
Abstract
Introduction
Digital mental health interventions (DMHIs) can offer affordable, accessible and anonymous delivery of mental health treatment as an alternative or complement to face-to-face services. To enhance acceptability of, and treatment engagement with, youth DMHIs, they should be co-designed with young people and their caregivers. This study focuses on co-design with caregivers.
Objective
To explore caregivers’ perspectives, preferences, and ideas to inform the co-design of a digital youth mental health platform for anxiety and depression: ‘Momentum’.
Methods and Measures
Six group discussions were conducted with 16 caregivers of young people aged 7–17 years. In relation to Momentum, and DMHIs more broadly, participants’ views were sought on purpose and acceptability, access, assessments and feedback, information sharing, caregiver involvement and engagement. Data were thematically analysed using an inductive codebook approach, guided by template analysis.
Results
Seven themes were identified: (1) providing therapeutic and educational resources; (2) promoting shared and positive communication about mental health; (3) enhancing user experience and understanding; (4) facilitating personalisation and offering customisation of platform features; (5) encouraging end-user engagement through interactivity, incentives, relatability and attracting and maintaining attention; (6) enabling caregivers to provide support while promoting young people's independence; and (7) reducing concerns about, and enhancing trust in, DMHIs.
Conclusions
Participants expressed favourable views towards DMHIs and Momentum. They shared design ideas for a user-friendly, engaging, interactive, trustworthy, personalised and transparent platform that offered educational resources and mental health treatment. Two sets of recommendations were derived from the study findings: (1) recommendations for co-designing DMHIs with caregivers and (2) recommendations for the design of youth DMHIs.
Keywords
Introduction
Mental illness is the foremost cause of disability in young people, accounting for almost half of the global burden of disease for people between 10 and 24 years of age.1,2 It is known that 14% of 10-to-19-year-olds live with a mental health disorder. 3 Despite improvements in mental healthcare access over recent decades, the morbidity and mortality rates associated with mental health disorders among young people have increased or remained largely unchanged in the last 20 years.2,4 Indeed, the prevalence of clinically elevated depression and anxiety in young people in Western countries, such as the United States of America, have increased markedly over this period,5,6 and doubled since the start of the COVID-19 pandemic. 7 Surveys have found similar effects in Australia.8,9
Barriers to seeking, accessing and engaging with mental health services
Young people face several challenges to seeking, accessing and engaging with mental health services.10–12 Radez et al.'s systematic review categorised these barriers into individual, social, relational, and systemic and structural factors. 11 Individual factors include reluctancy to attend appointments, self-reliance (wanting to cope with problems without help from others) and a lack of knowledge about mental health and services (e.g. how to make an appointment).10–12 Limited knowledge about the symptoms and effects of mental health problems, coupled with uncertainty about the kinds of help available and how to access services, impede help-seeking behaviours in young people. 13 Social factors include perceived stigma, experienced or anticipated embarrassment, peer or family members’ attitudes towards mental health and help-seeking, and concerns about privacy and confidentiality related to the sharing of information with caregivers.10–12 While regulations vary between Australian States/Territories, there are minimum ages of consent for accessing mental health treatment. Further, health information may be shared with caregivers when younger people are of an age where they are deemed unable to provide consent. 14 Relational factors include concerns about the therapeutic relationship and sharing information with someone unfamiliar.10–12 Systematic and structural factors include the complexity of accessing services, costs of services, transport and geographical access, service inflexibility (e.g. accessing help outside of school hours), long wait times and a lack of culturally appropriate services.10–12 Radez et al.'s review found that some of these barriers were more likely to be reported by a specific gender or by people from culturally and linguistically diverse groups. 11
Digital mental health interventions
Digital mental health interventions (DMHIs) offer alternative and/or complementary treatment delivery that addresses some of the barriers to accessing face-to-face mental health services. DMHIs, such as websites, interactive platforms and digital apps, providing psychoeducation, mental health support and treatment have proliferated in recent years. 15 Benefits of DMHIs include preservation of users’ anonymity (addressing the influence of stigma on help-seeking behaviours); accessibility (addressing long wait lists, costs and limited access to mental health services, such as in rural and remote areas); and ease of use (addressing complexities of navigating public and private mental healthcare systems as well as busy family schedules).15,16 Preliminary evidence suggests that DMHIs incorporating cognitive behaviour therapy (CBT) principles can lead to improvements in mental wellbeing, mental health literacy and anxiety and depression symptoms in young people.17–20 Accessing mental health treatment via digital tools has been reported in the literature to be a facilitator of help-seeking behaviour. 11
Role of caregivers in youth mental health treatment and their views of DMHIs
Parents and other caregivers often play a significant role in helping young people address mental health problems. 21 In many cases, they are the first to recognise that a problem exists, offer emotional support, and enlist professional support services.22,23 They are also likely to assist in the logistics of accessing services, such as transport to appointments, and providing financial support to access services. The level of involvement caregivers have in youth mental health treatment may shift as children progress into adolescence and become more independent. 22
Caregivers have generally expressed satisfaction with, and positive attitudes towards, youth-focused DMHIs,24,25 as well as a willingness to access DMHIs for their child(ren)'s mental health problems. 26 While caregivers have endorsed benefits of DMHIs including accessibility, cost-affordability, earlier access to treatment, anonymity and interactivity,25,26 they also share concerns about data security, privacy27,28 and the impersonal nature of digital resources compared to face-to-face treatments. 29 Caregivers have communicated a desire for reliable, jargon-free information about youth mental health, delivered on digital platforms that are user-friendly and easy to navigate. 27
Some DMHIs offer parent programmes or modules that complement youth-facing programmes, for example BRAVE-Self-Help. 30 Parent end-users of BRAVE-Self Help have cited lack of time, competing priorities, uncertainty in their ability to complete the programme correctly and the severity of their child's condition as barriers to engaging with the programme. 30 However, parents also reported that having a platform that was supported by evidence and associated with reputable organisations (e.g. health service or education facilities); was user-friendly; and provided education on parenting skills and strategies motivated them to use the programme. 30 They further expressed the desire for personalised and relatable platform materials. 30
Caregivers’ involvement in the co-design of DMHIs
It is important that DMHIs are designed with end-users to ensure that interventions meet their preferences, needs and contextual factors. 31 Co-design involves meaningfully collaborating with potential end-users and other relevant stakeholders early and often in the design process. 32 Thabrew and Fleming 32 argue that partnering with end-users in co-design is likely to enhance DMHI uptake, engagement and user satisfaction. Caregivers should be involved in co-designing youth DMHIs, as they are a key source of support for young people, 33 helping them to access and engage with mental health services.22,23
Few studies have actively sought caregivers’ input in the initial design of youth DMHIs.29,31,34 Bevan Jones et al.'s recent review of digital youth mental health technologies identified only 30 DMHIs across 25 journal articles that had been co-designed with end-users, with less than half (37%) involving caregivers. 31 Some of these interventions targeted specific settings (e.g. schools 35 ), single mental health disorders (e.g. depression 36 ), or narrow age groups (e.g. adolescents aged 15–18 37 ). Other studies have reported on the co-design on DMHIs for parent use only.22,38
The current study
This study formed part of a larger research project aiming to co-design, develop, implement and evaluate a self-directed digital youth mental health treatment platform (a type of DMHI) called ‘Momentum’ that helps children and adolescents with anxiety and depression and other related aspects of their wellbeing (healthy lifestyles, substance use, sleep and help-seeking). Momentum was co-designed with young people (7–17 years old), their caregivers and clinicians. The current study reports on caregivers’ involvement in the co-design phase, with the findings from co-design workshops with young people
39
and clinicians separately. The study objective was to explore caregivers’ perspectives, preferences and ideas to inform the co-design of a new digital youth mental health platform (Momentum). The following research questions guided the study.
