
Abstract
Introduction
In an era where geographical distance has become a barrier to equitable access to health services, an intelligent needs assessment of medical specialties is the key to enabling effective telemedicine. A systematic needs assessment of medical specialties is the cornerstone in designing a telemedicine roadmap. This study aimed to identify and prioritize key specialties based on needs-based criteria for the development of telemedicine in the community covered by Shiraz University of Medical Sciences.
Methods
This study's methodology was modeled on the “need-based planning framework for telemedicine services” developed by the University of Queensland, Australia. A mixed approach was used in the study design. In the first three steps, quantitative and qualitative data were collected to identify the community's specialized medical needs. In the fourth step, the identified needs were prioritized.
Results
A total of 11 specialties, including neurosurgery, cardiology, general surgery, general internal medicine, orthopedics, pediatrics, neurology, psychiatry, obstetrics and gynecology, imaging, and urology, were identified as key priority specialties needed for the development of telemedicine in the community covered by Shiraz University of Medical Sciences. These specialties were prioritized into eight ranks based on need-based criteria.
Conclusion
By identifying and prioritizing 11 key medical specialties, this study has laid a valuable foundation for the development of telemedicine services. Its findings provide policymakers with an effective guide to strategically allocate resources toward prioritized specialties, enhance technological infrastructure, and implement relevant educational programs, thereby ensuring equitable access to services and taking a significant step toward advancing justice in healthcare.
Keywords
Introduction
Telemedicine is the delivery of healthcare services and the exchange of medical information across distances using electronic communication technologies.1–3 Key modalities include store-and-forward (asynchronous), where patient data or images are sent to providers for later review, commonly used in dermatology and radiology3,4; remote patient monitoring, which employs devices to track patients’ health and transmit data to providers, particularly for chronic disease management4,5; and real-time interactive services (synchronous), which enable live video consultations for immediate interaction and diagnosis.3,4
The World Health Organization strongly supports telemedicine to improve healthcare accessibility and quality. 6 However, numerous studies highlight the significant challenges and complexities of telemedicine within existing healthcare systems.7–11 Telemedicine has been adopted across numerous medical specialties, including dermatology, psychiatry, cardiology, endocrinology, neurology, pediatrics, and chronic disease management, with its suitability and effectiveness differing by clinical context.12–15 Delivering care through telemedicine necessitates a distinct set of competencies and skills compared to traditional in-person practice; therefore, clearly identifying which specialties are most suitable for telemedicine is essential for developing targeted educational and training programs for healthcare professionals.16,17 In this context, systematically determining the professions and clinical scenarios best aligned with telemedicine facilitates the optimization of patient outcomes, enhances access to care, and improves patient satisfaction, while also addressing challenges related to technology adoption, regulatory compliance, and provider preparedness.5,16,18
Multiple studies highlight telemedicine's suitability across healthcare professions, with nuanced decision-making influenced by patient factors, clinical needs, and technological access. A Veterans Health Administration study during COVID-19 revealed that telehealth modality choices (video vs. telephone) depended on patient preferences, health status, and technology capabilities, prioritizing video for visual assessments and telephone for accessibility, while emphasizing telehealth's role in reducing burnout and infection risk, despite perceptions of inferiority to in-person care. 19 In specialized care, an app-based self-monitoring system paired with nurse follow-up achieved 80% adoption, 87% adherence, and high user satisfaction due to its low burden and personalized feedback. 20 A Kuwaiti survey of 421 providers found 42.3% preferred telemedicine, 88.5% rated it moderately to highly useful, and qualitative interviews identified acceptance, training needs, and systemic barriers, underscoring broad support for integration into national healthcare. 21 Collectively, these findings demonstrate telemedicine's multi-faceted applicability, driven by context-specific clinical, technological, and provider readiness factors.
Telemedicine should be driven by community needs, not simply driven by technological advances. Conducting a thorough needs assessment before implementing this technology will identify gaps and unmet needs in healthcare systems, which is critical for optimizing access, efficiency, and equity in healthcare. 22 Numerous studies have explored telemedicine's applicability and adoption factors across healthcare, yet a critical and often overlooked gap persists: aligning telemedicine services with the specific, localized needs of communities. Existing research often focuses on feasibility and user acceptance and neglects systematic and community-based needs assessments. Therefore, to address this research gap and provide innovative insight, this study, inspired by a need-based planning framework of the University of Queensland, Australia, seeks to identify and prioritize medical specialties to reflect the real needs of the community covered by Shiraz University of Medical Sciences and provide a comprehensive basis for the development of telemedicine services. This approach not only propels the advancement of telemedicine grounded in community-driven needs assessments rather than technology-centric assumptions but also enriches academic understanding, guides policymakers and healthcare providers in the strategic allocation of resources, and ultimately bridges the divide between telemedicine's theoretical potential and its practical clinical impact in the real world.
