
Abstract
Purpose
Family involvement in Coordinated Specialty Care (CSC) can enhance engagement and improve outcomes for young people with First Episode Psychosis (FEP). Digital interventions can circumvent many of the access and resource barriers that prevent families from engaging. The purpose of the current study was to better understand the experiences and challenges faced by caregivers who support a young person with FEP in the United States, and to use this information to guide the adaptation and further development of a digital intervention to support caregiver health and well-being.
Methods
Participants engaged in interviews and focus groups centered on their experiences supporting an adult child with FEP, connecting their relative to CSC, and their preferences for a digital intervention to support caregivers. This study used content analysis to develop themes and subthemes across interview and focus group data.
Results
Eight participants participated in the interviews and focus groups. Our findings support prior research indicating caregivers of young people with psychosis need evidence-based information about psychosis and assistance in managing systemic, social, and intrapersonal challenges. Participants advocated for a program with multimedia that could be accessed anywhere and anytime, facilitated connections with other caregivers, and emphasized messages of hope and recovery.
Conclusion
Interventions aiming to promote mental health and well-being for FEP caregivers in the United States should incorporate evidence-based information about psychosis specific to caregivers and their relative's recovery stage, guidance for navigating the healthcare system and privacy laws, and actionable skills related to illness management, effective communication, and self-care.
Keywords
Author summary
Family involvement in Coordinated Specialty Care (CSC) can significantly enhance engagement and improve treatment outcomes for persons experiencing First Episode Psychosis (FEP). Digital interventions can help overcome barriers that often hinder family participation in services. This study used content analysis to explore the experiences and challenges of caregivers supporting a relative with FEP in the United States. Analysis of eight individual interviews and two focus groups revealed caregivers’ need for evidence-based information about psychosis, support for managing challenges specific to their caregiver role, and access to resources emphasizing hope and recovery. Participants highlighted the value of a program that integrates practical guidance from others, interactive and accessible content, and connections with other caregivers. The goal is to use this information to adapt, expand, and further develop a digital tool to promote caregiver well-being. By addressing these needs, our work seeks to make mental health care more inclusive, accessible, and supportive for families supporting a young person with FEP.
Introduction
Approximately 3% of Americans will experience a psychotic episode in their lifetime.1,2 The peak age of onset of a primary psychotic disorder in the United States is 20.5 years. 3 Considering the developmental stage at which most people first experience psychosis, families can be a major source of support and stability.4,5 Families are often the first to notice early signs of psychosis and can be instrumental in connecting their relatives to Coordinated Specialty Care (CSC), the gold standard of First Episode Psychosis (FEP) treatment in the United States.6,7 Coordinated Specialty Care emphasizes early intervention and utilizes a multicomponent, team-based approach to maximize recovery.8,9
Active family involvement is a central component of early psychosis treatment and significantly improves engagement and outcomes.10,11 Family interventions in psychosis (FIPs) are associated with lower rates of relapse, shorter inpatient hospitalizations, reduced psychotic symptoms, and improved functioning.12–14 The FIPs can also significantly improve caregivers’ mental health and well-being and reduce expressed emotion in the family system. 14 Despite the benefits, less than 2% of families supporting a relative with Serious Mental Illness (SMI) have received a family-focused intervention.15,16
To begin to address this issue, Gleeson and colleagues developed a Moderated Online Social Therapy (MOST) program called Altitudes. 17 Altitudes blends evidence-based therapy skills and psychoeducation about psychosis with social support from clinicians and caregiver peers. Specifically, Altitudes provides continuous access to therapy content (called “Journeys”) and facilitates communication and resource-sharing among caregivers through a moderated forum (called the “Community”). 18 The program also includes guidance from family peer workers who provide encouragement and support on the platform, and clinical moderators who monitor content for appropriate use and facilitate individualized coaching calls. 19
Findings from randomized controlled trials in Australia suggest Altitudes is feasible and active engagement in the program is associated with reduced stress and increased social support among caregivers and fewer emergency room visits for the young person.18,19 We are interested in adapting, further developing, and tailoring Altitudes for FEP caregivers in the United States. Although there are similarities between Australia and the United States in that they are English-speaking and culturally, ethnically, and geographically diverse, there are significant sociopolitical and institutional differences that may impact treatment adoption and efficacy. 20 Most notably, whereas the United States has a complicated combination of private and public insurance, the universal healthcare plan is the main source of payment for mental and physical health services in Australia. 21 Furthermore, there are important legislative differences between the United States and Australia that impact the roles, responsibilities, and rights of family members who support a relative in mental health treatment (e.g., Health Insurance Portability and Accountability Act [HIPAA] vs. Queensland Mental Health Act of 2016 and Victoria Mental Health and Wellbeing Act 2022).22–24
To explore experiences, challenges, and needs specific to American caregivers, we conducted qualitative interviews and focus groups with parents whose family members were engaged in CSC for FEP in North Carolina (NC). We sought to determine their preferences for a digital intervention specifically designed to support caregivers of young people early in the course of psychotic illness in an American context. By gaining insights from those at the forefront of caregiving in the United States, we aim to inform the adaptation and enhancement of the Altitudes program with the hope of evaluating the impact of this targeted digital intervention on burden and social support for American caregivers in the future.