What do caregivers think the purpose of Momentum should be? What key features (content, function, design) do caregivers think would help ensure that Momentum is acceptable and useful to caregivers and young people? What are caregivers’ perceptions of the barriers to, and facilitators of, caregivers’ and young peoples’ engagement with DMHIs? What are caregivers’ perspectives on their involvement in Momentum?
Methods
Study design
This qualitative study involved dyads, triads and a focus group with caregivers of young people aged 7–17 years old. The research was guided by participatory and co-design practices, 40 which enabled participants to be actively involved in design processes and collaboratively contribute to decision making regarding the development of Momentum.
Participants and recruitment
Caregivers were eligible to participate in the study if (a) their child(ren) was participating in one of the youth co-design workshops and (b) their child(ren) reported current or past emotional problems, or (c) their child(ren) had experience using digital health or mental health programs or apps. Caregivers and their children were recruited via purposive, volunteer and convenience sampling methods. Participants were recruited until data saturation was reached, that is when participants were expressing similar ideas to those articulated in previous discussion groups, and there were limited novel data presenting. Some of the participants had a pre-existing relationship with members of the research team. Participants were allocated to workshops where they did not know the facilitator and all data were de-identified. Advertisements for the study were shared through social media, professional networks, and via Kids Helpline (an Australian national online and phone counselling service for people aged 5–25 years). Caregivers who were interested in participating in the study completed an online expression of interest and were contacted via email or telephone by a member of the research team.
Data collection, procedures and materials
Face-to-face dyads, triads and a focus group were held between December 2020 and February 2021 at one of three universities in Queensland, Australia: The University of Southern Queensland (Springfield), The University of Queensland (St Lucia) and Griffith University (Mount Gravatt). Informed written consent was obtained from all participants prior to data collection. The study comprised six 2-h group discussions: three dyads, two triads and a focus group (with four participants), collectively referred to as ‘group discussions’. Group discussions were facilitated by 1–3 facilitators from the research team with at least one facilitator in each group having experience conducting qualitative interviews and focus groups. Facilitators had completed an undergraduate level of study or higher in either psychology or speech pathology. At the start of each workshop, the facilitators explained the purpose and aims of the research project. The discussion guide is presented in Supplemental File 1 and covered the following topics in relation to Momentum and youth DMHIs: (1) purpose and acceptability, (2) access, (3) assessments and feedback, (4) information sharing, (5) caregiver involvement and (6) engagement.
Each participant received a $30AUD gift voucher at the end of the group discussion to thank them for their time. Participants were not informed prior to participation that they would receive a gift voucher to avoid the perception of coercion to participate. Group discussions were audio-recorded with participants’ consent and transcribed verbatim by a professional transcription service. Data were subsequently de-identified. After each discussion, facilitators produced reflective fieldnotes about their initial impressions of patterns in participants’ responses and the dynamics between participants.
Data analysis