Literature review
The literature on telemedicine and new healthcare technologies has expanded substantially, reflecting a dynamic and rapidly evolving field that integrates advanced digital tools to enhance healthcare delivery. Adoption and implementation of telemedicine and digital health technologies are best understood through established theoretical frameworks. Technology acceptance model (TAM) posits that adoption of digital health technologies is primarily influenced by perceived usefulness and perceived ease of use, which shapes user attitudes toward acceptance. The unified theory of acceptance and use of technology (UTAUT) expands on TAM by incorporating social influence and facilitating conditions, emphasizing the role of external factors and the user environment in adoption decisions. 23 Meanwhile, the diffusion of innovations theory explains technology adoption as a process driven by communication channels, time, innovation characteristics, and social systems, highlighting how innovations spread through early adopters to the wider population. 24 Recent research, building on these models, offers nuanced insights into the factors shaping digital health technology adoption. A study by Ankhwaldi emphasizes the importance of IT infrastructure, including Internet-enabled devices and facility readiness, in enhancing user confidence and adoption of contactless healthcare technologies. 25 Another study integrates task-technology fit, TAM, Internet of Things (IoT) concerns, and social incentives, demonstrating that perceived usefulness and attitude strongly influence IoT healthcare adoption, mediated by ease of use, security, and social influence. 26 Dbesan et al. reveal that performance expectancy, effort expectancy, social influence, facilitating conditions, and trust significantly drive physicians’ adoption of knowledge-sharing-driven blockchain technology in government hospitals. 27 Similarly, Alkhwaldi shows that behavioral intentions toward business intelligence systems are affected not only by traditional UTAUT constructs but also by medical–legal risk, rational decision-making culture, and perceived threats to professional autonomy. 28
In line with these theoretical frameworks, recent advances in artificial intelligence (AI), the IoT, and Big Data are substantively enhancing telemedicine's diagnostic precision, patient monitoring, and population-level health management. It has been shown that the diagnostic accuracy of AI in virtual primary care is high, with substantial concordance observed between AI-generated and provider diagnoses for acute conditions, especially those related to eye and urinary symptoms. The findings underscore AI's potential to enhance diagnostic decision-making and patient triage. 29 The integration of the IoT with cloud computing significantly enhances remote patient monitoring by enabling continuous, real-time data collection, storage, and processing through connected sensors and advanced networks such as 5G. 30 Cloud computing, AI, and the IoT have emerged as critical enablers in managing large datasets, providing real-time insights, and supporting telehealth delivery. Telemedicine's integration with Big Data has significantly enhanced its capabilities, allowing for the collection, processing, and analysis of vast amounts of patient data in real time. Furthermore, the combination of these technologies supports continuous monitoring and predictive analysis, allowing for earlier diagnosis and more proactive intervention in chronic disease management; ultimately, population health outcomes are better managed and improved. 31 For example, predictive models using Big Data have been shown to improve the management of chronic diseases such as diabetes, heart disease, and cancer by identifying risk factors and suggesting personalized interventions.31,32 However, challenges such as data privacy and security concerns, interoperability between healthcare systems, and scalability limitations persist. Additionally, gaps remain in the application of Big Data for mental health monitoring and underserved populations. 31
Beyond technological advancements, the global adoption and effective implementation of telemedicine also hinge on a complex interplay of socio-political and infrastructural factors. In recent years, telemedicine has witnessed widespread global adoption, driven by advances in digital health technologies and the urgent need to expand healthcare access across diverse populations. 33 The success of telemedicine globally depends on a delicate balance of factors, including strong government and political support, robust technological infrastructure, and clear legal frameworks. Equally important are public acceptance, skilled human resources, and effective coordination among stakeholders. 34 Studies from different regions—including America, Europe, Asia, and Africa—have consistently reported these factors.34–36 However, it should be noted that these elements vary in emphasis in different regions and are inherently shaped and changed by subtle regional social, cultural, informational, and geographic differences. 37 However, common barriers persist worldwide, including disparities in technology access, regulatory gaps, privacy concerns, outdated infrastructure, policy support and reimbursement limitations, technical skills, and digital literacy challenges, the severity of which varies depending on regional socio-economic and political contexts.27,38,39 The policy implications emphasize the need for binding ethical guidelines and legal regulations to ensure telemedicine balances technological benefits with responsible care, patient privacy, and equitable access, especially for aging and underserved populations.40,41
Complementing these implementation factors, extensive evidence highlights telemedicine's clinical effectiveness and economic benefits across diverse healthcare settings. Telemedicine is generally as effective as face-to-face care, with 83% of effectiveness reviews supporting its clinical benefits, including improved glycemic control, reduced hospitalizations, and enhanced management of chronic conditions. Also, about 39% of cost-effectiveness reviews indicated telemedicine can be cost-saving/effective. In addition, telemedicine has improved patient access, satisfaction, and engagement, particularly by overcoming geographical barriers. Provider workload was also optimized in some cases due to reduced time per consultation and more efficient care delivery.42,43
Method
The research methodology of this study was modeled after the “Needs-based Planning Framework for Telemedicine Services” developed by the University of Queensland, Australia. 22 In the first three steps, both quantitative and qualitative data were collected to identify the specialized needs of the community. In the fourth step, the identified needs were prioritized. This process resulted in a comprehensive needs assessment and precise ranking, providing a clear reflection of the real needs of the target community and establishing a solid foundation for the development of telemedicine services.
This study has been conducted in full compliance with the ethical standards established by the National Ethics Committee in Iranian Biomedical Research and has received formal approval under the code “IR.SUMS.NUMIMG.REC.1402.044” on July 15, 2023. All research methods were rigorously implemented in accordance with prescribed regulations, official guidelines, and ethical principles. Written informed consent was obtained from all participants through a written question included in the interview guide prior to the start of the interview.