Materials and methods
The study design, materials, and procedure were approved by the Institutional Review Board at the University of North Carolina at Chapel Hill prior to recruitment (IRB #22-1817). Participants were recruited using purposive sampling from NC CSC programs and were approached either via email by a member of their treatment team or through self-referral in response to study flyers posted at CSC clinics. Eligible participants were caregivers of a relative receiving FEP treatment through NC CSC programs, which serve individuals aged 15–30 years with a primary diagnosis of a schizophrenia spectrum or other psychotic disorder with symptom onset within the past three years. Although any family member providing support to a young person with psychosis was considered eligible, only parents expressed interest in participating. Participants were excluded if they were under 18 years old, not proficient in English, involved in legal action against their relative with FEP, or unwilling to be audio recorded. Participants provided written informed consent and completed a demographics questionnaire before engaging in any interviews.
This study employed a combination of individual qualitative interviews and focus groups with FEP caregivers. The qualitative interviews were semistructured and included questions about caregivers’ experiences and challenges connecting their young person to CSC, ways in which their caregiving role has impacted their health and well-being, perceptions of unmet needs, and the types of services and supports that would benefit FEP caregivers (see Appendix 1). The focus groups concentrated on eliciting ideas and preferences for therapy content and educational materials caregivers would want included in the Altitudes platform, as well as the format and way they would like information presented. Focus group participants answered questions about how the needs of caregivers may change over time based on recovery stage (e.g., early crisis vs. more sustained recovery) and their views of guided support from a clinical moderator or family peer worker (see Appendix 2).
A male-identifying clinical psychology doctoral student (BS) and a female-identifying master's-level study coordinator (EF), both trained in qualitative interviewing, conducted all interviews and focus groups. Sessions were held via HIPAA-compliant Zoom between September and November 2022 (interviews) and March 2023 (focus groups). Interviewers had prior experience conducting qualitative interviews, delivering digital interventions, and working with individuals affected by psychosis, but lacked extensive formal training in family dynamics or caregiver-focused interventions. Although they had no prior personal relationships with study participants, each caregiver was informed that the interviewers were members of a research team seeking to adapt digital interventions to better support families of young people with psychosis.
All interviews and focus groups were audio recorded, transcribed with any identifying information removed, and analyzed using an inductive qualitative content analysis approach. We followed Erlingsson and Brysiewicz's hands-on guide for inductive content analysis. 25 The study coordinator (EF) created an initial codebook organized into a hierarchical coding structure, which was refined by the lead author (KL) and updated iteratively with input from other members of the coding team. After reviewing each transcript and discussing reflexive notes as a group, the coding team comprised of a licensed clinical psychologist (KL, PhD) and two undergraduate research assistants (NL and VP), developed preliminary themes and generated initial codes. Each transcript was coded using a line-by-line, selective coding approach. Two analysts independently coded each transcript, followed by review from a third coder. From June 2024 to August 2024, the coding team met weekly to evaluate each interview, discuss emerging themes, add or modify codes, and reach consensus on discrepancies. Throughout data collection and analysis, the research team engaged in regular reflexive discussions to consider potential biases and assumptions stemming from their personal, clinical, and research backgrounds.