Data were thematically analysed using a seven-step inductive codebook approach, guided by template analysis. 41 Two researchers (RB and KL) listened to audio recordings and checked them against the professional transcripts to ensure their accuracy, which facilitated familiarisation with the data. Three researchers (RB, KL and JR) then independently applied open coding techniques to the six transcripts using NVivo V12 and V20. The coding was double blinded so that each transcript was reviewed by two researchers. The three researchers worked together to develop a coding template (codebook) by comparing their independent coding, merging related codes, grouping codes based on similarities in semantic meaning and re-labelling codes. The codebook was applied to all six transcripts by pairs of researchers (RB, KL and JR), so that each transcript was coded by two researchers. The researchers met to discuss their coding and collaboratively made minor refinements to the codebook. KL, JKR, RLB and SM then generated themes by identifying connections between codes and higher-order abstract meaning in the data and re-reading transcript excerpts in the context of the codebook. Field notes were reviewed to check themes against facilitators’ initial impressions of findings and to identify any potential researcher bias in the interpretation of results. 40
Trustworthiness
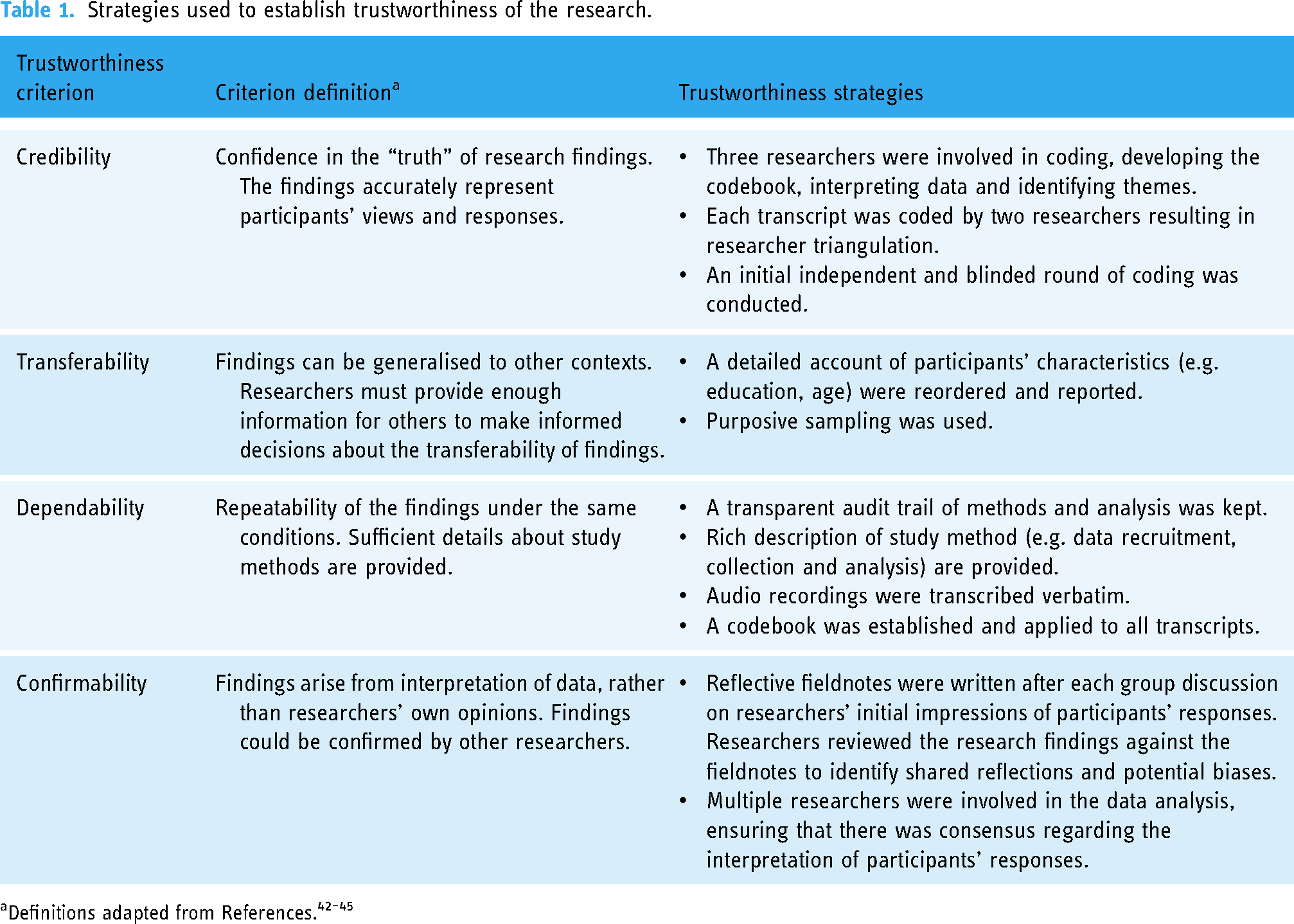
In qualitative research, trustworthiness of the research is achieved via credibility, transferability, dependability and conformability.42–45 Table 1 outlines specific strategies used to address trustworthiness and reduce researcher bias in the analysis and interpretation of findings.
Strategies used to establish trustworthiness of the research.
Results
Participant characteristics
Participants comprised 16 caregivers, aged 28–52 years (M = 43.33 years, SD = 6.80 years, with one caregiver's age unspecified). Participants were caregivers of young people simultaneously engaging in co-design workshops as part of the larger project. 39 Therefore, group discussions were held separately for caregivers of children (two dyads, one triad and one focus group; 11 participants) and caregivers of adolescents (one dyad and one triad; 5 participants). In this study, ‘children’ referred to young people aged 7–12 years and ‘adolescents’ referred to participants aged 11–17 years, with 11–12-year-olds electing to engage in children or adolescent workshops based on location or peer group (e.g. some participants completed workshops with their friends).
A quarter of participants (25%) were biological fathers, and 75% were biological mothers. Within the sample, 56.25% of participants endorsed that they had experience using a digital health or mental health platform in the past. All participants spoke English at home, with one caregiver speaking both French and English. No participant withdrew from the study. Demographic information is displayed in Table 2.
Participant demographic information.

Themes
Seven themes were identified relating to participants’ preferences and design ideas for Momentum: (1) providing therapeutic and educational resources, (2) promoting shared and positive communication about mental health, (3) enhancing end-user experience and understanding, (4) facilitating personalisation and offering customisation of platform features, (5) encouraging end-user engagement through interactivity, incentives, relatability, and attracting and maintaining attention, (6) enabling caregivers to provide support while promoting young people's independence and (7) reducing concerns about, and enhancing trust in, DMHIs. A description of each theme is presented in Table 3, followed by a detailed account of each theme and participant quotes. The group discussion that quotes originated from is denoted by the group discussion number (1–6) and the letter ‘A’ (caregivers of adolescents) or ‘C’ (caregivers of children).
Summary of themes.

