
Abstract
Background
With the rise of the global aging population, innovative solutions are needed to support healthy aging. Intelligent exercise systems using IoT, big data, and AI offer real-time monitoring, improved safety, interactive engagement, and remote supervision marking a shift from traditional models and promoting self-managed health in older adults.
Purpose
To investigate how Intelligent exercise influence older adults’ digital resilience and adaptation, by integrating quantitative outcome measures with qualitative insights into their real-world experiences.
Methods
This mixed-methods study recruited participants via purposive sampling from a senior fitness club. Participants completed a quantitative questionnaire and a one-to-one qualitative interview to discuss their experiences and adjustment processes when engaging in intelligent exercise.
Results
A total of 69 participants were randomly assigned to either the intervention or control group. The intervention group completed at least six months of an introductory smart sports equipment course. Data were collected via questionnaire, and 16 participants took part in interviews. Resilience scores in the intervention group increased significantly from 21.35 ± 4.37 at baseline to 23.35 ± 5.4 after six months (P = .023). Further analysis of the interview data revealed that the use of smart sports equipment results in three core themes: (1) participants’ health as transitioning from adapting to internalizing digital technology, (2) participants’ experiencing exercises as aligned with their needs, and (3) fostering of close peer relationships.
Conclusion
Intelligent exercise program can strengthen older adults’ digital resilience and promote healthy aging. Future development should enhance usability and accessibility to support sustained adoption.
Keywords
Introduction
According to the World Health Organization (WHO), health promotion empowers individuals to take greater control over their health through social and environmental strategies that extend beyond traditional medical care. 1 To support this, the WHO launched the Decade of Healthy Ageing (2021–2030), 2 urging governments to collaborate across sectors to promote physical activity, self-care, independence, and reduce chronic disease risks among older adults.3–5
Exercise has long been recognized as a key factor in enhancing older adults’ physical, mental, and social well-being6–8 However, motivation and mobility challenges often hinder long-term adherence. Emerging technologies—such as smart sports equipment with real-time monitoring, remote support, and interactive features—offer a safer and more engaging alternative.9–11
Despite the potential of smart sports technology, older adults still face barriers and limitations to using it, making many unable to maintain adequate physical activity levels. Factors such as the equipment's complexity, learning level, and suitability, as well as the user's technology acceptance, can influence exercise maintenance and performance. Although advances in artificial intelligence (AI) have opened possibilities for personalized health management. However, current research has focused on the benefits of intelligent exercise systems, with less attention given to structural barriers—such as limited digital literacy, financial constraints, and privacy concerns—that affect adoption among older adults. Further research is needed to explore the outcomes of smart sports technology use in this population to better address broader issues of equity and inclusiveness in digital health.
This study adopts a mixed-methods design to evaluate the impact of smart sports equipment on the Digital resilience of older adults and to qualitatively explore their lived experiences with intervention. Of particular importance is the concept of digital resilience—the capacity to adapt and thrive in digital environments—which aligns with theoretical models such as the Technology Acceptance Model (TAM). 12 TAM suggests that digital confidence, perceived ease of use, and autonomy are critical factors in supporting long-term engagement and technology adoption in health promotion contexts. 12 Therefore, the objective of this study is to investigate how Intelligent exercise influence older adults’ digital resilience and adaptation, by integrating quantitative outcome measures with qualitative insights into their real-world experiences.
Intelligent exercise and health promotion
Recent advancements in digital health have facilitated the integration of intelligent exercise technologies, such as smart sports equipment and AI-driven platforms into physical activity and health promotion strategies. Intelligent exercises typically combine interactive interfaces, virtual training environments, and gamified components to enhance user engagement and exercise adherence. 13 Smart exercise equipment, including wearables and sensor-based devices, enables real-time monitoring of physiological parameters such as heart rate, step count, and caloric expenditure. 11 These technologies not only track users’ movements and postures for accuracy and safety. 9 but also generate personalized feedback and adaptive training programs using AI algorithms and data analytics.7,11
Several studies have highlighted the benefits of intelligent exercise systems, including improved health self-management through real-time feedback, enhanced motivation via gamified experiences, and remote support for users by healthcare professionals and caregivers.6,14 Intelligent exercise platforms also provide backend management tools and data dashboards, enabling longitudinal health monitoring and facilitating more individualized exercise planning.7,11 Compared to traditional exercise equipment, which lacks remote connectivity and real-time data processing capabilities, smart exercise systems offer greater flexibility and responsiveness-features particularly beneficial for populations with specific health management needs. 15
Prior research has also noted that older adults often struggle to maintain physical activity using conventional equipment due to factors such as limited motivation, lack of feedback, and perceived monotony. 16 Additionally, determining appropriate exercise intensity without technological support is challenging, potentially resulting in ineffective or unsafe exercise practices. 17 Intelligent systems, in contrast, support optimal performance and safety through AI-based feedback, reducing the learning curve and enabling more efficient progress in physical function. 18
Intelligent exercises and digital resilience