In terms of study design, this is a comprehensive study that uses a mixed-method approach (quantitative–qualitative) to assess the needs for the development of telemedicine. It is founded on the recognition that effective telemedicine implementation should be driven by community needs rather than technological advancements. The study aimed to assess genuine community needs using quantitative and qualitative data, ensuring a multi-dimensional perspective on telemedicine development. In the quantitative phase, analysis was conducted using data generated by information systems to identify trends, uncover gaps in service delivery, and reveal potential demand for telemedicine interventions. This established a data-driven foundation for understanding current healthcare needs and guiding telemedicine development. Additionally, during the qualitative phase, structured interviews were conducted with medical professionals specializing in the fields identified in the quantitative phase. These interviews enriched the list of community needs for telemedicine development by capturing human-centered perspectives and identifying priority areas. To enhance clarity and methodological transparency, Figure 1 presents a detailed visual representation of the mixed-methods design flow.

Needs-based planning framework for telemedicine services.
Step 1: expressed need
The objective of this step was to assess the need for medical specialties within the community covered by Shiraz University of Medical Sciences. Which specialized medical services did patients need but had to seek outside their local area? Two outputs were expected in this step: a list of hospitals and the specialties available at each hospital based on referral rates.
Data source: Utilization of data from the Medical Care Monitoring Center (MCMC) system, the most comprehensive registry for patient referral information. Data collection tool: A customized data extraction form from the MCMC system was designed and used, capturing details such as the names of both referring and receiving hospitals, referral frequency, and referral rationale (required specialty). Sampling method: A census approach was adopted, analyzing all referrals recorded in the MCMC system. Analysis: Key hospitals were identified based on referral frequency, and medical specialties were determined using referral frequency and the area under the normal distribution curve (mean + standard deviation; specialties exceeding this threshold were identified as having the highest referral frequencies). In this way, the most critical destinations and specialties for patient transfer were determined.
Step 2: accessibility
In this step, the overall accessibility status was determined based on key indicators including travel time, travel distance, frequency of trips, and transportation costs. The two expected outputs of this phase were: (1) A comprehensive list of primary referral destination hospitals, categorized by distance, travel time, referral frequency, and referral costs. (2) Calculation of an accessibility index derived from these criteria to assess service reachability.
Data source: The number and destinations of patient referrals were determined using data extracted from the first step of the study. Travel distances and durations were calculated using Google Maps, and finally, cost estimations were based on reimbursement information from governmental programs (officially approved ambulance tariffs). Data collection tool: A data extraction form including the number, distance, time, and cost of referrals was used to refer patients from origin to destination. Sampling method: Since the data analyzed in this step—including trip frequency, travel distance, travel time, and transportation costs—are based on the number of patient referrals obtained in the first step, which a census sampling method was employed, the sampling approach in this step remains consistent with the first and is likewise considered a census.
Analysis
The assessment of specialized service accessibility at main referral hospitals was conducted using a simple additive weighting (SAW) method, a prevalent multi-criteria decision-making (MCDM) technique. SAW was selected after careful consideration of alternative MCDM approaches (e.g. technique order preference by similarlity to ideal solution, analytic hierarchy process) because of its conceptual simplicity, ease of implementation in geographic information system, suitability for integrating heterogeneous criteria in spatial accessibility analysis, and transparent aggregation process, which facilitates straightforward interpretation by both experts and stakeholders. 44 In this study, the accessibility index was determined based on four criteria: number of patient referrals, distance, time, and referral cost. Considering the nature of the different units of the criteria (km, min, IRR, number of referrals), normalization was performed prior to applying weights, and for this purpose, the standardization method based on the mean and standard deviation was employed. SAW ranks alternatives by assigning weights to criteria and aggregating normalized values, enabling comparative prioritization based on each criterion's relative importance. Higher composite index values in this study indicate greater priority and suitability for establishing telemedicine centers. 45 The expert panel, comprising physicians, administrators, and researchers, assigned a weight of 0.40 to the patient referral frequency criterion, with 0.20 allocated to each of the remaining criteria. This panel emphasized that referral frequency is a direct indicator of achieved access and successful utilization of care, whereas distance, time, and cost serve as barriers or enablers. Furthermore, the use of patient referrals as a primary access indicator is well established in health services research.46,47 This weighting is also justified by Andersen's Behavioral Model of Health Services Use, which conceptualizes utilization (such as referrals) as the ultimate outcome of access barriers and facilitators.45,48
It is important to emphasize that the foundational assumptions of the SAW method were critically considered to ensure methodological rigor. Given that the additive structure of SAW inherently assumes independence among criteria and permits compensatory trade-offs—where a lower score in one criterion can be offset by a higher score in another—special attention was devoted to the weighting process. 45 Although this assumption may not always hold in real-world contexts, the present study explicitly addressed it through the careful selection of criteria and the application of expert-informed weighting. This approach ensured a valid representation of each factor's relative importance and minimized potential sources of bias.
Step 3: expert perception of required medical specialties in the target community
This step aimed to establish a comprehensive understanding of the community's critical needs through expert interviews, gathering their insights to refine and prioritize identified medical specialties. The key deliverables were finalizing the list of required specialties for the target community and assigning priority scores to each specialty based on expert consensus.