Providing therapeutic and educational resources
Participants expressed that one of the main purposes of Momentum should be to provide education about mental health to both young people and caregivers. They discussed that DMHIs should provide psychoeducation for their children, including teaching them about skills to help manage their mental health. …thoughts linking to feelings is a really important skill they need to know about. So, diaphragmatic breathing and the thoughts–feeling link. (Workshop5A)
Participants also spoke about educational resources for caregivers that would serve to improve caregivers’ knowledge about their child(ren)'s mental health. This would assist caregivers in identifying when their child(ren)'s experiences required further support. They explained that they often struggled to find valid information to assist them in understanding their child(ren)'s experiences. …you don’t really know where to start or what to look for do you, you just say, this is my child and they're feeling this way, what do I do? I don’t know why they're feeling this way, I don’t know how to help them… (Workshop1C)
It was also suggested that Momentum could be an educational resource to guide caregivers’ responses to their child(ren)'s needs. This was discussed in relation to teaching caregivers skills to use with their child(ren) to help them manage any difficulties they experienced. Again, personalising that journey for the parents as well, saying okay, yes, you’re – you’re dealing with this – this emotional teenager, what can you do? These are the strategies that are going to help you, are going to help them learn how to cope with these situations as well. So you have sort of both parent and child learning the skills at the same time. (Workshop6A)
Participants discussed that Momentum should provide information for caregivers about where to go for additional help, or what to do in the context of a crisis. For example, if a young person was experiencing thoughts pertaining to suicide, caregivers wanted directive information about what steps to take next. Or even tell them about the emergency department if they’re really worried about the safety of their child, like it's not just for medical emergencies. A lot of parents don’t know that. They just think oh no, you have to be like medically wrong. Like you can’t just go there for mental health stuff. So telling them about that. (Workshop5A)
Promoting shared and positive communication about mental health
Participants viewed Momentum as a tool to promote shared and positive communication about mental health; this included child–caregiver, caregiver–child, child–other trusted adult(s), caregivers–caregivers, and child–friend(s) communication. Some caregivers expressed that it was not uncommon for young people to keep mental health difficulties to themselves or to only share information regarding mental health difficulties with their friends. They suggested that Momentum should contain information for young people about how to talk to their caregivers about mental health issues and how to help their friends who were experiencing mental health problems. How to help your friends if they’re in trouble and when to help them and when to break that silence, you know, when it's okay to break it … because they have this kind of you know, between us code of silence thing they may not realise when it's time to access an adult. (Workshop5A)
Participants identified that young people may have difficulty knowing when and how to reach out to adults for help, or who to reach out to. They recognised that not all young people have a safe adult within the family to turn to, and so having options for other support people was important. And maybe some options … because some people will be, not want to talk to their parent. So I think having some other options there is a good idea. You know, your mum's friend or your auntie or uncle. (Workshop5A)
Similarly, participants wanted to see guidance for caregivers about how to best approach conversations with their child about mental health, as well as where to seek external help once a line of communication had been established. Yeah, and what they might do with it … or how could they start conversations with their teen about it or where could they go from there. Like … who could help them work it out like maybe go to a – the GP [General Practitioner] … or at school like it's the, I don’t know, the year level coordinator or the guidance officer or … whoever else it is. (Workshop5A)
Another desired function of Momentum was the ability to share information with other caregivers, whose children may be experiencing similar mental health difficulties to their own. One suggested avenue to share this information was through social media platforms. Even what you’ve just read, or a video you watched…, and go okay I know these two people that are in my friends’ circle that it would be beneficial for them to watch this video or read this article and be able to just share it on my timeline … there's heaps of kids out there that need help, and there's lots of parents looking for it as well, like you don’t know where to go. (Workshop1C)
How Momentum communicated information about mental health difficulties was important to participants. They discussed that young people may feel alone in their mental health experiences and highlighted the importance of normalising mental health challenges and using de-stigmatising language throughout the platform. For some participants, it was important that mental health difficulties were not pathologised and young people were not overexposed to mental health concepts. These participants were not supportive of diagnostic labels such as ‘depression’ or ‘anxiety’ being used within the platform; rather, that various difficulties should be put forward as part of the human experience. I think, too, of trying to hit that fine line between educating people about symptoms, but not unnecessarily labelling them, because the last thing you’d want is for a kid to internalise a label or think, oh well, I have depression, and then internalising any negativity associated with it that it's probably better to talk about symptoms and that these are normal … (Workshop3C)
Enhancing end-user experience and understanding
Participants expressed a strong desire for Momentum to be easy to navigate, user-friendly and “simple” for both young people and caregivers. They suggested that this could be achieved through appropriate terminology, incorporating visual information with small amounts of text and a consistent layout. In addition, they advocated for language that is age appropriate, with many young people and caregivers needing simplified, jargon-free terminology. Participants also recognised young people's different learning and reading abilities, suggesting read-aloud options and videos. So that's also really helpful, just because you need to differentiate for those kids that don’t read so well … or also who listen more easily to instructions rather than reading them, so kind of different abilities there as well. (Workshop4C)
There was strong agreement that text should be kept short to enhance understanding and not overwhelm young people, and that text should be accompanied by visual information, particularly videos. Because my son's very visual, like he takes a lot in when he reads but he's very very visual. (Workshop1C)
Visual information was also requested for the presentation of caregiver feedback. Participants spoke about the value of graphs to display results (e.g. progress or norms). They agreed that information for caregivers should not be too long, but there should be options to find out more information. Like maybe in a graph – kind of form – of the things that they were worried about the most, or the things that they seemed to click on. (Workshop2C)
Some participants recognised the benefit of having a consistent layout, for example recognisable icons/buttons. This would facilitate familiarity with the platform and enhance useability. I feel it almost goes without saying, but I’ll just say it – is consistent method of navigation through the program … for a kid to be able to look at a new page that's got new information on it, but sort of already know the framework or how it works … and their attention and everything goes to the important points on the page, as opposed to trying to figure where they’re supposed to click next. (Workshop6A)
In terms of delivering the platform, there was a general consensus that Momentum should be accessible via computers and mobile devices. My girls would gravitate towards the app on an iPad. (Workshop1C)
Facilitating personalisation and offering customisation of platform features
Participants explained the importance of customisation of the platform to make it personalised to the individual user. Participants suggested that personalisation could be achieved via the customisation of avatars and backgrounds/themes; tailored content based on platform use; and age differentiation within Momentum. Customisation of avatars and backgrounds/themes was put forth as a way end-users could personalise their Momentum profile. For example, participants could create an avatar that represented the user. I think it would be good if they were able – the avatar was themselves, because then it's like they’re going through that, their avatar's going through it but it's actually them. (Workshop3C)
Customisation of avatars was also seen as a way to incentivise young people to engage with Momentum. Participants explained that young people could earn clothes and accessories for their avatar as a reward for completing treatment modules. I think the avatar should be quite simple in the beginning, and they need to earn rewards to change the avatar. Have an extra hat or different colour shoes or … just change it. (Workshop1C)
Participants expressed a desire for treatment content that was tailored to young people based on their answers to assessments or the way they interacted with the platform. So, you aren’t being bombarded by everything, but if ... the questions they answered all kind of stem towards bullying, then you would get some information about that. (Workshop2C)
A few participants suggested that tailored content could be achieved via artificial intelligence (AI) or algorithms. If you think you might have more significant concerns about anxiety, use a screening tool or whatever, and that could have an algorithm about whether or not then it would be appropriate to go onto a treatment module or something. (Workshop3C)
Throughout participant responses, there was recognition that the age of the young person should be taken into consideration, with responses often containing a variation of the phrase: ‘it depends on age group’. Participants expressed that language, visual information and content needed to be age appropriate. Some participants advocated for different versions of Momentum, or different sections within the platform, for different age groups. I think having sections for ages. So, and obviously, it’ll be tricky, but the way that you would deliver it to a 12-year-old versus an 8-year-old would be very different. (Workhop3C)
Encouraging end-user engagement through interactivity, incentives, relatability, and attracting and maintaining attention
Participants provided many different suggestions for engaging young people with Momentum. These strategies centred around four key concepts: interactivity, incentives, relatability, and attracting and maintaining attention.