Digital resilience is an individual's or organization's ability to adapt to and address challenges in shifting digital environments. It entails the adaptive use of digital tools, psychological acceptance of technological changes, and data-driven health management competence. As the use of smart sports equipment increases, digital resilience is critical for health promotion in older adults, as it enhances older adults’ exercise adaptation, health awareness, and digital engagement.19–21 Therefore, digital resilience can be practically implemented through smart sports equipment and exergames, serving as an important means to support older adults in practicing health promotion. In existing literature, digital resilience has been conceptualized as more than digital literacy or technological adaptability, emphasizing not only the ability to access and use technology but also the capacity to recover from digital disruptions, maintain psychological well-being, and continue functioning effectively in digital contexts. 22 Unlike digital literacy, which primarily concerns knowledge and skills in using technology, and technological adaptability, which refers to adjusting to new tools, digital resilience incorporates coping strategies, emotional regulation, and sustained engagement with digital systems.23,24 Applied in intelligent exercises to assist older adults in familiarizing themselves with and adapting to digital technologies. By engaging in health management through technological approaches, 25 users can learn how to interpret their health data and deepen their data literacy. In addition to enhancing autonomy and decision-making skills in personal health management, smart sports equipment is useful for shaping digital resilience. 24
The interactions and real-time feedback from smart sports equipment can enhance exercise motivation, reduce sedentary behavior, and foster global physical functioning.26,27 Exergames combine exercise with cognitive training to improve physical activity levels, cognitive functioning, and coordination. 28 Intelligent exercises improve users’ moods, help to alleviate their stress, motivate them to exercise regularly, and strengthen their mental well-being. Liu et al. 29 found that installing smart gym equipment in smart homes reduced depression symptoms in older adults. Smart sports equipment also enhances digital engagement in older adults by providing access to social media. Many smart sports equipment applications offer online competitions, workout challenges, and interactive healthcare communities, allowing users to overcome geographical barriers and engage in virtual social activities.27,30 These technologies are important tools for enhancing social engagement, particularly for older adults who feel socially isolated. By decreasing digital exclusion, fostering social connections, and empowering mental resilience, they help older adults to maintain contact with their family, friends, and workout buddies, increasing their social engagement and improving their overall quality of life. 13
Methods
Study design
The mixed-methods design to enhance data complementarity and research depth by integrating quantitative user data with qualitative feedback. Methodological triangulation was employed to combine both data sources, using qualitative themes to interpret and enrich the quantitative findings. This approach strengthened the interpretive depth and practical relevance of the study outcomes.31,32 Researchers recruited participants through purposive sampling at the senior fitness club of a university in Northern Taiwan from June to December 2024. Although recruitment was limited to a single site, the club's members came from three administrative districts: East District, North District, and Xiangshan District, providing a degree of regional representativeness. This purposive sampling strategy was chosen to ensure that participants had consistent access to and experience with structured exercise programs, thereby enhancing the feasibility and reliability of the intervention. The study design has two phases. The research flowchart is shown in Figure 1.

Research flowchart.
The quantitative component employed a quasi-experimental design, with participants assigned to the control and intervention groups based on their affiliated units. The control group continued with their daily conventional exercise routine, while the intervention group received a weekly intelligent exercise program in addition to their conventional exercise routine. The changes in the participants’ mental resilience after engaging in intelligent exercise were assessed through a pre- and post-test.
The second phase involved qualitative research, in which in-depth individual interviews were conducted with the participants to explore their multifaceted experiences with intelligent exercise. The interview data were primarily analyzed using a phenomenological approach, with content analysis applied as a complementary method. This process involved both coding frequency analysis and narrative synthesis. To ensure coding consistency and credibility, a double-coding the essence and core meaning of lived human experiences by emphasizing the subjective perceptions and feelings of the participants. 32
While grounded in the philosophical foundation of phenomenology, content analysis was applied as a complementary method to support the analysis by systematically and objectively organizing the data, identifying recurring themes or concepts, and constructing essential experiential structures and conceptual models. Coding frequency analysis was also conducted to quantify the data, and narrative interpretations were generated to further illustrate participants’ lived experiences.
Participants
The inclusion criteria were as follows: (1) age ≥65 years, (2) Participants who completed at least three months of an intelligent exercise course during the study period, Chang et al., 33 which suggests that a program of at least three months is necessary to observe meaningful improvements in health behavior and physical function among older adults, and (3) agreeing to participate after being informed of the study's purpose and procedures. Potential participants were excluded if they had a history of falls in the past three months or were diagnosed with cognitive impairment or mental disorders affecting consciousness, regardless of whether they were receiving treatment. The required sample size was estimated using G*Power (version 3.1.9.7) and Cohen's 34 equations, considering an effect size of 0.3 based on Bartholomaeus et al. 35 recommendation, a statistical power of 80%, and a significance level of 5% (α). The required sample size was preliminarily estimated as 52. It was then increased by 20% to account for potential withdrawal, resulting in a required sample size of 62. 36 As suggested by Marshall et al., 37 a sample size of 6 to 10 is typically adequate to achieve data saturation in phenomenological studies. Data collection will continue until redundancy is observed in the responses and no new information arise, ensuring data saturation.
Intervention
The intervention was developed through an expert review process. It was collaboratively designed by two doctoral candidates in nursing and four certified Level 2 fitness instructors. After the initial design, content validity was evaluated by four experts, including two professors of gerontology, one professor of rehabilitation medicine, and one practicing rehabilitation physician. The resulting Content Validity Index (CVI) was 0.92, which exceeds the acceptable threshold of 0.80, indicating high content validity. 38 Through incorporating the professional elements of physical therapy, nursing, and sports and health, the intervention included systematic aerobic and muscle strength training sessions that aligned with the needs of older adults. The training sessions lasted two hours and were held once weekly. The design of the exercise intervention is shown in Table 1.