Data source: Interview with experts (including representatives from various medical specialties). Data collection tool: The data collection instrument consisted of an interview guide designed to achieve two primary objectives: the identification of the list of required medical specialties and their prioritization for delivery through telemedicine from the perspective of experts. The interview guide was developed by convening an expert panel, comprising clinical specialists, managerial professionals, and researchers. The interview guide was structured using sample questions drawn from the guideline titled “Needs-based Planning Framework for Telemedicine Services,”
22
which acts as the main methodological reference for this study. The interview guide included eight questions—seven addressing the first objective and one distinct question focusing on prioritization for the second objective. The questions aimed at identifying and completing the list of specialties requested the experts to specify the specialties to which they most frequently referred patients, as well as those from which they most often received referrals. Additionally, experts were asked to share their opinions on specialties they believed were needed by their patients but required travel or referral to access care. They were also invited to identify services they wished to see offered at Shiraz University of Medical Sciences, which are currently needed but unavailable. Furthermore, based on data from step 1, the specialties were categorized into two groups. The first group consisted of six specialties selected as priority specialties, determined by referral frequency and the area under the normal distribution curve (mean + standard deviation). The second group included five additional specialties ranked subsequently by referral counts, identified as lower-priority specialties with a potential for exclusion. After explaining this classification to the experts, their opinions were solicited regarding the list and the possibility of moving specialties from the lower-priority category to the higher-priority group. Whenever consensus was reached among the experts for such reclassification, the changes were implemented. Finally, an open-ended question was posed to collect all additional suggestions concerning specialties that should be considered for telemedicine implementation. After finalizing the list of specialties—derived from two data sources (step 1: referral counts and area under the normal distribution curve; step 3: expert interviews)—the final list, which included 11 medical specialties, was provided to the experts. They were then asked to prioritize the specialties solely based on perceived community needs, independent of any other considerations, by assigning ranks from 1 (highest priority) to 11 (lowest priority). Sampling method: A targeted approach and snowball method were used for sampling. The inclusion and exclusion criteria were as follows:
- Inclusion criteria: Employment in areas covered by Shiraz University of Medical Sciences, willingness to participate with informed consent, accessibility throughout the study, and possessing experience or knowledge relevant to the research topic were the inclusion criteria for this study. - Exclusion criteria: Participants were required to complete all interview questions to ensure the comprehensive collection of data; otherwise, they were excluded from the study. Additionally, if participants withdrew their consent at any stage of the study, they were removed from the research. The interview continued until data saturation was confirmed. - To determine the medical specialists to be interviewed, an expert panel was initially formed, comprising key policymakers and decision-makers at Shiraz University of Medical Sciences and members of this research team. The list of specialties selected by field was predetermined based on the first step of the research and the number of referrals in each specialty (based on the area under the normal distribution curve, specialties that crossed the threshold of mean + standard deviation were identified as priority specialties). Since the medical specialists were recruited from Shiraz University of Medical Sciences, a list of specialists in each selected field was also prepared. Based on the knowledge of the panel members, at least one person in each selected specialty who possessed knowledge and experience related to telemedicine and met the required inclusion criteria was introduced. As is common in snowball sampling, initial participants recommended colleagues whom they believed had relevant experience or knowledge, which naturally led to the observed distribution. Importantly, the inclusion of each new medical specialist in the study was guided by the principle of data saturation in each specialty, rather than predetermined quotas. Data collection from the perspectives of specialists in each specialty continued until no new information or insights emerged. This approach explains why the distribution of experts across different disciplines varied. As a result, the final number and distribution of 44 specialists in different specialties reflects the natural achievement of data saturation in each area, rather than arbitrary selection (six orthopedics, four pediatrics, three psychiatry, three general surgery, six general internal medicine, seven obstetrics and gynecology, five cardiology, five neurology, five neurosurgery). To address potential biases, we assembled a diverse panel of experts, including policymakers, decision-makers, and researchers, to balance perspectives and reduce individual bias. Snowball sampling was conducted using explicit inclusion criteria focused on selected medical specialties, thereby minimizing reliance on personal networks and selection bias. Additionally, data saturation was systematically achieved within each specialty to ensure comprehensive, representative insights and prevent dominance of any single viewpoint during subsequent steps. - Analysis: In this step, by analyzing expert interviews, the list of medical specialties was completed and priorities were determined based on their perspectives. Experts were selected based on the specialties identified in the previous step, and the interview process adhered to the seven-phase qualitative analysis framework—thematization, design, interviewing, transcribing, analysis, verification, and report preparation.
49
It is noteworthy that the summative analysis method was used for the analysis.
50
To ensure the generalizability, reliability, and validity of the interview findings, the four established criteria of Lincoln and Guba—including credibility, dependability, confirmability, and transferability—were applied.
51
Step 4: determining and prioritizing community needs
The objective of this step was to analyze the quantitative and qualitative data from previous steps to determine the priority medical specialties for the development of telemedicine in regions covered by Shiraz University of Medical Sciences. The expected outcomes of this step included finalizing the list of specialties and ranking them based on priority.
Data source: Using the data extracted from steps 1 through 3. Data collection tool: No data collection tool was applied at this step. Use of data extracted from previous steps. Sampling method: No sampling method was applied at this step. Use of data extracted from previous steps. Analysis: A comprehensive list, resulting from the needs assessment process (based on steps 1 to 3) and encompassing 11 medical specialties, was compiled. Each specialty was assigned a score according to three evaluation criteria, and an overall score was awarded based on the total of these three. This cumulative score provided a comprehensive indicator of the level of priority assigned to the community's need for telemedicine services in each medical specialty. Regarding the “expressed need” criterion, since, according to the referral system data, there were 33 specialized services, each specialty was ranked from 1 to 33 based on referral frequency. Ultimately, since 11 specialties were selected for this study, only the referral frequency ranks for these specialties were determined (further details in step 1). For the “accessibility” criterion, as previously explained, potential centers for launching telemedicine for each specialty were defined based on this measure. Specifically, for each medical specialty, the hospital with the highest number of accepted referrals pertaining to that specialty was identified as the potential telemedicine center, and the accessibility index for that specialty was likewise determined based on that hospital. Given that the 11 selected medical specialties accounted for the highest admissions of referred patients in the seven main receiving hospitals, each specialty, in terms of the accessibility index, received a rank between 1 and 7 (further details in step 2). With regard to the “priority ranking of specialties from the experts’ perspective,” the list of 11 selected specialties was provided to the experts, who were asked to rank them from 1 to 11 based solely on the perceived need within the community (regardless of other considerations). Therefore, for this criterion as well, each specialty was assigned a rank between 1 and 11 (further details in step 3). The overall score for each specialty was obtained by summing the scores from these three criteria. Since all three criteria were defined so that a lower rank indicated a better status, a lower overall score likewise indicated a higher priority and greater potential for implementing telemedicine. This total score, which represents the priority of each specialty for establishing telemedicine based on a comprehensive community needs assessment, ranged from a minimum of 3 to a maximum of 51.