Interactivity
Participants explained that one of the best ways to engage young people in Momentum was through interactive activities, rather than passive learning (e.g. reading a lot of text). They proposed that a game-like feel to Momentum activities would make the platform fun and facilitate learning. If it's a game-based learning, then they will gravitate towards it and stay there, rather than visit and go, oh I did all this reading or I just have to listen. Whereas if it's interactive and it's more of a game they will learn but also have fun and stick around and go back if they need to. (Workshop1C)
While there were differing opinions among the participants about the style of the videos (e.g. cartoon vs real people), there was consensus that use of scenario-based videos and storytelling would facilitate interaction. They can watch a video of two people interacting or a group of people interacting and there's a scenario that they can ask questions about too, so who do you feel is struggling here or who do you feel sorry for? (Workshop4C)
Other suggested interactive features included quizzes, journaling, tracking functions (e.g. emotional check-ins) and avatars. However, participants explained that some interactive elements, including cartoons, avatars and storytelling, would be more appropriate for younger children and less so for adolescents. It can’t be patronising. They hate it if something looks babyish, childish; they want to be mature … so yeah. (Workshop5A)
Incentives
Participants saw incentives as a way to motivate young people to use the platform. One of the main types of incentives suggested by participants was a reward-based system for completing treatment content, for example, points, coins, medals, collectable items or accessories for avatars. Like points, like gold coins or something when they’ve answered so many points. (Workshop2C)
The other main type of incentive was monitoring progression through the platform. Participants spoke about pathways, levels and maps, where young people's ability to track their progression and achievements would motivate them to continue to use Momentum. Yeah, and then like, there's a map, and you move onto a different map, and then when you finish that map, you go onto the next map, and so, it's a progression. (Workshop2C)
Relatability
Participants thought that engagement with Momentum would be enhanced if young people could relate to people portrayed on the platform (e.g. characters, avatars, and people in videos). Having a little person who they can decorate and make their own, the way that they see themselves or they want to be portrayed. (Workshop3C)
Some participants explained that videos should include people similar to the age of platform users so that they could identify with them. The issue of inclusivity was also mentioned by some caregivers of children; they explained that the platform needed to consider people from different cultural backgrounds and genders. When talking about representation in videos, one participant said: Understand that it's everybody, not just age or that gender or that nationality or cultural background, that it's everybody, it's [mental health is] quite normal and it's quite common and this is how we manage it together. (Workshop4C)
Attracting and maintaining attention
Participants spoke about the need for Momentum to attract and maintain end-users’ attention to prevent boredom and disengagement. The following strategies were given by participants to achieve this: using catchy phrases or short headings, featuring nature and animals, having a colourful and bright platform, including music and sound, incorporating humour and favouring visual information over big blocks of text. But yeah, that's the engagement. And jingles – music, jingles, flashing stuff, and colours, and changing - interactiveness, I guess. (Workshop2C) I think, for me – and I know my kids and also the way I work, is anything that's text-heavy, copy-heavy – lose interest straightway. (Workshop6A)
Participants explained that assessments in particular have the potential to lose young people's interest, especially if they were text-heavy and too long. To enhance young people's engagement with assessments, caregivers put forward ideas such as making them interactive, chunking text/questions into sections to reduce cognitive load and offering mini rewards or encouraging messages. … maybe in between some you could do the avatar thing where they go, “great work, you can now add clothes to your avatar” and then go onto the next lot to break it up, because I think then it might feel overwhelming if it's too many questions in a row. (Workshop4C)
Participants also explained that caregivers and young people have limited time, so they wanted registration and assessments to be easy and short. [They are] always complaining about “I’m too busy, I’m too busy.” So I think you might want to make it short, whatever like short bite-sized bits and tell them how long it's going to take. (Workshop5A)
Enabling caregivers to provide support while promoting young people's independence
Participants shared a variety of ways that they thought caregivers should be involved in Momentum, including monitoring platform use (e.g. keeping track of their child(ren)'s progress), encouraging their child(ren) to use the platform, receiving feedback about their child(ren)'s mental health, receiving summaries of learning modules and actively engaging in the platform with their child(ren).
While some participants felt that being informed of module content via summaries was sufficient, other participants explained that a high level of involvement with Momentum would allow them to encourage their child(ren) to use the skills they learnt from the platform, model skills within the home and monitor the child(ren)'s practice of strategies outside of the platform. … It just reminds me of a lot of these skills need to be modelled at home. So, in terms of making it a joint journey with the parents. (Workshop6A)
The desired level of involvement in Momentum also depended on the age of the young person using a platform. For example, some participants discussed the importance of assisting younger children to complete questionnaires, due to their developing emotional literacy. I think, ideally if the parent and child were doing that part together, it allows for more, I guess open transparent communication – it allows for bridging any kind of health literacy or emotional literacy gaps, and then they’re kind of on the same page. (Workshop3C)
While participants recognised that caregivers’ involvement may become less prominent with older adolescents, it was still important to support them through their use of the platform. You could have it if you registered, so that you could open it up and get an idea of the progress with the modules or whatever if you wanted, but not necessarily have to put in … tick every module off with them or anything like that. (Workshop6A)
Some participants recognised that their involvement in Momentum may negatively impact young people's disclosure in completing questionnaires about their mental health experiences. They expressed a preference for allowing young people agency in completing the assessment questionnaires if it meant them providing more honest answers. It depends, I think sometimes kids need to do it on their own, and they’re more comfortable answering honestly if they're by themselves without having mum and dad over their shoulder … so, if you want honest answers, I think it needs to be asked in a way that kids can answer all by themselves. (Workshop1C)
Some participants also spoke about the need to offer young people some level of privacy around their information, but this was dependent on the young person's age. So yeah, parents understanding that they need space and privacy as well is important, but I think for the little ones yeah, they need to be sharing stuff. (Workshop5A)
While opinions varied in the group about the level of involvement caregivers should have in Momentum, there was an overarching consensus that involvement had to be balanced with allowing young people their independence. This was in relation to completing assessments about mental health difficulties, as well as involvement in the learning material presented within the platform. … I think that's part of the problem … trying to get that balance between giving them independence but also supporting and I think sometimes it goes too far the other way. You just go and do that yourself when in actual fact that's what's needed … the parent is needed to help navigate some of that stuff. (Workshop5A)
