
Abstract
Aim
To summarise the facilitators and barriers influencing the utilisation of mobile health (mHealth) for rehabilitation among older adults with hip fractures, family caregivers, and healthcare providers.
Methods
A total of five databases (PubMed, Cochrane Library, Embase, Web of Science Core Collection, and Ovid) were searched from inception to July 2025. Additionally, grey literature and reference lists were also searched. Publications were eligible if they reported on facilitators or barriers influencing the utilisation of mHealth by older adults with hip fractures, family caregivers, or healthcare providers.
Results
Nine articles were included. Our findings indicated that the influencing factors included patient-related and mHealth technology-related factors. Both patients and family caregivers recognised mHealth's advantages in communication with healthcare providers, finding it useful and efficient, and effective in delivering rehabilitation instructions. Healthcare providers emphasised its value in delivering holistic care, providing health education, and facilitating patients and family caregivers’ engagement in disease management. However, patients and family caregivers reported both preferences for traditional healthcare models and functional limitations as key barriers. All groups jointly reported adoption barriers, including patients’ inadequate technical literacy, patients’ characteristics, lack of critical resources, as well as technology-related challenges concerning external constraints.
Conclusion
The study reveals the unique characteristics of older adults with hip fractures have constrained the deeper implementation of mHealth. Future research should target family caregivers and healthcare providers by systematically examining the critical factors influencing their use of mHealth in managing older adults with hip fractures. Such investigations would enhance the quality of clinical care, facilitate patient recovery, and improve prognostic outcomes.
Introduction
Mobile health (mHealth) is a subset of eHealth and is defined as ‘the use of mobile wireless technologies for health’, 1 providing more person-centred, available, accessible, and scalable tools. Compared with other digital health technologies, mHealth systematically integrates mobile communications, geospatial positioning, multi-modal sensors (e.g. motion, optical, and proximity sensors), and Bluetooth transmission to form a portable health monitoring system. These technologies are organically embedded in smartphones, applications, and wearable devices, overcoming the spatiotemporal limitations of traditional healthcare services while significantly improving the accessibility and scalability of medical services.2–4 Since the outbreak of COVID-19, the application of mHealth in the medical field has been increasing, 5 covering several aspects, including patient treatment and communication, health monitoring and management, health education and advocacy, data collection and research, and more. 6 The mHealth system enhanced patient self-monitoring, management, and confidence in recovery, 7 while also supporting family caregivers in balancing work and caregiving. It provided guidance for caregiving tasks and helped healthcare providers identify patient issues for improved decision-making and quality care.3,8 mHealth technologies have demonstrated significant clinical utility in the management of various speciality diseases and are currently widely used in the diagnosis, treatment, and care of diseases such as tumours and cardiovascular diseases.9,10
Hip fracture is a great universal public health challenge with high mortality and morbidity rates; its incidence rate increases significantly with age, 11 with the number expected to double by 2050. 12 mHealth interventions can enhance self-management capabilities in hip fracture patients, facilitate their smooth transition from hospital care to rehabilitation training and subsequently to home care, reduce the risk of hospital readmission, and positively influence patient prognosis.13,14 Furthermore, rehabilitation interventions utilising mHealth technologies demonstrate beneficial effects on postoperative recovery in older adults with hip fractures. These interventions not only improve patient compliance with rehabilitation regimens and promote functional recovery but also contribute to psychological well-being and reduce complication risks.15,16 Prieto-Moreno et al. 17 developed an application named ActiveHip + mHealth specifically designed for older adults with hip fractures. The intervention improved patients’ physical function and alleviated anxiety and pain symptoms, though no significant effects were observed regarding depressive symptoms, fear of falling, or quality of life. Therefore, it is imperative to investigate how mHealth technologies can comprehensively improve both physical and psychological functions as well as the quality of life in older adults with hip fractures.
