
Abstract
Background
This study aimed to evaluate the influence of artificial intelligence (AI)-generated Digital Smile Design (DSD) on patients and clinician satisfaction, and overall aesthetic outcomes.
Methods
A comprehensive search of PubMed, Scopus, Cochrane Library, ScienceDirect, and Google Scholar was conducted to identify studies (2004–2024) evaluating AI-based DSD. Eligible studies reported patient/clinician satisfaction or facial esthetic outcomes. Data were extracted on study characteristics, participant demographics, DSD type, and outcome measures. A meta-analysis of satisfaction prevalence was performed using Jamovi with a random-effects model. Methodological quality was assessed using the ROBINS-I tool, and publication bias was evaluated via rank correlation, fail-safe N, and regression tests for funnel plot asymmetry.
Results
Seven studies were included after screening 387 records. AI-based tools (e.g. SmileCloud, REBEL, and Invisalign SmileView) improved esthetic outcomes, enhancing smile symmetry, lip arcs, and incisal edge visibility. Key predictors of success included philtrum height and buccal corridor. The meta-analysis showed a pooled satisfaction prevalence of 58% (95% CI: 0.30–0.86, p < 0.01), with high heterogeneity (I² = 60.23%). Studies had a moderate risk of bias, and publication bias was detected (regression test, p < 0.01).
Conclusion
These findings suggest that AI-generated DSD provides significant facial esthetic outcomes. However, future studies should explore the long-term sustainability of these outcomes and the cost-effectiveness of AI-based dental treatments.
Keywords
Introduction
Facial aesthetics, especially smiles, play an important role in expressing first impressions, social interaction, and self-esteem. 1 Achieving optimal facial aesthetics has become one of the main goals of modern dentistry, particularly in cosmetic and restorative dentistry. 2 Therefore, an increasing number of patients are seeking dental treatment, which not only restores function, but also improves the appearance of patients’ smiles. 3 Various elements, such as tooth shape, alignment, size, color, and symmetry, must be carefully considered alongside soft tissue components, including the lips and gingiva, to achieve an aesthetically pleasing outcome.4,5 Smile design concepts have evolved significantly over the past two decades. Initially, basic tools, such as pencils and markers, were used to create hand-drawn and hand-painted patient drawings. This method has gradually changed to digital photography of electronic images owing to the rapid advancement of information technology, in which computers and the Internet play a central role in nearly every aspect of our lives. In dentistry, cutting-edge software is used to design and enhance smiles, significantly transforming the field of aesthetic dentistry.6,7 Subsequently, progress has been made in manipulating three-dimensional (3D) files generated by intraoral scanners. In recent years, four-dimensional (4D) technology has been introduced into the smile design process, allowing the capture of a patient's dynamic smile motions through digital sensors. 8
Smile design using digital technology, such as the Digital Smile Design (DSD) technique, is a technological tool used to digitally modify the smile of the patient, which is helpful in the selection and visualization of the proposed changes in advance. 9 It creates and presents a digital mock-up of the new and changed smile design, enabling patients to see the expected results before physical treatment begins. 9 This technique enhances visual communication and actively engages patients in the smile design process, resulting in more predictable treatment outcomes and higher acceptance rates. 10 They also offer a wide range of solutions and predictions for smile design, allowing for the precise identification of minor adjustments. 6 Traditionally, DSD has been guided by the expertise of dental professionals who rely on their knowledge of facial anatomy, dental biomechanics, and aesthetic principles to craft an ideal smile for each patient. 11 As the utilization of DSD programs has increased in clinical settings, numerous innovations have been introduced to enhance accessibility and practicality. One key advancement is the integration of artificial intelligence (AI) into software. 12
AI can potentially revolutionize smile design by analyzing large amounts of data and creating highly personalized treatment strategies. AI algorithms can process facial images, perform proportion analyses, and provide advice according to established aesthetic principles.13,14 Additionally, AI can streamline the smile design process by recommending ideal treatments. 15 This not only improves the efficiency of dentists but also minimizes the potential for errors. Furthermore, AI algorithms can estimate the durability of various treatment options for patients, assisting dentists in selecting the most long-lasting and cost-efficient solutions. 16 A key advantage of the AI-powered solution is its ability to create accurate smile ratios using uploaded patient smile photos, which enables the quick and accurate assessment of preliminary images of the facial mucosa. 17 However, the comparative effectiveness of AI-generated versus human-designed smiles remains underexplored, particularly regarding patient and clinician satisfaction and long-term esthetic outcomes.
