
Abstract
Objective
Research on effective implementation options and key factors in blending face-to-face (FTF) psychotherapy with online treatment elements (i.e., blended therapy, BT) remains limited. This study aimed to explore patients’ experiences and to identify relevant factors in implementing BT in routine care.
Methods
Qualitative semi-structured interviews were conducted with 40 patients (10.7% of N = 375) from the PSYCHOnlineTHERAPY trial. The patients were adults with diagnosed anxiety or depressive disorders and received one of two versions of BT based on cognitive behavioral therapy, differing in the flexibility to decide on the sequence and ratio of BT elements (FTF sessions and online self-help sessions). The interviews were audio-recorded, transcribed, and analyzed using a deductive-inductive qualitative content analysis approach, partly theory-based on the “Efficiency Model of Support.”
Results
The analysis revealed 163 theme codes, categorized into 30 subcategories. The main categories were “motivation and expectations,” “active components, mechanisms of change, and effects,” “blending scenarios,” “therapeutic alliance,” “negative effects,” “fit,” “facilitators and barriers for engagement and daily life transfer,” “usability,” and “optimization possibilities.” Key findings highlight positive outcomes of BT, the important role of the therapist, the transformative interaction of FTF and online sessions, and the distinctive functions and benefits of each element, suggesting BT's added value over stand-alone treatments. Various patient, therapeutic, and treatment characteristics emerged as relevant facilitators and barriers across different domains. Heterogeneity in patient preferences emphasized the importance of personalization.
Conclusion
Overall, these results provide valuable insights for the practical implementation and further research on BT.
Trial registration
German clinical trial register (DRKS00023973, date of registration: December 28, 2020), https://www.drks.de/search/de/trial/DRKS00023973.
Introduction
Anxiety and depressive disorders are highly prevalent, carrying a notable burden of disease and a corresponding demand for appropriate treatment.1,2 Psychotherapeutic interventions, especially cognitive behavioral interventions, have demonstrated efficacy in treating both conditions,3,4 are highly recommended in established treatment guidelines,5,6 and are accepted treatment options for patients.7–9
Blended therapy (BT) is a psychotherapeutic treatment format that combines face-to-face (FTF) and internet- and mobile-based self-help interventions (IMIs), integrating the benefits of two evidence-based treatment approaches.10,11 IMIs present a flexible, low-threshold treatment option and have been shown to be comparably effective to FTF interventions in treating anxiety and depressive disorders. 12 Both approaches, however, have their respective limitations, such as dependency on time and location for FTF interventions, and lack of personal contact and overemphasis on self-help in IMIs. BT has additional benefits over standalone versions of both treatment formats: while FTF interventions offer the advantage of real-time personal contact with an on-site therapist, BT offers patients more variety within the therapeutic process by including both FTF elements and self-paced online elements for everyday life. This combination may lead to increased flexibility, reduced time required of the therapist (e.g., fewer FTF sessions required),11,13–15 and increased therapy-dose due to additional online sessions on top of a given number of FTF sessions.16,17 As added value to standalone IMIs, BT provides FTF contact, guideline conform treatment options during acute crises (e.g., therapist as professional contact person, FTF consultations in case of crises), and potentially fosters better participant acceptance and adherence.13,18,19 Patients might also prefer BT over treatment as usual (psychotherapy and/or pharmacotherapy). 20 BT has demonstrated acceptance among patients, therapists, and stakeholders,19,21–24 efficacy and effectiveness in treating mental disorders,18,25–27 potential time efficiency advantages over traditional FTF psychotherapy,14,15,28 and the potential of increasing effects of FTF interventions with IMIs as add-ons.11,16 However, whether the advantages of BT apply may depend on the specific treatment protocol, as there are various ways to implement BT. 20
Integrated concepts of BT apply IMI and FTF elements within the same period of time, whereas sequential concepts are implemented as stepped-care.10,11 Different ratios and sequences of IMI and FTF elements may be used,20,29–31 and the two components could take on different functions in the treatment.10,30,32 In this context, a Delphi study investigating suitable treatment protocols found that different contents were considered differentially suitable for either IMI or FTF treatment elements by patients and therapists. 30 For example, FTF was perceived as particularly appropriate for introducing treatment, progress evaluation, or addressing patient questions, whereas IMIs were rated to be useful for psychoeducation or mood and activity diaries. Further, different ratios of online to FTF sessions were preferred by patients, as some preferred an equal ratio while others preferred more FTF or more IMI sessions. 30 Regarding blending scenarios (i.e., the integration or interaction of IMI and FTF elements), one implementation option may be an active blending with reciprocal reference and transformation of the stand-alone elements, such as outsourcing content from the FTF sessions or the possibility of new treatment elements in FTF sessions.13,33 Another option could be a lack of active interplay or transformation, e.g., IMIs serving as an add-on without affecting the structure and content of FTF components.13,33 However, it remains unclear how different blending variations of BT may function in practice, which functions the two elements have in BT, and which barriers, facilitators, and blending scenarios should be considered during implementation in routine care. To our knowledge, no qualitative study has yet explored patient experiences across different predefined implementation variants of BT.
To address these questions, this qualitative interview study investigates patients’ treatment experiences with the implementation of two versions of integrated BT in routine outpatient care: one with a flexible ratio of cognitive behavior therapy (CBT)-based FTF to online elements, with element sequence determined by the therapist and patient, and the other with a predefined alternating sequence of FTF and online elements. This study aims to examine the implementation of BT in routine care and address existing research gaps, focusing both on BT in general and on comparing the two specific versions. The aims are to explore (1) patients’ motivations and expectations, (2) the functions of online and FTF elements, (3) blending scenarios (i.e., how the blending of both elements worked and was implemented), (4) relevant factors and associated barriers and facilitators in the implementation and subjective effectiveness of BT, and (5) negative effects occurring during BT.
Methods
This qualitative study was part of the PSYCHOnlineTHERAPY trial evaluating BT for patients with depressive and anxiety disorders. 34 The study was approved by the ethics committee of the German Psychological Society (BaumeisterHarald2020-07-29VADM, date of approval: September 23, 2020) and registered in the German clinical trial register (DRKS00023973, date of registration: December 28, 2020). Details of the study can be found in the study protocol. 34 Reporting of the results of this qualitative study follows the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines 35 (see Additional file 1).
Study design of PSYCHOnlineTHERAPY
Patients in the three-armed cluster-randomized controlled PSYCHOnlineTHERAPY study were recruited between January 2021 and April 2023 via 75 licensed outpatient psychotherapists in Germany (Baden-Wuerttemberg) who delivered the intervention and had been randomized to one of two versions of BT or standard CBT. As part of the recruitment process within routine care, participating psychotherapists screened their patients for eligibility and informed them about the study. Included patients were at least 18 years old and had a psychotherapist-diagnosed depressive and/or anxiety disorder according to the International Classification of Diseases (ICD-10). 36 Self- and observer-based assessments with online-questionnaires and clinical telephone interviews were conducted at several time points, with depression and anxiety severity (Patient Health Questionnaire Anxiety and Depression Scale, PHQ-ADS) 37 at 18 weeks post-inclusion (post-treatment) as the primary outcome.
