
Abstract
Objective
With the rise of social media, self-narration has become a critical way for people living with cancer to share their experiences and emotions through video blogs. This study examines four major narrative components of cancer vlogs to explore whether different narrative components are associated with emotions (positive, negative, or problem) and whether these components and social support requests influence the types of social support provision in comments.
Methods
This study employs quantitative content analysis. We conducted stratified random sampling on bilibili, selecting 131 eligible videos and all 12,427 affiliated comments as samples for this study.
Results
The results indicate that self-experience sharing is less prevalent in vlogs with positive emotions. Specifically, discomfort and new normal are more prevalent in vlogs with negative and problematic emotions than in those with positive emotions. Problem facing is more prevalent in vlogs with negative emotions than in those with positive and problematic emotions. Regarding social support exchanges, vlogs with the discomfort narrative component received less instrumental and emotional support, while vlogs with suggestion offering received more informational support. Moreover, this study finds non-optimal matching in social support request-provision. Although requesting instrumental support in vlogs evoked more instrumental support in comments, requesting emotional or informational support did not elicit corresponding support, and informational support requests even reduced emotional and instrumental provisions.
Conclusions
The results showed the relationship between the narrative components and emotional expressions of cancer vlogs and revealed the matching status of social support requests and provision in non-health-themed cancer online communities.
Introduction
Cancer is a public health issue of great concern in China and worldwide since it is the world's second-largest cause of death, with a high prevalence. 1 For decades, medical organizations and specialists have fought against various cancers. Their efforts have yielded deeper insights into the disease and advanced preventive and therapeutic strategies. With these efforts, cancer is now often managed as a chronic condition, 2 leading to prolonged survival and improved quality of life for people living with cancer (PLWC).3–5 Although medical knowledge of cancer has gradually improved, the general public's perceptions of cancer remain limited and biased. In particular, cancer goes beyond its medical meaning and has been extended into negative social metaphors. 6 It is often regarded as incurable and closely associated with metaphors of pain, hopelessness, and irreversible death. 7 Some negative signs of cancer are harmful to PLWC, leading to additional stress beyond the health consequences of cancer. 8 Therefore, attention to the public's understanding of cancer is essential, as it is closely tied to the well-being of PLWC beyond medical treatment.
The video blog, formed in a first-person narrative user-generated video, is a way for PLWC to self-narrate their cancer experiences. 9 It presents their subjective beliefs and feelings derived from personal encounters. 10 Cancer-related video blogs are beneficial for PLWC. On the one hand, they enable PLWC to present cancer characteristics through an emic approach, helping to overcome stereotypes and reconstruct public knowledge of cancer. 11 On the other hand, they serve as an adaptive coping tool for PLWC, helping to solve PLWC's physical and emotional problems and thereby enhancing well-being.12–14 Consequently, it has become an emerging form of self-presentation of PLWC in online communities. 15 Although video blogs contain multimodal content, this study focuses on the narrative, as it represents the core interests through which PLWC perceive and reconstruct their cancer experiences.16,17
The current study focuses on the outcomes of the narrative of PLWC through dual dimensions: psychological outcome embodied in emotional expressions, and social interaction outcome reflected in social support receptions. Emotion expression is considered to be closely intertwined with patients’ self-narratives and reflects the appraisal outcomes of personal and environmental circumstances.18,19 Although emotions are crucial for understanding patients’ current states, the relationship between narrative components and emotional expressions remains understudied. Moreover, self-narratives trigger social interactions on social media, with supportive communication being one of the most important forms due to its critical role in PLWC's well-being. Previous research has demonstrated that forms and components of PLWC's narratives caused different functional online social support provisions.12,20 Nevertheless, because narrative is deeply embedded in social and cultural contexts, 21 the relationship between narrative components and social support may be situational rather than constant.
Accordingly, the current study analyzes cancer-related video blogs to examine how narrative components are associated with emotions and the reception of social support. Notably, this study focuses on the Chinese context, one of the world's largest cancer-burden countries, with the annual new cases twice that of the US.22,23 The scarcity of culturally grounded research on PLWCs’ online self-narrative practices in China creates an urgent need for such context-specific investigations.
Self-narrative cancer
A self-narrative is an immersive personal storytelling of a specific sequence of events rather than an objective description of facts. It is meaningful because it represents the concerns of the narrator. 16 Narrative medicine is a research approach that addresses the self-narrative of patients. It is believed that the narrative is crucial because it allows researchers to assess patients’ life status and understand their feelings about the illness. 19 The self-narrative of PLWC involves the entire process of cancer, including the diagnosis, disease course, progress, and coping. 16 It is not only an adaptive coping mode used by PLWC to address problems caused by cancer24,25 but also helps medical practitioners build a patient-centered communication mode by standing from the perspective of PLWC.16,26 Notably, the scenarios of self-narratives of PLWC have changed significantly in the digital age. Social media enables them to share their stories beyond clinical settings, 27 and narrative medicine research also extends to their attention to narratives on social media. 28
The self-narrative is a construction of personal concerns, and its narrative component reflects what the narrator considers important.16,19 Previous studies on the narrative of cancer self-narratives have shown that there are four main narrative components: discomfort, problem facing, new normal, and suggestion offering.