As AI technologies become increasingly integrated into dentistry, understanding their efficacy compared with human expertise in designing optimal smiles is essential. AI-driven smile designs offer advantages such as precision, time efficiency, and data-driven decision-making, whereas dental professionals bring their clinical experience and artistic sensibility to the design process. This study provides a comprehensive comparison of esthetic outcomes and patient satisfaction. This evaluation will help clarify whether AI-based designs meet or exceed the quality of human-generated outcomes, thereby influencing future clinical practice. Additionally, the analysis may identify potential limitations and areas for improvement in AI algorithms, contributing to the enhanced integration of AI in aesthetic dentistry for optimal patient outcomes.
This study aims to systematically evaluate the impact of AI-based DSD on patient and clinician satisfaction and facial esthetic outcomes, addressing a knowledge gap in the efficacy of AI-driven tools compared to conventional methods. By synthesizing evidence from recent studies, this review seeks to inform clinical practice and guide future research in AI-enhanced aesthetic dentistry.
Methodology
This systematic review adhered to the guidelines of Preferred Reporting for Systematic Reviews and Meta-Analysis (PRISMA) for better transparency of the literature, and a clear and reproducible process presents a clear and rigorous understanding of each step followed until the final selection of studies.
18
This study was registered with the
Search strategy
An advanced literature search was performed using different electronic databases, including PubMed, The Cochrane Library, Scopus, ScienceDirect and Google Scholar, using different keywords such as “aesthetic dentistry” OR “esthetic dentistry” OR “facial aesthetic” OR “facial esthetic” AND “digital smile” OR “digital dentistry” OR “digital smile design” AND “artificial intelligence” OR “AI” OR “machine learning” (see Supplemental Table 1). Studies published between 2004 and 2024 in English were considered.
Eligibility criteria
Inclusion criteria, based on the PIO framework, were:
Population: Human subjects undergoing facial esthetic treatments. Intervention: AI-based DSD (e.g. SmileCloud, REBEL, and Invisalign SmileView). Outcomes: Patient/clinician satisfaction (measured via surveys or questionnaires), facial esthetic outcomes (e.g. smile symmetry, lip arcs, incisal edge visibility, philtrum height, and buccal corridor), or treatment planning accuracy. Study designs: Randomized controlled trials (RCTs), non-RCTs, and case studies (included due to limited RCTs in AI-based DSD research).
Exclusion criteria included:
Studies on animals, lacking specific esthetic outcome measures (e.g. smile symmetry and satisfaction scores), or published before 2004. Reviews, editorials, commentaries, or non-English studies.
Article selection process and assessment
Two independent reviewers (KK and RB) were responsible for the selection of each article. First, the titles and abstracts of each article were screened in accordance with our aim. After the initial screening, full-text articles were screened, and articles were selected after meeting the inclusion criteria. A third reviewer (AK) was also engaged in case of any disagreement, and issues were resolved through detailed discussions and evaluation of the eligibility criteria. Case studies were included in the meta-analysis to maximize data inclusion, given the emerging nature of AI-based DSD research, but their limitations (e.g. small sample sizes and potential selection bias) were noted in quality assessments.
Data extraction
A predefined data extraction form was utilized for the collection and extraction of information.
Study characteristics (author ID, country, study design, and sample size). Participant demographics (age, gender, treatment purpose, and comorbidities). Type of DSD-specific AI-based tool (e.g. SmileCloud and REBEL). Outcome measures Satisfaction scales (e.g. Likert scales and questionnaires), esthetic evaluation methods (e.g. smile parameters and clinician assessments). Outcomes: (patient satisfaction (for meta-analysis), facial esthetic outcomes (e.g. improved symmetry, lip arcs, and conclusion).
Quality assessment
Methodological quality assessment was performed by using the risk of bias (RoB) for non-randomized studies interventions (ROBINS-I), and seven domains, like confounding, participant selection, intervention, deviation, outcome data missing, measurement of the outcomes, and reporting outcomes were utilized for the quality assessment. 19
Statistical analysis
The extracted data were transferred to an Excel spreadsheet for the organization and construction of tables and graphs. For the meta-analysis, Jamovi software was utilized. The effect size was measured using a 95% confidence interval (CI). Cochran's Q test and I2 were used to analyze the heterogeneity among the studies, and a significant difference was considered when p < 0.01. Heterogeneity was assessed as low, medium, or high when I2 was 25%, 25%–50% and >50%, respectively. Additionally, publication bias was calculated using rank correlation, file-drawing analysis, and a regression test for funnel plot asymmetry.