Design of the exercise intervention.

The SMARC (Synchronized Monitoring Analyses Recording Cloud) intelligent exercise system is a medical-grade intelligent rehabilitation device composed of eight integrated training machines, designed to provide active exercise therapy for the upper limbs, core, and lower limbs. It is certified by the US FDA and EU TÜV, meeting international medical device safety and performance standards. SMARC incorporates AI-powered precision assessments to deliver customized exercise prescriptions tailored to each user's physiological parameters and health condition. Through high-end sensors, it continuously captures real-time data on muscle strength, joint angles, and movement patterns, providing immediate visual feedback to guide posture correction and improve training accuracy. Training intensity, frequency, and content are automatically adjusted by AI or manually fine-tuned by professionals to optimize outcomes. All training sessions are uploaded to a cloud platform, enabling healthcare providers or exercise specialists to monitor and analyze progress in real time. SMARC has been effectively applied to post-orthopedic surgery patients, older adults with sarcopenia, and elderly individuals requiring functional restoration or preventive decline management, demonstrating proven benefits in both clinical and long-term care settings. 39 The participants logged into the exercise system by swiping their ID cards. Then, based on a Plan–Do–Check–Action approach, Participants underwent a physical fitness assessment and a body composition analysis. Then, their exercise and health data were visualized. The fitness instructors provided them with plans that included warm-ups, cool-downs, and diverse exercises. The content was adjusted according to the learners’ progress and course demands. The AI-generated exercise prescriptions served as the foundation for individualized guidance, accounting for approximately 70% of the intervention structure. Instructors contributed the remaining 30% by making limited adjustments based on participants’ physical conditions, safety requirements, and motivational needs. These modifications were confined to intensity, pacing, and progression, ensuring that the program remained both personalized and consistent with the original protocol. Adherence to the weekly two-hour sessions was monitored through dual approaches: (1) attendance records maintained by the senior fitness club, and (2) usage logs automatically generated by the smart sports equipment, which captured exercise frequency, duration, and intensity. Each participant was expected to complete a total of 24 hours over the 12-week intervention. An adherence rate of ≥80% was defined as satisfactory. The design of the exercise intervention is presented in Table 1.
Measurement tools
In the first phase, quantitative data were collected using a structured questionnaire. The collected demographic data included age, sex, employment status, education, marital status, smoking status and drinking status. The participants’ resilience levels were assessed using the Chinese version of the Resilience Scale (CRS), 40 translated from the Brief Resilience Scale (BRS), developed by Smith et al., 41 to measure their psychological ability to bounce back from adversity or negative events. The CRS consists of six items; the odd-numbered items are positively worded (e.g., “I tend to bounce back quickly after hard times”), while the even-numbered items are negatively worded (e.g., “I tend to take a long time to get over setbacks in my life”). The items are rated on a five-point scale (1 = strongly disagree, 5 = strongly agree), with the negatively worded items scored in reverse. The total CRS score ranges from 6 to 30 points. The total score is calculated by summing all item scores, with a higher mean score as indicating greater resilience and vice versa. A score of ≥22 indicates high resilience, 14–21 indicates moderate resilience, and ≤13 indicates low resilience. Liu et al. 42 applied the CRS on community-dwelling older adults living with heart failure and reported that it has good reliability, with an internal consistency (Cronbach's α) of 0.96.
In the second phase of the study, all interview questions were specifically designed for participants in the intervention group, as the primary objective was to explore their experiences, perceptions, and responses to the digital health intervention. Since the control group did not receive the intervention, therefore not included in the interview process. Researchers created a semi-structured interview outline, based on the relevant literature and suggestions from field experts, to collect the qualitative data. The interview questions were as follows: (1) How did participating in the smart sports equipment intervention influence your physical activity level? (2) How did participating in the intervention influence or change your cognitive status (i.e., mood and memory)? (3) How did participating in the intervention influence your general purpose in life (i.e. psychological well-being and attitude toward life)? (4) Do you have any suggestions regarding the use of smart sports equipment?
Data collection and statistical analysis
The quantitative data were analyzed using the SPSS statistical software. The demographic data are described using numbers (percentages) and means (standard deviations). The mean resilience scores and pretest-posttest differences were compared between groups, using paired sample t-tests, using a 5% significance level.
A single trained interviewer conducted all interviews to ensure consistency when collecting the qualitative data. The interviews were conducted in quiet settings based on participants’ preferences. They were audio recorded and transcribed within 24 hours. Data saturation was determined through an iterative process of coding and thematic analysis. After each set of 3 interviews, the research team evaluated whether new categories or themes were emerging. Recruitment continued until no additional themes were identified in consecutive interviews, at which point data saturation was considered achieved.
The data were organized and analyzed using MAXQDA software. Its various automated functions, such as content search, data visualization, sorting and coding, data linking, and data mapping, replace manual reviews that require multiple readings. We followed Colaizzi's 43 descriptive phenomenological method during data processing. The procedure was as follows: (1) generating data or datasets, (2) coding the data (identifying events in codes and comparing them with the original and other codes), (3) categorizing the codes, and (4) forming a core concept.