The discomfort describes physical and mental damage due to cancer or its treatment. It encompasses features such as pain, fatigue, reduced functions, and body image changes.29–32 Pain is paradoxical in the narrative. Although caused by cancer, it is regarded as an indispensable part of healing. 32 Therefore, narratives of pain concern not only the catharsis of suffering but also strategies for living with it. 29 Narratives of fatigue highlight its impact on daily life, such as constant sleepiness that prevents PLWC from performing routine tasks. 31 Reduced functions refer to the impact of cancer on bodily functions (e.g. trembling and fainting) and the impact of treatment on bodily functions (e.g. amputation). It makes them unable to adapt and live independently.30,31 Narratives of body image changes show less severe physical consequences in the discomfort component, which involves surgical scars, hair loss, and sudden weight gain. However, it is highly related to mental disorders and is worthy of attention. 31
The problem facing describes the various types of social problems associated with cancer, including economic and occupational issues, policy issues, and COVID-19 issues. Economic and occupational issues are universal domestically and worldwide. In China, PLWC face high medical expenditures 33 and must balance their medical, basic, and luxury needs. 34 They also experience difficulties returning to work after treatment, 35 which are reflected in the narratives. Narratives of policy issues highlight the challenges in policy implementation (e.g. medical insurance) and efforts to seek solutions. 36 COVID-19 issues have emerged during the pandemic as people were required to make additional efforts to protect themselves. Narratives of COVID-19 issues primarily focus on the specific challenges encountered throughout the pandemic and related restriction measures. 37
The new normal describes the PLWC's identification of new identities, behaviors, and social norms. 38 Previous studies have pointed out that the new normal is PLWC's self-identity transitions after the critical turning point: diagnosis. After diagnosis, they self-identified as a “warrior” to fight against cancer 39 or a “changed man.” 40 With this change in identity, they shaped new behaviors to meet their physical and sociocultural needs. 41
The suggestion offering includes providing emotion-focused or problem-focused strategies for other PLWC or healthy people to solve their problems. PLWC often uses personal experiences to help others in the narrative. They provide emotion-focused strategies, such as staying positive and calm, as well as problem-focused strategies, such as exercising and following guidance. 42 Moreover, the suggestion offering is not only provided to PLWC but also to the general people. For example, the emotion-focused suggestions include maintaining a positive attitude toward life, while the problem-focused suggestions involve asking people to undergo a medical checkup to prevent severe illness. 12
Previous studies have shown that the online self-narratives of PLWC have the following characteristics. First, narrative can take various forms (e.g. text, videos, and photos). Second, the narrative scenarios differ, for example, health-themed online communities (i.e. patient groups and disease forums) and non-health-themed online communities. Third, the sizes of audiences are distinct. Private communication in a group has a few audience members, whereas videos posted on social media reach large audiences. It is important to clarify that the cancer-related video blogs in this study are video-form narratives for the public in non-health-themed communities, which remain understudied in China. Therefore, to explore the narrative components of cancer-related video blogs in China, this study proposes the following research questions: RQ1: What is the frequency of different narrative components presented in cancer-related video blogs in China?
Narrative components and emotional expressions
Many researchers have realized the importance of narratives and have analyzed different forms of narratives in previous research. However, most of the studies have concentrated on narrative features, functions, and contents rather than outcomes and interconnections with other factors in storytelling. 17 Yet these outcomes and interconnections are more critical to patients’ well-being. Medical narrative criticizes this trend in medical research as the overemphasis on objective statistics, but ignores humanizing care and well-being. 43 Notably, due to the uncertainties of self-narrative, the outcomes of unidimensional research on how patients describe their experiences would be doubted as not sufficiently stable to present the overall situations of PLWC's online self-narrative. Harter and her colleagues highlighted the indetermination and contextuality of patients’ self-narratives,17,44,45 and they used “curators” and “gatekeepers” 17 to describe patients’ subjectivity in self-narrative practices. Therefore, it is important to extend the narrative research of cancer-related video blogs to other factors to achieve a robust conclusion for presenting an overall picture of online cancer self-narrative.
The narrative components in cancer vlogs evoke specific emotional expressions.6,16,33,46,47 The appraisal theories of emotions 46 point out that emotions arise from appraisals of individuals, the environment, and their relationships. When feeling, coping, behavior, or mental responses change during the appraisal process, corresponding emotions are activated. In turn, these emotions can also lead to changes in other components. Since cancer self-narrative reflects not only how external stimuli change the appraisal processes, 26 but also represents how individuals cope with the circumstance-caused stimuli, emotions are inevitably involved in this process.
Based on the cognitive–motivational–relational theory, 48 emotions are classified into three categories: positive, negative, and problematic. If the situation is congruent with the goal, the emotions are classified as positive. Positive emotion is present if the situation is congruent with the goal and contains happy–joy, pride, love–thankfulness, and relief. When the situation is incongruent with the goal, negative emotions will be presented, including anger, fright–anxiety, and guilt–shame. A special case is problematic emotion, represented by hope. Although incongruent with the current goal, hope reflects a forward-looking expectation of possible positive change. It is considered a problematic emotion because hope does not align fully with either the consistency of positive emotions or the inconsistency characteristic of negative emotions. As Lazarus proposed, hope reflects the motivational tension arising from an unfulfilled or threatened goal while simultaneously maintaining an orientation toward potential improvement. 48 Detailed information about emotions is shown in Figure 1.