Results
Participants
Eight participants completed the qualitative interview about their experiences caring for a young person with psychosis, connecting their relative to appropriate mental health care, and preferences for support from a digital intervention (Appendix 1). Five participants (62.5%) contributed to the virtual focus groups, comprised of 2–3 parents each (Appendix 2). On average, the recorded interviews lasted 73.33 min (SD = 16.09; range: 55.72–100.17), and focus groups were 64.9 and 68.6 min. No participants withdrew from the study.
Participants were parents of a youth engaged in CSC in Chapel Hill or Wilmington, NC. The average age of participants was 56.4 years (SD = 7.3 years). Most participants identified as female/mothers (n = 6, or 75%) and Caucasian (n = 8, or 100%). Participants were well-educated (M = 18 years; SD = 2.67), employed (n = 7, or 78.5%), and living with the affected young person (n = 7, or 78.5%). This sample is consistent with prior studies involving caregivers of young people with psychosis, which generally characterize this population as predominantly middle-aged, female, and living with their affected relative. Caregiver studies also report high rates of parental employment and educational attainment26–28 (see Table 1).
Demographic and background information of the caregiver sample.

This table shows basic demographic and background information for the caregivers who participated in qualitative interviews and focus groups, including age, gender identity, race/ethnicity, employment, education, and number of household members. It also includes information about their relatives with early psychosis (e.g., if the person with FEP lives with the caregiver and how many years since they first engaged in the CSC program).
Key themes
Primary themes that arose during the coding process included: (1) Challenges faced by caregivers who support a young person with psychosis; (2) Types of services and supports that may ameliorate the burden of caregiving; and (3) Content and features of a digital intervention that would be most appealing and appropriate for early psychosis caregivers. The research team determined that thematic saturation had been achieved during the data analysis stage, as no additional themes emerged and the interviews and focus groups yielded sufficiently rich information to address the study aims. See Table 2 for the list of primary themes and related subthemes.
Primary themes and subthemes from the content analysis.
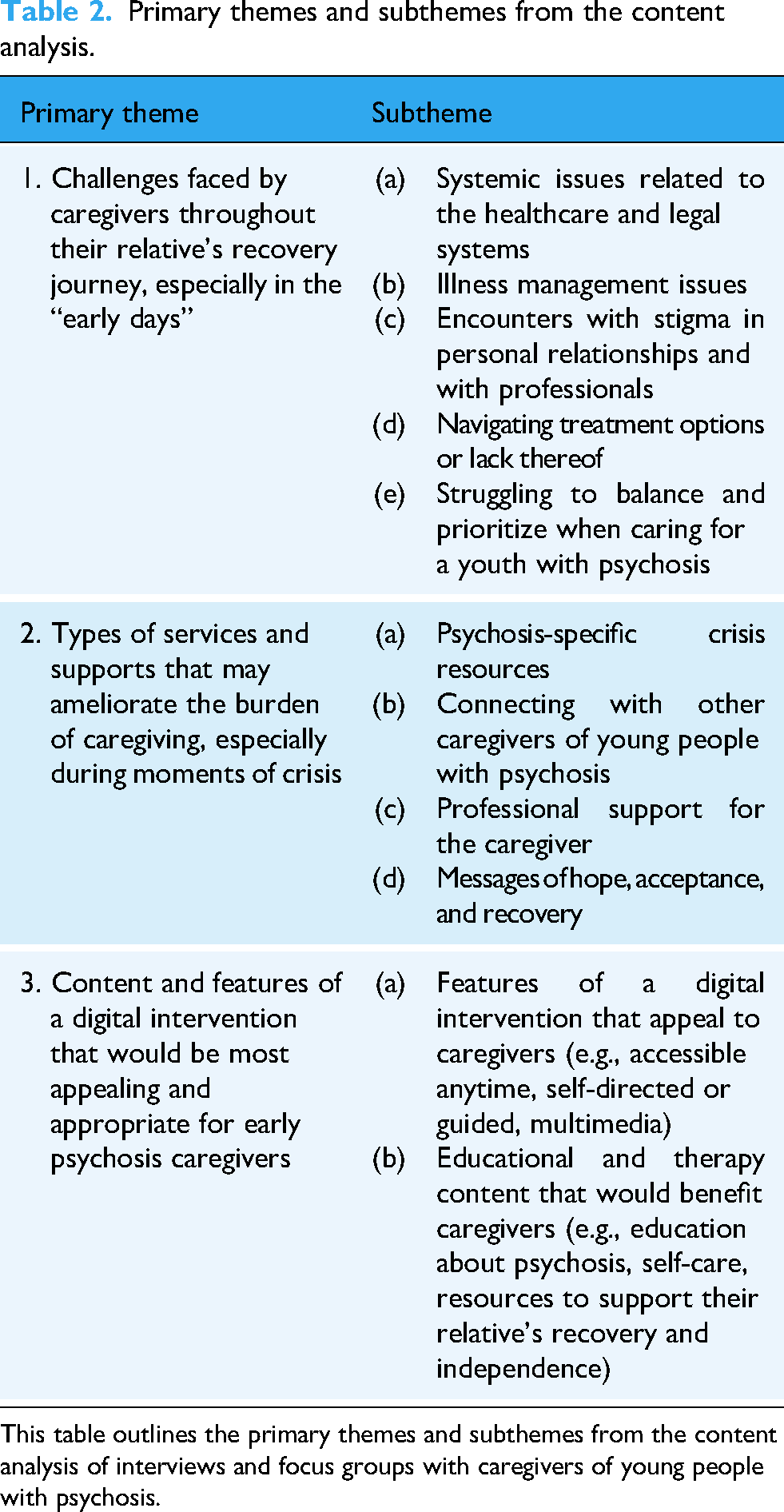
This table outlines the primary themes and subthemes from the content analysis of interviews and focus groups with caregivers of young people with psychosis.
Challenges faced by caregivers who support young people with psychosis
All caregivers described how harrowing it can be to support a young person experiencing serious mental health challenges, especially in the “early days,” which are often rife with feelings of uncertainty, isolation, and overwhelm. According to participants, the emotional sequelae of providing care to a young person experiencing FEP stemmed from five primary sources: (a) systemic issues related to the healthcare and legal systems, (b) illness management issues, (c) encounters with stigma, (d) navigating treatment options—or lack thereof, and (e) struggling to balance and prioritize when caring for a youth with psychosis.
Systemic issues related to the healthcare and legal systems
Parents are lost and confused when they realize their young person is struggling, and specific aspects of criminal justice, law enforcement, and mental health systems can make this experience even more distressing. One participant described the confusion and stress of trying to navigate these systems amid her daughter's initial psychotic episode: “I don’t really know what's going on because I haven’t been able to speak to a single doctor to give me a diagnosis…. I don’t know what her situation is, I don’t know what she's being treated for, I don’t know what drugs she's been given, I don’t know what the plan is for her. I don’t know anything… I was completely adrift in terms of knowledge, right? How do I get a criminal defense attorney, how do I find that person, how do I find that person and know that person is any good?” (501)