Results
Literature searched
Initially, 387 research papers were identified from different electronic databases, including ScienceDirect, PubMed, Scopus, The Cochrane Library, and Google Scholar. After identification, 47 duplicate research papers were removed before starting the title and abstract screening. Subsequently, 340 research papers were evaluated for their eligibility, and the criteria set for the selection of studies were strictly followed. After the screening process, 330 research papers were found that were not based on our aim of the study and were thus excluded. After screening, only 10 research papers were eligible for full-text assessment. Three research papers were excluded for the different reasons listed in Figure 1. Finally, seven studies were included in the present study.
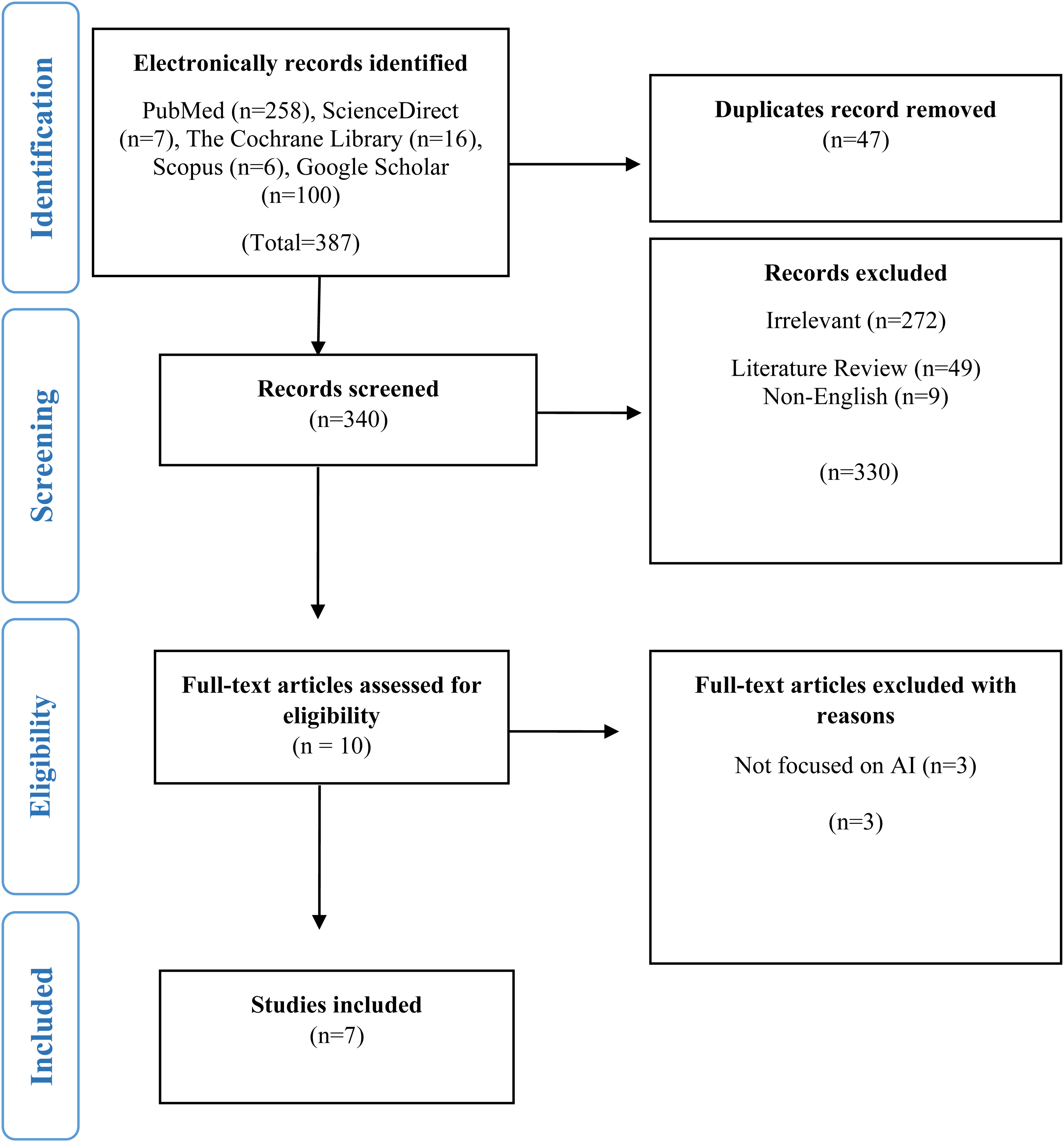
Preferred Reporting for Systematic Reviews and Meta-Analysis (PRISMA) flowchart for the selection of studies.
