
Abstract
Introduction
This study investigates specific behavioural and social factors influencing the adoption of mobile health (mHealth) technologies by Community Health Workers (CHWs) in rural Indonesia. Using the SMARThealth cardiovascular risk management programme in Malang as a case study, the study examines how constructs from the Technology Acceptance Model (TAM) and related frameworks explain CHWs’ intention to use and actual use of mHealth tools.
Methods
A cross-sectional survey was conducted with 573 CHWs participating in the SMARThealth programme. Data was collected using a structured questionnaire and analyzed using Partial Least Squares Structural Equation Modelling to test ten hypotheses derived from TAM and Unified Theory of Acceptance and Use of Technology.
Results
Five of the ten hypotheses were supported. Behavioural intention significantly predicted actual use of the SMARThealth app (β = 0.277, p < .001). Behavioural intention was positively associated with perceived usefulness (β = 0.513, p < .001), perceived ease of use (β = 0.372, p < .001), social relationships (β = 0.051, p = .037) and non-financial incentives (β = 0.071, p = .016). Other factors including financial incentives, government support, community support, IT training and motivation were not statistically significant.
Conclusion
Perceived usefulness, ease of use, social relationships and non-financial incentives significantly influence CHWs’ intention to adopt mHealth tools in Malang, Indonesia. These findings highlight the need for user-friendly design and peer-based, non-monetary support strategies. However, due to contextual differences in CHW roles, infrastructure and community dynamics, these results may not be generalisable. Further research is needed to assess their relevance across other low- and middle-income countries settings.
Introduction
Community Health Workers (CHWs) serve as a vital bridge between health systems and the communities they support, enhancing access to and coverage of essential health services.1–3 Substantial evidence highlights the effectiveness of CHWs in delivering preventive, promotive and curative care across various health domains, including the management of cardiovascular disease (CVD) risk.1–3 However, CHWs often encounter significant challenges in service delivery, such as limited access to updated knowledge, inadequate training resources, insufficient supervisory support and difficulties in tracking follow-up visits – particularly in rural areas where CVD risk is high.3–5
With the rapid growth in smartphone ownership and mobile applications, mobile health (mHealth) interventions are increasingly being leveraged to support CHWs by improving access to information, enhancing task planning and offering clinical decision-support tools.6,7 In low- and middle-income countries (LMICs), mHealth tools are now employed across twelve key functional areas, including behaviour change communication, diagnostics, data reporting and provider training.8–11 These digital solutions are designed to strengthen CHWs’ performance and overall service delivery. 11
Despite their promise, the adoption of mHealth technologies remains inconsistent. To explore the behavioural dimensions of this adoption, the present study is guided by the Technology Acceptance Model (TAM). Technology Acceptance Model posits that two main factors – perceived usefulness (the belief that a technology will improve job performance) and perceived ease of use (the belief that it requires minimal effort) – are central to predicting behavioural intention, which in turn determines actual system use.12–14 Technologies perceived as both valuable and user-friendly are more likely to be adopted. These constructs have consistently demonstrated strong predictive power in previous technology acceptance research and form a key foundation for understanding CHW engagement with mHealth solutions.
To extend this framework and better account for contextual influences, the study also incorporates the Unified Theory of Acceptance and Use of Technology (UTAUT), which builds on TAM by introducing four additional constructs: performance expectancy, effort expectancy, social influence and facilitating conditions.12,15,16 These factors reflect not only how CHWs perceive a technology's functionality and ease of use but also the impact of peer and supervisory support, availability of training and access to resources and infrastructure. This dual-theoretical approach enables a more comprehensive understanding of both individual-level and environmental factors shaping mHealth adoption.
Although TAM and UTAUT have been widely applied in high-income settings, their applicability among CHWs in resource-limited environments has been less explored. Furthermore, much of the existing literature has prioritised technical and infrastructural barriers, with limited attention paid to behavioural and social determinants – such as peer relationships, community support and the influence of financial or non-financial incentives.17–19 Addressing these gaps is crucial for understanding the real-world integration of mHealth into CHWs’ daily practices.