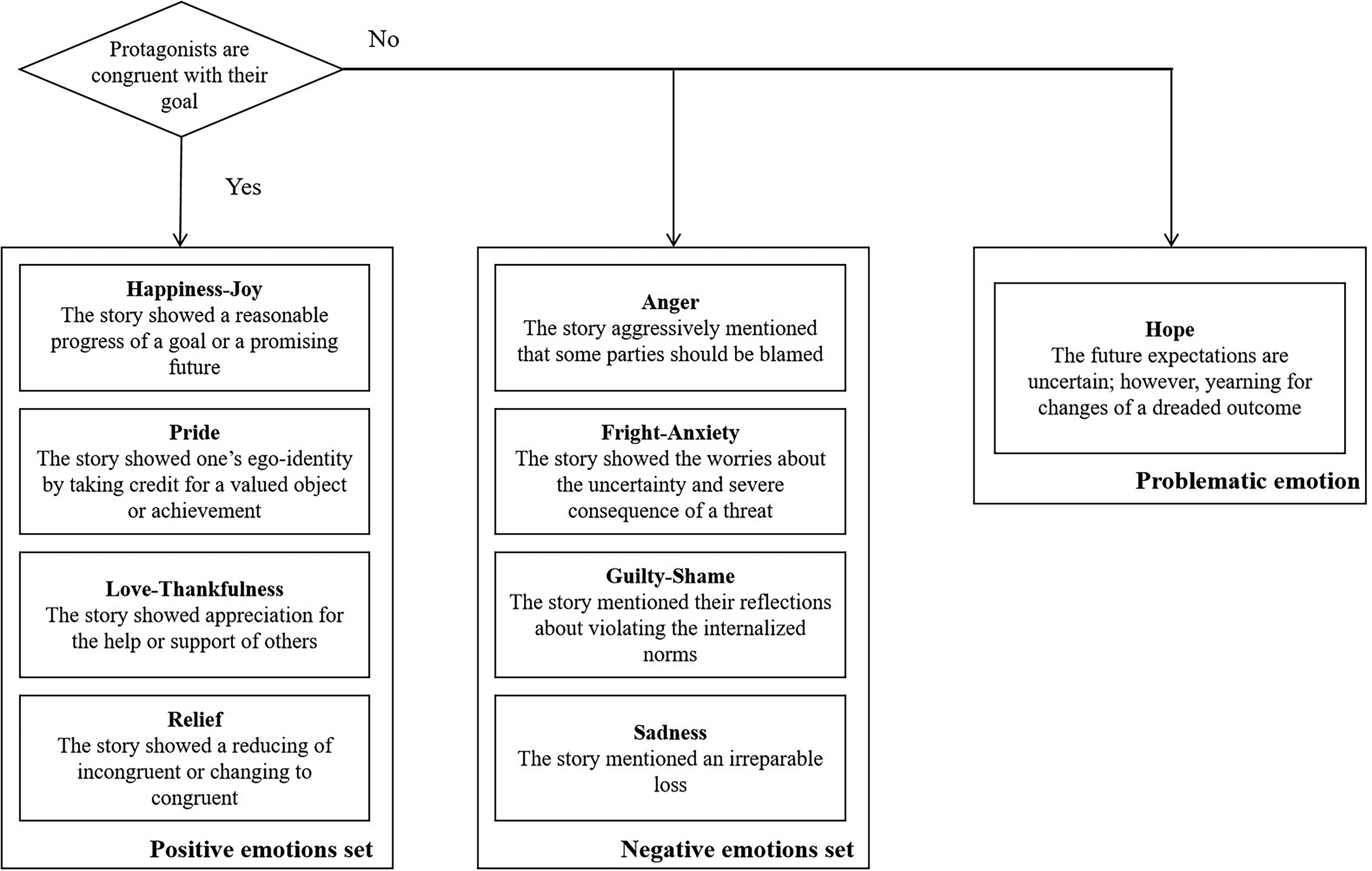
Emotion classification framework for cancer-related video blogs.
Appraisal theories of emotion emphasize the stable relationships between appraisal processes and emotions, with specific appraisals generating specific emotions. 46 Narratives are outward expressions of the external stimuli that PLWC encounter, 16 reflecting how individuals perceive and respond to these events. 6 The narrative component is a set of similar narrative content features that stem from comparable external stimuli. Since emotions arise from individuals’ appraisal of the certainty of a stimulus and the motivation congruence, 49 similar external stimuli are likely to trigger the same internal appraisals and emotions. Therefore, specific narrative components should be associated with corresponding patterns of emotional expression.
Notably, the present study adopts the appraisal perspective to investigate how the external stimuli rooted in the narratives influence the emotional expressions. Roseman 49 developed the emotion system model to explain the emotion outcomes based on the appraisal factors, including motivation consistency, control potential, uncertainty, attribution, and problem and motivation types. Among them, motivation consistency determines the valence of the emotion, and uncertainty caused by the stimuli gives rise to whether the problematic emotion, hope, arises. The relationships among narrative components, external stimuli, uncertainty, motivational consistency, and potential emotions are summarized in Table 1.
Narrative components, external stimuli, emotion appraisals, and potential emotions.
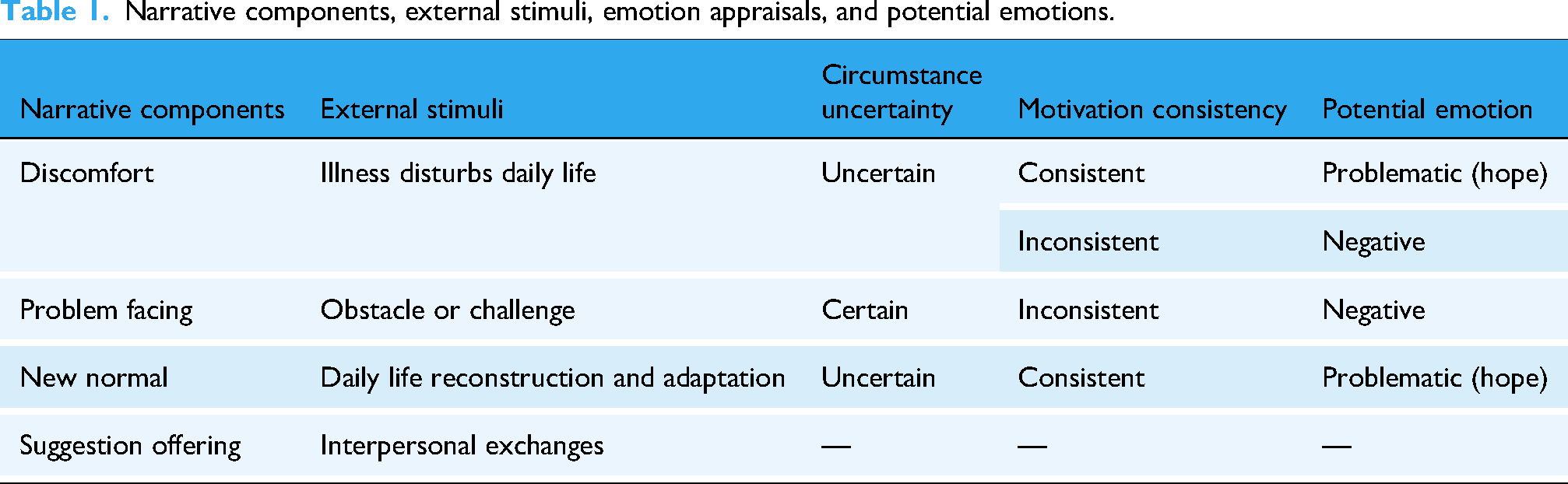
The discomfort narrative component is closely associated with the uncertain circumstances.50,51 Specifically, in discomfort narratives, the external stimulus primarily arises from the disruption and disturbance that illness imposes on an individual's original life. The disruption threatens the continuity of self-narrative and core assumptions about the world and the future, thereby increasing uncertainty. 50 Under these conditions, PLWC are forced to cope with this challenge while being unable to predict future outcomes, thereby experiencing a heightened sense of uncertainty. 51 According to the emotion system model, in a highly uncertain context, when the narrative content reflects motivational inconsistency, negative emotions are more likely to emerge. Conversely, when it conveys an expectation of motivational consistency, problematic emotion (i.e. hope) is more likely to arise. 49 Therefore, this study proposes the following hypothesis:
H1: Cancer-related video blogs containing the discomfort narrative component are expected to co-occur more frequently with negative and problematic emotional expressions than with positive emotional expressions.