Each step in the process is as follows: (1) Generating data or datasets: The interview text was transcribed, and the transcript was checked for missing or unclear data. If missing or unclear data were present, the participant was re-interviewed to verify the content's accuracy. All data were anonymized to ensure participant confidentiality. (2) Coding: Open coding was performed on the transcript to preliminarily name and categorize smaller chunks of data. (3) Categorizing: The preliminarily coded data were further categorized to establish meaningful connections with the theme structure. (4) Forming a core concept: The data analysis results were systematized to form a core concept. (5) Integrating and describing the findings: The findings of the phenomenon are collectively integrated and described. (6) Shaping the essence of the phenomenon: The fundamental meaning of the phenomenon was described. (7) Validating the findings from the participants: The participants reviewed the findings to ensure that their experiences had been portrayed accurately. 43
Qualitative rigor was assessed based on the four criteria proposed by Lincoln and Guba 44 : credibility, transferability, dependability, and confirmability. This process involved both coding frequency analysis and narrative synthesis. To ensure coding consistency and credibility, a double-coding process was conducted. Two researchers independently coded the same set of transcripts and discussed any discrepancies until consensus was reached, enhancing intercoder reliability. Inter-coder reliability was also calculated using Percentage agreement, which is appropriate for two coders and accounts for the possibility of agreement occurring by chance, thereby providing a quantitative assessment of reliability. For any discrepancies, the researchers first held consensus meetings to resolve differences. If consensus could not be reached, a third researcher with expertise in qualitative research was invited to arbitrate and finalize the coding to ensure objectivity and rigor. All codes and themes were then collaboratively reviewed and refined by the research team.
Rigorous process ensured that the coding structure accurately reflected the lived experiences of participants and increased the trustworthiness of the findings. To avoid researcher bias, the data were peer-reviewed by a researcher with at least 10 years of experience in conducting qualitative research. The trained interviewer was a third party unassociated with the research team and was tasked with conducting the interviews and analyzing the data. Using software to analyze the qualitative data also helps to minimize personal bias and achieve a consistent interpretation of the data. The interview outline, participant data, interview content, and data were recorded and reviewed on a computer. As such, rigor was maintained throughout this study.
Ethical considerations
This study was approved by an institutional review board (approval number: YM111099E) and funded by the National Science and Technology Council (program number: NSTC 111-2314-B-A49-013-MY3). All participants signed an informed consent form and could withdraw from the study at any time. The study data were kept confidential. All research procedures adhered to research ethics, and conducting the study at the senior fitness center posed no ethical concerns. The equipment and training services were provided by the Health Promotion Administration and Public Health Bureau of Hsinchu City.
Results
Quantitative analysis
A total of 69 participants were randomly assigned to an intervention group (n = 35) or a control group (n = 34). To ensure the validity of demographic variables across different groups. P-values > .05 indicating no significant differences among the groups and suggesting homogeneity. Their mean age was 71.54 years. Most were women (49/69, 71%), had graduated from a university (43/69, 62.4%), were married (57/69, 82.6%), were retired (48/69, 69.6%), and (66/69, 95.7%,68/69,98.6%)did not drink or smoke (Table 2).
Participants’ demographic data (N = 69).

*p < .05.
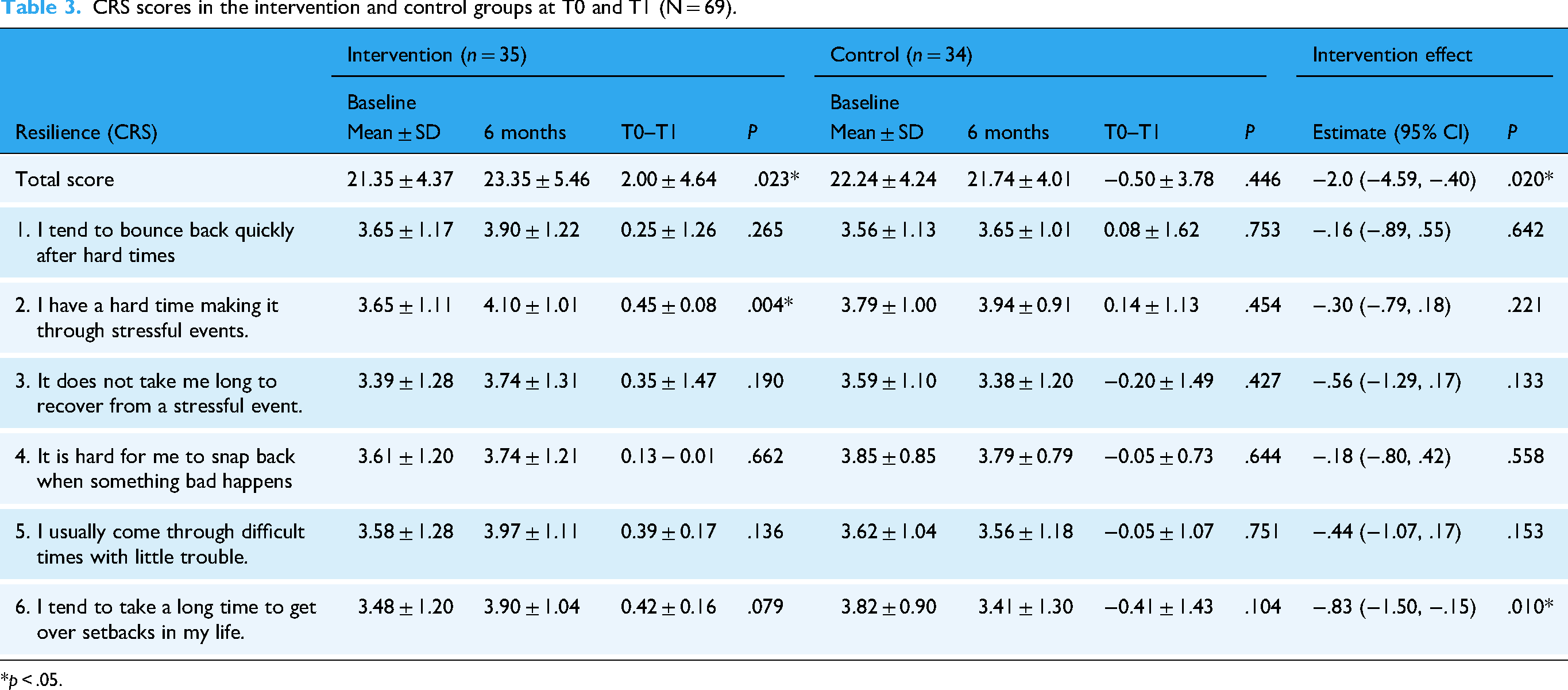
The changes in total CRS scores from baseline (T0) to six months (T1) did not differ significantly between the intervention and control groups. The intervention group showed a significant increase in CRS scores from baseline (21.35 ± 4.37) to six months (23.35 ± 5.46, P = .023), while the control group showed no significant change, demonstrating the positive effects of the intervention on enhancing resilience. In contrast, the total CRS scores did not change significantly from baseline (22.24 ± 4.24) to six months (21.74 ± 4.01) in the control group (P = .446). The between-group comparison showed a significant estimated effect on the intervention group, which was −2.0 (95% confidence interval [CI]: −4.59, −0.40, P = .02), indicating that the intervention significantly enhanced resilience. In summary, the intervention significantly affected the CRS scores in the intervention group (P = .02). The results are presented in Table 3. No items attained statistical significance, except Item 6 (the time to get over setbacks in life; P = .01). The number of comparisons was limited, and applying a Bonferroni correction might have been overly stringent, potentially leading to Type II errors (i.e. failing to detect true differences). Therefore, the correction was not applied.