To contribute to this understanding, the study investigates the behavioural and social determinants influencing CHWs’ adoption of mHealth technologies for CVD risk management. Grounded in the TAM framework, it examines how perceived usefulness, ease of use and behavioural intention are shaped by individual, social and contextual dynamics. Specific focus is given to the roles of social relationships, incentives, training and institutional support. The research is guided by three key questions: (1) To what extent do CHWs in rural settings adopt mHealth technologies for CVD risk management? (2) What individual and contextual factors facilitate or impede this adoption? (3) How do social relationships and support systems influence CHWs’ behavioural intentions to adopt mHealth? While the primary aim is to identify behavioural barriers, the findings also highlight the enablers that underpin successful mHealth adoption in community health settings.
Method
Study settings
This study was conducted in Malang District, East Java Province, where, since 2020, the health authority has been scaling up a digital health-enabled primary care intervention for CVD risk management, known as SMARThealth. 20 By August 2023, the programme had been implemented in 248 villages, involving approximately 500 CHWs, locally referred to as kaders. The SMARThealth application enables kaders at Posbindu (Pos Pembinaan Terpadu) to assess CVD risk using basic equipment and a clinical decision support tool accessed via a tablet device.20,21 Posbindu is a community-based programme focused on the early detection and monitoring of risk factors for non-communicable diseases such as heart disease, diabetes and hypertension. 22 Figure 1 illustrates the SMARThealth platform.

SMARThealth platform.
The application allows kaders to collect essential health information, inform individuals of their risk status, offer lifestyle advice and refer high-risk individuals for consultation with nurses or physicians. A shared electronic record system enables both synchronous and asynchronous entry and retrieval of patient data, which is securely transmitted to a central server. Nurses and physicians also use a mobile application to receive decision support regarding the appropriate prescription of preventive medications, drawing on data collected by kaders as well as information gathered during consultations. Treatment plans are made immediately available to kaders, ensuring continuity of care and community-based follow-up. The system is supported by community-wide health promotion, training, performance management, activity-based remuneration of health workers and access to essential medications. This study focuses specifically on the adoption of digital health tools by kaders within this programme.
Hypothesis
Building on the TAM and UTAUT, this study hypothesises that CHWs’ behavioural intention to use the SMARThealth app is positively associated with their actual use of the app (H1). Consistent with TAM, we propose that two key factors – perceived ease of use and perceived usefulness – are significant predictors of behavioural intention. Accordingly, CHWs who find the SMARThealth app easy to use (H2) and useful in performing their tasks (H3) are more likely to intend to use it.
To extend the model and better reflect the realities of CHWs in rural Indonesia, we incorporate additional contextual factors. We hypothesise that technological support, such as IT training or technical assistance, enhances CHWs’ confidence and positively influences their intention to use the app (H4). We also propose that financial incentives (H5) and non-financial incentives – such as certificates, uniforms or community recognition (H6) – serve as motivational drivers for adoption.
Furthermore, we posit that CHWs’ intrinsic motivation, reflecting their commitment to improving community health, is positively associated with their intention to use SMARThealth (H7). In terms of social factors, we hypothesise that strong social relationships, including peer encouragement and support from supervisors, increase CHWs’ likelihood of adopting the app (H8). We also suggest that government support, in the form of resources, policy frameworks and training programmes, positively affects behavioural intention (H9). Finally, community support, such as local involvement in Posbindu activities or logistical support, is expected to reinforce CHWs’ intention to use the SMARThealth app (H10). Table 1 provides a summary of the hypotheses tested in this study.
Summary of study hypotheses on CHWs’ adoption of the SMARThealth app.

Study design
This study was a community-based cross-sectional study in which the data was collected by means of interviews. No sampling was involved, as all eligible kaders were invited to participate. The data was collected from January to March 2023.