Compared with discomfort narratives, the problem facing is generally associated with relatively certain circumstances. The external stimulus in the problem-facing narratives often involves a clearly identified obstacle or challenge that requires active problem-solving or decision-making from individuals. 52 Moreover, the problem-facing narratives are often marked by motivational inconsistency, as circumstances or required actions hinder goal achievement and elicit negative affect in line with the emotion system model. 49 Therefore, this study proposes the following hypothesis:
H2: Cancer-related video blogs containing the problem-facing narrative component are expected to co-occur more frequently with negative emotional expressions than with positive or problematic emotional expressions.
The new normal reflects the appraisal of the transformation of their new subjectivity. The external stimulus in new normal narratives often stems from life changes that lead individuals to reconstruct their identity and adapt to new circumstances. 53 Although the circumstances remain uncertain, these narratives are oriented toward positive adjustment to a new identity and environment. 53 This adaptive orientation is more likely to align with motivational consistency. 54 According to the emotion system model, when high uncertainty is coupled with motivational consistency, problematic emotion (i.e. hope) is more likely to be evoked. 49 Hence, this study proposes the following hypothesis:
H3: Cancer-related video blogs containing the new normal narrative component are expected to co-occur more frequently with problematic emotional expressions than with positive or negative emotional expressions.
Discomfort, problem-facing, and new normal narrative components are self-focused, centering on the narrator's own experiences and appraisals. In contrast, suggestion offering is an other-focused narrative component. It reflects the narrator's interactions with other members of online communities. Previous research has primarily focused on emotional expressions related to one's personal circumstances, 55 and analyses based on the emotion system model have followed this approach. However, interactional emotions arising from interpersonal exchanges are also common in the context of cancer. 56 Therefore, this study explores the following research question:
RQ2: Does the suggestion-offering narrative component differ in its patterns of co-occurrence with emotional expressions?
Online social support
Since the 1970s, research on social support has gained significant prominence. 57 In recent decades, the functional definition of social support has been extended and enriched. Cobb 58 believed that social support is the information that makes people feel cared for, loved, esteemed, and networked, which was one of the earliest definitions of social support. He focused on the information properties and emotional outcomes of social support. House 59 focused on action outcomes and extended the forms of social support to include instrumental, informational, appraisal, and emotional support. Cutrona and Suhr 60 integrated previous studies on social support and categorized it into action-facilitating and nurturant support. Action-facilitating support refers to outcomes that facilitate problem-solving, while nurturant support refers to emotional outcomes that reassure individuals in coping with mental discomfort. 60 This functional classification has been widely applied in offline social support research.
Although Cutrona and Suhr's 60 definition was systematic in the offline context, online social support differs greatly from offline social support in terms of participants, quantity, quality, space, and flow. Most participants in online social support have weak-tie relationships, while strong-tie relationships dominate offline social support.61,62 Online social support involves massive amounts of information due to the massive number of participants involved, 63 while offline social support involves limited information. The qualities of online social support are precarious. Individuals can receive high-quality social support, such as professional medical help, 61 while they can also receive low-quality social support, such as misinformation.64,65
Therefore, Wright et al. 61 analyzed computer-mediated social support systematically and suggested that opinions, insights, experiences, and perspectives shared in online social communities involve exchanges of online social support. Moreover, he proposed classifying online social support as informational, instrumental, or emotional. The definition and classifications of online social support have been widely adopted in research.66–68 Therefore, this study also utilizes classification to examine the different types of online social support.
Social support is essential for PLWC, as it helps them solve problems and maintain mental health, thereby enhancing quality of life. Previous studies have suggested that online social media platforms are one of the main channels through which PLWC receives social support.15,67 Users of social media platforms construct online communities that allow people to freely communicate and exchange social support. PLWC present their feelings and propose their requests in video blogs, and other social media users provide their help. Although previous studies have discussed the preferences of social support providers in different contexts,69–71 few studies have discussed whether the request for the corresponding functional type of social support can directly lead to a greater presence of that type of social support in the community. Optimal matching theory of social support, developed by Cutrona, 72 points out that social support works best when the type of support provided matches the demands of the recipient's coping needs. 72 Previous studies in the context of cancer have also provided empirical support for this proposition.73,74 Taken together, these findings underscore the importance of the match between support seeking and support provision in online contexts. Therefore, this study examines the matching between support requests and support provision triggered by cancer-related vlog narratives and proposes the following research question:
RQ3: Do narrators’ requests for (a) information, (b) instrumental, and (c) informational support in video blogs influence the provision of these three types of support in the comment section?
Moreover, online social support provision in the comment sections was regarded as an outcome elicited by the self-narratives of PLWC. Previous studies have shown that different narrative components and forms influence online social support reception.12,15 However, these studies lack attention to instrumental support reception and were mostly discussed in the context of Western societies. This study undertakes an exploratory examination of the relationship between specific narrative components and the types of social support provided in response in the Chinese context, for two main reasons. First, as emphasized in narrative medicine, both self-narratives and the responses they elicit are highly context-dependent, suggesting that any observed associations may be contingent rather than universally generalizable. 19 Therefore, previous research on the relationship between narrative components and social support reception has also tended to adopt an exploratory approach. 15 Second, the objective of this research is not to offer strategies for instructing the self-narratives of PLWC, but to identify the underlying structural issues embedded in the process of social support exchange. Based on the above, this study proposed the following research question:
RQ4: Do the (a) discomfort, (b) problem facing, (c) new normal, and (d) suggestion offering narrative components influence the reception of informational, instrumental, and emotional support in the comment section?