Illness management issues
Caregivers described struggling to manage the burgeoning mental health needs of their relative with FEP. Caregivers reported many challenges understanding and supporting their young person when their signs and symptoms of psychosis are insidious, capricious, or precarious. For example, one parent described feeling uncertain if her daughter's experiences were normative for adolescence or cause for more concern: “She was in high school when I started to notice that she seemed to have these little episodes of paranoia and I thought it could be those little episodes were simply ordinary social stress that most kids experience as they grow up, especially their teenage years, they become hyper-focused on what people think about them and what they might be saying about them or how they might be looking at them, but her- these little episodes often seemed to be out of the ordinary to me.” (501) “She was just violent and upset with me, she hated me, she was angry at me, she couldn’t say why… And my terror for her when I realized that she was more or less living on the streets… some old guy she met in a bar and he wanted her to move into his apartment, and she did.” (501)
Encounters with stigma
Caregivers described stigmatizing encounters with friends and family, and during interactions with law enforcement and healthcare staff. For example, one parent described an uncomfortable interaction with friends providing unsolicited and unrealistic advice when their son first received a diagnosis: “You talk to your friends that you go out and have book club with, well hell that's the worst possible thing you can do. [Impersonating friends] ‘Oh, I would force him to take those medications’, I would say, ‘You’re not gonna…’” (507)
Navigating treatment options—or lack thereof
Parents described challenges associated with obtaining appropriate and effective treatment, including struggling to find services, feeling unprepared for discharge from inpatient care, impediments to receiving an accurate diagnosis, and delays being informed about or referred to CSC. One participant described challenges unique to families who live in areas that lack qualified mental health providers and barriers to referral to CSC: “What we were coming up against was where we live, there's only one psychiatrist who's about 45 min away. And the psychotherapist and therapist and psychologists that were in our area… were not accepting new patients… Before we ended up, I read an article about [FEP clinic], and that was the first time we reached out, we were able to find them and connect. And even at that point, the psychologist that our son was seeing at the time said, ‘Oh, that's something for later.’ Didn’t put it in context about what he needed. So, it was frustrating.” (502)
Struggling to balance and prioritize when caring for a youth with psychosis
First Episode Psychosis caregivers often experience significant changes in relationships, disruptions to their employment/finances, and other challenging transitions. A mother shared how her son's experience with psychosis affected their family dynamics: “He's got a younger sibling, so disruption with [my daughter] because we can’t go do the things she wants to do because he can’t do it, or he doesn’t want to do it… and it's hard for my husband, because he feels like we’re in a rut. You know, like we can’t do anything, we can’t get out, we can’t go, we can’t go just take the boat out… and even when you do have that down time where everything's okay, it almost always turns into conversations of ‘well, how was this appointment,’ because he's going to occupational therapy, regular therapy, and then he sees the psychiatrist every two weeks now… so we end up just talking about it anyhow. So, it's always there.” (508) “And the disruption of daily life, especially the initial few days, I had to just call in and cancel patients… so there was some financial hardship there.” (504) “My employer as well, I couldn’t go to work, I mean I had such a difficult time that he allowed me to work from home.” (505)