Interventions
Two versions of BT (PSYCHOnlineTHERAPYfix, PSYCHOnlineTHERAPYflex) combined FTF sessions with a psychotherapist and self-help online sessions, and were accessible on the online platform eSano.38,39 The study treatment of both versions comprised up to 16 sessions in total but could be concluded earlier, e.g., if the therapeutic goals were achieved before reaching this maximum. PSYCHOnlineTHERAPYfix (FIX) patients were intended to receive a fixed alternating sequence of up to eight FTF sessions and up to eight online sessions. PSYCHOnlineTHERAPYflex (FLEX) patients were intended to receive up to 16 FTF sessions and up to 16 online sessions with a flexible number and order determined by the therapist and their respective patient (e.g., 11 FTF sessions and five online sessions). CBT-based online sessions were assigned by the on-site therapist, who could choose from seven depression-specific sessions, seven sessions for each anxiety disorder, 22 transdiagnostic sessions, one introductory, and one closing session. The online sessions had an intended duration of 45–60 minutes each and comprised textual, audio, and video material, interactive elements, homework assignments, and downloads (e.g., worksheets). The CBT-based FTF sessions did not follow a predefined treatment protocol within the study.
Participants and recruitment
We aimed to achieve sufficient theoretical data saturation for the qualitative interviews, with a predefined target sample size of n = 20 patients per study group 34 based on established principles. 40 Between December 2021 and August 2022, 85 (FIX: n = 42, FLEX: n = 43) of 274 patients already enrolled at this time of the trial were invited to participate in qualitative interviews. Written informed consent was obtained of all study patients at baseline. Study patients were invited if they (a) belonged to either the FIX or the FLEX study group according to the randomization condition assigned to their therapists, (b) had completed the post-treatment assessment (as an indicator of treatment completion), (c) consented to audio recording during the interviews, and (d) had not withdrawn from the main study. Patients who started the intervention before April 2021 were excluded from participating in this qualitative study to avoid bias due to technical issues with the online platform before that date. Invitations were sent via e-mail, directing patients to book an interview appointment on an online booking page. Patients were reminded up to three times via e-mail and up to one time via phone. We recruited 20 patients from the FIX group and 22 from the FLEX group (response rate of n = 42/85, 49.4%). Two FLEX patients were excluded due to technical problems that prevented the audio recording of their interviews. All patients received 30€ for participating in the qualitative interview.
Qualitative data collection
A semi-structured interview guide was developed (TS, IT, AZ), drawing partly on our considerations of potential blending scenarios related to our research questions and partly on the Efficiency Model of Support. 41 The Efficiency Model of Support was selected as the theoretical basis for our research, as it explains the outcomes of technology-based interventions based on both technological characteristics and characteristics of the interaction between participants and guidance providers (in our case, the on-site therapists). The model encompasses five categories of factors assumed to influence an intervention's effectiveness: factors regarding (a) the alignment of the intervention with the participants’ needs (fit), (b) participants’ intention or motivation to use the intervention (engagement), (c) integration of the intervention into participants’ daily lives (implementation), (d) correct application and use of the intervention (knowledge), and (e) the intervention's user-friendliness (usability).
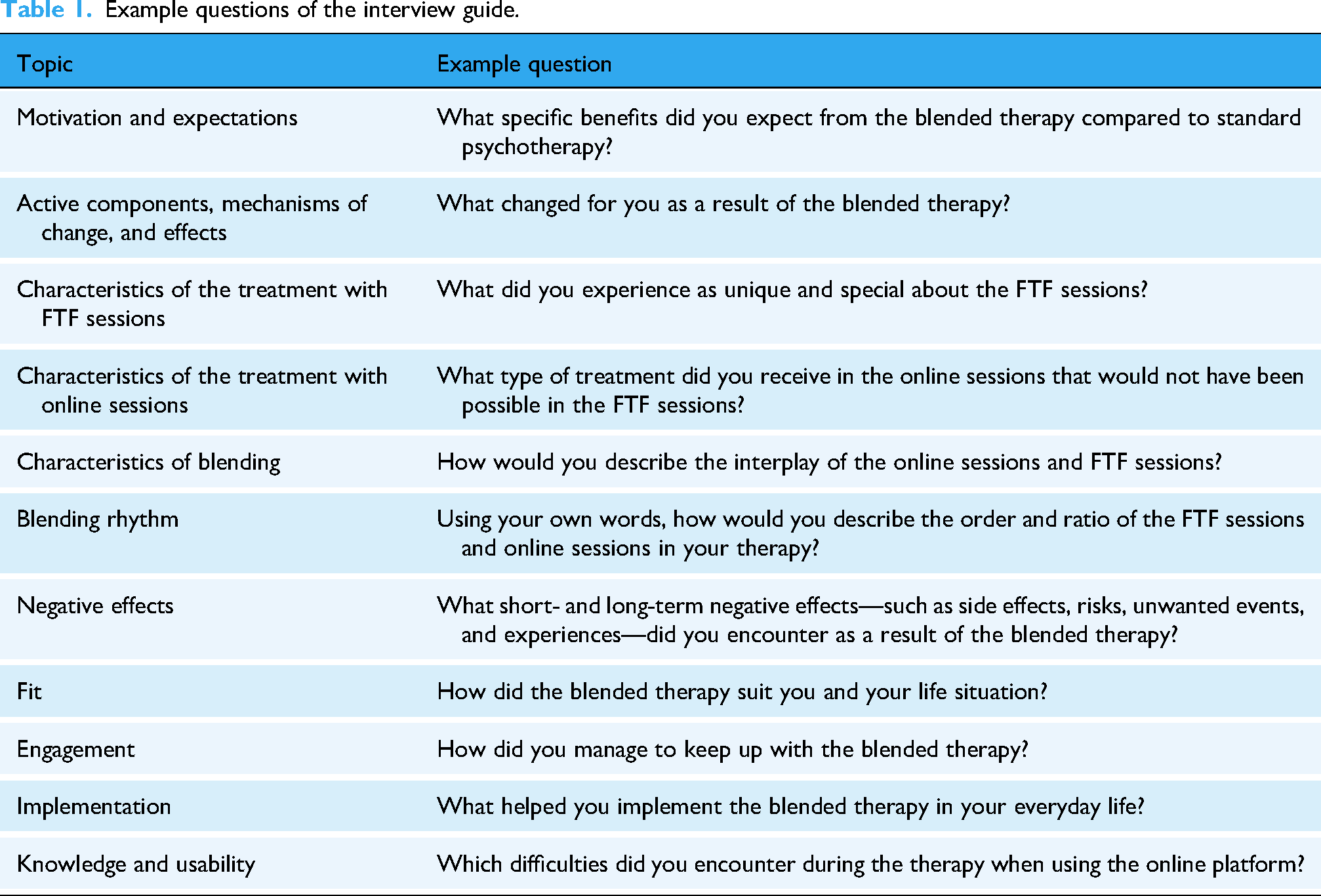
The self-developed interview guide (see Additional file 2) consisted of 54 open questions from 12 topics: motivation and expectations (three questions); active components, mechanisms of change, and effects (two questions); characteristics of the treatment with online sessions (four questions); characteristics of the treatment with FTF sessions (seven questions); characteristics of blending (nine questions); blending rhythm (six questions); negative effects (four questions); fit (four questions); engagement (five questions); implementation (five questions); knowledge and usability (four questions); further comments (one question). Table 1 shows exemplary questions for each topic. Two questions regarding session ratio and frequency were tailored to the patient's study group (FIX or FLEX). Other than these, all patients were asked the same set of questions.