Result
Expressed need/output 1: list of hospitals based on referral frequency
A total of 21,328 referral patient admissions were made, of which 15,291 were admitted to the seven main referral hospitals (Table 1) and another 6037 to 46 other hospitals (a long list of these hospitals is reported in Appendix Table 1; see it for more details). Namazi Hospital, with the admission of 6012 patients, has been recognized as the main referral center for patients under the coverage of Shiraz University of Medical Sciences. The hospitals of Shahid Rajaee, Shahid Motahari, Shahid Faghihi, Hazrat Qaem, Hafez, and Ghalb Al-Zahra ranked next, providing approximately 1000 to 2000 referrals annually.
List of hospitals based on referral frequency.

Expressed need/output 2: list of medical specialties based on referral frequency
Findings revealed that the highest number of referrals was allocated to six specialties: neurosurgery, cardiology, general surgery, internal medicine, orthopedics, and pediatrics. Neurology, obstetrics and gynecology, and psychiatry followed in subsequent rankings. It was also found that the specialties with the highest number of referrals were located precisely in the main referral hospitals (Table 2). Further details regarding the referral rates for each specialty at each hospital are provided in Appendix Table 2.
List of medical specialties based on referral frequency.

Accessibility/output 1: list of hospitals based on referral distance, time, frequency, and costs
Data related to this step was extracted from seven priority hospitals (Namazi, Shahid Rajaee, Shahid Motahari, Shahid Faghihi, Hazrat Qaem, Hafez, Ghalb Al-Zahra), which had the most inter-hospital referrals. Namazi Hospital, with the admission of 6012 referred patients, was identified as the largest and primary destination for referred patients within the regions covered by Shiraz University of Medical Sciences. The average distance from various referral origins to this hospital was 77.75 km, with an average travel time of 1:15. The average cost per referral amounted to IRR 8,610,089.844, and the total cost of referrals to this hospital reached IRR 43,005,516,050 (Appendix Table 3). The hospitals Shahid Faghihi, Shahid Rajaee, Shahid Motahari, Hafez, Ghalb Al-Zahra, and Hazrat Qaem, with 1861, 1841, 1646, 1369, 1312, and 1250 referred patients respectively, were ranked next in order. Additional information regarding each hospital is provided in Appendix Tables 4 to 9.
Accessibility/output 2: accessibility index based on main referral destination hospitals
Ultimately, using the MCDM method, the SAW model, the overall accessibility status was determined based on four criteria: number of referrals, distance, time, and cost. Given the differing units of the criteria (km, min, IRR, number of referrals), normalization was performed prior to applying weights using the standardization method based on the mean and standard deviation. Finally, the status of the access index was determined. It should be noted that higher accessibility index values indicate greater priority and a more favorable position for establishing a telemedicine center, whereas lower values reflect lower priority for such an establishment. Overall, the accessibility index calculated using the SAW method ranged from 0.79 for Namazi Hospital in Shiraz to 0.45 for Hafez Hospital in Shiraz. Based on the selected criteria, the evaluation of these factors in priority hospitals and the SAW analytical approach, the final results indicate that Namazi Hospital (SAW = 0.79) is the most optimal choice for establishing a telemedicine center in terms of accessibility. This analytical finding is partly rooted in the fact that this hospital has a significant gap—almost six times greater—in the criterion of the number of patient referrals compared to the other six centers. It is noteworthy that this gap pertains to the most important accessibility criterion, the number of referrals, which was assigned twice the weight of the other criteria in the SAW analysis. Hazrat Qaem Hospital (SAW = 0.68) ranks second. Other hospitals in Shiraz, including Shahid Faghihi, Shahid Motahari, Shahid Rajaee, and Ghalb Al-Zahra, follow in order, with very narrow differences in their rankings. Hafez Hospital (SAW = 0.45) holds the lowest accessibility index value, placing it last in priority for establishing a telemedicine center among the selected hospitals (Table 3).
Accessibility index in the main hospitals of the dispatch destination.

SAW: simple additive weighting.
Experts’ perception of the services needed/output 1: completing the list of specialties needed by the community under study
Following the previous steps of the research, the community's medical specialty needs were identified. These specialties, ordered by priority based on the number of referrals, included neurosurgery, cardiology, general surgery, internal medicine, orthopedics, and pediatrics. In this step, through the analysis of expert interviews, the list of priority specialties—initially identified in the previous step based on the number of patient referrals —was completed and finalized. Two specialties, neurology (proposed 18 times) and psychiatry (proposed 13 times), which were ranked lower in priority in the previous step based on referral numbers, were elevated to priority specialties based on expert opinions and were added to the final list. Additionally, experts were consulted through interviews to refine this list further. Based on the analysis of the interview results, three additional specialties—imaging, obstetrics and gynecology, and urology—were included in the final list (Appendix Table 10).