What carers want or need to reduce the burden of caregiving
Caregivers described several services and supports that may ameliorate the burden of caregiving, including (a) psychosis-specific crisis resources, (b) connecting with other FEP caregivers, (c) professional support for the caregiver, and (d) messages of hope, acceptance, and recovery.
Psychosis-specific crisis resources
Caregivers expressed the need for emergency resources staffed by people trained in and knowledgeable about psychosis. Parents who attempted to utilize emergency resources wanted targeted support, reassurance, or guidance in moments of crisis: “One big thing I guess I would say that I was disappointed in too, and this again was the helpline. Calling the mobile crisis. Because that's a very general type line, I think, with this so maybe—and yes, their therapist, but the therapist and things can only do so much with their time…It's having somebody to be able to reach out to I guess—Sometimes I think we need our own line or our own support to say, ‘Hey, I’m really worried, he's decided to stop his medication.’” (507)
Connecting with other FEP caregivers
Participants were particularly keen on connecting with other families who had lived experience of supporting a young person with psychosis: “I mean even boards are great, just being able to just talk to someone, ‘this is what happened today’, you know?” (505) and “There's value in being with people who have had a year's time pass and have had to deal with this whether their person is recovering faster or slower, they’ve still been doing this for a year, you’ve been doing this for a year, it would be helpful to compare notes of how they’re coping with it.” (503)
They reported that other caregivers could normalize and share strategies for managing stress, ambiguous loss, and grief. Several parents shared that it would have been helpful to talk with other caregivers about navigating privacy laws and advocating for the young person's care.
Professional support for the caregiver
Participants reported that they could have benefitted from connecting with mental health professionals to discuss their own well-being earlier in this process. As one parent explained: “For most families, more intensive therapy is probably gonna be really helpful, not just the psychosocial educational piece that [FEP clinician] does which is incredibly valuable, but also just day-to-day, week-to-week support from a therapist who is really just going to help you through the crisis which isn’t over right away. Anybody with psychosis is going to be suffering for quite a while before—even after they’re stable, there are going to be big issues.” (501)
Others expressed interest in science-backed recommendations for making sense of their young person's recovery journey and responding appropriately to common but concerning observations of their relative. For instance, someone to answer questions like “Why aren’t they bathing? … Why don’t they want to take their medication?” (507)
Messages of hope, acceptance, and recovery
Parents asserted that any caregiver would benefit from the instillation of hope and recovery. As one parent described: “I really, really, really wanted to know that she could recover, that there was hope. I was so convinced that there was no hope that it took me a long time to accept the fact that there was… I was terrified when my daughter got sick and for good reason because I had seen some really poor outcomes in our family… helping people understand that there is a path to recovery and stability and that there is hope and there are things that can be done, interventions that are evidence-based that work. Boy, would that have been great to know early on.” (501)
Content and features of a digital health program that would be most appealing and appropriate for early psychosis caregivers
Overall, participants wanted the platform to be user-friendly, accessible, private, self-directed, flexible, welcoming, and nonjudgmental.