Example questions of the interview guide.
The interviews were conducted via phone between January 2022 and August 2022 by two psychologists with university-degrees and in CBT training (JF, LM) who received specific training for this task by the responsible study team members (TS, AZ). On average, the interviews lasted 59 minutes (SD = 13 minutes), with durations ranging from 24 to 100 minutes. The audio recordings of the interviews were transcribed verbatim using the software tool MAXQDA 42 following a predefined transcription guide. All qualitative data were anonymized during the transcription process.
Quantitative data collection
Quantitative data were collected through online questionnaires and diagnostic interviews at baseline, prior to the start of the intervention, as part of the PSYCHOnlineTHERAPY study. 34 Sociodemographic patient data included age, gender, educational level, relationship status, employment status, residence size, and prior psychotherapy experience. Diagnoses were assessed by the therapists for their respective patients. Depression and anxiety severity was assessed with the PHQ-ADS, where higher scores indicate greater levels of anxiety and depressive symptoms (score range: 0–48, α = .89). 37 Data on whether an alternating session sequence (i.e., alternating FTF and online sessions as defined for the FIX condition) was implemented for each patient were derived from standardized therapist reports completed after each FTF session, which also included information on the assigned online sessions. Therapist characteristics were assessed via online questionnaires and included information on age, gender, time since licensed as therapist, and experience with digitally supported psychotherapy. Quantitative data was analyzed descriptively using SPSS. 43
Data analysis
Using the software tool MAXQDA, 42 we conducted a qualitative content analysis following a deductive-inductive approach 44 with the following procedure: (1) Within the deductive approach, main categories were derived based on the research questions and the topics outlined in the interview guide. (2) Within the inductive approach, subcategories and codes were initially developed by two independent coders (KB, LL). Starting with two interviews, additional transcribed material was sequentially added during this process until a total of 70% (n = 28) of interviews were included for the development of the code system. Existing codes were refined, and new codes were added and discussed during regular consensus meetings (KB, LL, TS). Coding rules were simultaneously developed, defining one sentence as the smallest coding entity, a complete statement as the context entity, and allowing multiple codes for a single text passage. (3) The initial code system, including code definitions and illustrative statements, was refined through feedback loops with CBT-therapists and experts in IMIs and qualitative research (AZ, IT, JS, TS). (4) A second dyad of independent coders (LL, JS) applied the revised preliminary code system to the previously coded 70% (n = 28) of interview material to assess its applicability. (5) The code system was revised in further consensus meetings and additional feedback loops (AZ, IT, JS, TS). (6) A test coding of three interviews (from the 28 interviews) was performed by a third dyad of independent coders (JS, LM), leading to final adjustments of the code system and the coding rules (JS, LM, TS). (7) The independent coders (JS, LM) performed the final coding on the entire dataset (100%, n = 40). (7) The inter-coder agreement with a targeted code overlap of 70% was weak 45 to moderate, 46 with a Kappa value of k = 0.46. Coders were psychology students (KB, LL, and LM) and a researcher and clinical psychologist (JS), and were trained by the responsible study team member (TS). Frequencies of the final theme codes are reported for the whole sample as well as separately for the FIX and FLEX study groups.
Results
Sample characteristics
The sociodemographic and clinical characteristics of the interviewed sample are shown in Table 2 (see Additional file 3 for details on the non-interviewed sample). The mean age of the 40 interviewed patients was 39.2 (SD = 14.1), with 28 (70.0%) being female. Most patients were in a relationship (n = 30, 75.0%) and employed (n = 31, 77.5%). About half of the sample (n = 22, 55.0%) had a high level of education, and the majority of the patients (n = 34, 85.0%) lived in a small town with less than 20,000 inhabitants. Regarding their diagnosis at inclusion, 20 (50.0%) had a depressive disorder, 11 (27.5%) had one or more anxiety disorders, and 9 (22.5%) had comorbid depressive and anxiety disorders or a mixed anxiety and depressive disorder. The severity of depression and anxiety at baseline on the PHQ-ADS was, on average, moderate (M = 22.5, SD = 9.3). The 22 therapists treating the interviewed patients were predominantly female (n = 16, 72,7%) and had a mean age of 49.1 years (SD = 11.0). The average number of years since being licensed as a therapist was 8.42 (SD = 11.6), with 5 (22.7%) therapists having previous experience with digitally supported psychotherapy.
Baseline characteristics of the interviewed sample.
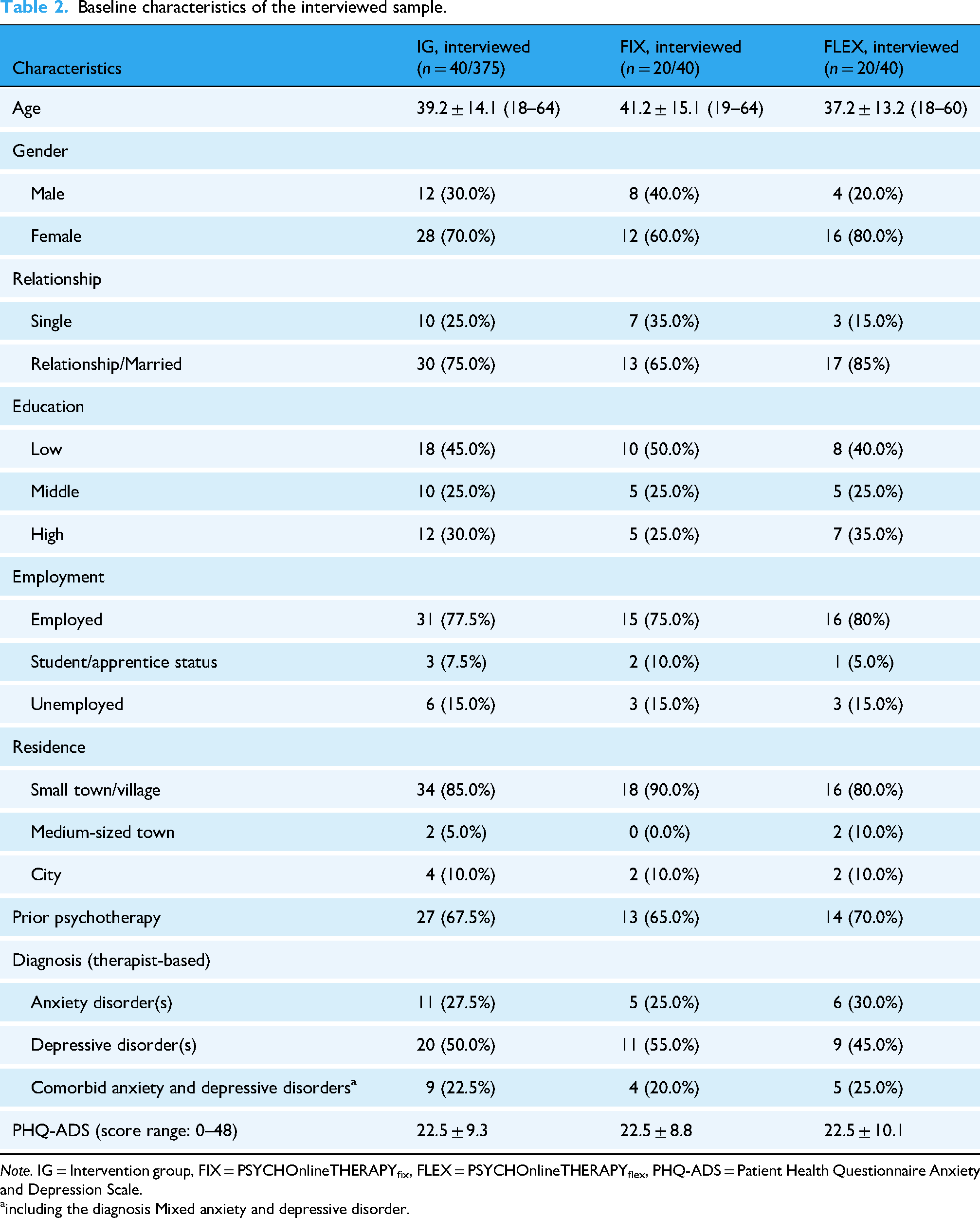
Note. IG = Intervention group, FIX = PSYCHOnlineTHERAPYfix, FLEX = PSYCHOnlineTHERAPYflex, PHQ-ADS = Patient Health Questionnaire Anxiety and Depression Scale.