Data collection
The questionnaire was designed on KoboToolbox, and the link was sent to 574 eligible kaders. For individuals who have difficulty using the KoboToolbox app, data collection was conducted by trained field researchers. Among 574 kaders, 70 of them were assisted by field researchers to complete the online questionnaire. One incomplete response was eliminated.
Questionnaire design
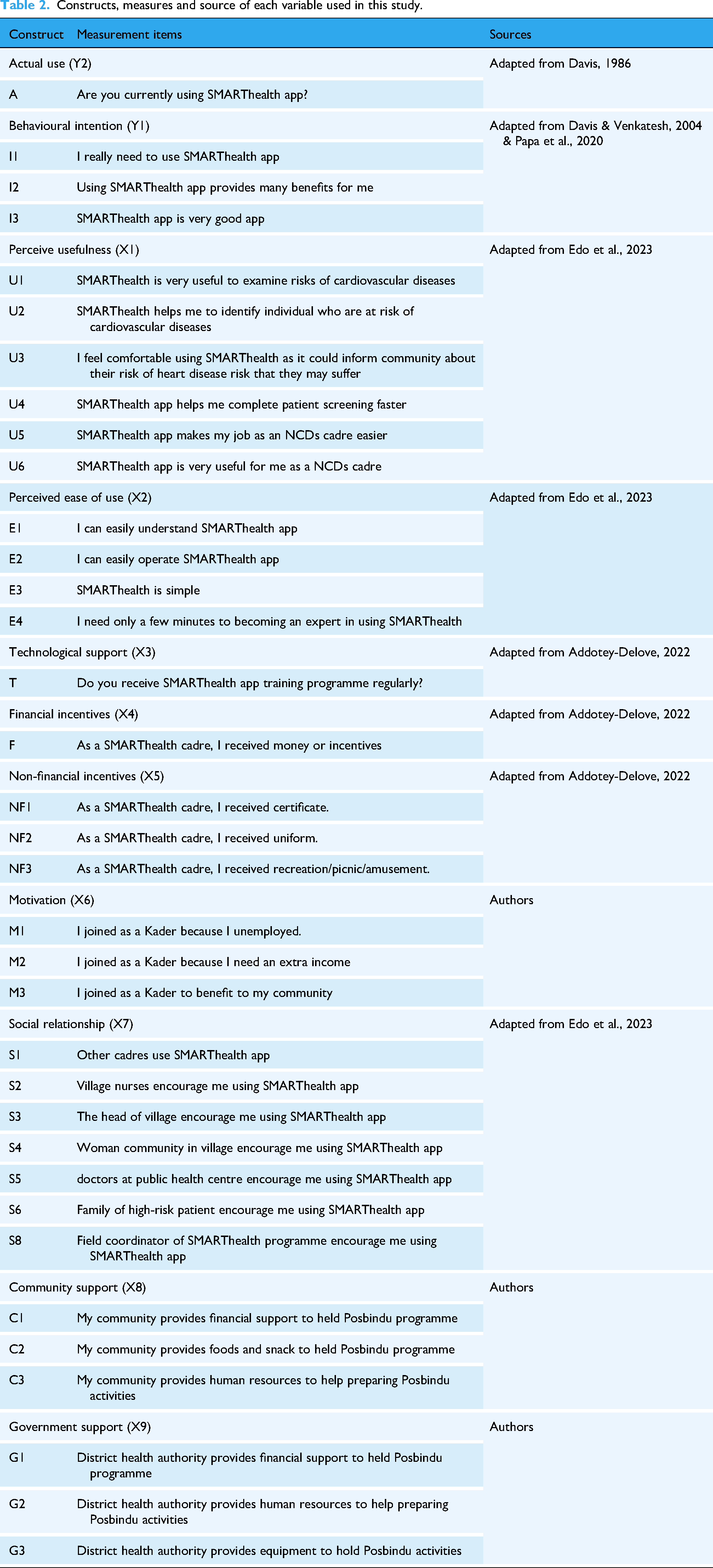
A series of questions adapted from previously validated studies was used in this research, with minor modifications to enhance relevance for kaders in rural Malang. These adaptations ensured cultural and contextual appropriateness, and the questions were pre-tested with 30 kaders to minimise ambiguity. One construct – perceived availability – was self-developed based on contextual needs. The selection of facilitating factors and constructs was guided by established theoretical models and empirical evidence. We primarily drew on TAM and UTAUT, both widely applied in health and non-health technology adoption research. To contextualise these frameworks for CHWs in rural Indonesia, we incorporated constructs identified in mHealth studies from LMICs.23–26 In addition to core TAM constructs – perceived usefulness and perceived ease of use – we included factors such as technological support, financial and non-financial incentives, motivation, government support and social relationships. These reflect broader enablers and social dynamics affecting CHW engagement. Their inclusion was further informed by qualitative insights and implementation experiences from the SMARThealth programme in Indonesia,2,27 which underscored their relevance. The final constructs and items were selected to capture both individual-level perceptions and structural conditions influencing mHealth adoption in resource-limited, community-based primary care contexts. A summary of these constructs, their operational definitions and references is provided in Table 2. The questionnaire comprised 15 sections, including demographic information and modules aligned with the study constructs (Supplementary File 6).
Constructs, measures and source of each variable used in this study.
Validity and reliability of the questionnaire
To confirm the validity and reliability of the questionnaire, a pre-test was conducted using a questionnaire with 11 variables, distributed to 30 healthcare workers. The Cronbach alpha was used to assess the validity and reliability of the variables. The internal consistency coefficient of Cronbach's alpha (CA) ranged from 0.723 to 0.893, which fall within the minimum acceptable threshold for a study of this nature.28,29 This suggests that the results were reliable and had consistency above the norm.