General characteristics
Table 1 summarizes the general characteristics of the participants in the studies. The studies spanned different countries, and most of the studies were reported from Yemen,20–22 while the remaining studies were reported from Brazil, Türkiye, Egypt, and Romania.11,23–25 Similarly, in terms of study design, most studies were case studies,20–22,24 cross-sectional,11,25 and prospective studies. 23 The sample sizes varied from individual case studies20–22,24 to a larger sample size of 628. 11 participants’ ages ranged from 18 to 73 years.24,25 The gender distribution varied across studies, including males and females, while others involved only one gender, with treatments primarily focused on esthetic improvements20–22,25 and malocclusion correction with clear aligner therapy. 23 Most participants were healthy, with only one study reporting no chronic diseases. 23
General characteristics summary of the studies and participants.

NA: not available; M: male; F: female.
Outcomes
These studies utilized a range of AI-based techniques, including 3D digital designs, 24 REBEL,20–22 and smile simulation tools, such as Invisalign SmileView and SmileCloud,23,25 for esthetic evaluation. The key smile parameters assessed included the smile lines, lip arcs, incisal edge visibility, and facial symmetry (Table 2). These studies generally reported improved esthetic outcomes, with some noting the acceptance and preference of clinicians and patients for AI-generated smile designs. 11 Additionally, specific smile parameters, such as philtrum height and buccal corridor, were reliable predictors of successful simulation. These studies concluded that AI-driven smile designs offer time-saving advantages, predictability, and personalized facial esthetic outcomes in dental practice (Table 2).
Summary of outcomes.

3D: three dimensional; CBCT: cone bean computed tomography; CAD-CAM: computer-aided design-computer-aided manufacturing.
Meta-analysis
The pooled prevalence of satisfaction among patients/dentists from the six studies was 58%, and the 95% CI ranged from 0.30 to 0.86, suggesting that the true proportion lies within this range (Figure 2). High heterogeneity (I2 = 60.23%) was observed among studies, with a statistically significant difference (p < 0.01). However, the wide confidence interval and high heterogeneity suggest variability in study designs, populations, or AI tools, necessitating cautious interpretation. Subgroup analysis was not feasible due to the limited number of studies and variable outcome measures, but future research should explore this to address heterogeneity.

Forest plot for the prevalence of patient and dentist satisfaction with artificial intelligence (AI)-based smile designs.
Publication bias
The fail-safe N value of 96 suggests that 96 additional studies with null results are required to nullify the observed effect, indicating that the findings were robust. Statistical significance was set at p < 0.01, indicating high statistical significance. The rank correlation test for funnel plot asymmetry yielded Kendall's tau of 0.11 (p-value = 0.78), suggesting no significant asymmetry. However, the regression test for funnel plot asymmetry produced a Z-value of 4.014 (p < 0.01), indicating a potential publication bias (Table 3).
Summary of outcomes for publication bias.

Quality assessment
Most studies were found to have a moderate risk of bias,11,20–22,24 while two studies had a low risk of bias.23,25 The main risk of bias was observed in the participant selection domains (Figure 3).

The quality assessment of non-RCTs (ROBINS-I).
Discussion
This systematic review and meta-analysis found that AI-based DSD significantly enhances patient and clinician satisfaction (58%, 95% CI: 0.30–0.86, p < 0.01) and improves facial esthetic outcomes, such as smile symmetry, lip arcs, and incisal edge visibility. These findings align with the precision and personalization offered by AI algorithms, which analyze facial and dental features to create tailored smile designs.26,27 The high satisfaction rate reflects AI's ability to produce predictable, aesthetically pleasing outcomes and facilitate patient–dentist communication through digital simulations.28,29
The use of digital design has the potential to increase patient satisfaction and improve clinical success, 30 although DSD programs are valuable tools. However, the most appropriate features to be included in these programs are still being investigated. Another review of commonly used DSD programs observed that overlooking one or more aesthetic criteria can interfere with achieving the most ideal treatment plan and esthetic outcomes. 31 Therefore, landmark selection plays an important role in treatment planning for the aesthetic quality of restorations produced using these programs. In the present study, different landmarks (Table 2) were identified that play important roles in smile design based on AI. These landmarks include the dental midline, incisal edge position, gingival contour, and smile symmetry, which serve as reference points that guide the AI algorithm in creating a balanced and harmonious smile. Each landmark influences important elements such as the proportion, alignment, and harmony of the face. All of these landmarks are necessary for achieving aesthetically pleasing outcomes. This minimizes the need for revisions and improves the overall treatment success rate. Consequently, the careful selection and use of these landmarks in AI-based smile design contribute to greater patient satisfaction and more predictable and optimal results.