including the diagnosis Mixed anxiety and depressive disorder.
Intervention characteristics
Within the FIX group, 70.0% (n = 14/20) of patients received BT with the intended alternating sequence of FTF and online sessions. For the remaining 30.0% (n = 6/20), therapist reports indicated deviations from the intended alternating session rhythm. Within the FLEX group, 10.0% (n = 2/20) had an alternating sequence.
Qualitative findings
The qualitative content analysis resulted in 10 main categories with s = 30 subcategories and m = 163 theme codes. Main categories were: motivation and expectations (s = 2, m = 19); active components, mechanisms of change, and effects (s = 2, m = 14); blending scenarios (s = 8, m = 51); therapeutic alliance (s = 2, m = 7); negative effects (s = 3, m = 11); fit (s = 1, m = 10); facilitators of treatment adherence and engagement and daily life transfer (s = 3, m = 15); barriers to treatment adherence and engagement and daily life transfer (s = 3, m = 9); usability (s = 2, m = 8); and optimization possibilities (s = 4, m = 19). Key themes (m = 88, 54% of 163) mentioned by at least 25% (n ≥ 10) of interviewed patients (regardless of the study group) are reported below and summarized in Table 3 with definitions, frequencies (for the total sample and separately for FIX and FLEX), and supporting quotations. A complete listing of all m = 163 theme codes with their frequencies, definitions, and supporting quotations can be found in Additional file 4.
Key themesa of the qualitative content analysis with frequencies, definitions, and supporting quotations.
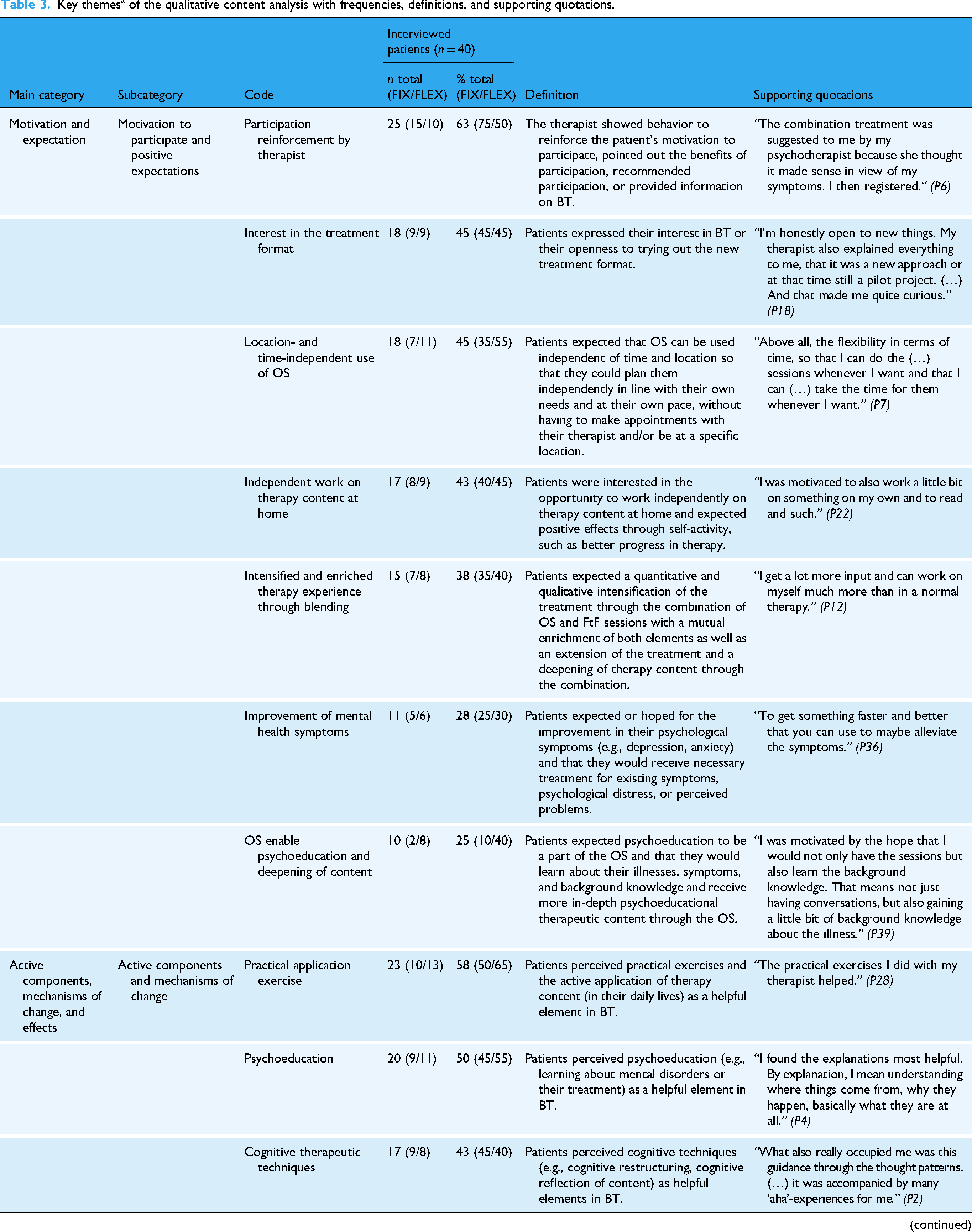
Note. n = number of patients reporting a theme, % = percentage of patients reporting a theme, BT = blended therapy, OS = online session, FtF = face-to-face.
Key theme = mentioned by at least 10 patients (25% of N = 40 interviewees).
Motivation and expectations
Patients mentioned themes related to their motivation for participation, expressing positive expectations (m = 13) and negative expectations (m = 6) regarding the BT, with m = 7 (37%) key themes identified. Positive and motivating factors included reinforcement of participation in BT by the therapist (n = 25, 63%), interest in the blended treatment format (n = 18, 45%), expectations of flexibility regarding a location- and time-independent use of the online sessions (n = 18, 45%), and the ability to work on therapy content independently at home (n = 17, 43%). Further, an anticipated intensified and enriched therapy experience through blending (n = 15, 38%), hope for improvement in mental health symptoms (n = 11, 28%), and the expectation that online sessions would enable psychoeducation and deepening of therapeutic content (n = 10, 25%) were reported. None of the negative expectation themes emerged as key themes (n ≤ 7).