CRS scores in the intervention and control groups at T0 and T1 (N = 69).
*p < .05.
Qualitative analysis
The demographic data of the 16 interviewees, all of whom were recruited from the intervention group, are shown in Table 4. Following an in-depth analysis and reflection, three themes emerged: (1) participants’ health as transitioning from adapting to internalizing digital technology, (2) participants’ experiencing exercises as aligned with their needs, and (3) fostering of close peer relationships. These findings underscore the older adults’ transition from adapting to intelligent exercise in the early stage and gradually integrating it into their daily lives.
Interviewee demographic data.

Participants’ health as transitioning from adapting to internalizing digital technology
In addition to being an intervention component in the intervention, smart sports equipment is a form of technology use, and over time, the exercises became more structured and targeted. The interviewees went from trying out intelligent exercises to incorporating them into their lives, improving their training outcomes, and feeling more confident in continuing to engage in intelligent exercises. Regular physical activity became a routine once they incorporated exercise into their daily life. Training outcomes included improved muscular strength, endurance, and balance, and the interviewees’ sense of control over their health.
From unfamiliarity to proactive integration
Using smart sports equipment became more than an activity completed during the intervention. The interviewees were initially unfamiliar with the smart equipment but gradually began to use it more often, experiencing its health benefits, particularly physical and spiritual changes. At first, I wasn’t used to using the smart sports equipment and thought that the procedure was complicated. Now I use it regularly every week. (C13) Incorporating the smart sports equipment enriched the course content, and now it is a habit of mine to use it. (D3) I try to use more types of smart sports equipment and maintain regular exercise, which is an excellent habit. (F11) When it comes to physical activity, I’m not a flexible person. But given the opportunity to use the equipment regularly definitely helps me to keep exercising. (M1) Exercise can be integrated into life. When I first participated in this course, I didn’t understand why smart sports equipment was necessary. I gradually understood that new technologies are intertwined with our lives. (P3)
Finding balance and sound sleep
Although the intervention occurred during the daytime, its effects were key to a good night's sleep. The interviewees felt physically revitalized after the intervention, fell asleep more easily, and slept more soundly at night, as if after a hard day's work. Their overall sleep quality improved. Every time during the week when I come here to take part in the course, I definitely sleep better later that night. Workout day, to me, is a time to adjust my body. I sleep better after doing physical exercise. (F13) I usually sleep for 6–77 hours, but I can get an additional 1–2 hours of sleep on workout day. The sleep quality is indeed better because I won’t wake up at night. (F4) After exercising, I always have a good night's sleep and wake up feeling reenergized. (K5) I normally sleep late, at around 11 or 12 at night. But after doing the exercises recently, I’ll feel tired at around 9 o’clock, and I’ll hit the sack. (M3) I fall asleep easily after exercising. The sleep quality is excellent, and I wake up the next day feeling fresh. (O6)
Improving chronic disease management and recovery skills
The interviewees noted how the smart sports equipment became a turning point for their engagement in physical recovery and health management. The fitness training yielded stable blood pressure, improvement in heart rate, and chronic pain relief and served as a proactive strategy for resisting physical decline and living with chronic conditions. Using the smart sports equipment improved my chronic condition. I still continue taking my medications without altering the dose, and my blood test parameters remain the same. (E6) Although you can’t eliminate your illness by using the smart sports equipment, doing so improves your body's ability to combat it. (G7) The shoulder press corrected my hunched shoulders and improved my body posture. I am also able to maintain my regular exercise habits. (J3) I