Previous studies have demonstrated that the utilisation of mHealth technologies among older adults is jointly influenced by technological and personal factors.18–21 Specifically, at the technological level, system complexity, data privacy concerns, and issues related to device accessibility and network coverage diminish user adherence, whereas robust technical support systems along with personalised and age-adaptive feature designs significantly improve acceptance rates.18,19 At the personal level, age-related cognitive and physical decline, limited health literacy, and a lack of knowledge, skills, or confidence in using mHealth technologies collectively constitute primary barriers to adoption, while learning motivation and previous positive experiences enhance engagement.20,21 Notably, hip fracture patients exhibit distinct clinical needs due to concurrent musculoskeletal impairment and geriatric complexity, necessitating tailored mHealth solutions. 22 In addition to individual and technological considerations, mHealth for older adults with hip fractures must account for two crucial support systems. Research confirmed the indispensable role of family caregivers in the rehabilitation process, where their involvement has been shown to enhance physical functional recovery, improve health-related quality of life, and significantly reduce hospital readmission rates.23,24 The provision of targeted communication and educational solutions by healthcare providers through mHealth technologies, with content encompassing essential post-fracture guidance such as anti-osteoporosis treatment and fall prevention, has been demonstrated to significantly improve patient adherence and treatment continuity, thus effectively mitigating refracture risk. 22 In this context, the active participation of family caregivers and healthcare providers may become an important factor in enhancing patients’ compliance with mHealth treatments. Technology acceptance model (TAM) served as a theoretical framework for this study, providing a structured approach to identify and measure determinants influencing users’ adoption and utilisation of mHealth technologies. 25 As a validated instrument for assessing technology acceptance, TAM has been extensively applied in medical research.26–28 To the best of our knowledge, there has been no systematic review that synthesises the evidence on the facilitators and barriers of mHealth for older adults with hip fractures. This study aimed to identify the facilitators and barriers to implementing mHealth for older adults with hip fractures, family caregivers, and healthcare providers to inform better mHealth interventions in the future.
Methods
The review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 29 The study protocol had been registered in PROSPERO (CRD420251110065). Our study did not require ethics committee approval, as it involved neither animal nor human clinical trials nor any unethical procedures.
The theoretical framework guiding this study is TAM, which serves as a robust tool for understanding technology adoption and has been extensively applied in healthcare research. 25 As an extension of the theory of reasoned action, TAM incorporates several key constructs: perceived usefulness, perceived ease of use, attitudes, and behavioural intention. Among these, perceived usefulness (the degree to which a person believes using the system would enhance their performance) and perceived ease of use (the degree to which a person believes using the system would be free of effort) emerge as the two most critical determinants influencing adoption intention in healthcare contexts. 30 Therefore, guided by the framework, we derived our analytical framework from its two foundational constructs, namely perceived usefulness and perceived ease of use. This theory provided a systematic basis for categorising influencing factors during data analysis, ensuring structural alignment with established theories.
Search methods
Two independent researchers developed a preliminary search strategy, which was then piloted on PubMed. Continuous modifications were made to refine the search strategy. In July 2025, a comprehensive search of the following five databases: PubMed, Embase, Web of Science Core Collection, The Cochrane Library, Ovid, Scopus, and ProQuest Dissertations & Theses Global (PQDT Global) was conducted to look for peer-reviewed articles and grey literature from inception to July 2025. Additionally, we also manually searched the reference lists of all included studies.
For each database requirement, we tailored our search strategy using the following search terms and descriptors: hip fracture (Hip fracture* OR Brittle hip fracture OR Fragility hip fracture OR Femoral neck fracture* OR Intertrochanteric Fracture* OR Subtrochanteric Fracture*), mobile health (Telemedicine OR mobile applications OR digital health OR videoconferencing), facilitator and barrier (Barrier OR Facilitator OR Enabler OR Health Knowledge, Attitudes, Practice OR attitude to health OR Perception OR Knowledge OR Health literacy OR Attitude OR Public Opinion OR Awareness). To ensure the comprehensiveness of the literature search, additional term combinations related to the concept were included. The search strategy for each database is accessible in Appendix 1 to ensure transparency and replicability.