It should be noted that due to the inherent limitations of information systems in achieving comprehensive data coverage, there may be a divergence between real needs and expressed demand (which in this study is represented by the referral pattern recorded in the system). Such gaps may arise from human errors attributable to insufficient training, time constraints, heavy workloads, or unintentional inaccuracies, which may result in the omission of certain data 52 ; thus, while such referrals do occur, they are not reflected in the system's official statistics. Furthermore, there are instances when centers or individuals fail to enter data due to technical difficulties or disruptions in Internet connectivity. 52 Most significantly, the system registers only formal referrals between healthcare facilities. In practice, however, many patients are directed to specialists through informal channels—either by personal choice or upon recommendation from a physician or acquaintance—without following the official referral process. These informal referrals remain undocumented within the system, yet they likely account for a substantial proportion of the actual referral flow. 53 The methodological framework employed in this study, in an effort to comprehensively cover information and address the divergence between actual needs and expressed demand in the referral system, used interviews with medical specialties as experts aware of the real needs of the community as a tool to bridge the gap. This process ultimately led to the inclusion of three new specialties—imaging, obstetrics and gynecology, and urology—in the list, as well as refining the priority rankings of neurology and psychiatry.
Experts’ perception of the services needed/output 2: prioritizing the list of specialties from the experts’ perspective
In this prioritization process, experts were asked to rank the list of specialties for telemedicine delivery solely based on perceived community needs, disregarding other factors. Based on the analysis of the prioritization results, it was determined that, from the experts’ perspective, cardiology and internal medicine emerged as the top-priority specialties for telemedicine services by a significant margin. Neurosurgery, neurology, pediatrics, general surgery, and psychiatry followed with similar average scores and were ranked next in order of priority. Imaging, orthopedics, obstetrics and gynecology, and urology were subsequently ranked in the following positions (Table 4).
Prioritization of specialties for provision via telemedicine from the experts’ perspective.

Determining and prioritizing community needs/output 1: determining the list of selected specialties
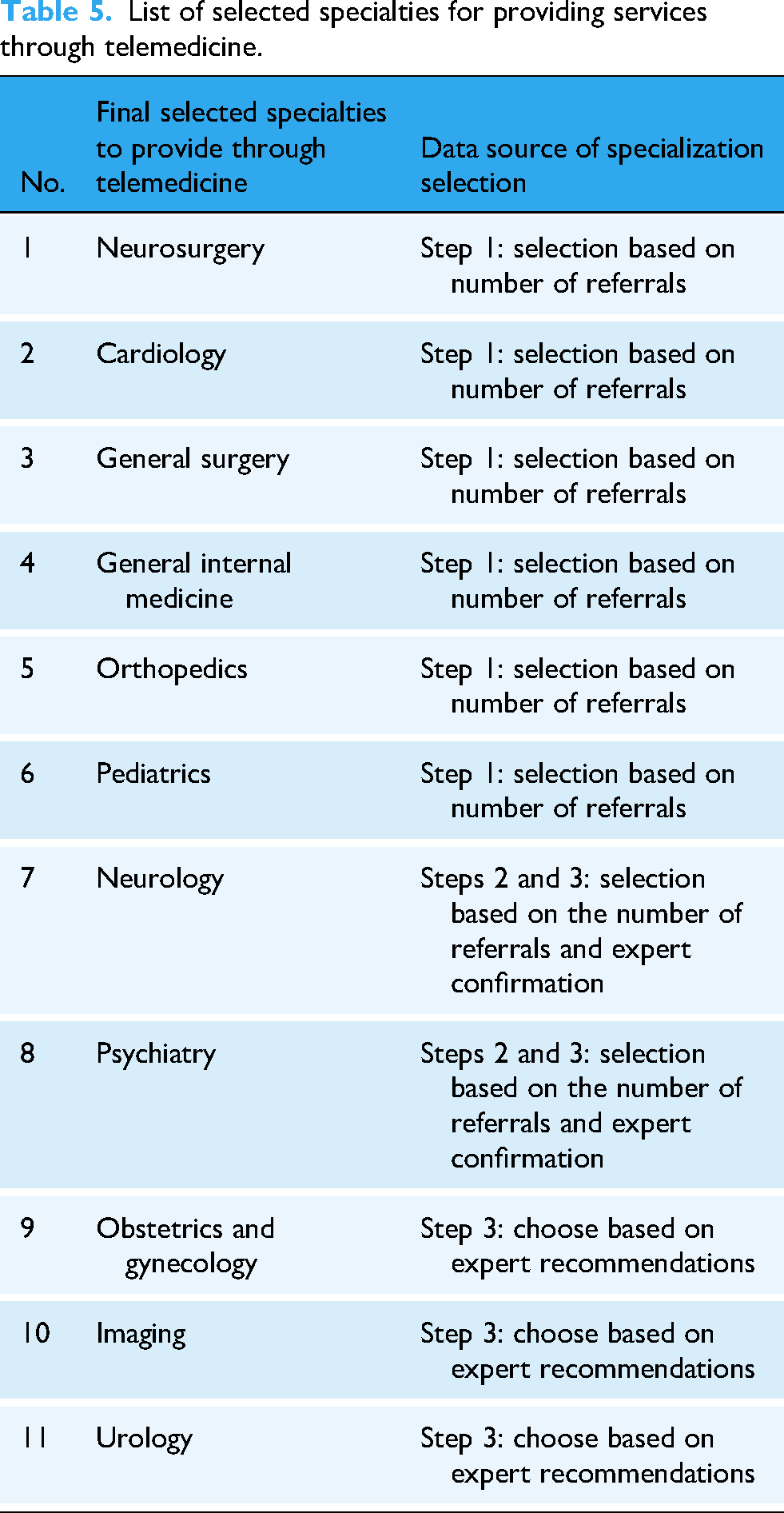
The final list of selected specialties for telemedicine delivery was identified based on three primary data sources. A total of 11 specialties were chosen, including neurosurgery, cardiology, general surgery, internal medicine, orthopedics, pediatrics, neurology, psychiatry, obstetrics and gynecology, imaging, and urology (Table 5).