Features of a digital intervention that appeal to caregivers
Two parents explained the advantages of a program that is available anytime, self-directed and/or involving an individual coach or guide: “I do things at weird hours of the day, having a full-time job, multiple kids, and then all of these doctors’ appointments that come with this journey, so sometimes it's midnight when I get around to doing something. So self-directed for me.” (508) “I actually enjoy having somebody that I could go talk to, as in a therapist, who could help me worry about me instead of always being worried about him, which I was, which we do because we’re mothers and we care about our child… I think some people may be looking for that. People may especially have a little bit of that barrier to looking for the self-directed information the way we do, like reading the book, it may, this person maybe could say, ‘Well, why don’t you wanna read the book? What's preventing you?’ in a roundabout, therapeutic way. I think that would be helpful, but I think I’d like self-directed, too.” (507)
Portraying information via a mix of written content, infographics, audio, and videos with transcripts would facilitate access for people who have different preferences and learning styles. Participants emphasized optionality and information that could be accessed surreptitiously in various settings (in bed, at work, waiting room, etc.).
Educational and therapy content that would benefit caregivers
Regarding specific content that would be helpful for caregivers, parents noted education about psychosis, self-care strategies, and resources that could promote recovery, stability, and independence for their relative “But it took a while to figure out how we were going to get the medicine at a reasonable cost, ‘cause it was very expensive, monthly… Insurance, medicine, social security, disability, Medicaid, and what are the steps, what, how do you go about doing this? Is it necessary to do this? If you don’t do this, what are the consequences? [Also], I think employment. How can we access employment opportunities? Education? How can we access education opportunities? Those would be broad categories. Even simple categories, which might not be an issue at this point in time, but might be at another point in time, is that how can we monitor, or maintain self-care for our loved one, and make sure that's being taken care of. Not for myself, well then that’d be another category, self-care for myself, so those are two categories.” (504)
Several participants described wanting to learn about services that may advance their young person's recovery and prepare them for success in the future.
Discussion
The purpose of the current study was to better understand the experience of caring for a young person with psychosis in the United States, including the unique needs of American caregivers in this role, and to adapt a digital intervention with this information to improve family support throughout their relative's recovery process. The authors identified three key themes that emphasized the internal and external stressors faced by parents as they navigate complex systems of services to support their relative with FEP as well as their preferences for supports to ameliorate the burden of caregiving.
Our content analysis indicated that the transition from prodromal symptoms to acute psychosis is wrought with challenges and may require multifaceted and individualized support for families. Because prodromal symptoms often appear subtle or nonspecific, they may not be recognized as early indicators of psychosis. 29 As a result, families may delay help-seeking until symptoms worsen or begin to impair functioning. 30 By the time the young person enters an acute phase, caregivers are often deeply concerned but uncertain about what is happening or how best to respond. Providing families with education about early warning signs, phases of illness, and the benefits of timely treatment may help reduce delays in care and counteract the stigma that frequently surrounds early psychosis. 31
The current findings align with prior research suggesting caring for a relative with a SMI is stressful, stemming from both objective and subjective aspects of caregiving. 32 Like the qualitative needs assessment for Bolster, participants in the current study highlighted the need for psychoeducation about psychosis, assistance responding to emergent situations, guidance navigating the healthcare system and connecting their young person to CSC, and ways to effectively respond to sources of stigma. 33 As evidenced in the quotes above, caring for an FEP relative can have tangible effects on daily life, including changes in relationships, employment, and difficulty “just to take care of yourself” (502). It is not uncommon for caregivers to put their own lives on hold to support their affected relative or for the family to be “all hands on deck” in moments of crisis (507). Experiences of stigma, negative appraisals of caregiving, and feelings of discouragement are common issues articulated by families that can intensify the stress of caring for a young person with FEP.34,35
Caregivers articulated an interest in digital interventions where they can access accurate information, ask questions, and receive support anytime, anywhere, and without serious risk of incidental disclosure. Considering caregivers tend to have multiple roles and responsibilities, a digital resource allows for flexibility to meet the unique needs of family members, including the ability to read, watch, or listen to information at their own pace and the option of working with a guide to discuss the information, track progress, and promote a sense of accountability. Although Altitudes is neither an emergency service nor intensive individual therapy for families, the MOST framework allows caregivers to access much-desired information about psychosis and to learn therapy skills to manage stress and promote well-being.