There was a strong desire for receiving feedback about the results of assessments. Some participants expressed that they wanted information about whether their child(ren)'s results sat within normative ranges, and if not, instruction in how to their support their child. I wonder if that sort of thing would be a nice visual for parents to easily look at it and go oh phew, they’re in the average range or … they’ve got more depressive symptoms then the average teen … and maybe then some easy things you could do about this like immediately point to … spend quality time with your child. You know, stuff that they feel like they can do. (Workshop5A)
Reducing concerns about, and enhancing trust in, DMHIs
While participants expressed positive attitudes towards Momentum, they also communicated concerns about DMHIs. The most discussed concerns were around credibility, transparent information about Momentum, confidentiality of contact details and privacy of personal information. The credibility of Momentum was important to participants; they wanted to know that the platform was built on evidence and research. And just about what sort of treatment. Why? What's the treatment approach? Is there an evidence base, is there any sort of credibility or endorsement by someone else that's maybe recognised in the field as knowing what they’re talking about, or a symbol that sort of connects it with something reputable, so it's not just some like weird website? (Workshop3C)
Participants said that they were more likely to trust a DMHI if it was associated with a university or government and endorsed by a trusted source. Most participants explained that school-endorsement would give them trust in Momentum, with other sources including general practitioners, psychologists, organisations like Beyond Blue (Australian mental health and wellbeing support organisation) and caregivers’ peers. … Perhaps if it was linked to a university, or linked, sort of endorsed by some other organisation, like Beyond Blue - that would give it credibility. Yeah, associated with a university, or a statement by a psychologist or a psychological organisation, or a psychiatrist just makes it seem legit. (Workshop3C) Coming from teachers and – and being brought out by a university actually adds an air of authenticity that you can trust, I think. (Workshop6A)
One participant also expressed the importance of knowing that caregivers and children had participated in the design of Momentum. I’d want to see that it's been developed by clinicians and researchers and with input directly from parents, and kids that have been – experienced those things, maybe again having those logos from the university or from mental health foundation. (Workshop3C)
Participants discussed the need to have clear and accurate information about the platform that could help them decide whether Momentum was relevant to their child(ren). Several participants spoke about their child(ren) wanting to sign up to different apps or different apps being advertised, so they needed to be able to make quick and easy decisions about which digital websites and apps their child(ren) could access. So things like actually, as a parent wanting to know initially, is that is the right app for your child to be exposed to, and being able to determine that fairly quickly, without having to put a lot of effort in to figuring that out as a time-poor parent who doesn’t have time to sit there and analyse every app that my kids ask them to download … Being able to determine relevance pretty quickly is important to me. (Workshop6A)
Another main concern was around confidentiality of young people’s and caregivers’ information, for example contact information. Participants wanted transparency about what happens with information collected by Momentum to ensure that it was not shared with others. I guess we'd need to know where the information goes and who sees it … You would need to absolutely know that … there's nothing that can happen with information, I suppose. I think that's what most parents worry about. (Workshop2C)
While chat functions, cost and family dynamics were less commonly discussed topics, they were still concerns for some participants. Some participants expressed safety concerns around the use of chat functions and were wary about the sharing of inappropriate information, especially by people who should not be using the platform. Some kids go through really horrible experience and then they are hurting themselves or cutting or anything like that, you don’t want your kid to – who had never thought of it – all of a sudden go, oh that's an interesting way to deal with stuff, maybe I should do that. (Workshop1C)
A few participants brought up the issue of cost. While they were not against paying for Momentum, they wanted this information to be clear upfront. Does it cost anything? Not that I mind paying for things – I sound like I do, I don’t, but, if it's the right thing, but I just – I’m cautious of them clicking yes, yes, yes, yes and then you get this lovely bill. (Workshop4C)
When discussing requirements around caregiver consent to use the platform, some participants recognised the issue of different family dynamics or difficult family relationships, including abusive caregivers or divorced/separated parents. These participants suggested that young people should have the option to nominate another trusted adult (e.g. relative or school counsellor) who could consent to the young person using the programme and receive feedback on their assessments and progress. There was also a suggestion to include resources for young people who could not talk to their caregivers about their mental health, for example contact details for helplines. Crisis Line or whoever else it is that they can ring immediately. They don’t – if that parent is not a safe parent and that parent is actually the cause of a lot of the stress, then yeah, that child or teenager would need to have access to a safe place, so definitely resources there, but yeah, there's a duty of care. (Workshop4C)
Discussion
Summary of key findings
This study demonstrated caregivers’ unique insights into the intersection of their child(ren)'s technology use, behaviours, interests and mental health. While there were various ways participants envisaged caregivers being involved in Momentum, there was a general consensus that caregivers should seek a balance between supporting their children to use DMHIs while considering their independence. This balance is particularly important for adolescents who become progressively less reliant on family as they grow older, actively pursue autonomy and develop self-identity. In our related co-design workshops with young people, 39 participants discussed the benefits and pitfalls of caregiver involvement in DMHIs, with some adolescents expressing strong negative reactions to parents having access to information about their platform use. Previous studies have found that young people report concerns about obtaining caregiver consent to access mental health services (including digital interventions), particularly in relation to confidentiality.12,46 Young people suggested that Momentum should offer options for different levels of caregiver engagement suited to the individual.
Participants recommended that DMHIs should support positive interactions between young people and others, especially shared and positive communication about mental health. Choi et al. found that in their web-based programme ‘Stepping Stone’, parents were most satisfied with the session that provided strategies for promoting parent–child relationships. 38 Parents also wanted more practical parenting skills that could be applied in daily interactions with their children. 38 Similarly, participants in Clarke et al.'s study wanted caregiver-facing platforms to provide resources on communication skill development. 27 While some parents in Clarke et al.'s study thought a website should be developed for parents only, others requested an ‘all-inclusive’ website for both parents and young people to foster dialogue and create a shared approach to addressing mental health problems. 27 The dual functionality of Momentum will aim to facilitate communication between young people and their caregivers, and create opportunities for interactions relevant to youth mental health.