Partial least square structural equation modelling
Partial least square structural equation modelling (PLS-SEM) was used to analyse the model as it offers an optimum method for analysing a complicated path model with various types of indicators either binary or continuous. 29 The analysis followed three steps: assessing common method bias, evaluating the measurement model and analysing the structural model. Common method bias was examined using collinearity diagnostics, where the variance inflation factor (VIF) was required to be below 3.3. 30 The measurement model was then assessed for reliability and validity. Reliability was evaluated using CA and composite reliability (CR), with greater emphasis on CR values above 0.7. 31 Convergent validity was tested through item loadings (≥0.6) and average variance extracted (AVE ≥ 0.5).28,29 Discriminant validity was established using the heterotrait–monotrait (HTMT) ratio (<0.85), Fornell–Larcker criterion and cross-loadings. 32 The structural model was assessed through bootstrapping with 5000 resamples to estimate path coefficients and test hypotheses. Model quality was further evaluated using effect size (f²), explained variance (R²) and predictive relevance (Q²). Predictive performance was additionally tested using PLS prediction, comparing root mean square error (RMSE) and mean absolute error (MAE) values from PLS-SEM against a linear benchmark model.28,29
Results
Common method bias
The major issue in the survey samples is common method variance bias. In PLS-SEM using Smart-PLS, a collinearity assessment test using VIF value was used to assess whether the common method variance bias existed in the constructs. 30 The accepted value of VIF is below 3.3. According to the result, the VIF value for each variable was lower than 3.3 ranging from 1 to 2.04, which means that the variables don’t have any indication of strong method bias (Supplementary File 4).
Measurement model evaluation
Measurement model evaluation is aimed to evaluate the reliability and validity of the 11 variables as can be seen from Figure 2. To evaluate the reliability of the measurements, CA and CR score were evaluated. The value of CA and CR, which is larger than 0.7, is considered reliable. Some of CA scores were lower than 0.7, however CR scores for each variable were higher than 0.7 ranging from 0.76 to 1.0 (Supplementary File 1). Since CR is generally acknowledged as more useful than Cronbach alpha and more robust in SEM estimation, and all of CR's scores were high, therefore we can conclude that all of the measurements were reliable although some of the CA scores were lower than 0.7. 31

Structural Equation Modelling (SEM) results.
