-and-Spokes model of telemedicine in the Hohoe Municipality.
Study population
To obtain expert views on the implementation of TM, our study was conducted among healthcare professionals within Hohoe Municipality who were actively involved in running TM. This includes nurses, physician assistants, and midwives.
Sampling and sample size
Purposive sampling, incorporating maximum variation sampling, was employed. This ensures that health professionals of different cadres (nurse, midwife, physician assistant) and qualifications (degree, diploma) were recruited. The sample size was determined by selecting a health professional from each of the facilities: 14 from the spokes and 1 from the hub, resulting in a sampling of 15 health professionals. None of the participants dropped out of the study.
Data collection procedure and instrument
In-depth interviews were used to collect data from health professionals through face-to-face interactions at the health facilities. Data collection was conducted in 2024, approximately 3 years after the inception of TCC in October 2021 in the Hohoe Municipality. The interviews were conducted by BSL, who was a Master of Public Health student and a registered nurse at the time of data collection, with an experienced research team member under the supervision of the team leader (HA). Data collection occurred during working days at each of the health facilities. Interviews were conducted at a distance where privacy was ensured and all interviews were conducted in English. Each interview lasted for about 20 minutes and there were no repeat interviews.
Handwritten notes (with pens and notebooks) and audio recorders were used to record the interviews. To ensure that interviews don’t end if any equipment malfunctions during the procedure, both handwritten notes and audio recordings were used. An interview guide served as an instrument for interviewing participants (see Appendix 1). The instrument was structured into three sections; Section A focused on the socio-demographics of the participants (e.g. sex, age, marital status, religion, educational level, and years of working at TCC). Section B contained information on the contribution of the TCC in extending healthcare services to remote areas; and Section C contained information on the challenges and opportunities for sustainable integration of TM in the healthcare system. Participants were probed for further explanation whenever necessary. The instrument was pre-tested among 2 health professionals.
Trustworthiness
According to Ref., 19 trustworthiness entails credibility, transferability, dependability, and confirmability.
Credibility in this study centers on establishing the truth value of the findings. Health professionals working at various levels of the healthcare system in the Hohoe Municipality provided insights that aligned with themes, such as the contribution of TM in extending healthcare and opportunities for sustainable integration, which were presented cohesively without the need for location-based comparisons. Our study also ensured credibility by maintaining transparency in data collection and analysis. Audios were systematically transcribed, and a reflective analysis was conducted. Direct participant quotations were consistently used to illustrate key themes and to ensure authenticity. This process helped reinforce the credibility of the thematic findings by ensuring that they accurately reflect participants’ perspectives on TM and its challenges in the Hohoe Municipality.
Transferability is a thick description. This includes not only a description of the experiences and behaviors of study participants but also provides a detailed account of the study's context. This ensures that the experiences and behaviors become meaningful to an outsider. 19 In our study, transferability was ensured by describing the study setting, the sample size and sampling procedure used, and the socio-demographics of the study participants. Transferability was also ensured in the study by providing the thematic table and sample of the interview guides used in collecting data from the participants.
Dependability and confirmability focus on the audit trail. 19 The audit trail is about transparency in the description of the research processes from the beginning of a study to the development and reporting of the results. In this study, the audit trail was ensured by documenting the entire research process from the background to the conclusion section. Regarding analyses, the thematic table has been provided. The interpretations of the data were derived from the data collected and were not based on the researcher's own preferences and viewpoints.
Confirmability was ensured by engaging five (5) participants to review their transcripts and our preliminary findings. This process ensures the accuracy of the researchers’ interpretations and confirms the themes from the participants’ view.