Method
This study utilized quantitative content analysis to test the hypotheses and address the research questions. The research was conducted from February to June 2022. The study design was completed in February 2022, data collection was conducted in March 2022, the coding process took place from March to June 2022, and data analysis was conducted in June 2022. This study was conducted at Macau University of Science and Technology, located in Macau SAR, China.
This study received a waiver of ethics approval from the Research Ethics Committee of the Faculty of Humanities and Arts at Macau University of Science and Technology (Certificate No. MUST-FA-2025004), as it did not involve human participants. In terms of data protection, this study collected and processed data in accordance with national and regional regulations (e.g. the Personal Information Protection Law of the People’s Republic of China and the Personal Data Protection Act of Macau SAR) and the AoIR guidelines. During data collection, the principle of data minimization was applied, and only the information necessary to answer the research questions and test the hypotheses was collected. Accordingly, we did not store the video files and retained the uniform resource locators for coders to view the videos online. In addition, an anonymization procedure was applied to remove highly identifiable information (i.e. usernames and user IDs), which were replaced with numerical identifiers before coding. Regarding data management, anonymized datasets were provided to coders, who are prohibited from sharing the data with any other party.
Sampling
This study sampled videos and comments on bilibili, a Chinese YouTube-like social media video platform. We chose bilibili for the following reasons. First, it is a representative active online social community in China with nearly 100 million daily active users. 75 Second, it imposes no duration limit on uploaded videos, making it suitable for the format of video blogs. Third, it provides a large number of cancer-related video blogs available for analysis.
This study collected data on 25 March 2022, covering all cancer-related video blogs uploaded prior to the sampling date. Stratified random sampling was conducted based on the number of video plays to capture a range of audience reach and engagement levels. The first step involved using the keywords “cancer vlog (癌症vlog)” and “living with cancer (患癌)” to search and collect 2448 related videos. The second step was to divide these 2448 related videos into 10 groups according to their play count (top 10%, 11%–20%, 20%–30%, …, 91%–100%). The third step utilized simple random sampling to obtain 10% of the videos in each group. Therefore, 245 videos were sampled. The fourth step was to manually exclude videos that were not accessible (n = 11), not in video blog form (n = 64) (e.g. videos that were edited compilations of news or scenes from dramas), or not related to cancer (n = 39) (e.g. “green cancer” referring to Crohn's disease, or offensive expressions such as “Zhinan cancer (直男癌)”). Finally, 131 eligible videos and all 12,427 affiliated comments were used as samples in this study. The sampling procedure is presented in Figure 2.

Videos and affiliated comments sampling procedure of the current study.
Coding
In this study, (a) each video and (b) each comment were two separate coding units. The researcher established different coding schemes for videos and comments after reviewing previous studies and gaining a simple qualitative understanding of the sample.
According to the video coding scheme, the coders were asked to code each video according to its content, title, and description. Cancer types were coded according to the International Statistical Classification of Diseases and Related Health Problems (10th Revision). 76 Protagonist characteristics were coded as expressions in the video content or categorized as unspecified if the coders could not tell. Emotional expression was coded as positive, negative, or problematic emotions, following Lazarus's research (see Figure 1). 48 If a video expressed more than one emotion, the stronger emotion expressed in this video was adopted. Four narrative components, discomfort, problem facing, new normal, and suggestion offering, were coded according to whether they were present in the video. The social support request was coded for whether the video content requested information, emotional, or instrumental support. After training, the author and another native Chinese coder with medical knowledge separately coded the same 29 (20%) video samples to examine the intercoder reliability. Then, the two coders split the rest of the video samples and separately coded them according to the coding scheme. The coding scheme for videos is presented in Table 2.
Coding scheme for analyzing narrative components and social support in video blogs.

According to the comment coding scheme, the coders were asked to code whether each comment provided informational, emotional, or instrumental support. Detailed information is provided in Table 3. After training, the author and two other native Chinese coders separately coded the same 800 (5%) comments to examine the intercoder reliability. Then, the three coders split the rest of the video samples and separately coded them according to the coding scheme.
Coding scheme for analyzing social support in comments.

Note. 1 rb refers to retinoblastoma. 2 Sanlian refers to likes, coins, and favorites for video; it is linked to creator revenue.
Intercoder reliability
This study utilizes Bennett et al.'s 77 S score to examine the intercoder reliability of each variable to assess intercoder reliability, as the individual distribution was highly uneven in this study, which could bias Krippendorff's α and Cohen's κ. 78 The intercoder reliability (S) is presented in Table 4.
Intercoder reliability (Bennett et al.'s S score) for variables coded for video blogs and affiliated comments.

Note. Bennett et al.'s S score was used to assess intercoder reliability for each variable. Values range from 0 to 1, with higher scores indicating greater agreement among coders. Scores above .70 are considered to represent acceptable reliability.
A MATLAB function 79 was used to calculate the S of the two video coders. The results show that the intercoder reliability of cancer type (S = .96), sex (S = .86), age (S = .86), emotional expression (S = .74), discomfort (S = .79), problem facing (S = .93), new normal (S = .79), suggestion offering (S = .79), information support request (S = .79), emotional support request (S = .93), and instrumental support request (S = 1.00) were acceptable.
This study also calculates the S score of three comment coders. The results show that the intercoder reliability of informational support provision (S = .90), emotional support provision (S = .74), and instrumental support provision (S = .96) were acceptable.
Data analysis
SPSS Version 26 was used to analyze the data. Differences in categorical variables were examined using chi-square tests. Assumptions for the chi-square tests were checked to ensure that no more than 20% of the expected cell counts were below five. Multiple linear regressions (MLRs) were performed to assess the relationships between continuous dependent variables and multiple independent variables. For the MLRs, multicollinearity was assessed using variance inflation factors, and the independence of residuals was evaluated using the Durbin–Watson test. Effect sizes were reported in the Results section, as Cramer's V for the chi-square tests and as Cohen’s f 2 for the MLRs. Statistical significance was set at p < .05 (two-tailed) for all analyses.
