
Abstract
Objective
To systematically investigate the key determinants influencing health information quality in social media environments and elucidate their hierarchical relationships, thereby providing evidence-based guidance for quality improvement.
Methods
This study employed an innovative integration of meta-ethnography and Decision-Making Trial and Evaluation Laboratory-Interpretive Structural Modeling (DEMATEL-ISM) methodologies. Through systematic extraction and multi-dimensional analysis of influencing factors—including centrality metrics, causal relationships, and hierarchical structures—we developed a comprehensive mechanism model clarifying factor interactions and their cumulative impacts on health information quality enhancement.
Results
Our analysis identified 18 critical factors affecting health information quality, which were categorized into six distinct hierarchical levels through rigorous computational modeling. The results revealed complex cross-level interactions and mutual influences among these determinants. Nine core factors emerged as pivotal: information accuracy, authority orientation, platform reputation, creator expertise, information utility, health information literacy, content originality, source authority, and health concepts.
Conclusion
The findings establish a hierarchical quality improvement framework, suggesting that targeted interventions focusing on the nine core factors can significantly enhance health information quality in social media ecosystems. This study provides both theoretical foundations and practical insights for multi-stakeholder collaborative governance in digital health communication.
Introduction
In recent years, with the rapid development of mobile internet technology and the rise of social application software, the market scale of social media platforms in China, such as WeChat, Weibo, Zhihu, and Douyin, has been continuously expanding. These platforms have increasingly become the most common channels for the public to generate, obtain, and share information. The health information published on these platforms, due to its richness and vividness, has reduced the cost for users to understand medical terminology and has gradually become an important channel for the dissemination of health information and for people to access health-related information. These social media platforms have made contact with health information more widespread and have provided convenience for individuals to engage in proactive health management.
Problem statement
Despite the convenience that social media platforms provide for users to access and utilize health information, the open nature of social media allows any user to post and disseminate health information without verifying its authenticity. This has led to the creation and spread of a significant amount of false health information, severely misleading users’ judgment of the information's credibility. Through research, the author has found that social media is a complex ecosystem where the quality of health information is influenced by multiple factors.1,2 However, which of these factors play a critical role in determining the quality of health information? What are the complex relationships between these factors? Current understanding of these questions is still quite limited.
To address this gap, this study comprehensively employs meta-ethnography and the Trial and Evaluation Laboratory-Interpretive Structural Modeling (DEMATEL-ISM) methodology to deeply analyze the influencing mechanisms of health information quality in the social media environment, with the aim of providing assistance in improving the quality of health information.
Literature review
Social media has emerged with the development of mobile internet technology and big data technology as an information dissemination medium centered on user experience. In recent years, with the rapid growth of social media users, it has gradually become a mainstream communication medium in society. 3 According to a 2017 social survey in the USA, 74% of internet users have used social media, and among them, 80% have searched for health information through social media. This indicates that social media has become an important channel for the dissemination of health information. 4 However, due to the varying quality of information currently available on social media, 5 many scholars have begun to focus on the quality of information in social media.
In the research on the quality of health information, scholars mainly focus on health information quality evaluation, health information quality governance, detection of false health information and the study of factors influencing health information quality.
The quality of health information on contemporary social media platforms demonstrates significant heterogeneity. Consequently, evaluating health information quality within social media has emerged as a prominent research priority, prompting scholarly investigations into this domain. Objective assessment of social media health information quality necessitates specialized evaluation instruments. While traditional tools such as the decision-making information support criteria for evaluating research and evidence-based content (DISCERN) checklist and Health on the Net (HON) certification remain in use, their frameworks—originally designed for static web environments—exhibit limited adaptability to the dynamic, interactive architectures characteristic of social media platforms. 6 To address these constraints, Ghalavand et al. 7 implemented a mixed-methods study establishing accuracy, credibility, and reliability as paramount dimensions through expert consensus, while assigning diminished priority to metrics such as information originality given their marginal utility for practical application. Building upon this work, Robillard et al. 8 operationalized quality assessment through their QUEST framework, specifically testing its efficacy in evaluating Alzheimer's disease-related content. In the Chinese social media context, researchers like Hu et al. 9 and Zhang et al. 10 extended these principles by developing platform-specific evaluation systems. Hu's dual-pathway model for Weibo integrates source credibility metrics with content quality indicators, whereas Zhang's multidimensional framework for WeChat accounts for platform architecture and user interaction patterns, reflecting the need for culturally adapted evaluation tools.
In terms of health information quality governance, Friedman's 11 foundational argument positions health information governance as an evolutionary necessity in digital health ecosystems, requiring balanced integration of regulatory oversight and technological innovation. For instance, within China, hospitals frequently employ functional optimization of social media services to enhance health information quality. 12 In contrast, investigations conducted by the Dutch Health Care Inspectorate indicate that medical rating platforms (e.g. Zorgkaart Nederland) can mitigate regulatory deficiencies inherent in conventional oversight frameworks. However, regulatory efficacy remains substantially limited on open platforms such as Twitter and Facebook. 13 This divergence underscores the requisite adoption of stratified governance strategies. Such disparities underscore the necessity for implementing tiered platform governance strategies. These strategies enable precision interventions focused on high-impact scenarios, thereby addressing the governance challenges specific to open digital platforms. For addressing governance dilemmas in open platforms, Moorhead's 14 research further unpacks this complexity, proposing a hybrid governance model that strategically combines AI-driven natural language processing (NLP) detection with human expertise to address the scalability challenges inherent in social media platforms. This aligns with Zhou's 15 advocacy for polycentric governance, emphasizing collaborative participation from governmental bodies, professional organizations, and user communities to create adaptive regulatory environments. A more substantive transformation originates in Bornkessel's “networked care” model. 16 This model advocates repurposing social media as instrumental platforms for physician-patient collaboration, wherein healthcare providers iteratively optimize services through dynamic social platform engagement. Concurrently, direct patient feedback mechanisms drive continuous quality enhancement, thereby constituting a closed-loop governance framework.