Validity test was measured using several measurements. First, factor loadings score with at least 0.6 was used to evaluate the item's validity. 29 Second, the AVE would assess convergent validity. The measurement items can explain the measured construct or variable if the AVE value is higher than 0.5. Items included in the model have scores higher than 0.6, while the items with factor loadings lower than 0.6 were deleted in the estimation model (Supplementary File 1). After the deletion, all of the AVE scores are higher than 0.5, indicating that all of the variables have internal consistencies.
Finally, discriminant validity was also assessed to measure whether the items really measured their own construct and can be distinguished from items for different constructs. The evaluation used three measurements (HTMT, Fornell–Larcker criterion and cross loading). The result showed that all of HTMT values were less than 0.85,32,33 indicating that discriminant validity is proved, while each score of the right side of diagonal table of Fornell–Larcker criterion was higher than the correlation score between latent variables, proving that each item predicted latent constructs and could be distinguished from indicators in other constructs (Supplementary File 2). Cross-loadings for each item were also examined to assess discriminant validity. The findings revealed that each measured item has the highest score compared to the score from different construct (see bold numbers), which indicated that every item reflected their construct and has no strong correlation with the different constructs (Supplementary File 3).
Structural model for hypothesis testing
The second stage of SEM was structural assessment including hypotheses testing and goodness-of-fit analysis through evaluating the effect size (f2), R2 and Q2 displayed in Supplementary File 4. The f2 value was lower to medium with perceived ease of use (f2 = 0.221) and perceived usefulness (f2 = 0.442) having the largest effect on behavioural intention. Those values indicated the model's fitness. In addition, the R2 value for endogenous construct was 0.077 for actual use and 0.695 for behavioural intention, meaning that behavioural intentions only contributed 7% to predict actual use behaviour, while all measured independent variables accounted for 69.5% of the variation of behavioural intention which is deemed highly fit. The Q2 value also supported the fitness of the model as the values were higher than 0.