have a heart condition; my heart rate soars to 140–150 bpm when exercising vigorously. After completing the course, I feel that my heart rate has decreased during exercise. (I1) I think my chronic conditions have improved. The blood test, hypertension, and hyperlipidemia reports have green-colored values [normal values], which means that my health has improved. (K6) My physical activity levels have changed for the better after completing the course. My blood pressure used to be 130–140 mmHg, but after exercising, it dropped to 120–130 mmHg. It has improved, but not so noticeably…. The weakest part of my body is my muscular endurance. I think I have improved it after completing the course. The balance trainer activated my bones and muscles and improved my balance. (L3) The instructor allowed us to use the smart sports equipment, which helped stabilize my blood pressure and improve my physical activity level. (N2) The physical activity outcomes are pretty decent. I used to suffer from chronic pain, but now the bouts of pain are shorter. (N6)
Advancing toward delayed aging
Exercising with smart sports equipment enabled the interviewees to maintain their physical functioning, slow their aging, and maintain their mobility and autonomy. This course basically represents good governance. The government subsidizes the use of smart sports equipment and allows me to realize the importance of delayed aging through exercise. (A16) The balance trainer is greater for training balance and reaction time. Older people like us have slower reactions and are susceptible to falls. The instructors here are astute and help us a lot by encouraging us to work out more. (G4) I don’t feel any improvements in my muscular strength after using the smart sports equipment, but it did delay the aging process. (G6) I managed to correct my hunched back after attending the course and gain a better posture. (J3) I enjoy using the squat machine the most. My legs feel better when I sit down. I used to overuse my legs. When I was 40 years old, the doctor told me to go for a knee replacement. I had mobility issues, and I couldn’t walk. But after attending the course for several sessions, I am able to walk for longer durations without using a knee brace. (I5)
Participants’ experiencing exercises as aligned with their needs
The real-time data records of the smart sports equipment enable users to better understand their fitness. The equipment should not only be an exercise tool but also should meet patients’ needs so that exercising is a “friendlier” process.
Accessing exercise performance results in real-time
Using the smart sports equipment gave the interviewees a better understanding of their physical fitness and allowed them to observe their physical changes, such as improved muscular strength and cardiorespiratory function, and to see the associated data. The smart sports equipment allows me to observe my heart rate and calories burned, and it also records my data. (A10) To me, the smart equipment is an excellent device for assessing mobility. After using the shoulder press, I understand better about my shoulder problem. (B1) The smart equipment keeps records based on your performance and personalizes your exercise status. (F10) The smart equipment has a calorie monitoring function that provides reference values for us to check whether we have improved our exercise performance. (G9) I think it's convenient to use the smart equipment. Based on the physiological parameters like heart rate and blood pressure, I can check whether my physical fitness has improved or not. (K7)
Developing equipment-user alignment
Despite its benefits, the interviewees believed that smart sports equipment should better align with users’ needs to make exercising more straightforward and user-friendly. The equipment interface should include easy-to-understand instructions so that the user is able to use it correctly. (B15) When the equipment detects that the user's force input has decreased, it should automatically adjust the load rather than increasing it. (J12) When powered up, the interface should first ask whether the user is a beginner. If they answer yes, it should launch a series of tutorials. Like what the frame displayed on the equipment means, how you should move the ball on the screen, and what moving means…. It should be like a game mode. (K16) I feel that the instructions on the smart equipment are a bit unclear. I don’t understand what different exercises represent. (M9)
Fostering of close peer relationships
In addition to improving physical fitness and mental health, the intervention significantly reduced the interviewees’ stress and negative emotions. It brought them joy and increased their confidence in themselves and control over their lives. The peer interactions throughout the intervention allowed them to build supportive emotional connections, which further mitigated their loneliness and anxiety.