List of selected specialties for providing services through telemedicine.
Determining and prioritizing community needs/output 2: ranking of the list of selected specialties
Ultimately, based on three criteria—expressed need, accessibility, and expert perception regarding specialty ranking—the specialties were prioritized in terms of the severity of the community's need. This ranking shows that internal medicine ranks first, followed by cardiology and neurosurgery, which rank equally. Pediatrics and neurology also have the same rank and are in the next positions. General surgery is next, followed by orthopedics and obstetrics and gynecology, which are similarly ranked. Finally, psychiatry, urology, and imaging are ranked next in order (Table 6).
List of selected specialties for providing services via telemedicine.

Discussion
This research commenced with a noble and practical purpose: to assess needs and prioritize key medical specialties for provision through telemedicine, as a bridge between limitations and needs for the community covered by Shiraz University of Medical Sciences. This study, through meticulous quantitative–qualitative data analysis and strategic needs assessment, outlines a clear pathway and a scientific-practical framework for telemedicine development. In this study, 11 prioritized medical specialties were identified, which, based on data analysis, were ranked across eight different levels. General internal medicine ranked highest due to its exceptional importance, while imaging held the final position. It is essential to emphasize that all the specialties identified in this needs assessment study hold significant importance and are prioritized above other specialties.
Internal medicine, securing the highest rank among the identified priorities, underscores the widespread necessity of establishing telemedicine. Evidence further substantiates this imperative: from the vital role of this specialty as a primary point of referral 54 to the efficacy of telemedicine in addressing behavioral health issues. 55 Additionally, the transformative potential of digital health technologies in enhancing care quality and managing chronic disease56,57 reveals the unparalleled significance of this innovation in meeting societal needs in this medical specialty.
Neurosurgery and cardiology were jointly ranked second in this needs assessment, likely due to their high expressed need indicator (patient referral). The referral patterns observed in this study, with an emphasis on specialties such as neurosurgery and cardiology, align with global trends, as these fields often require advanced care and are frequently subject to referral. 58 Telecardiology has established its position by reducing patient readmissions and improving treatment adherence, especially in the management of hypertension and heart failure.59,60 The integration of robotic surgery with telemedicine has also increasingly drawn attention to the need to develop this technology in these specialties due to its transformative role in increasing access to specialized services in underserved areas, despite challenges such as high costs and communication delays. 61
Pediatrics and neurology, ranked third in the needs assessment, highlight the critical importance of establishing telemedicine in these fields. Evidence indicates that telemedicine can play an important role in enhancing pediatric care, particularly in resource-limited areas, 62 where virtual medical evaluations have demonstrated considerable success. 63 In neurology, telemedicine has demonstrated its potential in transforming in-person healthcare into remote care over the past two decades and has been recognized as a response to ongoing societal needs. 64 General surgery ranked fourth, which may be due to the specialty's inherent dependence on physical examinations. 55
Orthopedics and obstetrics and gynecology were the next two specialties with similar scores in this needs assessment. In orthopedics, telemedicine has shown that it can facilitate continuity of care and expansion of services, responding to community needs for better access to this specialty. 65 In obstetrics and gynecology, telemedicine has also proven its role as a solution to critical community priorities by providing specialized services in underserved areas and reducing health inequalities.66,67
Psychiatry (ranked sixth) has had the highest acceptance of telemedicine use due to its speech-based nature and lack of need for extensive physical examination. 55 Psychiatrists consider telemedicine to be an appropriate response to the needs of this specialty and do not deem in-person visits necessary in most cases. 68 In urology (ranked seventh), the need to reduce in-person visits for elderly patients and mitigate the risk of nosocomial infections further underscores the necessity of telemedicine. However, meeting the needs of the community requires special attention to expert training and the development of clinical guidelines. 69 Finally, in the case of imaging (ranked eighth), the need for equitable access to diagnostic services, especially in underserved areas, has heightened the importance of telemedicine. This technology can play an important role in reducing health inequalities and enhancing equity in access to specialized services. 70
Strengths, limitations, and implications
This research has outstanding strengths, including utilizing a comprehensive and scientific process to assess the needs of medical specialties and drawing a precise framework to determine the specialized priorities needed by the community for the development of telemedicine. The use of a globally recognized framework in this study ensures a systematic, evidence-based identification of community healthcare needs, providing a solid and context-specific foundation for the strategic development of telemedicine at Shiraz University of Medical Sciences. Multi-dimensional analysis of data and a focus on community priorities with a scientific approach have added to the value and credibility of the results of this research. This approach, by grounding telemedicine development in a community-based needs assessment, aims to address genuine healthcare needs rather than relying solely on assumptions driven by technological progress.