Finally, PLS prediction as can be seen in Supplementary File 5 can also be used to calculate the predictive relevance of the model. 29 The model has strong predictive power when the values of PLS-SEM RMSE and PLS-SEM MAE are lower compared to the value of LM_RMSE and LM_MAE as well as Q2 were higher than zero. Supplementary File 5 explained that all of the values in PLS-SEM RMSE and PLS-SEM MAE were lower than LM-RMSE and LM_MAE, while all of the Q2 predictions were higher than 0, indicating that the model has a strong predictive power.
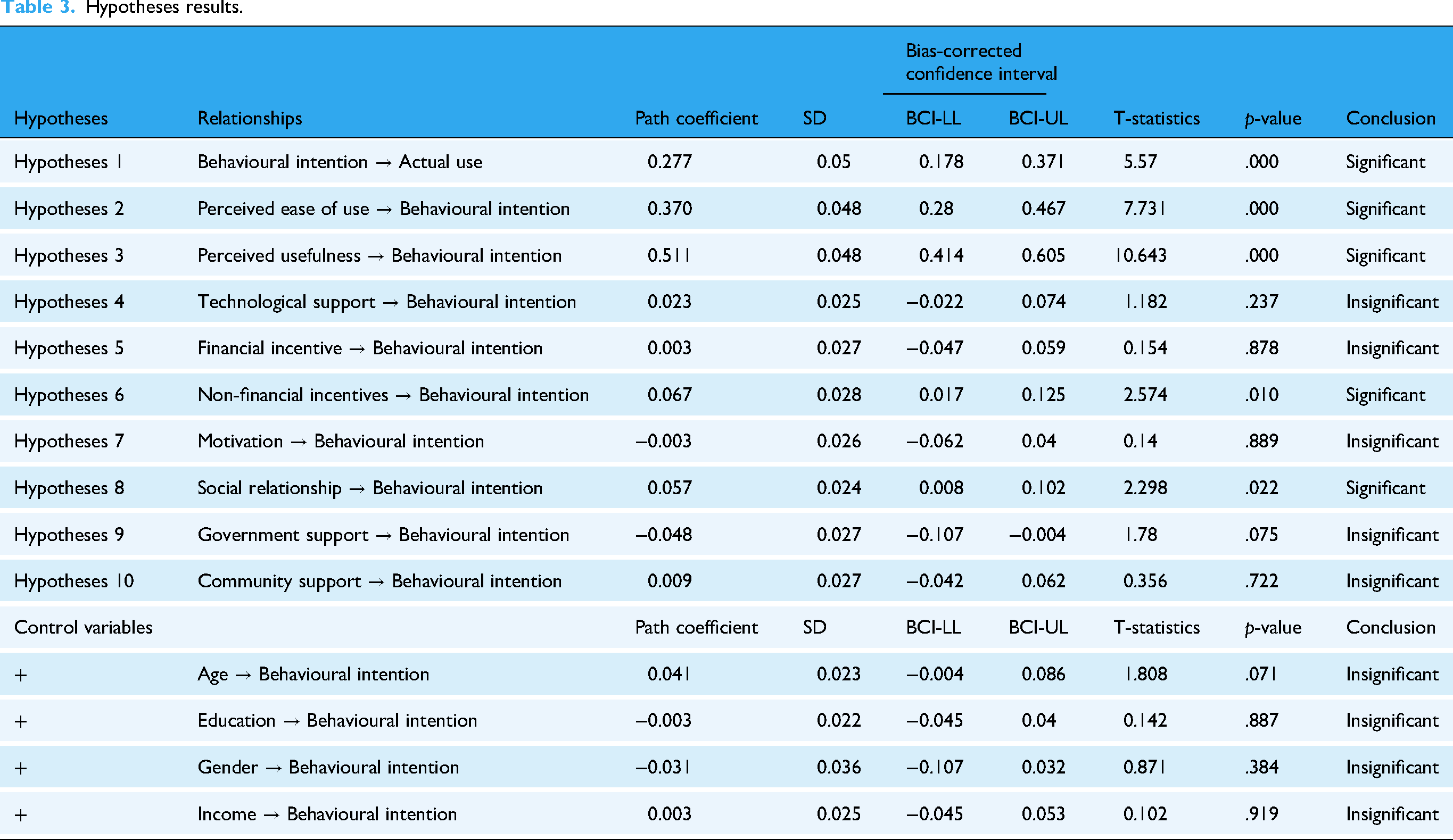
In Table 3, the result of hypothesis testing through bootstrap analysis with 5000 samples was presented. The hypotheses proved significantly were five out of ten hypotheses. First, actual use was proved to be associated with behavioural intention. The higher the intention to use SMARThealth, the higher the probability of actually using the app (β = 0.277). Secondly, behavioural intention was determined by social relationship from community or villagers , non-financial incentives , perceived ease of use and perceived usefulness . If cadres had good social relationships with various stakeholders (β = 0.051) and got higher non-financial incentives (β = 0.071), such as transportation fee, uniform or recreation/amusement reward, the intention to use the SMARThealth app would increase. Also, the cadres would have a higher intention to use the app when they perceived that the app was easy to be used (β = 0.372) and was useful (β = 0.513).
Hypotheses results.
Discussion
This study examined factors influencing mHealth adoption among CHWs in rural Indonesia, drawing on TAM and UTAUT. Of ten hypotheses tested, five were confirmed. Behavioural intention significantly predicted actual mHealth use and was itself shaped by perceived usefulness, ease of use, social relationships and non-financial incentives.
The strong link between intention and actual use supports the Theory of Planned Behaviour, 34 echoed in LMIC settings such as Malawi and Ethiopia,35,36 where CHWs’ intent reliably predicts technology adoption. Perceived usefulness emerged as a key factor – CHWs were more likely to adopt tools they believed improved their efficiency and benefited their communities. This aligns with findings from Pakistan and Afghanistan, highlighting the importance of clearly demonstrating value to end-users. 37
Perceived ease of use also influenced intention. Community Health Workers favoured tools that were simple, intuitive and minimally demanding. This reinforces evidence from Uganda and Ethiopia on the role of user-centred design in driving adoption.36,38 Simplifying interfaces and minimising technical barriers can significantly boost engagement.