Inclusion and exclusion criteria
Detailed inclusion and exclusion criteria followed the PICOS framework: (1) Participants: older adults with hip fractures, family caregivers, or healthcare providers; (2) Intervention: mHealth technologies for rehabilitation (e.g. applications, remote monitoring, wearable devices); (3) Comparison (if applicable): usual care (conventional rehabilitation); (4) Outcomes: perceived barriers and facilitators to use mHealth in general or one aspect of mHealth; (5) Study design: qualitative, quantitative, or mixed-method studies published in English were considered. Studies that solely focused on technical development or evaluated technical effectiveness/feasibility without assessing user acceptance were excluded.
Search outcomes
The process entailed the collaboration of two authors. Initially, all literature retrieved from databases was imported into NoteExpress 4.0 for deduplication. Two independent authors (JS and BYY) screened titles and abstracts based on eligibility criteria. Subsequently, they independently assessed the full-text papers to determine which studies were included. Any discrepancies during this process were resolved through discussion between the two authors until a consensus was reached, or, if necessary, through arbitration by a third researcher.
Quality appraisal
We used the Critical Appraisal Skills Programme Qualitative Research Checklist 31 for qualitative studies, the Quality Assessment Tool for quantitative studies, and the Mixed Methods Appraisal Tool version 2011 for mixed-methods studies. 32 All included studies were assessed independently by authors (JS and BYY). Any ambiguities or discrepancies related to quality assessment were discussed and resolved between the two researchers and, if necessary, by a third author.
Data extraction
A data extraction form was used to extract data, which included authors, country, study design, setting, sample size, data collection, and analysis methods. Data extraction was completed by two researchers and reviewed by a third researcher. The associated factors were classified into barriers (−) and facilitators (+) for the use of mHealth. Any disagreements were resolved through discussion or by a third party. In addition, during data extraction, when identical influencing factors were reported across patient, family caregiver, and healthcare provider groups, only the most representative original statement was retained as the evidence source for each factor. This approach prevented redundant extraction and presentation of repeated reports from different stakeholder groups, thereby ensuring comprehensive coverage of all key factors while avoiding evidence redundancy from multiple reporting.
Data synthesis
To better address our research questions, we analysed the qualitative components from each study type that could answer our research questions. The qualitative study was selected for its unique ability to explore the lived experiences, perceptions, and acceptance of mHealth rehabilitation among older hip fracture patients, family caregivers, and healthcare providers. This approach provides in-depth, first-person insights into both the barriers and facilitators of implementing mHealth in clinical rehabilitation practice. 33
Thematic synthesis has been widely used in qualitative evidence synthesis. It was employed as it optimally synthesises qualitative evidence while maintaining contextual richness, particularly valuable given the limited studies directly addressing mHealth implementation in hip fracture rehabilitation. This method enabled inductive analysis of participants’ perspectives across studies to derive fundamental barriers and facilitators, ultimately generating novel insights that transcend individual study findings while respecting original contexts. 34
Thematic synthesis consisted of three stages: line-by-line coding of the findings of primary studies, the organisation of free codes into descriptive themes, and the development of analytical themes. 34 First, two authors (JS and BYY) familiarised themselves with the abstract, results, conclusions, and discussion sections of each study and applied line-by-line coding of the findings of primary studies. Then, descriptive themes were grouped by codes that were agreed upon by the two authors. Lastly, analytical themes were created from the descriptive themes based on the understanding and identification of new insights from the synthesised data. 35 Factors reported were classified as either barrier or facilitator factors, irrespective of the reporting party, and duplicate factors were not classified twice. To ensure methodological rigour, each stage was reviewed by another author (LLP). Because we only included qualitative studies, we were unable to standardise summary measures as would be performed in a meta-analysis. Appendix 2 presents the complete thematic synthesis process in detail.