While accessing evidence-based information and connecting with professionals appealed to many caregivers, several participants wanted to connect, share stories, and exchange messages of hope and support with other parents. Altitudes align with self-determination theory to accommodate caregivers’ varying goals and requisites. 36 The therapy content scaffolds learning to facilitate competence and mastery and the social networking features aim to foster connection and a sense of belonging among caregivers. Encouraging users to engage with the platform in a way that suits their needs promotes autonomy and emphasizes choice. In addition to allowing family members the flexibility to participate in a manner that is most comfortable and useful for them, the community components of Altitudes can foster social connection, validate and buffer against some of the more stigmatizing and stressful aspects of caregiving, and reduce isolation and loneliness.
Although relatively nascent and not available everywhere, there is a growing number of community-based resources intended to support and connect caregivers, including Psychosis Recovery by Enabling Adult Carers at Home (Psychosis REACH) and the National Alliance on Mental Illness family support groups.16,37 Although these programs are designed to support the mental health and well-being of supporters, they can be limited by capacity constraints and geographic restrictions. Additionally, while many training programs and family connection groups are scheduled to accommodate caregiver availability, programs that deliver synchronous virtual groups may not be available to everyone. Digital interventions like Altitudes which involve asynchronous access to human support may address these gaps. Further, considering the benefits of peer-led interventions and connecting caregivers to other families, an important aspect of the Altitudes digital intervention is the inclusion of “Family Workers,” individuals with lived experience supporting an FEP relative. Family workers use their knowledge, experience, and recovery stories to instill hope and share valuable insights with Altitudes users.
Our research team will use the feedback from participants to amend and expand the self-directed psychoeducation and therapy content in Altitudes to reflect the specific needs of American caregivers (e.g., understand privacy, confidentiality, and HIPAA to better advocate for an FEP relative). We also plan to revamp and reorganize the therapy content to align with the recovery stage of the young person with FEP. For example, we will develop materials specific to caregivers whose relative recently started experiencing symptoms (e.g., how to talk about psychosis with family and friends after an initial diagnosis) and add prompts to help caregivers reflect on ambiguous loss when there are delays or setbacks in the recovery journey.
In response to the perspective that the digital intervention for caregivers should include a mixture of written and audiovisual elements, we plan to update Altitudes with new infographics and multimedia content for implementation in the United States. We will also incorporate audio files that explain and demonstrate important skills to make the therapy materials more approachable, accessible, and interactive. We hope that providing the adapted Altitudes program to family members of young people with psychosis is an important step toward “the day that there's more understanding and parity” (500) in destigmatizing psychosis and supporting American caregivers.
Limitations
The current study is not without limitations. First, we interviewed a relatively small sample of predominantly white, well-educated, middle-aged parents of adult children with psychosis. Furthermore, participants were caregivers of young people who had successfully enrolled in CSC. This is important as CSC programs may not be accessible to a significant portion of individuals who are eligible for such care. Therefore, the experiences may not be representative of persons with more significant barriers to CSC treatment or who require a higher level of care than what may be available through such services. Additionally, these findings may not reflect the experiences of nonparent supporters such as siblings or partners, persons living in other regions of the United States, or cross-culturally.