The strengths of this study include its comprehensive evaluation of AI's role of AI in enhancing dental aesthetics and patient satisfaction, as well as its inclusion of multiple available studies that provide robust data on clinical and aesthetic outcomes. This analysis leveraged advanced AI methodologies to assess their practical application in dental treatment, offering valuable insights into emerging trends.
However, this study has limitations, such as high heterogeneity (I² = 60.23%) and potential publication bias, as indicated by the regression test for funnel plot asymmetry (p < 0.01). Selection bias in participant recruitment, particularly in case studies, may also skew results. Patient expectations and cultural differences, which vary across regions (e.g. preferences for smile aesthetics in Yemen vs. Brazil), may influence satisfaction scores and were not adequately addressed in the included studies. The lack of cost-effectiveness studies limits understanding of AI-based DSD's practical implementation in diverse healthcare settings; only one study briefly mentioned costs, highlighting a gap in economic evaluations. Ethical considerations, such as ensuring informed consent for AI-driven treatments and addressing potential over-reliance on technology, remain underexplored and warrant further investigation to ensure responsible AI use in medical aesthetics. In addition, the long-term impact of AI-generated smiles on patient satisfaction and treatment durability remains underexplored. Notably, very few studies are available, and further high-quality prospective studies are required to validate the findings across diverse populations and clinical settings. In addition, further exploration of integrating AI with 3D images and advanced facial recognition technology may increase the precision and accuracy of smile designs. Finally, evaluating cost-effectiveness and patient-reported results will help provide a more comprehensive understanding of the overall benefits and limitations.
Clinical significance: These findings are significant for clinical practice, as AI-based DSD offers a scalable, data-driven approach to enhance patient satisfaction and esthetic outcomes. For researchers, the results underscore the need for standardized protocols and diverse, high-quality studies to validate AI's long-term efficacy. The historical evolution of smile design, from ancient practices (e.g. Phoenicians carving animal tusks in 800 BC) to modern AI-driven tools, highlights the transformative potential of technology in dentistry. 5
Conclusion
AI-based DSD significantly improves patient and clinician satisfaction (58%, 95% CI: 0.30–0.86) and facial esthetic outcomes by leveraging precision and personalization. Despite high heterogeneity and publication bias, AI-driven tools show promise in enhancing treatment predictability and communication. Further research is needed to standardize methodologies, evaluate long-term outcomes, and assess cost-effectiveness and ethical implications to fully integrate AI into dental practice.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251388392 - Supplemental material for Impact of artificial intelligence-based digital smile design on patient and clinician satisfaction and facial esthetic outcomes: A systematic review and meta-analysis
Supplemental material, sj-docx-1-dhj-10.1177_20552076251388392 for Impact of artificial intelligence-based digital smile design on patient and clinician satisfaction and facial esthetic outcomes: A systematic review and meta-analysis by Ravinder S Saini, Kanwalpreet Kaur, Vishwanath Gurumurthy, Rayan Ibrahim H Binduhayyim, Ashish Kaushik, Mohamed Saheer Kuruniyan, Mario Alberto Alarcón-Sánchez and Artak Heboyan in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251388392 - Supplemental material for Impact of artificial intelligence-based digital smile design on patient and clinician satisfaction and facial esthetic outcomes: A systematic review and meta-analysis
Supplemental material, sj-docx-2-dhj-10.1177_20552076251388392 for Impact of artificial intelligence-based digital smile design on patient and clinician satisfaction and facial esthetic outcomes: A systematic review and meta-analysis by Ravinder S Saini, Kanwalpreet Kaur, Vishwanath Gurumurthy, Rayan Ibrahim H Binduhayyim, Ashish Kaushik, Mohamed Saheer Kuruniyan, Mario Alberto Alarcón-Sánchez and Artak Heboyan in DIGITAL HEALTH
Footnotes
Acknowledgements
All the authors are thankful to the King Khalid University, Saudi Arabia, for the financial support.
Ethical approval
Not applicable.
Consent for publication
Not applicable.
Informed consent statement
Not applicable.
Authors’ contributions
R-S and K-K: conceptualization and methodology. A-K, V-G, MAA-S, and AH: formal analysis. R-S: investigation. R-S: resources. A-K and V-G: data curation. R-B, M-M, and MAA-S: writing–original draft preparation. R-S and AH: writing–review and editing. MAA-S and AH: validation. R-S, MAA-S, and AH: visualization. R-S and AH: supervision. R-S and AH: project administration. M-S: funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors extend their appreciation to the Deanship of Research and Graduate Studies at King Khalid University for funding this work through the Large Research Project under grant number RGP2/633/46.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Guarantor
Ravinder Saini.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.