Results
Search results and study selection
The search strategy resulted in 1548 studies. Thirty-two articles were obtained after removing duplicates and screening the titles and abstracts. Then, the full texts of 32 articles were reviewed based on the eligibility criteria, and finally, nine eligible studies published between 2019 and 2024 were included, comprising six qualitative studies, two mixed-methods studies, and one quantitative study. Additionally, 23 studies were excluded due to reasons presented in Figure 1.

PRISMA flow diagram. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics
The characteristics of the included studies were detailed in Appendix 1. The total sample size was 217 participants, consisting of 77 patients, 106 family caregivers, and 34 healthcare providers. The patients were older adults who had undergone hip fracture surgery. The included studies were conducted across multiple countries, with three studies from Spain,36–38 two from Denmark,39,40 and one each from China, 41 Canada, 42 Australia, 43 and the United Kingdom. 44 The studies were implemented separately at home (n = 3)38,39,41 and in hospital (n = 2),36,44 hospital and home (n = 2),37,40 hospital and geriatric rehabilitation service (n = 1), 42 and not reported (n = 1). 43 Data was collected using various methods, including semi-structured interviews, structured interviews, focus groups, in-depth interviews, and follow-up records. The data analysis method involved content analysis, thematic analysis, a systematic six-step approach, and an immersion–crystallisation technique. The included studies can be categorised into two groups: (1) pre-implementation studies: three qualitative studies36,42,43 systematically explored patients, family caregivers, and healthcare providers’ acceptance levels, willingness to adopt, and potential concerns regarding the application of mHealth technologies; and (2) post-implementation studies: six studies37–41,44 focused on evaluating patients’ and their family caregivers’ user experiences and technology acceptance during actual mHealth technologies utilisation.
Critical appraisal
The critical appraisal results of the included studies are summarised in Appendix 1. After the two researchers discussed critical appraisal results, no studies were excluded.
Main findings
Two primary factors were identified: (1) patient-related factors and (2) mHealth technology-related factors. The systematic categorisation of specific themes and subthemes is presented in Table 1, along with the frequencies of reported main themes across stakeholder groups (patients, family caregivers, and healthcare providers).
Themes, subthemes, and frequencies among stakeholder groups.
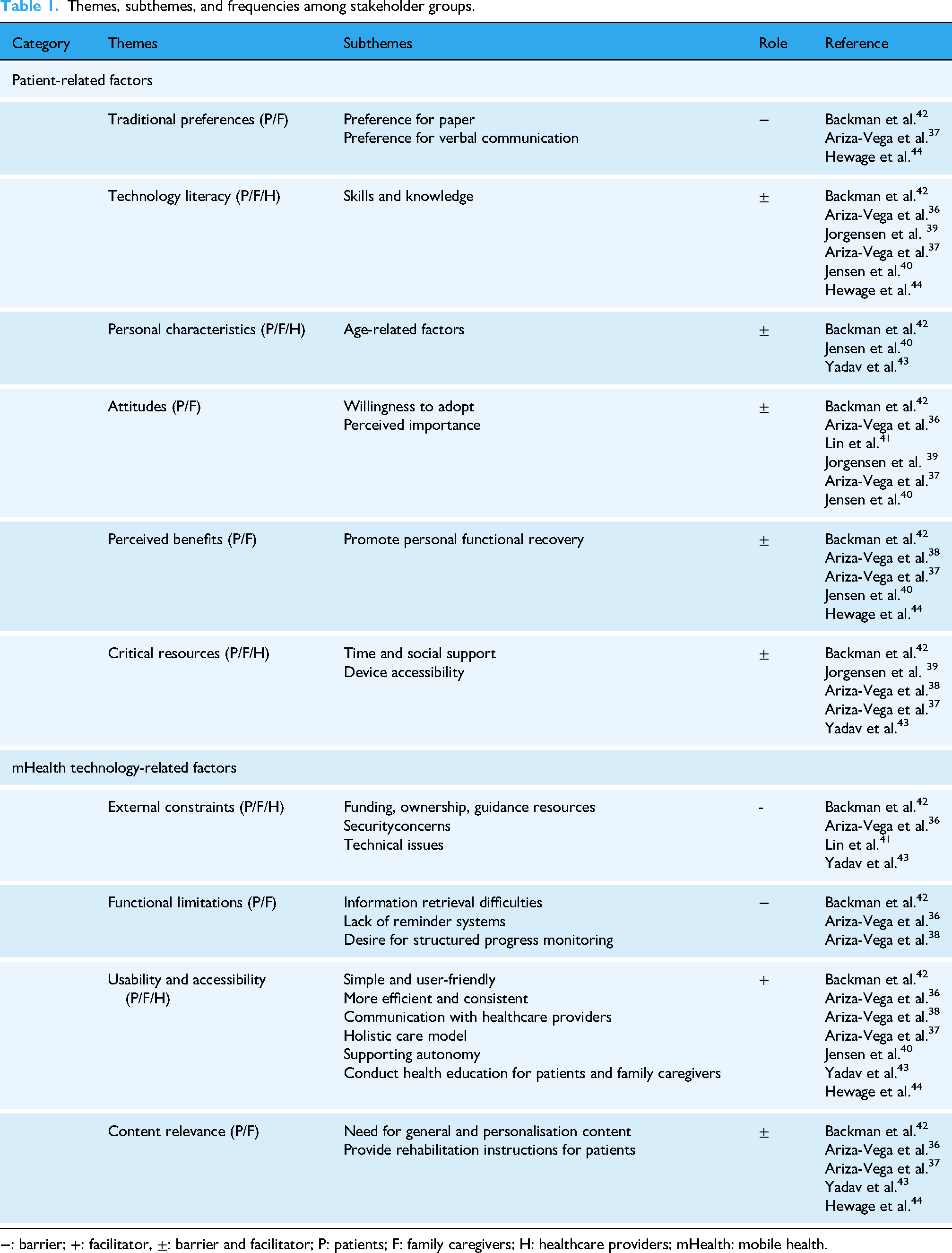
−: barrier; +: facilitator, ±: barrier and facilitator; P: patients; F: family caregivers; H: healthcare providers; mHealth: mobile health.
Patient-related factors
The study identified traditional preferences as significant barriers to mHealth adoption among older adults with hip fractures and their family caregivers. Patients and family caregivers demonstrated a marked preference for conventional healthcare approaches,37,42,44 particularly in-person rehabilitation guidance and paper-based educational materials.