The other suggested key function of youth DMHIs was to provide therapeutic resources (e.g. calming and coping strategies) and education (e.g. about where to access help) for both young people and caregivers. Based on parents’ and mental health professionals’ perceptions of the limitations of existing parent education programmes, Choi and Kim recommend that caregivers’ psychoeducation should be interactive, structured, accessible and relatable while enabling opportunities for self-reflection. 47 The primary goals of Momentum proposed by study participants (fostering communication between young people and others, and providing psychoeducation) are consistent with Sobowale et al. who identified two key themes around the perceived usefulness of Internet interventions for youth mental health in Vietnam: sharing problems with others (social support) and learning about mental illness (psychoeducation). 48 This finding is further supported by Ho et al.'s systematic review of web-based mental health interventions for young people, where mental health education was reported as one of the most useful benefits of youth DMHIs. 49 This review also reported ‘connectedness’ with others as a common facilitator of youth engagement with DMHIs, including parents’ involvement in DMHIs. 49
Participants’ preferences and ideas for Momentum largely echoed the findings from our co-design workshops with children and adolescents. 39 Both caregivers and young people advocated for a DMHI that enhances the end-user experience, and is user-friendly, easy to navigate and simple. Usability has been emphasised by caregivers and young people as a vital feature of DMHIs.27,50,51 Interactivity and engagement were also important for both participant groups. Caregivers emphasised the need for DMHIs to gain young people's initial interest (attract attention) and keep them engaged throughout the programme (maintain attention). Participant-proposed strategies to achieve this include creating a game-like feel,51–54 offering rewards for completing treatment content, 28 using multimedia and visual elements, 52 and presenting treatment content through narratives. 55
Similar to young people in our research, 39 and caregivers and young people in other studies,30,50,52,56 caregiver participants wanted a DMHI that was customisable (e.g. customising avatars or backgrounds), relatable (e.g. diversity of characters) and personalised (e.g. age appropriate, tailored treatment). Some caregivers spoke about the merit of AI to personalise platform content. Caregivers in O’Dea et al.'s study conveyed apprehension about computerised algorithms in determining young people's needs, worrying that an automated process may over or under pathologise their child. 29 Some participants in our study also expressed concerns about DMHIs over-pathologising young people, highlighting the need for self-directed DMHIs to incorporate validated clinical assessments and evidence-based procedures for assigning treatment content.
Overall, participants expressed favourable attitudes towards Momentum and DMHIs more generally, although they shared concerns about privacy, trustworthiness and credibility. These concerns were shared by children and adolescents in our larger research project, 39 as well as caregivers in previous research.27,29,56 Participants put forth the following strategies to overcome their concerns: having an evidence-based platform that had undergone a formal research evaluation; endorsement by reputable and trusted sources (e.g. universities, schools, GPs); clear information about the platform prior to registration; transparency about data use; and co-design of the platform with end-users.
Recommendations
When designing youth DMHIs, researchers should consider caregivers’ potential role as both end-users and as gatekeepers. Study participants suggested a variety of ways in which they would want to interact with a DMHI: actively engaging with their child when using the intervention (especially for younger children); interacting with a caregiver version of the platform to receive feedback on their child's mental health and progress in the platform; and accessing educational resources and important contact numbers (e.g. helplines) through the platform. We also recommend that DMHIs should facilitate meaningful interaction between children and their caregivers, both within and outside of the platform, by providing conversation ‘starters’ around mental health topics for example.
Caregivers may act as gatekeepers for their children's access to mental health services 57 or digital technologies 58 and are likely to introduce children to DMHIs and encourage their use, further emphasising the importance of their involvement in the co-design of DMHIs. When conducting co-design workshops or focus groups with caregivers, we recommend allocating participants to groups based on their child(ren)'s ages to foster shared experience and relatability amongst participants.
A critical way to inform the role of caregivers in a DMHI is to involve them alongside children in co-designing. Even when it is anticipated that caregivers will not be directly involved in using the platform, they can provide unique knowledge about their child(ren) that is likely to enhance young people’s engagement with the platform and treatment content. In addition to recommendations for co-designing DMHIs with caregivers, we developed 11 recommendations for the design of youth DMHIs, based on our study findings (Textbox 1).
Researchers, clinicians and platform-designers need to strike a balance between what end-users envisage or want, versus what is feasible, appropriate and evidence-based. For example, some participants suggested non-guardians could consent to a young person using DMHIs, but this is likely inappropriate due to legal and ethical implications. Evans et al. refer to the need “to balance the desirable, the possible and the viable” when co-designing; we would add “the evidence-base” to this list. 59
Another consideration is that participants’ experiences with other digital technologies such as video/computer games, and knowledge of technologies capabilities (i.e. what technology can do), do not necessarily align with clinical expertise and evidence-based treatments. For example, participants expressed interest in using AI to modify the content end-users were presented with. However, given AI’s current capabilities, validated clinical assessments are more appropriate for guiding treatment. 60 Ecological momentary interventions (EMIs) offer an alternative to AI, as they are pre-programmed and non-generative, thus minimising risk. EMIs collect data in real-time on end-users’ interactions with digital tools to adjust content (e.g. by delivering prompts and alerts, or delivering feedback). 61 EMIs have previously been incorporated into digital mental health applications to personalise content. 61
Recommendations for the design youth DMHIs
1. Provide educational resources for both caregivers and children to enhance knowledge (e.g. where to access help and what do in a crisis) and skills (e.g. parenting skills and coping strategies for young people) relevant to mental health. 2. Deliver information and tools that foster communication between young people and prominent people in their lives (peers, caregivers and other adults). This could include offering conversation starters and advice for children and caregivers on how to approach difficult conversations around mental health. 3. Normalise mental health problems, for example, by using de-stigmatising language. 4. Ensure that DMHIs are user-friendly and easy to navigate. This could be achieved by using jargon-free and age-appropriate terminology, minimising the amount of text presented, having a consistent layout with recognisable menus and buttons, and making digital platforms accessible across different devices. 5. Incorporate multimodal elements such as videos, images and graphs to enhance understanding and avoid overwhelming end-users with too much textual information. 6. Allow for the customisation of features so that end-users can personalise the platform, giving them a sense of ownership (e.g. customising themes or avatars). 7. Tailor content to young people based on their answers to questions (e.g. assessments) or in how they interact with the platform (e.g. via artificial intelligence). 8. Facilitate engagement with DMHIs through:
• Interactive activities such as games, videos, storytelling and quizzes; • Incentives, for example, reward systems or tracking progression; • Relatability in terms of characters, diversity and representation; and • Attention-grabbing and attention-maintaining features such as bright colours, music/sounds, humour, visual elements, nature and animals. 9. Involve caregivers in a variety of ways, for example enabling them to monitor their child's platform use, receive feedback about their child's mental health, and actively engage in DMHIs with their child. 10. Develop DMHIs that are evidence-based, credible, transparent, and secure.
11. Consider the needs and preferences of different age groups and tailor DMHIs accordingly, for example offering read-aloud options for younger children or presenting age-appropriate terminology and mental health content. It might be appropriate to design different versions of a DMHI or have different sections dedicated to different age groups.