Active components, mechanisms of change, and effects
Patients experienced active components and mechanisms of change (m = 8) that, from their perspectives, contributed to the effects of the BT (m = 6). A total of m = 11 (79%) key themes were identified. Regarding active components and mechanisms of change, patients found practical exercises and the active application of content (n = 23, 58%), psychoeducation (n = 20, 50%), cognitive therapeutic techniques (n = 17, 43%), normalization of symptoms (n = 13, 33%), blending of online and FTF sessions (n = 11, 28%), and the therapeutic alliance (n = 10, 25%) to be most helpful. The most frequently mentioned effects of BT included behavioral changes in daily life (n = 18, 45%), improved coping with existing symptoms or related situations (n = 17, 43%), improvement of psychological symptoms (n = 17, 43%), increased understanding of their own disorder (n = 15, 38%), and strengthened self-concept or self-esteem (n = 11, 28%).
Blending scenarios
Patients described characteristics of the blending of online and FTF sessions (m = 8) and the therapist's activities to integrate the two elements (m = 3). Additionally, they highlighted the importance (m = 3) and specific features of the online sessions (m = 16) and FTF sessions (m = 10). Patients also provided insights into the blending rhythm, including how the ratio and sequence of online and FTF sessions were structured (m = 6), who determined the blending rhythm (m = 3), and their evaluation of it (m = 2). In total, m = 32 (63%) key themes were identified in this category.
The majority of patients reported that online content was discussed during FTF sessions (n = 31, 78%) and that both the content of online and FTF sessions referred to each other (n = 27, 68%). One-third perceived a reciprocal enrichment between online and FTF sessions (n = 14, 35%) and noted that therapy seemed to continue between FTF sessions (n = 11, 28%). Therapists were observed to have played a role in selecting suitable online sessions (n = 31, 78%), providing guidance (n = 30, 75%), and coordinating the BT (n = 16, 40%). About half of the patients considered FTF sessions more important than online sessions (n = 21, 53%), while others perceived both elements as equally important (n = 17, 43%).
The key features and contents of the FTF sessions from the patients’ perspective included personal contact with the therapist (n = 37, 93%), addressing individual and acute problems (n = 31, 78%), fostering a change of perspective (n = 17, 43%), reflecting on, deepening, and repeating therapeutic content (n = 13, 33%), and learning and applying practical exercises and homework (n = 12, 30%). Additionally, the limited session duration (n = 10, 25%) was mentioned as a key feature of FTF sessions.
According to the interviewed patients, the key features and contents of the online sessions included fictional patient examples (n = 26, 65%), flexible and location- and time-independent use of the online sessions (n = 24, 60%), psychoeducation (n = 20, 50%), reflection and repetition of therapy content (n = 16, 40%), use of diverse media formats (n = 14, 35%), variable duration of online sessions (n = 14, 35%), practical exercises (n = 13, 33%), lack of personal contact (n = 13, 33%), self-directed, active engagement (n = 12, 30%), and lack of individualization of the online sessions to patients’ needs (n = 10, 25%).
Regarding the implementation of the blending rhythm, and independent of their study group, approximately half of the patients reported that their treatment followed either a flexible blending rhythm (i.e., no predefined or regular sequence of online and FTF sessions; n = 23, 58%) or a regular sequence of online and FTF sessions (n = 18, 45%). Nearly one-third of all patients experienced an equal ratio of online and FTF sessions (n = 12, 30%). Both a flexible (n = 20, 50%) and a regular (n = 17, 43%) blending rhythm were considered advantageous. The decision-making process regarding the blending rhythm was reported to be led by the therapist (n = 17, 43%) or through joint decision-making (n = 12, 30%).
Therapeutic alliance
Facilitators (m = 4) and barriers (m = 3) to the therapeutic relationship were identified, with a total of m = 4 (57%) key themes emerging. Regarding interpersonal aspects and communication, positive (n = 32, 80%) and negative (n = 18, 45%) themes were mentioned. Additionally, patients reported agreement with therapeutic procedures and the therapists’ behavior (n = 14, 35%), as well as favorable organizational and treatment conditions (n = 11, 28%).
Negative effects
Patients reported themes related to negative effects of the BT (m = 2), FTF sessions (m = 4), and online sessions (m = 5), identifying a total of m = 4 (36%) key themes. Most patients perceived no negative effects from the BT (n = 26, 65%), FTF sessions (n = 22, 55%), or online sessions (n = 22, 55%). The only negative effect mentioned by ≥ 10 patients was emotional distress caused by the online sessions (n = 13, 33%).
Fit
We identified m = 10 themes related to patients’ fit with the treatment, with m = 7 (70%) key themes emerging. Half or more of the patients highlighted the relevance of content that is tailored to their individual needs (n = 26, 65%), the indication and contraindication of specific symptoms (n = 21, 53%), and the need for flexibility in the treatment (n = 20, 50%). Additional factors included self-discipline and drive (n = 15, 38%), basic skills such as written self-expression (n = 14, 35%), socio-demographic characteristics like age (n = 10, 25%), and technical knowledge and equipment (n = 10, 25%).
Facilitators and barriers of treatment adherence and engagement and daily life transfer
Patients identified facilitators (m = 15) and barriers (m = 9) of treatment adherence and engagement and the integration of BT into daily life. Out of these, m = 9 (60%) facilitators and m = 4 (44%) barriers emerged as key themes.
The majority of patients mentioned therapeutic guidance (n = 33, 83%) and self-discipline and drive (n = 29, 73%) as crucial facilitators for both adherence and engagement as well as implementation of treatment into daily life. Other facilitators included hope for improvement (n = 20, 50%), perceived symptom improvement and achievements in BT (n = 14, 35%), location- and time-independent flexibility (n = 14, 35%), and structured treatment elements and processes (n = 14, 35%). A sense of commitment, such as agreements with the therapist (n = 11, 28%), was mentioned as a specific facilitator for treatment adherence and engagement. Meanwhile, learning and applying practical exercises (n = 20, 50%) and utilizing therapeutic materials (n = 11, 28%) were identified as specific factors aiding daily life integration.
Common barriers included limited time and life circumstances (n = 18, 45%), lack of drive (n = 16, 40%), and symptom-related difficulties, such as behavioral patterns linked to the existing disorder (n = 13, 33%). A specific barrier affecting daily life integration was difficulties implementing learned strategies (n = 14, 35%).
Usability
Patients identified facilitators (m = 4) and barriers (m = 4) related to the usability of the BT, resulting in m = 5 (63%) key themes. Key facilitating factors included patients’ ability to independently manage BT demands or challenges using own (technical) skills (n = 25, 63%), receiving support from the therapist, social environment, or technical assistance from the online platform provider (n = 23, 58%), and patients’ technical affinity (n = 18, 45%). Key barriers involved technical problems with the online sessions (n = 20, 50%) and feelings of being overwhelmed by difficult or demanding treatment tasks (n = 17, 43%).