A substantial proportion of the identified factors demonstrated dual potential as both facilitators and barriers to mHealth adoption. These included patients’ technology literacy36,37,39,40,42,44 and personal characteristics,40,42,43 attitudes towards mHealth utilisation,36,37,39–42 perceived benefits,37,38,40,42–44 and critical resources.37–39,42,43 Both patients and family caregivers reported that insufficient technological literacy – characterised by limited relevant knowledge,37,39,40,44 inadequate operational skills,36,37,39,42,44 and lack of prior experience with technologies 42 – posed significant adoption barriers among older adults with hip fractures. However, healthcare providers noted interindividual variability in technological competence within this population. 36 While patients and family caregivers acknowledged that age-related factors (e.g. cognitive decline, frailty, and comorbidities) could impede mHealth use,40,42 healthcare providers observed that some patients successfully overcame these physiological limitations. 43 In terms of attitudes, patients and family caregivers exhibited divergent attitudes levels towards mHealth – some expressed interest and trust in its ability to aid recovery, 42 while others remained hesitant.36,37,39–41 Notably, the majority of patients and their family caregivers reported that despite their willingness to adopt mHealth technologies, the lack of technical equipment significantly hindered their practical application.38,41–43 In terms of perceived benefits, the study revealed a cognitive divergence between patients and family caregivers regarding mHealth's efficacy in facilitating functional recovery. In contrast to patients’ generally positive perceptions,40,42,44 some family caregivers remained unconvinced of mHealth's efficacy in promoting functional recovery in patients.37,38 Similarly, though time constraints were reported by patients who prioritised competing responsibilities,37,39,42 this barrier was not universally experienced. 42 From the perspective of social support, family caregivers’ involvement and guidance enhanced patients’ willingness to adopt the technology, 42 particularly by providing timely assistance when operational difficulties arose. Nevertheless, healthcare providers emphasised that not all patients received consistent family caregivers support for mHealth use. 43
mHealth technology-related factors
Both patients, family caregivers, and healthcare providers consistently identified external constraints36,41–43 as significant barriers to the adoption and utilisation of mHealth technologies. Specifically, the lack of guidance resources,36,42 concerns over data security,42,43 and technical issues41,43 such as system instability have significantly affected the willingness to use technology. Healthcare providers particularly pointed out two key issues: the unclear responsibility subject for technical training and the absence of a support mechanism for clinical practice change. 43 It is worth noting that healthcare providers pay attention not only to common privacy concerns, but also to economic factors such as finance and technology ownership, which presented significant barriers to sustained use of this technology. 43 In addition, the functional limitations36,38,42 reported by patients and family caregivers are mainly manifested as difficulties in information retrieval 42 and the absence of reminder and monitoring systems,36,38 which compromised both the accuracy of patient data obtained by medical teams and the user experience.