Broadening meaningful social circles
The intervention fostered positive emotional bonds and well-being, including vitality and satisfaction with life. It provided opportunities for the interviewees to interact and share experiences, build solid social connections, and enrich their purpose in life. Regarding the mental health benefits, the exercise instructor guided us to interact with each other, which improved our moods. (A24) I honestly enjoy this course; it is relaxing, and I feel better when attending it. (N11) Attending the course is like going back to school. We feel younger and have improved well-being. (L10) I feel happier, and I am able to suppress my negative thoughts by interacting with others. I feel more at ease. (O11) Aside from feeling healthier physically, I also learned a lot of new things and enhanced my social bonds. I don’t feel alone because I have a group of friends whom I can talk with. (B12) There is a sense of rapport during the course. Everyone talks to one another and expresses concern. (D8) By getting along with these classmates, I improved my interpersonal interactions and learned how to communicate with unfamiliar people. (J6) After exercising, my interpersonal interactions have improved, from mental well-being to discussing our purpose in life. (K12) The team cohesion during the course improved my mood. I get to engage in physical activity and meet my friends every time I come here. (N9) I seldom participate in social activities in my daily life. This course allows me to communicate with the instructors and peers and connect with the world outside. (O9) By joining the senior fitness club activities, you are guaranteed to have a thirst for knowledge. You can learn how to plan your life after retirement and make it more meaningful. (P11)
Expanding the influence of health in communities
The interviewees emphasized the social benefits of smart sports equipment and exercise courses, especially in slowing aging and decreasing medical expenditures. They felt that the course should be broadened to a larger population of older adults and could be a strategy for rationally allocating national healthcare resources and exhibiting the value of public health. I don’t feel like there is a need to improve the smart equipment, but I think the implementer should market it more actively so that more people can benefit from it. (M9) Like the saying goes, prevention is better than cure, so promoting the course and slowing the aging process through exercise can help our country cut down on medical expenditures. (M9) The smart equipment made me a healthier person; it is awesome. (M9) We should introduce the course to a wider older adult audience. This course is very helpful. (M9) I feel that it is worth promoting this intelligent exercise course. (M9) The government should help popularize the use of smart sports equipment. (M9)
Discussion
This study adopted a mixed-methods approach to explore the effects of an intelligent exercise intervention on older adults. The quantitative results showed that the resilience of participants in the intervention group improved after participating in the intervention. The qualitative interviews further revealed three core concepts in older adults’ experiences of engaging in intelligent exercises: (1) participants’ health as transitioning from adapting to internalizing digital technology, (2) participants’ experiencing exercises as aligned with their needs, and (3) fostering of close peer relationships. These findings underscore the older adults’ transition from adapting to intelligent exercise in the early stage and gradually integrating it into their daily lives.
In addition to effectively improving older adults’ digital resilience, the intelligent exercise intervention fostered their adaptability and technology engagement. Our findings showed that the CRS scores of participants in the intervention group increased significantly from the pre-test to the post-test. Participating in intelligent exercises helped older adults to adapt to digital technologies, reduce their technology anxiety, and build their confidence in using smart equipment. After adapting to the smart sports equipment, the older adults internalized their technology usage behavior and reinforced their digital participation and intentions through social support. The establishment of digital resilience is a process of constant adaptation and learning. Consistent with Davis's 12 technology acceptance model, while adapting to smart sports equipment, older adults who perceived technology as useful and easy to use are more likely to use it in the long term. When using intelligent exercises, suitable support plans and opportunities for lifelong learning can effectively reduce thresholds in learning and fortify older adults’ digital confidence and adaptation. 12
The primary purpose of intelligent exercises is to help older adults to improve their health management skills by adapting to the exercises and then incorporating them into their daily lives. Our results showed that intelligent exercises improved older adults’ sleep quality, management of chronic conditions, and exercise maintenance, thereby delaying the onset of functional decline. 45 One barrier to older adults’ use of fitness apps or smart sports equipment is that many are unaccustomed to digital technologies, such as smartphones and wearables, and are, therefore, less willing to use such technologies. Providing appropriate learning resources and instructions can help them to develop regular exercise habits. 46 Further, smart sports equipment offers real-time data monitoring and feedback, enabling users to understand their health status in a straightforward manner. 12 In addition to fostering health management, smart sports equipment promotes safety during exercise, social interactions, and mental well-being and is particularly suitable for older adults and individuals with chronic conditions. The interviewees expressed that the intervention assisted them in building social connections and further enhancing their exercise maintenance through peer encouragement and support. Further, team courses foster interaction and mutual learning, meaning that exercise is no longer perceived as a solitary activity. The shared exercise experiences enriched the participants’ learning outcomes and increased their enjoyment and engagement during exercise.
Despite agreeing that intelligent exercises offer a wide range of benefits, most interviewees had a few concerns and offered suggestions for existing technologies and designs. For example, they felt that the equipment interfaces were too complex and not intuitive. Domingos et al. 47 identified ease of use and usability as the key factors in older adults’ use of digital and new technologies. Although data visualization in intelligent exercises enhances older adults’ understanding of exercise performance, due to their lack of data interpretation skills, they may rely excessively on equipment parameters when assessing exercise performance instead of focusing on their actual feelings and health status. Faverio 48 reported that users might even feel stressed for failing to achieve target values, decreasing their enjoyment of exercising, which could influence their intention to use smart sports equipment.
Using the smart equipment for several months and becoming familiar with it reduced the interviewees’ technology anxiety and improved their willingness to learn new technologies. This finding aligns with Anderson et al.'s 49 notion that older adults will increase their technology acceptance when they have greater demands. However, some studies argued that older adults are concerned about damaging expensive equipment due to improper use or failure to follow instructions. 50 Simple graphics or audio descriptions can help older adults to better understand how to use the equipment.