Optimization possibilities
Patients reported preferences regarding the blending rhythm (m = 3) and suggestions or wishes for optimizing the blending approach (m = 6), FTF sessions (m = 1), and online sessions (m = 9), leading to the identification of m = 5 (26%) key themes. Some patients expressed a preference for more FTF sessions within BT (n = 23, 58%), while others favored a balanced ratio of online and FTF sessions (n = 16, 40%). Half of the patients preferred a regular blending rhythm similar to the one used in the FIX study group (n = 20, 50%), whereas others preferred a more flexible approach (n = 13, 33%). The only key theme for optimizing other aspects was the customizability of online sessions in terms of lengths, content, or scope (n = 13, 33%), with some patients expressing a desire for additional online materials or more detailed or shorter online sessions.
Differences between the FIX and FLEX study groups
Across most key themes, FIX and FLEX patients reported these key themes with generally similar frequencies (Table 3). However, several key themes were reported by at least five more FIX patients than by FLEX patients (difference of at least 25%). These included the advantages of a regular blending rhythm (85% FIX vs. 0% FLEX), the implementation of a regular sequence of FTF and online sessions (80% vs. 10%), a preference for a regular blending rhythm (75% vs. 25%), therapist-led decision-making regarding the blending rhythm (60% vs. 25%), a preference for a balanced ratio of online and FTF sessions (55% vs. 25%), therapist reinforcement of participation (75% vs. 50%), and self-discipline and drive as a key factor in patients’ fit with the treatment (50% vs. 25%).
Several key themes were reported by at least five more FLEX patients than by FIX patients. These included advantages of a flexible blending rhythm (95% vs. 5%), implementation of a flexible blending rhythm (95% vs. 20%), the experience that therapy continued between FTF sessions (45% vs. 10%), a preference for more FTF sessions (75% vs. 40%), and a preference for a flexible blending rhythm (50% vs. 15%). Additionally, FLEX patients more often mentioned practical exercises and homework as part of FTF sessions (45% vs. 15%), the expectation that online sessions provide psychoeducation and deepen content (40% vs. 10%), the treatment effect of gaining a better understanding of the disorder (50% vs. 25%), discussing online content during FTF sessions (90% vs. 65%), and experiencing overload as a barrier to the intervention's usability (55% vs. 30%).
Discussion
This qualitative interview study conducted as part of the PSYCHOnlineTHERAPY study investigated the experiences of 40 participants across two versions of BT. It examined patients’ motivations and expectations regarding BT, the blending of online and FTF sessions and their roles and functions in BT, as well as key factors influencing the implementation and perceived effectiveness of BT, based on the Efficiency Model of Support. 41 Additionally, the study elucidated potential negative effects of BT.
Main findings
Patients reported more positive expectations than negative ones, aligning with previous research on BT acceptance. 19 Therapist behavior, specifically in encouraging participation, emerged as a crucial motivating factor, potentially influencing patient uptake of BT. Previous studies have shown therapists’ positive attitudes and high acceptance of BT21,22,24 that might play a significant role in motivating their patients in BT. It is possible there is an interaction between therapists’ attitudes and patients’ own motivation and willingness to use BT, which are both highlighted as key facilitators from the blended therapists’ perspective. 23
In line with previous findings, 47 nearly all patients emphasized the importance of personal contact with the therapist during FTF sessions. This contact allowed individual and acute needs to be addressed and encouraged fostering of new perspectives, which were features not reported for online sessions. These findings align with patients’ frequent mentions of positive aspects of the therapeutic alliance, supporting previous research on a positive and strong working alliance in BT. 48 Therapeutic guidance also emerged as a key facilitator for patient engagement and for integrating BT into the patients’ daily life, and support from others was a strong facilitator in enhancing the usability of BT. This result is consistent with other qualitative studies, which noted that connections with the therapist and supportive relationships motivated patients to persist with BT, 49 and that the therapist was important in supporting patients’ use of the online platform. 50 The importance of contact and support is further corroborated by quantitative research, which shows significant effects of guidance on the effectiveness and adherence of IMIs. 51 Therefore, compared to stand-alone IMIs or IMIs with low levels of guidance, the BT modality itself might be beneficial by including FTF contact with a therapist. Specific factors - especially therapist-related ones, such as the therapeutic alliance—can further facilitate or hinder engagement, as other previous findings indicate. 18 However, as our and previous research18,23,29 shows, other factors, such as patient characteristics, perceived treatment outcomes, and treatment-specific features, should also be considered as facilitators and barriers. These factors might play a role not only in patient engagement but also in a successful implementation of BT in the other categories (fit, knowledge, usability, implementation) influencing treatment effects, as outlined in the Efficiency Model of Support. 41
In their expectations and experiences with online and FTF sessions patients noted distinct advantages and disadvantages. Our results suggest that time constraints in FTF sessions could be compensated by the highlighted location- and time-independent flexible use and the variable duration of the online sessions. The interviewed patients noticed actual specific benefits (e.g., FTF: personal contact, online: flexibility) and disadvantages (e.g., FTF: time constraints, online: no personal contact) of both BT elements, and not only expected these characteristics, as our findings on expectations and prior research have shown.32,52 The respective advantages (e.g., of FTF sessions) seem to compensate for the limitations of the other element (e.g., of online sessions). This corresponds with previous work identifying patients as perceiving advantages and disadvantages of FTF and online elements as complementary. 53
Moreover, across the interviewees’ statements on the characteristics of the two elements, it appears that some content is specifically suitable for each modality, like fictional patient examples and psychoeducation in the online sessions, or individualized topics in the FTF sessions. This aligns with insights from a Delphi study involving therapists and patients with varying experience in online therapy, which found that FTF and online elements were both considered appropriate for certain therapeutic content. 30 However, content perceived as appropriate for both elements (cognitive techniques, practical exercises) possibly promotes reciprocal referencing between FTF and online sessions and the repetition and deepening of content. The results on online and FTF sessions characteristics from the interviewed patients’ perspectives imply that each seem to be essential core components of BT, with some content uniquely appropriate to each element, but may also serve supplementary functions and have overlapping content, as described in other studies. 18 A meta-analysis on BT by Nunes-Zlotkowski et al. (2024) suggested that supplementary BT (e.g., FTF as the main component and online sessions supplementary without new content, eight studies) may be more effective than designs with FTF and online sessions as integrated core elements (e.g., both elements indispensable, delivering unique therapeutic content, five studies). 18 In contrast, our findings show that the unique features of both elements are reflected as core components in the subjective change mechanisms, underscoring the importance of both FTF and online elements for the perceived BT's effectiveness in our interviewed participants.