The facilitators reported by patients, family caregivers, and healthcare providers were predominantly associated with the intrinsic characteristics of mHealth technologies.36–38,40,42–44 Specifically, the ability to communicate with healthcare providers,42,43 efficiency and consistency,36–38,42 and enhanced patient autonomy in disease management40,43 collectively constituted key factors attracting patients and family caregivers to use mHealth. Although additional time investment was required during usage, family caregivers generally perceived this as not increasing their burden. 37 Healthcare providers reported that this technology enhanced patient education, enabling both patients and their family caregivers to better participate in disease management. 43 In addition, healthcare providers emphasised that mHealth allowed them to deliver comprehensive care that extended beyond hip fracture treatment and rehabilitation, enabling holistic management of various health issues and facilitating the formation of an integrated healthcare team. 43
In terms of content relevance, both patients and family caregivers reported that mHealth technologies can provide rehabilitation-related information. However, the degree of information matching exerts a dual effect: when the content aligns well with individual needs, it significantly enhances users’ willingness to engage with the technology37,42; conversely, mismatched information reduces participation.36,42,43
Discussion
This study systematically investigated the application of mHealth technologies in the rehabilitation of older adults with hip fractures, based on the theoretical framework of TAM. The findings revealed that mHealth adoption and usage behaviours are primarily influenced by the dynamic interaction between ‘patient-related factors’ and ‘mHealth technology-related factors’, which align with the core constructs of TAM. Specifically, the perceived usefulness (e.g. rehabilitation efficacy improvement) and perceived ease of use (including operational simplicity, enhanced sense of disease control, and content relevance) among patients, family caregivers, and healthcare providers directly determine their behavioural intention to adopt mHealth. Notably, this study identified critical factors not fully captured by the framework. At the patient level, these included technology literacy, traditional healthcare preferences, and access to critical resources. At the technological level, these included functional limitations and external factors. These findings suggested that when applying the TAM to older adults with hip fractures, model adaptations accounting for population-specific characteristics are warranted. The results not only validate the applicability of TAM in the mHealth domain but also provide a theoretical foundation for optimising mHealth interventions for hip fracture rehabilitation, offering crucial insights for ensuring effective implementation and long-term sustainability of these technologies.