Results
Descriptive
In general, most video blogs presented the sex and age characteristics of protagonists. A total of 53.4% of the cancer video blogs (n = 70) included female protagonists, 35.9% of the cancer video blogs (n = 47) included male protagonists, and 10.7% (n = 14) did not clearly show the sex of the protagonists. Young-middle-aged protagonists are shown in 57.3% of cancer video blogs (n = 75), the most commonly shown. Older protagonists were shown in 19.8% of the cancer video blogs (n = 26), and adolescent protagonists were shown in 16.0% (n = 21). The protagonist's age could not be determined in the rest of the cancer video blogs (6.9%, n = 9). Moreover, most of the video blogs did not mention the specific cancer type of the protagonists (60.3%, n = 79). Detailed information is provided in Table 5.
Descriptive statistics results of the cancer vlog samples in the current study.

The different types of social support provided in the comments were uneven. Emotional support was most prevalent, as 52.4% of the comments (N = 6505) provided emotional support. Only 7.1% of the comments (N = 887) provided informational support, and 4.5% of the comments (N = 556) provided instrumental support (see Figure 3).
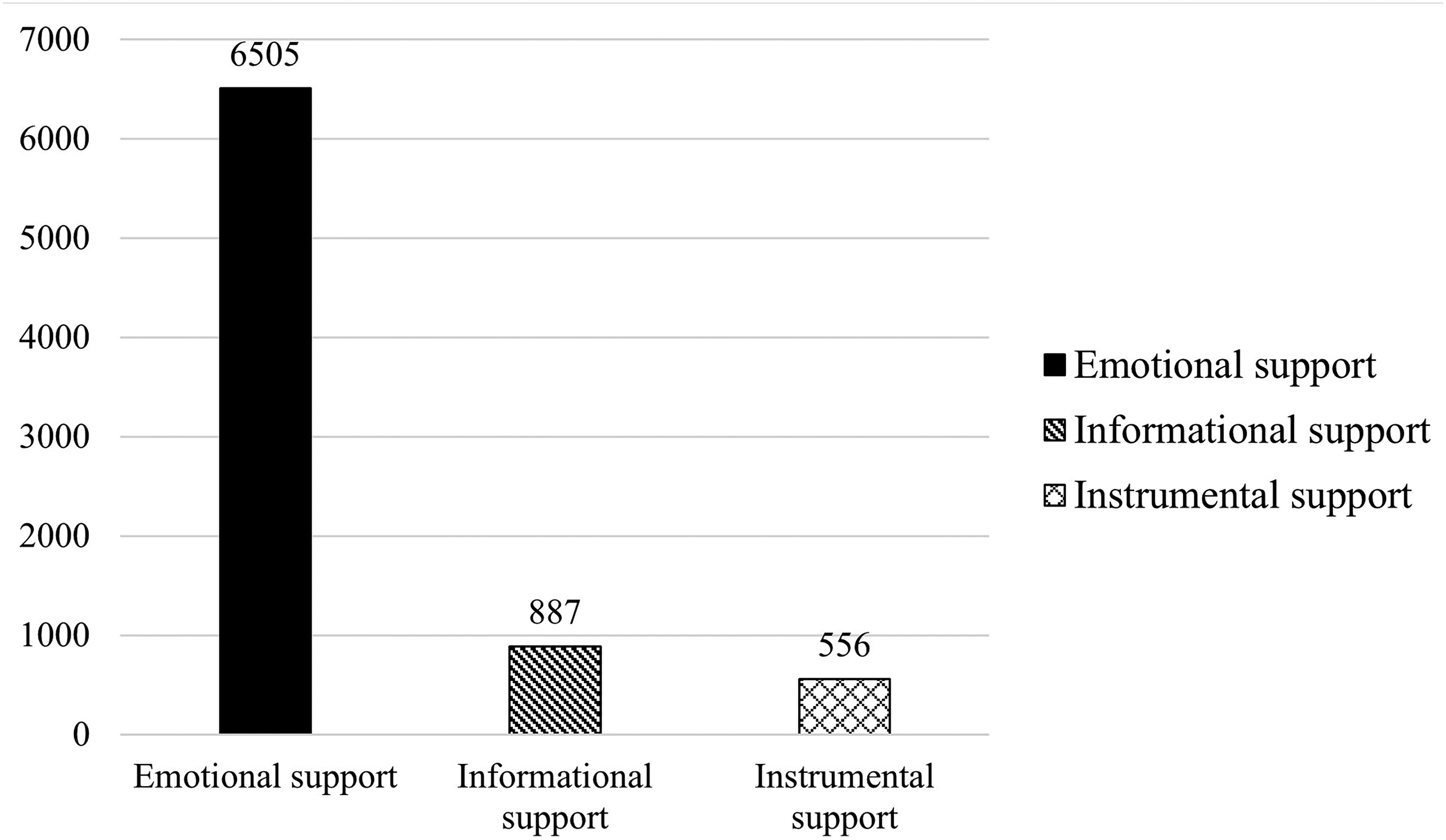
Number of social support provisions in comments on cancer-related video blogs.
Narrative components and emotional expression
The results showed that discomfort was the most prevalent narrative component, and 46.6% of video blogs (n = 61) presented discomfort. The new normal was presented in 35.9% (n = 47) of the cancer video blogs. Both problem facing and suggestion offering was presented in 20.6% (n = 27) of the cancer video blogs.
A total of 48.1% of the video blogs (n = 63) showed positive emotions, 35.1% of the video blogs (n = 46) showed negative emotions, and 16.8% of the video blogs (n = 22) showed problematic emotions. The results answer RQ1.
Chi-square tests were conducted to test H1, H2, H3, and answer RQ2. The results show that there were significant differences in discomfort (
Specifically, compared with positive emotions, discomfort was significantly more prevalent in negative (
Frequencies, percentages, and chi-square test results of narrative components in cancer-related vlog samples associated with different emotions.