Although the sample included only eight participants across two phases of interviews and focus groups, Hennink and Kaiser found saturation of themes can be reached with relatively small sample sizes, 38 and we determined that saturation was achieved in the present study. Nonetheless, we acknowledge that the concept of saturation has recognized limitations in qualitative research, as new insights could always emerge with additional participants or under different contextual circumstances. 39 Our determination of saturation reflects the richness and depth of data obtained within this particular sample and study design.
Finally, the themes generated are based on narratives provided by participants during in-depth interviews and small focus groups completed over a relatively short period of time. Given the often-episodic course of psychotic disorders and the dynamic nature of familial relationships, it is possible that participants’ responses were impacted by current mood states, recent experiences, relational factors such as tension in the parent–child relationship, or relative dis/comfort disclosing private or sensitive information about their family with the interviewer. Thus, the findings of the current study should be interpreted with caution.
Future directions
While the current investigation provides insights into the experiences of parents who were active in connecting their FEP relatives to appropriate mental health care, future research should explore the experiences, challenges, and needs specific to caregivers who support individuals who are unable or unwilling to engage in CSC. This is particularly important as the literature underscores implementation barriers to CSC service provision and engagement, including stigma, cultural competence, and impediments related to issues with transportation, finances, and proximity to care.40,41
As delivering family interventions during the “critical period” of psychosis can bolster caregivers against feeling isolated and overwhelmed, we plan to test the feasibility, accessibility, and potential treatment benefits of Altitudes for families whose relatives are enrolled in or on the waitlist for services at NC CSC programs. 42
Conclusions
This study highlights the complex needs and preferences of caregivers supporting a young person with FEP in the United States. Many caregivers experience significant stress as they struggle to understand what is happening to their relative and navigate the process of connecting them to appropriate care. Digital interventions like Altitudes, when adapted to reflect caregivers’ experiences and priorities, hold promise for enhancing education, connection, and resilience among families of young people with psychosis. The findings underscore the value of supplementing traditional services with flexible care options that offer timely access to information, resources, and opportunities to connect with other families. Caregiver-focused digital tools may help mitigate stress and promote more positive outcomes for families navigating the challenges of psychosis recovery.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251378608 - Supplemental material for Altitudes adaptation and development: Content analysis of experiences and preferences for a digital intervention to support early psychosis caregivers in the United States
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251378608 for Altitudes adaptation and development: Content analysis of experiences and preferences for a digital intervention to support early psychosis caregivers in the United States by Kelsey Ludwig, Elizabeth Fraser, Bryan Stiles, Vinitha Panchikarla, Natasha Lang, Hanna Campbell, John Gleeson, Mario Alvarez-Jimenez and David Penn in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251378608 - Supplemental material for Altitudes adaptation and development: Content analysis of experiences and preferences for a digital intervention to support early psychosis caregivers in the United States
Supplemental material, sj-docx-2-dhj-10.1177_20552076251378608 for Altitudes adaptation and development: Content analysis of experiences and preferences for a digital intervention to support early psychosis caregivers in the United States by Kelsey Ludwig, Elizabeth Fraser, Bryan Stiles, Vinitha Panchikarla, Natasha Lang, Hanna Campbell, John Gleeson, Mario Alvarez-Jimenez and David Penn in DIGITAL HEALTH
Footnotes
Acknowledgements
This research was supported by the Early Psychosis Intervention Advisors of North Carolina (EPI-NC) and the North Carolina Department of Health and Human Services (NC DHHS). The study was funded by the Federal Community Mental Health Services Block Grant (CFDA #93.958). The authors would like to thank all caregivers and supporters of young people with psychosis who participated in this study, including all research participants and collaborators for their valuable insights and significant contributions to the study design, implementation, and analysis.
Ethical standards statement
As noted in the enclosed manuscript, the study design, measures, and procedure have been approved by the Institutional Review Board (i.e., ethics committee) at the University of North Carolina at Chapel Hill (IRB #22-1817). All participants provided written informed consent prior to their involvement in the study. All identifying information has been removed from the manuscript so as to minimize any risk of incidental disclosure of the identity of any caregiver participants or their family member(s) who have experienced psychosis. The study was completed in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the North Carolina Department of Health and Human Services (grant number CFDA #93.958).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
All supplemental material mentioned in the text is available in the online version of the journal.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.