Findings from this study revealed that barriers to mHealth technologies adoption primarily stem from two dimensions: at the individual level, both patients and family caregivers demonstrated a persistent preference for traditional medical care models37,42,44; and at the technological level, functional limitations and external constraints of the technologies themselves posed significant adoption barriers.36,38,41–43 These barriers have been documented in existing literature as common challenges faced by older patients.18–21 Although systematic review evidence demonstrated that digital health technologies can effectively improve functional outcomes in older adults following hip fracture surgery, 14 this study found that this population still prefers traditional rehabilitation models. This preference may stem from older patients’ general hesitancy towards adopting new technologies due to their familiarity with alternative disease management methods and their perception of these devices as non-essential. 45 Patients and family caregivers reported functional limitations in the technology, which is consistent with previous research findings. 46 Studies demonstrated that comprehensive functional modules (such as medication reminders, rehabilitation progress tracking, etc.) can significantly improve users’ adherence to technology use.47,48 In addition, research indicated that over 75% of older users require external assistance to operate smart devices such as smartphones or tablets. 49 This finding demonstrated that inadequate instructional support reflected users’ difficulties in both usability and perceived usefulness. 50 Similarly, studies focusing on older adults with heart failure revealed their willingness to adopt mHealth for disease management when provided with sufficient training. 51 Consequently, these findings demonstrate the necessity for ongoing development of multifunctional systems to address user requirements, development of the personalised and easily comprehensible training programmes, and ensuring of robust data privacy protection and establishing responsive technical support frameworks.
The ActiveHip + mHealth system, specifically developed by Prieto-Moreno et al. 17 for older adults with hip fracture rehabilitation and implemented in Spain and Belgium, has shown effectiveness in improving objectively measured physical performance and reducing anxiety and pain. However, it appeared to have no significant effects on functional status, depression, fear of falling, or quality of life. Notably, none of these effects persisted beyond 1 year post-surgery, suggesting that a 3-month intervention may be insufficient to promote lasting behavioural changes. This underscored the chronic nature of hip fracture recovery, where the optimised design, accessibility, and usability of mHealth solutions directly influence long-term user adherence. The study also highlighted the necessity of family caregiver support to overcome patients’ lack of technical skills, while noting that current research in this field excludes older adults who have hip fractures and cognitive impairment – a finding consistent with our study results. Given the high prevalence of cognitive impairment among older adults with hip fractures, the special needs of this subgroup cannot be overlooked. Future research should explore family caregiver-centred intervention strategies to gradually transform their current auxiliary role into a more central position in the care paradigm.
Lower technological literacy among older adults with hip fractures (e.g. lack of relevant knowledge and skills) constituted another barrier to mHealth adoption. While it is commonly assumed that this technological deficiency correlates with advanced age, and previous studies have indeed confirmed the association between age-related cognitive decline and interface navigation difficulties, 50 our study similarly found that older age, memory impairment, and frailty hindered mHealth utilisation. However, this investigation also revealed significant individual variability in technological literacy, with some older patients demonstrating remarkable adaptability – a finding consistent with prior research showing no significant correlation between advancing age and technology adoption. 52 This heterogeneity may stem from differences between age subgroups and within-age-group variations, reflecting the individualised nature of ageing processes and disease progression. 52 Particularly among older adults with hip fractures – a population with considerable age diversity – attitude differences towards mHealth across age strata require further investigation. Consequently, clinical implementation should adopt stratified training strategies, tailoring interventions according to individual technological proficiency and physiological status. Furthermore, some patients exhibited disinterest in mHealth technologies and lacked confidence in their ability to utilise it for functional recovery, aligning with previous findings of low user trust in application usability. 50 These results suggested that future interventions should employ a sequential approach: first addressing attitudinal acceptance before facilitating behavioural change, prioritising the resolution of cognitive barriers to adoption.
This study found that facilitators primarily concentrated on technological features (e.g. enabling communication with healthcare providers and patient empowerment). These findings aligned with mHealth research conclusions in other fields,53,54 confirming its core value in improving health outcomes through technological empowerment. Notably, while only a few studies reported mHealth's capacity to empower patients, this finding showed high consistency with previous research, indicating that when patients acquired disease knowledge through mHealth, it enhanced their self-management responsibility, thereby improving technology adherence. 55 However, controversy remains regarding whether mHealth can provide personalised information guidance and improve functional recovery. Current studies have demonstrated that physical therapist-led mHealth interventions showed significant effectiveness in rehabilitation for older adults with hip fractures, 14 but more high-quality studies are still needed to confirm the efficacy of mHealth-assisted rehabilitation for this population.