Our findings on the implementation of the blending suggest that the combination of online and FTF elements has the potential to enrich treatment as most patients reported an active interplay between these elements, with reciprocal referencing or blending itself seen as a beneficial feature with positive treatment effects. Our results indicate that the online sessions are not merely conducted as a supplement to FTF therapy (or vice versa), but rather that a significant change of treatment, with integration and interaction between the two elements occur (e.g., incorporating online content into FTF sessions and blending activities of the therapist, like selecting suitable online sessions). This aligns with findings from a qualitative study, where therapists and patients noted that the integration of online elements positively transformed FTF therapy. 33 The combination of the two elements allows for leveraging their respective benefits, and their interaction may result in additional advantages, such as more intensive treatment or further deepening of therapeutic content. However, preferences for the ratio of the elements varied. About half of the patients felt that FTF sessions were more important than online sessions, with more than half expressing a preference for having more FTF than online sessions. This preference was particularly expressed in the FLEX group, suggesting that the (regular) FTF contact with a therapist is an important element of BT, especially for patients receiving a flexible BT format. This could reflect a greater need for structure through the therapeutic guidance or the therapeutic contact as an important active component of BT. However, a conflicting finding of a meta-analysis indicates that a lower ratio of FTF sessions versus online sessions is associated with higher effect sizes. 18 Preferences of patients seem to be diverse, with some participants valuing both FTF and online sessions equally or favoring a balanced ratio in this interview study. Other studies found that most patients prefer an equal ratio or more online than FTF sessions, 30 that actual BT session ratios vary between patients and primary and secondary care, 20 and that therapists might favor more FTF sessions. 23 Along with a range of optimization suggestions (each mentioned by only a few patients), our findings indicate that other factors might influence how BT should be implemented. Variables such as specific symptoms, the need for flexibility, socio-demographic characteristics, and individual skills and abilities—factors previously highlighted in research23,31—may play a role in shaping preferences and the fit between patients and the treatment.
Overall, the main differences between the two BT versions, FIX and FLEX, primarily concerned themes closely related to the actual implementation of the versions, such as patients’ descriptions of the implemented blending rhythm and their preferences in this regard. Apart from these aspects, our findings indicated largely similar patient perceptions of the two versions, e.g., regarding treatment effects, characteristics of the treatment elements, facilitators, and barriers. Other factors may have been more influential in determining how patients perceived BT, such as how individual therapists implemented the assigned BT version. It is also possible that patient experiences were shaped more by shared characteristics of both versions, such as the use of online sessions per se, than by version-specific features. In existing BT formats, an alternating design (as implemented in the FIX group) is chosen more often than a case-to-case design (as implemented in the FLEX group). 18 However, our results show that patients emphasized advantages of both intervention groups, as the FIX condition might offer more structure, whereas the FLEX condition allows for adaptation of the blending rhythm to better suit individual needs. Patients’ preferences may be shaped based on their experiences with a specific implementation of BT. However, other factors might also play a role in preferentially choosing one of the two formats. For example, patient characteristics such as individual life circumstances and the need for flexibility, as well as therapist-related factors such as the therapists’ time capacities for offering FTF sessions (e.g., weekly, bi-weekly, or at irregular intervals) might be decisive. In this context, our results of comparing FIX and FLEX imply that the therapist may play a more important role in an alternating (FIX) design that may require more time capacities, while the time between FTF sessions (e.g., with exercises) might be more important in the FLEX blending rhythm.
Limitations
This study involves certain limitations. First, our sample was self-selected, limiting the representativeness of patients in the intervention groups of the PSYCHOnlineTHERAPY study. Nevertheless, all eligible patients at the time of this qualitative study were invited, achieving a high response rate of 49.4%. We excluded participants enrolled during the first months of the study due to technical problems with the online platform, as their inclusion might have biased the results. Patients who dropped out of BT before the interview invitation was sent (4.7%, n = 4/85) could not be included as they did not respond to the interview invitation. This may have resulted in an overrepresentation of favorable patient experiences in the data. However, some of the interviewed participants did report discontinuing online sessions during the interviews. While these participants were not formal dropouts, their experiences have provided insights into negative aspects and potential barriers regarding the engagement with the online sessions.
Second, we deviated from the study protocol by adopting a different theoretical model for the interview guide and deductive analysis approach. As outlined in the study protocol, 34 the initial plan was to use the Unified Theory of Acceptance and Use of Technology model. 54 Instead, we decided to choose the Efficiency Model of Support as the theoretical basis, as this model was particularly suited to the study of BT in its consideration of the interaction with a support figure (the on-site therapist in our case) and incorporation of multiple dimensions crucial for the implementation of BT.
Third, the final independent coding of the interview material yielded only weak to moderate inter-coder agreement. Despite extensive training, numerous consensus meetings, and the coders’ familiarity with the coding system, achieving higher agreement proved challenging. This was likely due to the large number of research questions, theme codes and detailed categories that were not further generalized to preserve essential information, the broad range of interview topics, or the different professional qualifications of the coders.
Fourth, we found that 30% of the patients in the FIX group did not receive the predefined alternating session rhythm of FTF and online sessions, limiting our possibility to compare these two BT formats. However, a considerably larger proportion of patients in the FIX, compared to the FLEX group received alternating FTF and online sessions, and there were also missing data as we had to rely on the therapist's session reports.
Fifth, due to the large number of 163 theme codes, only the main themes based on the predefined selection criterion are discussed in detail. An overview of all identified theme codes can be found in Additional file 4.
Lastly, data saturation remains uncertain, as some theme codes were mentioned by only one patient. This reflects the wide and diverse range of patient experiences but also shows that we might have obtained different results with more interviewees.
Implications and future research
We identified factors, such as fit and active components and mechanisms of change, that could serve as moderators or mediators in randomized controlled trials to determine who benefits from BT and which mechanisms drive treatment outcomes. 55 As prior research shows,20,23 personalization emerges as a key theme and reflects patients’ diverse preferences. Although research on outcome moderators in BT, as well as in IMIs 56 and FTF treatments,57–59 is still limited, therapists can tailor BT to the patients’ preferences, such as the need for flexibility or the desired BT version (FIX vs. FLEX) and ratio of online and FTF sessions. Existing recommendations on implementing BT, such as reviewing specific requirements (e.g., writing skills, motivation, internet access), can provide valuable insights. 31 Given that both BT versions were positively evaluated and largely comparable in terms of patient experiences, it seems warranted to pursue both formats in practice. Future research should further examine differential treatment effects of these BT versions to inform personalized treatment allocation and support the improvement of BT approaches. Our findings imply that important elements and advantages of FTF sessions (e.g., sufficient therapist contact and guidance) and online sessions (e.g., psychoeducation, symptom normalization by including fictional examples, stimulating self-management) should be given greater consideration in further development of BT and the practical application of the elements. Additionally, addressing negative expectations, adverse experiences, and perceived barriers also seem crucial. Although most participating patients did not report negative effects from BT, emotional distress due to online sessions and technical difficulties were commonly mentioned. Therefore, providing technical support and troubleshooting is essential to ensure the quality and further development of the offered BT. Potential negative effects of BT should be carefully investigated and managed with appropriate procedures, as these issues can also arise in stand-alone FTF treatments and IMIs.60–62 Finally, comprehensive therapist training23,29,50,63 is vital to ensure high-quality BT delivery, as the therapist, the therapeutic attitude towards BT, and the therapists’ BT implementation skills appear to be central components of successful BT.
Conclusion
The study revealed overall positive evaluations of BT, with interviewed patients reporting a variety of positive outcomes and more positive expectations and facilitators than negative expectations and barriers. Specific advantages of both online and FTF sessions were highlighted, with each potentially compensating for the other's limitations, underscoring the value of integrating both elements. Comparing the two BT versions, both variants appear to offer advantages from the patients’ perspective, with only minor differences across the investigated aspects of BT implementation. Thus, both flexible and fixed approaches should be pursued in further BT research, as the choice between variants may depend on various patient- and therapist-related factors that warrant further investigation. Overall, the therapist emerged as essential in successfully implementing BT. Understanding the diversity of patients’ preferences and the suitability of certain types of content for specific modalities allows for the future optimization and personalization of online and FTF sessions, as well as their integration in a blended manner. Further, the study demonstrated the transformative potential of combining these two modalities, suggesting that BT may provide added benefits beyond stand-alone FTF treatments or IMIs. By identifying key barriers and facilitators, our extensive results provide a basis for further practical implementation and research on BT in outpatient care.