The Metaverse Equitable Rehabilitation Therapy (MERTH) Framework, proposed by Veras et al., outlines five critical domains—equity, health services integration, interoperability, governance, and humanization—which provide a comprehensive structure for evaluating digital interventions in aging populations. 51 In the context of smart sports equipment for older adults, this framework helps highlight not only functional and behavioral outcomes but also broader social and ethical considerations, such as digital inclusion and accessibility. For instance, the equity domain emphasizes the need to accommodate diverse abilities and digital literacy levels, which directly relates to the usability challenges reported by participants in this study. Personalization through AI and adaptive interfaces aligns with MERTH's humanization principle, ensuring that interventions respect older adults’ identities, autonomy, and cultural backgrounds. Furthermore, the interoperability and integration components encourage coordinated care and consistent digital engagement across platforms, contributing to sustained technology adoption. Future design and implementation of smart exercise systems could be enhanced by aligning with MERTH to support inclusive, ethical, and sustainable digital health solutions for older adults.
The interviewees also felt that the personalized functions could be further optimized. For example, one stated, “I enjoyed using the smart sports equipment, but my only concern is user discomfort caused by the equipment's height, which may not suit everyone,” while another stated, “The equipment should be able to automatically adjust the loading when its sensors detect the user is not exerting enough strength. I feel stressed when it continues to increase the loading instead.” Choudhary noted that AI can help to achieve safer and more efficient exercise by automatically adjusting the intensity based on the user's health status. 52
Health promotion through the integration of intelligent exercises and digital technologies is a key opportunity for healthy aging, a notion that has gained traction among government and social organizations, and smart sports equipment can serve as an important tool to help formulate public health policies. 53 Our results also revealed that intelligent exercises can be used as a medium to foster social connections. By leveraging the potential of smart sports equipment to expand social influence, policies could, for example, call for the integration of team challenges and online sports communities to motivate older adults to establish social support systems through their interactions. Consistent with Grey et al., 50 these programs have been shown to be effective. The government can offer digital adaptive training programs to help older adults integrate into intelligent exercise environments. The popularity and accessibility of intelligent exercises can be further promoted by combining community centers with healthcare institutions, which would contribute to the overall well-being of older adults.
Challenges in promoting intelligent exercises persist, including gaps in policy planning, older adults’ digital adaptation, and financial limitations-all of which affect the long-term feasibility of implementation. As learning motivation may decline over time, particularly among those unfamiliar with digital tools, 54 the promotion of intelligent exercise must extend beyond technology introduction to include the cultivation of digital resilience.
To align with the WHO 55 Digital Health Guidelines and advance digital health equity, we recommend prioritizing several feasible, evidence-supported strategies. First, community-based integration should be emphasized by installing intelligent exercise stations within local health centers or senior activity hubs, which increases accessibility and supports place-based health promotion. Second, adaptive digital training programs tailored to older adults’ learning pace and abilities should be embedded into public health systems to build confidence and self-efficacy. Third, low-cost access initiatives, including free trial programs, government subsidies, and equipment rental schemes, can significantly lower the entry threshold for economically disadvantaged older adults. In addition, offering structured exercise education and digital literacy resources can alleviate technology-related anxiety, enhance participation, and reduce the digital divide. Collectively, these strategies foster equitable access to smart health technologies and support the sustainable development of digitally inclusive, age-friendly communities.
This study has several limitations. First, participants were recruited through purposive sampling at the senior fitness club of a university in Northern Taiwan, which may have introduced selection bias and limited the generalizability of the findings. Although members were drawn from three administrative districts—East District, North District, and Xiangshan District—providing some degree of regional representativeness, the sample may not fully reflect older adults from other regions or those not regularly engaged in structured exercise programs. Second, group allocation was not randomized but based on institutional affiliation, which may have selection bias. To mitigate this, demographic characteristics and baseline data were included as covariates in the analyses, and statistical controls were applied. Future studies are recommended to recruit from multiple sites, adopt randomized designs, and include more diverse populations to enhance representativeness and external validity. Third, participants were self-selected and likely more motivated and health-conscious, introducing the possibility of selection bias. Third, Participants’ resilience was assessed using the Chinese Resilience Scale (CRS), Participants’ resilience was assessed using the Chinese Resilience Scale (CRS), though self-reports may involve response bias due to over- or underestimation. Future research should consider longitudinal designs to assess the sustained impact of intelligent exercise interventions, incorporate objective physiological measurements (e.g., muscle strength), and explore cross-cultural applications to examine contextual influences on digital resilience and technology adoption. Expanding to larger, more diverse populations and implementing randomized controlled trials would strengthen the evidence base for integrating smart sports equipment into community health promotion strategies.
Conclusion
Intelligent exercise represents a promising form of digital health intervention that can strengthen Digital resilience, enhance digital engagement, and promote healthy aging among older adults. To ensure sustained adoption, future developments should align with digital health equity principles by prioritizing user-centered design, improving usability, and addressing accessibility barriers. Intelligent exercise systems into broader digital health ecosystems such as community health centers, telehealth services, and personalized care platforms may further support long-term behavior change, reduce the digital divide, and empower older adults to take a more active role in their health management.
Footnotes
Contributorship
Hui-Chen Tsai: conceptualization, data curation, formal analysis, investigation, methodology, writing—original draft, and writing—review and editing; Ching-Wen Wei: conceptualization, data curation, methodology, writing—original draft, and writing—review and editing; Fong-Ping Tang: data curation, formal analysis, and methodology; Kuan-Yu Peng: investigation, methodology, and supervision; Heng-Hsin Tung: conceptualization, supervision, validation, and writing—review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Science and Technology Council (Project No. NSTC 111-2314-B-A49-013-MY3).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.