Data analysis
Recordings from the interviews were transcribed and compiled in Microsoft Word files. To reduce errors, interview transcripts were verified with interview notes and proofread while listening to the audio recordings. To address the issues of subjectivity in the analysis, two of our research team members analyzed the data. Data was analyzed using reflective thematic analysis. 20 Thus, transcription was read and re-read to ensure familiarization with data and to take note of key ideas and recurrent themes. ATLAS.ti. v7.5 was used in developing the themes and codes, which are both analytic emergent in nature. Sentences, phrases, and words that were relevant were coded. Similar codes were combined into sub-themes and themes as data analysis progressed. The themes and sub-themes were conveyed in a manner that precisely reflects the participants’ actual experiences. Quotes from participants were used in presenting the findings to provide evidence on the issues discussed by the participants. A frequency table was used to present the socio-demographic characteristics of the study participants.
The researchers held regular meetings to review and validate the accuracy of the emerging themes and their interpretations. A theme was only finalized once the research team reached a consensus. To enhance the credibility of the analysis, member checking was conducted. The identified themes: the contribution of TM, challenges and potential benefits of extending TM were shared with five (5) participants via email for feedback. All five participants confirmed that the findings accurately represented their perspectives as conveyed during the interviews.
Ethical issues
Ethical approval was obtained from the University of Health and Allied Sciences (UHAS) Research Ethics Committee (REC) UHAS REC (A.4 [031]23-24. Permission was sought from the Volta Regional Hospital, Hohoe Municipal Directorate, and the respondent's consent was obtained. The content or subject matter of our study was disclosed and explained to participants. Their consent was obtained before the commencement of the study. Unique codes were assigned to participant data and were stored in an encrypted computer accessible only to the lead investigator. Data collected from this study was used for the purpose for which it was taken. The data was processed anonymously by replacing names with identification numbers to which no personal information about the participants was connected. Respondents were free to opt out of the study at any time during the data-gathering procedure without any implications. The study was conducted in accordance with the ethical principles outlined in the Helsinki Declaration.
Results
Socio-demographic characteristics of health professionals
Table 1 presents the background characteristics of health practitioners. 60% were between 25 and 34 years. The majority were females (73.3%), nurses (46.7%) and more than half (60%) had diploma qualifications. Most of them had worked in the health system for about 1 to 9 years and 86.7% had worked at the TCC center for almost 3 years.
Socio-demographics of health professionals.

Thematic findings
Table 2 presents the themes from our analysis. The main themes were the contribution of the TCC, challenges of the TCC, addressing the challenges of TCC, and opportunities for integrating TCC in healthcare.
Thematic findings.

Contribution of Teleconsultation Center in extending healthcare to remote area
From the perspective of the health profession, TM has contributed significantly to the health system in Hohoe Municipal. In our analysis, five sub-themes emerged. These were types of services, accessibility to healthcare, quality of service, patient satisfaction, and improvement in service delivery, which have enhanced healthcare delivery by increasing accessibility and ensuring equitable care for remote communities.
Regarding the type of service, the health professional mentioned that TM provides a wide range of services including case management, pediatric services, referrals, and guidance (consulting specialist). They mentioned that TM is used for referral and management of cases such as minor illnesses and emergency cases, thereby reducing the number of referrals to the higher facility. For case management through TCC, they seek guidance from specialists to help them manage or solve cases at their facilities without any casualties. They emphasized that TM plays a critical role in referrals for cases that exceed the facility's capabilities. The following quotes summarize their responses, “so, I think basically we do more of a referral due to some issues at the lower facilities, but the concept is to be able to build the capacity for staff at the lower level to be able to handle cases that they will need little assistance to do so” (Nurse, Male, 32 years). Oh OK. You know we do minor, we treat minor illnesses and then sometimes we get maybe advice from staff or the doctors from the hospital. We also manage emergency cases and then we also refer cases that are beyond maybe our capability” (Nurse, Female, 28 years). “The services that the teleconsultation provides, they provide mental health services, Pediatrics any services that involve health Yeah, they mostly provide those services to us when we call they provide all those services to us” (Nurse, Male, 36 years).