Strengths and limitations
By adopting co-design methodology, we were able gain a rich understanding of caregivers’ perspectives on youth DMHIs as well as their design ideas for Momentum. This helped the research team understand how caregivers would like to engage with Momentum, and how they could facilitate young people’s engagement with the platform. Participants were given minimal information about the platform to facilitate a ‘blank slate’ approach. This allowed participants to generate ideas freely regarding the purpose of the platform, engagement strategies and features (e.g. content, function and aesthetics). The approach also allowed participants to voice their concerns about DMHIs more broadly and to suggest solutions to address their concerns. Another strength of this research was the allocation of caregivers into group discussions based on their child(ren)'s age. This facilitated discussions about age-related considerations such as privacy of young people's information, caregiver involvement and appropriate terminology.
The participant sample had diversity in terms of young people’s and caregivers’ experience with digital health or mental health platforms, as well as young people’s self-reported emotional problems. However, the sample was skewed towards female participants, individuals from higher socio-economic brackets, and those with higher levels of education. Furthermore, the study was conducted across three sites in Brisbane, Australia. These sample characteristics pose limitations to the generalisability of study findings to other populations and contexts. While data saturation was reached, new ideas may have presented with a more heterogeneous participant sample. The sample size (n = 16) did not permit for comparisons between the responses of caregivers with younger children and older adolescents to be made.
Translating knowledge into practice
Drawing upon the results of this study and our related co-design study with young people, 39 prototype designs of Momentum were developed in collaboration with a professional web design service. Young people played an active role in shaping the design of the platform through a series of iterative prototype feedback surveys and workshops. The research team are currently finalising the build of Momentum which will undergo usability testing through think-aloud methods and interviews with caregivers and young people to further refine the platform. Momentum will then be evaluated via a series of randomised control trials to assess end-user adherence to treatment, effectiveness in reducing mental health symptoms and cost-effectiveness, and will be made available to the Australian public.
Future directions for research
The focus of this research was on macro-level design. For example, caregivers were not asked to design home pages or other platform features. As young people will be the primary end-users of Momentum, we wanted the specific designs for the platform to come from children and adolescents themselves. 39 However, future studies may involve caregivers in micro-level design stages, for example, in a dyad with their child. These studies could adapt the recommendations for conducting co-design and intervention development research outlined in our previous research with young people, 39 by incorporating interactive design activities such as drawing and using design templates to enable participants to visualise design concepts. Researchers and clinicians would need to ensure that caregivers’ ideas do not overpower or shape young people's design ideas. Another important consideration for future research is the integration of technological advancements (e.g. EMIs 61 ), AI and other automatic processes into the design of DMHIs to enhance the personalisation of content for end-users. The potential benefits (e.g. personalisation) and pitfalls (over-pathologising) of AI for DMHIs however, needs to be considered.
To improve the generalisability of research findings, future studies should strive to include a larger and more diverse sample in terms of demographic characteristics (e.g. education, socio-economic status) and geographical locations. While Momentum is intended as a national intervention, designed for the Australian context, researchers and designers should ensure that interventions are co-designed with end-users for their local context. Sobowale et al. remarked that culture should be considered when designing youth mental health interventions. 48 As an example, the authors note that Vietnam (where their study was conducted) is a Confucian society where parents have a strong influence on young people's decisions and behaviours that could influence their access to mental health services and intervention. 48 End-users’ access to technology, and their digital literacy, must also be considered when designing DMHIs. Parikh et al.'s study of school-based mental health services in India found that parents and adolescents viewed DMHIs as unfeasible due to low ownership of personal digital devices. 62 Furthermore, Rost et al. noted that DMHIs have the potential to exclude end-users who have low digital literacy or do not have access to digital technology. 52 Relevant to Momentum, 93% of Australian households have access to the Internet. 63
Conclusions
As part of a larger body of co-design research, this study aimed to collaborate with caregivers of young people aged 7–17 years in the design of a self-directed digital youth mental health treatment platform for children and adolescents with anxiety and depression, called Momentum. Caregivers shared their perspectives on, and ideas for, Momentum's purpose, content, functionality, design and end-user engagement strategies. Participants believed that DMHIs should provide therapeutic and education resources for both young people and caregivers, and should promote shared and positive communication about mental health between young people and others (e.g. caregivers, peers, other adults). They advocated for DMHIs to be simple to use and easy to understand, and suggested ways to enhance the personalisation of the platform, including the use of customisable platform features. Participants thought that young people's engagement with DMHIs would be enhanced by presenting interactive activities, offering incentives, creating a relatable platform and including features that attract and maintain young people's attention. Although participants held varying views on the role of caregivers in the platform, there was consensus that caregiver support should be balanced with young people's autonomy. Participants shared some apprehension about youth DMHIs but were able to suggest strategies that would ease their concerns. Caregivers’ design ideas will complement the design ideas of young people from an earlier study stage, to inform the creation of Momentum.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241263693 - Supplemental material for Co-designing a new digital mental health platform, ‘Momentum’, with caregivers of young people aged 7–17
Supplemental material, sj-docx-1-dhj-10.1177_20552076241263693 for Co-designing a new digital mental health platform, ‘Momentum’, with caregivers of young people aged 7–17 by Kristiana Ludlow, Sonja March, Jeremy K Russell, Brooke Ryan, Renee L Brown, Leanne Hides, Caroline Donovan, Susan H Spence, Joseph Saxby and Vanessa E Cobham in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241263693 - Supplemental material for Co-designing a new digital mental health platform, ‘Momentum’, with caregivers of young people aged 7–17
Supplemental material, sj-docx-2-dhj-10.1177_20552076241263693 for Co-designing a new digital mental health platform, ‘Momentum’, with caregivers of young people aged 7–17 by Kristiana Ludlow, Sonja March, Jeremy K Russell, Brooke Ryan, Renee L Brown, Leanne Hides, Caroline Donovan, Susan H Spence, Joseph Saxby and Vanessa E Cobham in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank Dr Genevieve Smith for co-facilitating one of the group discussions. They would also like to thank participants for their time and contributions to the co-design of Momentum.
Contributorship
SM, VEC, LH, CD and SSH conceptualised the work with VEC leading the study. JKR, SM, VEC, BR collected the data, and KL, JKR, RLB and SM analysed the data. KL, JKR, BR and JS drafted the manuscript with all other authors providing intellectual contributions. All authors reviewed and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by Children's Health Queensland Human Research Ethics Committee (HREC number: 65847) and the University of Queensland's Human Research Ethics Committee (2020/HE002416). Every participant gave informed written consent prior to participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Australian National Health and Medical Research Council under a Million Minds Mission Grant [number APP1179490].
Guarantor
VC.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.