Family caregivers and healthcare providers reported fewer barriers and facilitators regarding their use of mHealth. However, this study found that family caregivers were willing to use mHealth as it did not increase their burden. The ActiveHip+ study showed that mHealth intervention significantly reduced caregiver burden and depression after 3 months. 17 This suggested that future research should pay more attention to the role of this group in patient rehabilitation systems. It is recommended that future studies place greater emphasis on the role of family caregivers and provide them with corresponding care knowledge to promote comprehensive patient recovery. Healthcare providers emphasised the critical importance of technical training systems and policy support. Previous research indicated that healthcare providers considered official approval from national health service systems as a key facilitator for adopting digital health technologies, highlighting the importance of institutional support for technology implementation. 56 Therefore, it is advised to identify relevant training providers and establish supportive policies to promote standardised and systematic technology adoption. Furthermore, mHealth enabled healthcare providers to deliver holistic care, increasing their willingness to use it. This is particularly important for older adults with hip fractures who often have multiple comorbidities. mHealth has the potential to provide interdisciplinary integrated care for these patients, optimising medical resource allocation and reducing healthcare costs. However, current applications remain limited to single domains such as physical therapy, failing to fully realise mHealth's potential in comprehensive care. 57 Consequently, there is a need to further develop mHealth applications in multiple dimensions, including comorbidity management and medication guidance to bridge the gap between clinical practice and mHealth interventions.
Limitations
There are some limitations in this review. First, the restricted number of included studies with moderate sample sizes may increase the risk of publication bias, as older adults with hip fractures decline participation or withdraw from studies due to their compromised physical condition and disease burden. Second, the predominance of studies conducted in Western countries (with only one study from China) may limit the generalisability of findings to older adults with hip fractures from diverse cultural backgrounds. Furthermore, although this review synthesised barriers and facilitators from three stakeholder perspectives (patients, family caregivers, and healthcare providers), the available evidence primarily presents feedback from patients and family caregivers, with relatively scarce research data specifically focusing on healthcare providers.
Conclusion
The findings demonstrate that the application of mHealth technologies for rehabilitation in older adults with hip fractures is dually influenced by individual patient factors and technological characteristics. The distinctive physiological vulnerability of this population, coupled with the technical complexity, may constrain the adoption of mHealth for self-managed rehabilitation. Therefore, a critical research priority lies in translating technological advantages into viable solutions. Future work should focus on ensuring that these solutions are accessible and effective for older adults with hip fractures across diverse age groups, comorbidity profiles, and stakeholder networks.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251382826 - Supplemental material for Facilitators and barriers to mobile health adoption among older adults with hip fractures: A systematic review
Supplemental material, sj-docx-1-dhj-10.1177_20552076251382826 for Facilitators and barriers to mobile health adoption among older adults with hip fractures: A systematic review by Jian Song, Binyu Yang, Mayur Desai, Zirong Tao and Lingli Peng in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251382826 - Supplemental material for Facilitators and barriers to mobile health adoption among older adults with hip fractures: A systematic review
Supplemental material, sj-docx-2-dhj-10.1177_20552076251382826 for Facilitators and barriers to mobile health adoption among older adults with hip fractures: A systematic review by Jian Song, Binyu Yang, Mayur Desai, Zirong Tao and Lingli Peng in DIGITAL HEALTH
Footnotes
Informed consent
This study constitutes a systematic review that involves secondary analysis of published literature data without direct contact with or intervention in human subjects. It complies with the ethical waiver criteria for systematic reviews as stipulated by the Declaration of Helsinki and the International Committee of Medical Journal Editors (ICMJE).
Author contributions
JS, BYY, LLP, and ZRT: made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data. JS, BYY, LLP and ZRT: involved in drafting the manuscript or revising it critically for important intellectual content. JS, BYY, MD, LLP, and ZRT: given final approval of the version to be published. Each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content. JS, LLP, and ZRT: agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Yale Li Foundation Faculty Grant Program, 2024LFG01 and Yale-China Association 2023 Chia Community Health Services Program, 2023YC02.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.