For accessibility, health professionals expressed that there is an increase in accessibility to healthcare services. They emphasized that TM has now made healthcare available at the health center and patients can access any healthcare service, whether by referral or management. Through TCC, geographical location is no longer a barrier to accessing healthcare. They explained that they only have to contact the TCC, and they can provide services to the patient without the patient traveling long distances to receive healthcare. “Sometimes not even necessarily referrals of the clients, but by the time they (doctors) are done guiding you. The client doesn't even need the referral anymore” (Midwife, Female, 38 years).
Concerning patient satisfaction, they have observed that patients are highly satisfied with telemedicine services. They said, patients appreciate the quality of care they receive through the TCC, particularly the process, where patients are directed straight to the care they need without unnecessary delays, they noted that patients feel more confident and assured, knowing that their details are already communicated and they will receive timely and accurate treatment, leading to a high level of satisfaction. Some nurses had this to say, “Our clients always come back with that happy moment that when they get there, immediately they start working for us in this area. So it's something that is improving our work, and clients are satisfied with the referral” (Nurse, Male, 36 years) OK, Zero to ten, I'll give it nine because you know, one thing that the patients are very happy about this TCC when we are explaining to them, is the fact that they don't have to go and wait when they come, they know where they are going and they know that they are not now going to be asking them what is your name? What is your address and things like. So for that particular one, they are really ok about it (Nurse, Female, 28 years)
With the quality of service, according to the practitioner, the quality of service provided through TCC is described as high and accurate. TCC enables them to access specialist advice and guidance, which enhances their ability to deliver precise and effective care. To them, telemedicine improved the management of complex cases, and overall higher standards of healthcare delivery. “Is of high quality because it helps us, sometimes getting a car from here to Hohoe is very difficult, so we do call them if there is a need that they will get us an ambulance, the Teleconsultations unit provides the ambulance for us” (Midwife, Female, 34 years).
For improvement in service delivery, the health profession stated that telemedicine has significantly improved service delivery by enhancing referrals, reducing mortality and stillbirth, patient response to treatment, and mostly improving case management. They reported that case management and referrals have improved. Most of them emphasized that through the use of telemedicine, the Hub is prepared adequately to receive the client upon arrival which saves time and ensures quality service is rendered. Some of them had this to say, “Ohh yeah, there is an improvement … now that there is the teleconsultation unit, when you call, before the client will get there everything is set they (doctors) will just start taking care of the clients, which is of great help to us. so because of that, there is nothing like maternal death or stillbirth” (Midwife, Female, 34 years). “let's say, in where I stay right now, not every case really needs to come to the main hospital so with the introduction of this teleconsultation you would just call them and then maybe they will speak with the … And at the end of the day, you end up treating them at our facility so that they don't have to come to the Regional Hospital” (Nurse, Female, 28 years).
Challenges of implementing a Teleconsultation Center in healthcare delivery
We found that several challenges were identified, and it was categorized into two sub-themes these were communication challenges and logistical challenges.
Logistical challenges emerged as one of the main challenges faced by health professionals. The stress on the lack of a telephone is leading to dependence on personal phones, lack of funds to buy airtime, and lack of a transport system. They reported that these challenges affect the services they render. Here are some quotes from the health profession on logistical challenges, “OK, so one of the challenges that we have faced is that right here, I have an emergency, and I call the tele center and I said, oh, I have a case, they say, OK, bring the case right here, but now how the client will move it's a problem, so there is transportation gap” (Physician Assistant, Male, 32 years). “And also, you know we are calling we are using credit and then who is providing that credit. And I think we don't have like a specific telephone for calls we use our own personal phone.” (Nurse, Female, 28 years).