Social relationships played a critical role. Support from peers, supervisors and communities strengthened CHWs’ intention to adopt mHealth tools, in line with social influence theory.39,40 Positive peer experiences and supervisory encouragement created a culture of acceptance and collective efficacy, while social networks facilitated knowledge exchange and confidence-building.9,40,41
Non-financial incentives – such as recognition, appreciation and professional development – were also significant. These rewards tap into intrinsic motivations and are often more sustainable and context-sensitive than financial incentives.42,43 Tanzanian studies support this, showing that public recognition and skill-building opportunities can enhance CHW morale and engagement. 44
Interestingly, technological skills, financial incentives, motivation to serve and support from government or communities were not significantly associated with mHealth adoption. The lack of impact from financial incentives is notable, especially given the poverty faced by many CHWs.45–47 One might expect financial rewards to matter more; however, they may be seen as inadequate, inconsistent or secondary to practical concerns such as usability and relevance.3,17,18,23,48 This highlights the need to understand the socioeconomic realities of CHWs – often underpaid or volunteering – when designing incentive structures.
Similarly, CHWs’ own digital proficiency had limited influence, likely because tools were simple and perceived benefits outweighed skill concerns. Structural support from governments or communities was also not impactful, possibly due to poor visibility, inconsistent implementation or weak alignment with CHWs’ day-to-day needs.9,10,18
Contribution
This study makes a significant contribution to the discourse on digital healthcare technology adoption among CHWs in the management of CVDs at the primary care level, particularly within the context of developing countries such as Indonesia. While much of the existing research on digital health adoption focuses on developed nations, studies situated in LMICs often overlook critical contextual variables.23,49,50 This study addresses this gap in three key ways.
First, it extends the existing body of literature by investigating digital health adoption in a developing country context – specifically Indonesia – where empirical research remains limited. Second, it adapts and refines established models by applying frameworks developed in high-income settings to the Indonesian context, incorporating context-specific factors such as social relationships, which have been underexplored in previous studies. Third, it identifies critical success factors by rigorously examining 11 variables derived from established models such as TAM and UTAUT, offering insights into the key drivers of digital health adoption among CHWs engaged in CVDs management within Indonesia's primary healthcare system.
Overall, this research offers valuable guidance to stakeholders in the healthcare sector – including policymakers, programme implementers and health institutions – on designing and delivering effective digital health interventions tailored to the needs of CHWs in primary care settings in LMICs.
Practical implications
The results of this study provide insights into factors associated with digital health technology adoption among CHWs for hypertension management. Enablers associated with adoption decision were identified (especially social relationship and non-financial incentives) from which it could be understood that rural CHWs are driven by a sense of collective efficacy and shared responsibility and social networks that serve as valuable platforms for knowledge sharing, problem-solving and peer support, mitigating potential anxieties and enhancing confidence in using new technologies. Surprisingly, technological skill, financial incentive, motivation, government and community support are not associated to CHW intention to use digital health app. Evidence from this study reveals underscores the importance of focusing on designing user-friendly and intuitive digital health tools that are tailored to the specific needs and contexts of CHWs, rather than solely relying on their existing technological skills.