However, the limitation of the generalizability of the results, which results from the study's focus on the population covered by Shiraz University of Medical Sciences, is a significant challenge. To address this limitation, it is suggested that future studies be conducted on a larger scale and in different communities to allow for generalization and comparison of results in a favorable manner. The mixed-methods framework employed in this study offers a robust and systematic approach for needs-based telemedicine planning that is broadly generalizable to diverse settings, as it integrates quantitative epidemiological data with qualitative stakeholder insights to capture comprehensive community health requirements. However, the specific prioritization of specialties reflects the unique epidemiological profile, demographic characteristics, and healthcare infrastructure, which may constrain direct transferability of the exact specialty ranking to other regions. Contextual factors such as population health profile and local burden of disease, distribution of specialized providers and hospitals, resource availability, referral patterns (in terms of referral distance, time, frequency, and costs), insight and attitudes of medical specialists, and existing technological capacity may influence the exact ranking of specialties, limiting direct transferability of specific priorities.22,71 Consequently, although priority specialties will vary across contexts, the methodological rigor and adaptability of this hybrid approach make it a valuable model for guiding telemedicine service planning across a wide range of geographic settings, particularly in resource-poor or rural areas, and within diverse health system types worldwide. Another limitation of this study concerns the criteria weighting process within the SAW method. The expert weighting process, while systematic, is subject to potential bias and subjectivity, which may influence the prioritization outcomes. Additionally, reliance on referral system data as a primary source may not fully capture all unmet healthcare needs within the community, potentially overlooking underserved populations or emerging demands. The use of Google Maps for travel time estimations, although practical, may introduce inaccuracies due to dynamic traffic conditions or mapping limitations. Future research should focus on developing and applying more robust consensus-building techniques, such as iterative Delphi methods with larger and more diverse expert panels, to minimize bias and enhance the objectivity of weighting processes. Expanding data sources beyond referral records to include comprehensive population health surveys, electronic health records, and community-based assessments will enable a more accurate identification of unmet healthcare needs, particularly among underserved groups. Furthermore, integrating advanced geospatial analytics employing real-time traffic data and validated transportation models will improve the precision of travel time estimations, thereby providing a more reliable measure of geographic accessibility. Finally, given that this study centers on needs assessment grounded in real-world data, future research may build upon its foundational findings to explore the feasibility of telemedicine in addressing the community's prioritized specialized service needs.
Having acknowledged the limitations of the study, it is essential to highlight the practical implications and potential applications of the findings in advancing the development of telemedicine. The prioritized specialties identified provide a strategic foundation for targeted resource and technology allocation, as well as educational planning in telemedicine services. General internal medicine emerged as the most suitable specialty for remote care, followed by neurosurgery and cardiology, while imaging and urology showed lower suitability. Policymakers can leverage the ranked specialties—such as internal medicine, cardiology, and neurosurgery—to effectively direct funding and human resources toward high-need areas, ensuring the optimal use of limited healthcare funds and maximizing the impact of telemedicine services. Applying a results-based planning approach, as endorsed by strategic resource allocation frameworks, would enable allocation decisions grounded in equity and population needs, aligning financial resources with the prioritized specialties to maximize healthcare outcomes in the region.72,73 In terms of technological infrastructure enhancement, the findings offer guidance on where to invest in telemedicine platforms, diagnostic equipment, and digital health tools. For example, equipping cardiology and neurosurgery units with advanced teleconsultation and remote-monitoring technologies would address the top-ranked specialties’ needs, facilitating timely specialist access and reducing geographic barriers in care delivery. Additionally, development of integrated telehealth networks tailored to the identified specialties can enhance interoperability, data sharing, and remote patient management capacities, thereby improving service quality and efficiency.74,75 Regarding educational programs, the prioritized list supports targeted curriculum development and continuous professional training to build competencies necessary for telemedicine deployment in these specialties. Initiatives such as specialized telemedicine training modules in internal medicine, simulation-based learning for remote examination techniques, and interdisciplinary workshops can strengthen provider readiness. Moreover, community education programs emphasizing utilization of telemedicine services in these prioritized specialties can promote patient engagement and acceptance. This focused approach ensures that workforce development aligns with the strategic specialty priorities identified in this needs assessment.74,76
Conclusion
This study emphasizes the importance of scientific needs assessment in identifying specialty priorities for telemedicine development. Internal medicine, as a first priority, shows a wide need to respond through telemedicine. Similarly, neurosurgery and cardiology specialties should also make important contributions to the provision of Internet-based care. This comprehensive needs assessment study has clarified the path for the development of telemedicine and provided a scientific framework to meet the vital needs of society. Determining medical specialty priorities is a fundamental step toward achieving equity in access to specialized services. It is recommended that policymakers in this field develop telemedicine programs by prioritizing the specialties identified in the results of this study. This measure not only covers the basic needs of society, but also plays an important role in reducing health inequalities by creating equity in access to specialized services.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251374215 - Supplemental material for Needs assessment and prioritization of key medical specialties: A telemedicine roadmap based on a mixed-methods framework
Supplemental material, sj-docx-1-dhj-10.1177_20552076251374215 for Needs assessment and prioritization of key medical specialties: A telemedicine roadmap based on a mixed-methods framework by Reyhane Izadi, Abdosaleh Jafari, Ali Goli, Mohsen Khosravi and Mohammad Amin Bahrami in DIGITAL HEALTH
Footnotes
Ethical approval
This study adheres to ethical standards outlined by the National Ethics Committee in Iranian Biomedical Research, with approval granted under code “IR.SUMS.NUMIMG.REC.1402.044” on 2023-07-15.
Consent statement
All participants provided informed verbal consent prior to the interviews and were free to withdraw from the study at any time.
Contributorship
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Guarantor
MAB serves as the guarantor for this paper, taking responsibility for the integrity of the work as a whole, including the accuracy of the data and analysis.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.