With regards to the communication challenges, they highlighted network issues that disrupt communication between the staff, poor feedback from the center, and one way of communication, which poses a significant threat to service delivery. Most of them reported that TM in the Hohoe Municipality is mostly via phone calls and they need a stable network to render these kinds of services, but network issues have become a barrier for them. A female nurse had this to say, “So, the first one would have to be, you know, sometimes when you are calling the call doesn't go through but even that we have like about three lines or four of them. But sometimes when you are speaking to them, they're like we can’t hear very well, so I think that is one of the challenges” (Nurse, Female, 28 years
Addressing the challenges of Teleconsultation Centre
From the study, two sub-themes emerged to address the challenges of TCC. These were management roles and government roles. There is a need to address the challenges before it is too late, most of them, find a way to overcome and solve the challenges but it is not enough. They suggested that some of these challenges can be addressed by the government, and some are within the management's ability to provide.
Regarding the government's role, they play an important role in addressing the challenges. For the health staff, since telemedicine can help in achieving universal healthcare, the government has a responsibility to play in ensuring that telemedicine functions properly. The Government should provide ambulances to curb the transportation gap and extend TCC to remote areas. The following quotes summarize their response, “As for the challenge when it comes, some are just beyond our control as staff. You can't do much about it because it's the government that is supposed to do it. So like the bus like this, the government should provide an ambulance” (Midwife, Female, 38 years). “TCC is really working, it's helping us to save lives. So it has to be implemented they said health for all, they (government) want everyone to have access to healthcare … so they (government) should provide the necessary funding, support with resources so that it can be implemented and then you can make use of” (Nurse, Female, 28 years).
Concerning management's role in addressing the challenges, the health professionals emphasize that management has a responsibility to play. They suggested management should ensure funds are available for airtime, and provide logistics, especially telephones for calls. Some of them had this to say, “I think provision of the telephone and airtime if it can be monthly. There are some monthly subscriptions they can do with the network providers to give us an airtime” (midwife, Female, 27 years). “The only platform to be able to communicate with the telecenter is via a phone call. But if there could be a means of like, you could also type, leave messages, scan certain documents, and send them across” (Physician Assistant, male, 32 years).
Opportunities for integrating telemedicine into the healthcare system
From the perspective of practitioners in the Hohoe Municipality, TM is an intervention that has been beneficial to the healthcare system, especially for health centers and CHPS compounds. Its main purpose is to improve the quality of service and make health services available and accessible to all.
In the aspect of the potential benefit of integrating TCC several benefits emerged. TM holds the promise of improving healthcare from their perspective. Some potential benefits of integrating TCC into the health system reported by the health professionals were: telemedicine will ensure timely referrals, reduce the burden on higher facilities, bridging knowledge gap between practitioners and improve the quality of services. They emphasized that with telemedicine integration, quality service can be assured and geographical gaps that hinder healthcare accessibility will be addressed. This may reduce mortality. For instance, they had this to say regarding the opportunities, “If we are able to manage cases through TCC at our level, not all the cases will be reaching there (regional hospital). That will make more work out there so it's something important that needs to be integrated into service” (Nurse, Male, 36 years). “We those at the hard-to-reach areas if it were not to be TCC maybe Hohoe would have recorded so many maternal cases or maternal death cases or other conditions that may lead the clinic to something else” (Midwife, Female, 34 years). “It makes working efficient and less stressful … and makes access to healthcare very easy, yes, because when we get the intervention (consulting specialist), they still have to be with us and then we give them the management here” (Midwife, Female, 27 years).
Discussion
This was a qualitative study that explored the implementation of TM in the Hohoe Municipality using the Hub-and-Spokes model. Our findings revealed that TM has significantly enhanced healthcare accessibility, improved patient satisfaction, and strengthened the quality of service delivery, particularly in remote areas. Key contributions included improved case management, timely referrals, and cost savings for patients. However, challenges such as communication barriers (network issues, one-way communication) and logistical constraints (lack of transport, telephones, and airtime) were reported. Health professionals also identified several opportunities for integrating TM into the health system, including ensuring timely referrals, reducing the risk of further complications, and increasing accessibility.