Note. (%) indicates the proportion of a given narrative component used in videos with a certain emotion. Because a video may contain more than one narrative component, the total percentages exceed 100%. Problematic emotion refers to hope, as it does not fit neatly into either the positive or negative category. *p < .05, **p < .01, ***p < .001.
Narrative components and social support
MLR models were used to answer RQ3 and RQ4. The narrative components and social support requests in cancer video blogs were the independent variables. The protagonist characteristics and cancer types were control variables. The informational, instrumental, and emotional support received in comments were separately set as dependent variables, and detailed information is provided in Tables 7 to 9.
Multiple linear regression model predicting informational support reception from narrative components and social support requests in cancer-related vlog samples.

Note. *p < .05, **p < .01, ***p < .001. Female (sex), young-middle-aged (age), unspecified, metastatic, or had multiple cancers (cancer type) were excluded from these models due to collinearity with other variables. 95% LLCI = lower limit of 95% confidence interval for the unstandardized coefficient B, 95% ULCI = upper limit of 95% confidence interval for the unstandardized coefficient B. Covariants: sex of protagonist, age of protagonist, and cancer type.
Multiple linear regression model predicting instrumental support reception from narrative components and social support requests in cancer-related vlog samples.

Note. *p < .05, **p < .01, ***p < .001. Female (sex), young-middle-aged (age), unspecified, metastatic, or had multiple cancers (cancer type) were excluded from these models due to collinearity with other variables. 95% LLCI = lower limit of 95% confidence interval for the unstandardized coefficient B, 95% ULCI = upper limit of 95% confidence interval for the unstandardized coefficient B. Covariants: sex of protagonist, age of protagonist, and cancer type.
Multiple linear regression model predicting emotional support reception from narrative components and social support requests in cancer-related vlog samples.

Note. *p < .05, **p < .01, ***p < .001. Female (sex), young-middle-aged (age), unspecified, metastatic, or had multiple cancers (cancer type) were excluded from these models due to collinearity with other variables. 95% LLCI = lower limit of 95% confidence interval for the unstandardized coefficient B, 95% ULCI = upper limit of 95% confidence interval for the unstandardized coefficient B. Covariants: sex of protagonist, age of protagonist, and cancer type.
The MLR results indicate that the videos that involved the discomfort narrative component decreased the reception of instrumental (β = −.23, t = −2.70, p = .008) and emotional support (β = −.25, t = −2.69, p = .008), and the videos that involved the suggestion offering narrative component increased the reception of informational support (β = .24, t = 2.69, p = .008). Moreover, requesting instrumental support in videos increased the reception of instrumental support (β = .32, t = 3.88, p < .001). However, requesting informational support via video decreased the reception of emotional (β = −.20, t = −2.06, p = .04) and instrumental support (β = −.23, t = −2.70, p = .008).
The MLR results also showed that videos involving the eyes, brain, and other parts of the central nervous system (type: C69–C72) positively influenced the reception of informational (β = .30, t = 2.72, p = .008), instrumental (β = .30, t = 3.14, p = .002), and emotional support (β = .39, t = 3.58, p < .001). The videos that involved thyroid and other endocrine gland cancers (type: C73–C75) positively influenced the reception of informational support (β = .18, t = 2.09, p = .04). Breast cancer videos (type: C50) positively influenced the receipt of instrumental support (β = .35, t = 4.52, p < .001). The videos that showed an unspecified sex protagonist positively influenced informational (β = .35, t = 2.63, p = .01) and emotional support reception (β = .30, t = 2.30, p = .02). The videos that showed an unspecified age protagonist negatively influenced emotional support recepition (β = −.28, t = 2.24, p = .03).
Discussion
This study combines the narrative medicine approach and emotion appraisal theories to analyze the relationship between narrative components and emotional expression in a more systematic way. The results showed that, unlike traditional media, where PLWC is constructed as weak and painful images and expresses negative emotions, 80 nearly half of the cancer-related video bloggers expressed mainly positive emotions. However, the key narrative components, discomfort, problem-facing, and new normal, were less likely to be associated with positive emotions. According to the proposition of the appraisal theories of emotion, we suggest that the appraisal outcome of the self-experience of cancer may be more strongly associated with negative and problematic emotions. This suggests that PLWC's mental health should be focused on because their daily life is strongly associated with negative emotions.
Our findings analyze and verify the appraisal processes and emotional outcomes associated with discomfort and problem facing from the emotion appraisal perspective. In line with our hypothesis, discomfort narratives were linked to both negative and problematic emotions, while problem-facing narratives were linked exclusively to negative emotions. We believe that discomfort refers to the narrative of deteriorating physical and psychological conditions after cancer. Individuals may differ in their mindsets and coping strategies when facing cancer. Overall, however, cancer survivors carry a heavier emotional burden. Expressions of discomfort are often linked to negative emotions such as fear, anxiety, low self-esteem, stigma, and hopelessness.11,81 In addition, discomfort may also appear more often with hope (i.e. problematic emotion), where PLWC express concerns about the current situation in their self-narratives while still harboring visions of things getting better in the future. The association between problem-facing narratives and negative emotions further underscores the significance of secondary adversities caused by cancer for PLWC. These adversities extend beyond the illness itself to affect their social existence, contributing to negative emotional experiences such as fear, anxiety, and guilt.
Partially inconsistent with our hypothesis, the new normal narrative component elicited both negative and problematic emotions, rather than exclusively triggering problematic emotions. The new normal reflects PLWC's identification with a new identity, the adoption of new behaviors, or the adherence to new norms. While hope in this context can be understood as a form of self-motivation arising from accepting the new patient identity and envisioning a future within this new life, it may also conceal unarticulated anxieties associated with the identity transition. This suggests that research should not limit its analysis to the explicit narratives of a stimulus. It is also important to pay attention to elements that are not presented in the foreground. Such non-foregrounded content may exert a meaningful influence on emotional arousal. In addition, we found that the other-focused suggestion offering component did not elicit any specific emotions. One possible explanation is that the content of the suggestion offering is primarily prepared for interaction with the audience, and the associated stimuli may not be personally salient enough to activate the appraisal process and trigger emotions for the narrator.