Limitations
This study, while offering valuable insights, suffers from several limitations that warrant careful consideration. First, the findings are limited to the perceptions of CHWs within public health facilities in rural Indonesia. Given potential differences in work practices and organisational culture between rural and urban contexts, as well as across regions, the generalisability of the generalisability of these results may be limited. Comparative analyses involving urban and other geographic settings are needed to assess the robustness of these associations. Second, the cross-sectional design precludes causal inference, limiting interpretation of observed relationships to correlations. Longitudinal approaches, such as panel studies, would help elucidate the causal mechanisms underpinning TAM and UTAUT. Third, reliance on self-reported data introduces potential bias, particularly in relation to CHWs’ reported use of the SMARThealth app. Although anonymity and confidentiality were ensured to mitigate social desirability bias, misreporting remains possible. Collinearity diagnostics confirmed that common method bias was not present (VIF < 3.3), yet future studies should consider triangulating survey data with objective usage metrics (e.g., app log data) or qualitative methods to enhance validity. Finally, while this study is among the first in Indonesia to integrate social factors into mHealth adoption research, it may not capture the full range of behavioural influences. Future research should incorporate additional contextual and psychological variables to provide a more comprehensive understanding of mHealth adoption among CHWs.
Conclusion
This study applied the TAM and UTAUT frameworks to examine CHWs’ adoption of digital health technology in rural Indonesia. The findings show that CHWs have adopted the SMARThealth app to a meaningful extent, with behavioural intention strongly predicting actual use, indicating that when tools are perceived as useful and easy to use, they are integrated into daily CVD risk management practices. The study highlights the pivotal role of social relationships and support systems, where encouragement from peers, supervisors and community members enhanced CHWs’ intention to use the app. Together with the influence of non-financial incentives, these results emphasise that beyond individual perceptions, collective and contextual factors are critical drivers of adoption. For policymakers and programme implementers, the implication is that user-friendly design, peer support and recognition-based incentives should be prioritised to ensure sustainable and scalable mHealth implementation in similar LMIC settings.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251390314 - Supplemental material for Exploring community health worker acceptance of mobile health for cardiovascular risk management in rural Indonesian communities
Supplemental material, sj-docx-1-dhj-10.1177_20552076251390314 for Exploring community health worker acceptance of mobile health for cardiovascular risk management in rural Indonesian communities by Sujarwoto Sujarwoto, Tri Yumarni, Rindi Ardika Melsalasa Saputri, Holipah Holipah and Asri Maharani in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251390314 - Supplemental material for Exploring community health worker acceptance of mobile health for cardiovascular risk management in rural Indonesian communities
Supplemental material, sj-docx-2-dhj-10.1177_20552076251390314 for Exploring community health worker acceptance of mobile health for cardiovascular risk management in rural Indonesian communities by Sujarwoto Sujarwoto, Tri Yumarni, Rindi Ardika Melsalasa Saputri, Holipah Holipah and Asri Maharani in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to thank the communities and their CHWs for their kind cooperation and for facilitating the development of this study.
Ethical clearance and informed consent
The study protocol was reviewed and approved by the Ethical Committee of the Ministry of Research, Technology, and Higher Education, Universitas Brawijaya (Ref: 235/EC/KEPK/09/2020). All procedures were conducted in accordance with the ethical principles of the Declaration of Helsinki and relevant national regulations. Written informed consent was obtained from all participants before data collection. Consent was documented through the statement: “I am aware that my responses are confidential, and I agree to participate in this survey”, and only participants providing affirmative agreement were enrolled. Participation was voluntary, and individuals were free to decline or withdraw at any stage without consequences or the need to provide a reason.
Contributorship
SS conceptualised the study, designed the methodology, analyzed the data, drafted the manuscript and reviewed and edited the manuscript. RS contributed to the study design, assisted with data collection and reviewed and edited the manuscript. TY & HH contributed to the study design, provided critical review and feedback on the manuscript. AM contributed to the study design, supervised the research project and provided guidance on the study design and analysis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Department of Public Administration Universitas Brawijaya Funding Scheme.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Disclaimer
As part of the SMARThealth programme implementation in Malang District, the lead author (SS) served as the Co-Principal Investigator (Co-PI), collaborating with the Malang district health authority. In this role, the lead author had access to the SMARThealth digital platform. All necessary permissions to use the SMARThealth app for research purposes were obtained as part of the programme's governance and research framework. The use of the app and its associated data for this study complies with institutional and programme-level ethical standards.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.