Our study found that TM has made significant contributions to health service delivery, particularly in the areas of accessibility, service improvement, service type, and the assurance of quality care within the healthcare system. In terms of accessibility, our study revealed that healthcare services are now consistently available to people regardless of their geographical location. This improvement in healthcare accessibility aligns with,21–23 which demonstrates how TM enables access for patients who might otherwise lack safe treatment options, meeting their unique needs for discretion, convenience, and scheduling. In Ghana, this accessibility is crucial, as it reduces the burden on secondary healthcare facilities by ensuring that people receive necessary care regardless of their location. Similarly, our finding was consistent with a systematic study in SSA, which reported that TM improves access to high-quality healthcare. 24
Our findings in relation to the type of services provided were that TM is primarily used for seeking guidance and referrals, which is consistent with, 25 who highlighted the role of TM in enhancing peer-to-peer support and education among healthcare workers, as well as reducing hospital congestion. The study also indicated that the quality of service has improved since the inception of telemedicine, a finding that aligns with, 15 who reported that telemedicine has been implemented in rural areas of Ghana to address the shortage of medical professionals and improve access to healthcare services. Lastly, the study found that patients are highly satisfied with TM services, a finding that confirms the results of, 26 who reported positive patient experiences with TM in Ghana. In a nationally representative sample, the quality of patient experiences was closely associated with high satisfaction levels, further validating the effectiveness of TM in enhancing healthcare delivery.
Our findings regarding the contribution of TCC to the healthcare system align with the conceptual framework, which focuses on the Hub supporting spokes to render healthcare service to remote areas. 13 This also corroborates a study that reported high levels of satisfaction and increased accessibility and increased service utilization. 27 This implies that TCC can enhance healthcare access and improve the quality of service in remote areas of Ghana which will reduce the number of deaths and stillbirths and will contribute to better health outcomes and reduced disparities in healthcare access. These findings were due to the extension of TM into remote facilities.
Our study also identified communication and logistical challenges as the main challenges that pose a threat to TM services. We found that network issues, one-way communication, as a challenge that slows the delivery of service. This finding is consistent with, 28 which found that network challenges were another critical hurdle for TM adoption. Connectivity and network issues can significantly impact the quality and reliability of TM services. Poor network connectivity has hindered the expansion of successful pilot projects to cover the entire city of Kumasi and surrounding villages. 15 Similarly, a study reported that poor network was a major challenge hindering the use of TM. 29
With regards to logistical challenges, lack of transportation system, telephone and funds for airtime were found as the main challenges. These findings align with several studies; for instance, studies have highlighted that the lack of reliable transportation can undermine the benefits of TM by limiting patients’ ability to access necessary in-person follow-up care or diagnostic services, even after initial remote consultations.21,23 The lack of adequate infrastructure for TM deployment is a major challenge in Ghana. 25 These challenges affect the effectiveness of TM in timely and reliable healthcare delivery. They also have the potential to limit healthcare accessibility and increase the burden on higher facilities.
Our study also found that ensuring timely referrals, bridging the knowledge gap between practitioners, reducing the burden on higher-level facilities, improving quality of service, efficiency, and less stress, reducing the risk of further complications, and increasing accessibility were the potential benefits of integrating telemedicine into the healthcare system. TM offers numerous potential benefits in healthcare delivery, particularly in improving access and quality of care. Our findings align with multiple studies that have revealed that TM can ensure timely referrals, enhance service quality, increase efficiency, and reduce stress for both patients and providers.30–32 One of the key advantages of TM is its ability to improve access to specialty care, especially in rural and remote areas. Again, connecting patients with specialists remotely, telemedicine can reduce travel time, costs, and the need for unnecessary referrals.22,33
The extension of telemedicine into Ghana's healthcare system presents significant opportunities, despite facing several challenges. A study revealed that health professionals in Ghana are ready to adopt TM, with a statistically significant relationship between health facilities’ core readiness, engagement readiness, staff knowledge, attitude readiness, and health professionals’ readiness 34 TM offers a promising solution to address the shortage of medical professionals in rural areas of Ghana, which is primarily caused by low student intake in medical schools and the emigration of graduates. 15
These findings hold the promise of achieving SDG goal 3.8, which focuses on achieving universal health coverage, including financial risk protection, access to quality essential healthcare services, and access to safe, effective, quality, and affordable essential medicines and vaccines for all.