Additional files
Additional file 1 (AdditionalFile1_COREQ-Checklist.pdf): Consolidated criteria for reporting qualitative studies (COREQ): 32-item checklist
Additional file 2 (AdditionalFile2_InterviewGuide.pdf): Interview Guide (translated form German)
Additional file 3 (AdditionalFile3_NonInterviewedSample.pdf): Sociodemographic and clinical characteristics of the non-interviewed sample.
Additional file 4 (AdditionalFile4_OverallResults.pdf): Overall results of the qualitative content analysis (n = 40) with all 163 theme codes and their frequencies, definitions, and supporting quotations.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251377943 - Supplemental material for Patients’ perspectives on implementing fixed and flexible variants of blended therapy in routine care: A qualitative study of the project PSYCHOnlineTHERAPY
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251377943 for Patients’ perspectives on implementing fixed and flexible variants of blended therapy in routine care: A qualitative study of the project PSYCHOnlineTHERAPY by Theresa Sextl-Plötz, Ingrid Titzler, Juliane Schmidt-Hantke, Mira Denninger, Lena Sophia Steubl, Harald Baumeister, David Daniel Ebert and Anna-Carlotta Zarski in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076251377943 - Supplemental material for Patients’ perspectives on implementing fixed and flexible variants of blended therapy in routine care: A qualitative study of the project PSYCHOnlineTHERAPY
Supplemental material, sj-pdf-2-dhj-10.1177_20552076251377943 for Patients’ perspectives on implementing fixed and flexible variants of blended therapy in routine care: A qualitative study of the project PSYCHOnlineTHERAPY by Theresa Sextl-Plötz, Ingrid Titzler, Juliane Schmidt-Hantke, Mira Denninger, Lena Sophia Steubl, Harald Baumeister, David Daniel Ebert and Anna-Carlotta Zarski in DIGITAL HEALTH
Supplemental Material
sj-pdf-3-dhj-10.1177_20552076251377943 - Supplemental material for Patients’ perspectives on implementing fixed and flexible variants of blended therapy in routine care: A qualitative study of the project PSYCHOnlineTHERAPY
Supplemental material, sj-pdf-3-dhj-10.1177_20552076251377943 for Patients’ perspectives on implementing fixed and flexible variants of blended therapy in routine care: A qualitative study of the project PSYCHOnlineTHERAPY by Theresa Sextl-Plötz, Ingrid Titzler, Juliane Schmidt-Hantke, Mira Denninger, Lena Sophia Steubl, Harald Baumeister, David Daniel Ebert and Anna-Carlotta Zarski in DIGITAL HEALTH
Supplemental Material
sj-pdf-4-dhj-10.1177_20552076251377943 - Supplemental material for Patients’ perspectives on implementing fixed and flexible variants of blended therapy in routine care: A qualitative study of the project PSYCHOnlineTHERAPY
Supplemental material, sj-pdf-4-dhj-10.1177_20552076251377943 for Patients’ perspectives on implementing fixed and flexible variants of blended therapy in routine care: A qualitative study of the project PSYCHOnlineTHERAPY by Theresa Sextl-Plötz, Ingrid Titzler, Juliane Schmidt-Hantke, Mira Denninger, Lena Sophia Steubl, Harald Baumeister, David Daniel Ebert and Anna-Carlotta Zarski in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to thank all PSYCHOnlineTHERAPY project members of Clinical Psychology and Psychotherapy and Institute of Databases and Information Systems at Ulm University, Clinical Psychology and Psychotherapy at Friedrich-Alexander-Universität Erlangen-Nürnberg, Psychology & Digital Mental Health Care at Technical University of Munich, MEDIVERBUND AG, AOK Baden-Wuerttemberg, Bosch BKK and the collaborating professional associations MEDI Baden-Wuerttemberg e.V., Freie Liste der Psychotherapeuten and Deutsche Psychotherapeutenvereinigung, as well as all those who have contributed to and worked on the project. We also thank all student assistants who supported the study and all patients and therapists who participated.
The authors wish to thank Janna Fröhlich (JF) and Lucille Mayer (LM) for conducting the interviews. The authors thank Katharina Bößer (KB) and Leonie Ley (LL) for the transcription of the interviews and their participation in developing the coding system. Further, the authors wish to thank Luz Morczinnek (LM), who was involved in the development of the final coding system and as an independent rater in the analysis. We also thank Sebastian Deutscher, who assisted in the preparation of the quantitative data. Further, the authors wish to thank Hannah Rudat, who assisted in the development of the coding system, Dora Forisek and Anne Neuhaus, who were involved in the translation of the coding system, and the study team for their engagement in the study administration. The authors wish to thank all the interview participants.
ORCID iDs
Ethical approval
The study was approved by the ethics committee of the German Psychological Society (BaumeisterHarald2020-07-29VADM, date of approval: September 23, 2020).
Consent to participate
All participants gave written consent to participation.
Consent for publication
All participants gave written consent to publication.
Contributorship
All authors (TS, IT, JS, MD, LSS, HB, DDE, AZ) have made substantial contributions to the design of the study. TS, IT, and AZ developed the interview guide. TS was responsible for the recruitment of participants, the coordination and collection of interview data, the analyses, and the development of the code system. IT and AZ provided feedback on the code system. AZ supervised the trial management. TS drafted the manuscript. All authors contributed to the further writing. All authors read and approved the final manuscript.
Funding
The project PSYCHOnlineTHERAPY on which this publication is based was funded by the Innovation Committee (Innovationsausschuss) of the Joint Federal Committee (Gemeinsamer Bundesausschuss) with the funding code 01NVF18036. The funding source had no role in the study design, data collection and analysis, interpretation of the results, writing of the manuscript, or decision to submit this article for publication.
Declaration of conflicting interests
AZ receives royalties for a digital health application (DiGA) for sexual dysfunction implemented in routine care in Germany. She reports having received fees for delivering presentations at scientific conferences and for producing expert videos for a DiGA. DDE has served as a consultant to/on the scientific advisory boards of Sanofi, Novartis, Minddistrict, Lantern, Schoen Kliniken, Ideamed, and German health insurance companies (BARMER, Techniker Krankenkasse) and a number of federal chambers for psychotherapy. He is also a stakeholder in an institute for health training online (formerly GET.ON, now HelloBetter), which aims to implement scientific findings related to digital health interventions in routine care. HB reports to have received consultancy fees, fees for lectures or workshops from chambers of psychotherapists and training institutes for psychotherapists, and license fees for an Internet-intervention. LSS reports to have received fees for workshops on Internet- and mobile-based interventions. IT reports to have received consultancy fees, fees for lectures or workshops from training institutes for psychotherapists and doctors, as well as from scientific conferences. TS, MD, and JS report no conflicts of interest.
Data availability
The qualitative interview material analyzed during the current study is not publicly available due to data privacy reasons, as individual participants might be identified from the material. The interview guide (see ![]() ) and the generated code system (see Additional file 4) are included in this published article.
) and the generated code system (see Additional file 4) are included in this published article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.