This study also reveals the exchange of social support in cancer-related video blogs with different narrative components. A noteworthy finding is that although discomfort due to physical and psychological discomfort from PLWC makes audiences aware of their need for help, cancer-related video blogs containing the discomfort component decreased the reception of instrumental and emotional support. This may be because discomfort is often accompanied by negative emotions that evoke health anxiety and fear. Overwhelming fear and anxiety may cause the audience to avoid and reject information, 82 which in turn may lead to a decrease in social support. In particular, this study reveals social support exchanges in online communities. We find that the narrative component of suggestion offers increased informational support. This means that PLWC provides informational support to other PLWC or healthy individuals via their own experiences, as well as triggering feedback from others’ informational support to themselves. Self-narratives of cancer that rely on new information and communication technologies empower PLWC to exchange information on an equal footing with healthy people. This makes the cancer experience destigmatized and effectively helps other people. This unique space, non-health-themed online social communities, helps to curb the hegemony of able-bodiedness and breaks down the power structure inherent in the binary distinction between health and illness.83,84
Notably, this study presents the matching status of social support requests and provision in non-health-themed online communities. Our findings demonstrate that the online social support exchange does not always follow the optimal matching principle, and we identify two distinct matching modes in this context: optimal matching and counterproductive matching. On the one hand, we observe the optimal matching in instrumental support requests and provision. When PLWC requests economic and other tangible support, community members are more likely to offer the corresponding functional support. This finding echoes the previous research on cancer-related instrumental support exchanges across online and offline communities.85,86 On the other hand, we observe the counterproductive matching in information support requests. When PLWC requests effective information to solve their health issues, community members did not correspondingly increase their provision of informational support. Rather, their provision of instrumental and emotional support decreased. We believe that the reasons for this phenomenon are multifaceted. First, the absence of corresponding support may be explained by low capacity. Informational support typically pertains to medical problems and thus requires greater capacity to provide, as it involves specialized knowledge or personal experiences.70,87,88 Most members of non-health-themed communities lack the requisite expertise, which limits their ability to meet informational requests. Second, the reduction in instrumental and emotional support can be interpreted from a cultural perspective: Chinese culture places a strong emphasis on relationship maintenance, extending beyond close ties to include interactions with strangers. 89 There is a tendency to avoid interference if one cannot help.89,90 This reflects the relational motive of preserving harmony and avoiding embarrassment. 91 Consequently, when individuals are unable to provide effective informational support, they may prefer silence and disengagement, which causes a reduction in social support provision. Third, algorithmic visibility further reinforces this dynamic. Social media algorithms are driven by popularity and engagement metrics.92–94 Due to informational requests often involving specialized scientific or medical knowledge, they are less likely to be promoted under these algorithms’ preferences. This algorithmic bias reduces exposure, thereby objectively lowering the likelihood of receiving diverse forms of support. Previous studies demonstrate that optimal matching of social support is essential for positive outcomes. When the type of support aligns with the recipient's specific stressor, well-being improves. 95 Conversely, mismatching social support may undermine coping effectiveness and exacerbate distress.61,96 The present study reveals that the alignment of online social support exchanges elicited by cancer self-narratives is limited and even results in a decline of social support. This situation may generate adverse effects on narrators. Future research may need to explore further and reveal its mechanisms.
Limitations
This study has several limitations. First, due to data constraints, it only focuses on the four major narrative components in PLWC's self-narratives, which may obscure alternative components associated with emotion. Second, the study adopted a cross-sectional design, restricted to videos uploaded before March 2022. This limitation of the cross-sectional design may reduce the generalizability of the findings. Third, self-selection bias should be noted: only PLWC who were willing to publicly narrate their experiences contributed data, which reflects context-specific communication patterns rather than the broader population of PLWC. Fourth, the analysis was based on bilibili, a video platform whose users are predominantly younger and more highly educated. Consequently, the narrators who chose to publish on this platform may share similar demographic traits, which restricts the representativeness of the findings. Fifth, while we included various characteristics of the video protagonists as control variables, we did not directly control for aspects of video exposure and visibility, such as video length, number of views or likes, and the video channel size. Future research could address this limitation by incorporating such measures to more thoroughly assess their potential influence. Finally, as this was a content analysis of existing data, the conclusions cannot establish robust causal relationships between narrative components and emotional expressions. Future research could employ experimental or longitudinal designs to yield more robust and generalizable insights.
Conclusion
This study examined the relationships between different narrative components and emotion expressions in cancer-related video blogs, as well as between narrative components and online social support reception. The results indicated that the discomfort and new normal narrative component presented more negative and problematic emotions, and the problem-facing narrative component presented more negative emotions. Moreover, the discomfort narrative component negatively affected the reception of instrumental and emotional social support, and the suggestions offering narrative component positively affected the reception of informational support. Additionally, the results also revealed the matching status of social support requests-provision in this context. The instrumental support requests increased the instrumental support provision, while informational support requests decreased the emotional and instrumental support provision.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251386655 - Supplemental material for Self-narrating cancer on social media: Examining the relationships among narrative components, emotional expressions, and social support reception
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251386655 for Self-narrating cancer on social media: Examining the relationships among narrative components, emotional expressions, and social support reception by Yuanming Guo and Xiao Yang in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076251386655 - Supplemental material for Self-narrating cancer on social media: Examining the relationships among narrative components, emotional expressions, and social support reception
Supplemental material, sj-pdf-2-dhj-10.1177_20552076251386655 for Self-narrating cancer on social media: Examining the relationships among narrative components, emotional expressions, and social support reception by Yuanming Guo and Xiao Yang in DIGITAL HEALTH
Footnotes
Acknowledgments
We would like to extend our sincere gratitude to Ms. Wang Yueliang, Ms. Fan Mingming, and Mr. Li Shaoyi for their invaluable contributions in the coding process.
Ethical considerations
This study used publicly available data without human participants. Therefore, ethical review is not required.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.