Limitations
The study relied on self-reported interviews, which could lead to a possibility of response bias, where participants may have provided desirable answers rather than accurate accounts.
A significant challenge encountered was the reluctance of some healthcare staff to engage in the study, which reduced the diversity.
There is also potential for selection bias. The participants were purposively selected, thus health professionals directly involved in the TCC, which may not fully represent the perspectives of all healthcare workers in the municipality. This selection approach was intentional, as the study aimed to capture the experiences of those most engaged with the intervention. However, it limits the generalizability of findings. Future studies should include a broader range of stakeholders, including patients and providers outside the TCC, to reduce selection bias and strengthen the transferability of findings.
Our study also did not collect quantitative data on the number of patients who received care through the TCC. As such, while we were able to capture health professionals’ perspectives on the range of services supported (e.g. case management, pediatrics, mental health, and referrals), we could not provide estimates of patient utilization of the platform.
Conclusion
The integration of telemedicine in the Hohoe Municipality has proven beneficial in addressing healthcare inequalities. TCC has improved the quality of healthcare and increased accessibility for healthcare services in remote areas with the application of the HSM. TCC has not only bridged the accessibility gap in urban and remote areas but also has the potential to enhance the quality of healthcare services by bridging the knowledge gap between practitioners if it is extended to various parts of the country with the application of HSM. This integration serves as an important way toward achieving healthcare equity and ensuring that all people have access to the healthcare they need, regardless of their location. The findings highlight telemedicine as a strategy for achieving universal health coverage (SDG 3.8) and improving health outcomes.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251390927 - Supplemental material for Implementation of telemedicine in the Hohoe Municipality, Ghana: A qualitative study using the Hub and Spokes approach
Supplemental material, sj-docx-1-dhj-10.1177_20552076251390927 for Implementation of telemedicine in the Hohoe Municipality, Ghana: A qualitative study using the Hub and Spokes approach by Joshua Oppong, Bridget Setornyo Letsa, Gifty Botwey, Felix Mbiba, Selasi Amu and Hubert Amu in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251390927 - Supplemental material for Implementation of telemedicine in the Hohoe Municipality, Ghana: A qualitative study using the Hub and Spokes approach
Supplemental material, sj-docx-2-dhj-10.1177_20552076251390927 for Implementation of telemedicine in the Hohoe Municipality, Ghana: A qualitative study using the Hub and Spokes approach by Joshua Oppong, Bridget Setornyo Letsa, Gifty Botwey, Felix Mbiba, Selasi Amu and Hubert Amu in DIGITAL HEALTH
Footnotes
Ethical considerations
Ethical approval was obtained from the University of Health and Allied Sciences (UHAS) Research Ethics Committee (REC) UHAS REC (A.4 [031]23-24. Permission was sought from the Volta Regional Hospital and Hohoe Municipal Directorate. Data collected from this study were used for the purpose for which they were taken. The data was processed anonymously by replacing names with identification numbers to which no personal information about the participants was connected. Respondents were free to opt out of the study at any time during the data-gathering procedure without any implications. The study was conducted in accordance with the ethical principles outlined in the Helsinki Declaration.
Consent to participate
Written and oral consent was obtained from the participant. The content or subject matter of our study was disclosed and explained to participants. Their consent was obtained by signing the consent form or verbally agreeing before the commencement of the study.
Consent for publication
Not applicable.
Author contributions
All the authors conceived the study. BSL and JO collected the data. JO and FM analyzed the data. JO and GB drafted the initial manuscript. HA and SA supervised and reviewed the manuscript, which improved the quality of the manuscript. All authors reviewed the final manuscript and approved it for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All relevant data are within the manuscript. Any further requests regarding the data used for this study could be made through the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.