Research on detecting false health information in social media environments reflects a synergistic evolution of identification technologies and corrective approaches. Initial detection methods predominantly utilized content analysis techniques, which achieved high precision but were limited by low operational efficiency. Subsequent advancements in machine learning facilitated breakthroughs in algorithmic detection, with NLP-based deep learning architectures (e.g. Bidirectional Encoder Representations from Transformers [BERT]) demonstrating significant progress in automated identification of potentially misleading content. These systems have been empirically validated in detecting vaccine-related health misinformation. 17 Recent developments have witnessed a paradigm shift toward multimodal integration. Li's 18 systematic examination of the Multimodal False News Detection framework proposed a comprehensive methodology integrating data-level, entity-level, and knowledge-level information processing. In a complementary approach, Tommasel 19 developed an advanced deep learning architecture incorporating content features, information diffusion patterns, and user behavioral data, achieving 89.7% classification accuracy for COVID-19-related misinformation instances.
Regarding corrective interventions, Sui's 20 empirical investigation employing the Elaboration Likelihood Model established that combining message quality with source credibility enhances corrective efficacy. Berger's 21 longitudinal analysis revealed that while fact-checking interventions demonstrate short-term effectiveness for specific misinformation instances, media literacy education produces sustained improvements in critical information evaluation capacity. However, intervention strategies must account for the “post-truth paradox”—wherein users experiencing high cognitive dissonance exhibit greater responsiveness to authoritative source endorsements than to factual argumentation.
The quality of health information is dynamically shaped by interdependent individual, technological, and societal determinants. At the individual level, educational attainment and proactive health engagement exhibit positive correlations with information evaluation competence. Clinical studies involving cardiovascular and cerebrovascular patient populations demonstrate that individuals with advanced eHealth literacy consistently select authoritative health information sources and maintain effective information filtering behaviors despite health anxiety states. Conversely, populations with limited eHealth literacy demonstrate heightened susceptibility to low-quality health information. 22 Shaw's 23 analysis of health information national trends survey (HINTS) data demonstrates how eHealth literacy mediates technology adoption patterns, with digitally proficient users exhibiting stronger preferences for authoritative sources—a finding that challenges assumptions about passive information consumption.
Within the technological environment dimension, Chen's study 24 identifies that algorithm-induced information overload on WeChat precipitates trust crises. This phenomenon aligns with deficiencies in medical social search platforms documented by Han et al., 25 collectively demonstrating an “Accessibility-Quality Paradox” wherein technological convenience inadvertently heightens misinformation risks by compromising judgment accuracy.
Social capital simultaneously reconfigures societal perceptions of health information quality at the macro-level. As evidenced in Jia's research, 26 trust relationships and shared cognitive frameworks within Zhihu users’ social network architectures modulate information dissemination patterns. Nabi's 27 cross-cultural study in Bangladesh provides counterintuitive insights, revealing that social capital often outweighs institutional credibility in health information valuation, suggesting community-driven information ecosystems may require distinct governance approaches.
Although current research on the quality of social media information and health information has yielded substantial results, there are still two areas that need to be strengthened: first, the depth of research on factors influencing health information quality can be further enhanced. Existing studies have mainly summarized the various factors affecting health information quality but have not sufficiently explored the complex multidimensional causal relationships between these factors. Second, there is room for innovation in research methods. Most existing research uses single methods to study the influencing factors of health information quality; however, combining multiple methods can allow for a more comprehensive exploration of influencing factors and their multidimensional complex relationships. Based on this, the present study comprehensively employs Meta-ethnographic methods and the DEMATEL-ISM approach to reveal the intrinsic mechanisms influencing health information quality, thereby providing theoretical support for enhancing health information quality in social media environments.
Methodology
Research design
Since health information quality in social media environments is subject to the complex interplay of multiple factors, improving this quality first necessitates identifying the diverse factors influencing it. Subsequent analysis of these factors can reveal their intrinsic interrelationships and mechanisms, thereby facilitating the identification of key pathways for enhancement. Therefore, this study addresses the following research questions:
What are the key factors influencing health information quality within social media environments? What hierarchical relationships and interaction mechanisms exist among these factors? How can health information quality in social media be enhanced through strategic management of critical factors?
To address these research questions, this study examines “Factors Influencing Health Information Quality” through a systematic three-phase approach:
The first phase involves searching Web of Science (WOS) and China National Knowledge Infrastructure (CNKI) databases for literature related to “health information quality” published between 2018 and 2022. Articles were screened according to Critical Appraisal Skills Programmed criteria. Meta-ethnography was then applied to the included studies to extract factors influencing health information quality specifically within social media contexts, thereby addressing RQ1. This methodology was selected for its capacity to systematically integrate dispersed, interdisciplinary findings concerning this complex topic without reliance on predetermined hypotheses. It facilitates inductive derivation of influencing factors from fragmented literature, establishing a structured qualitative foundation for subsequent quantitative analysis.
The second phase employs the integrated application of the DEMATEL method and ISM to analyze hierarchical relationships and interaction mechanisms among influencing factors (addressing RQ2). This combined approach was adopted because it effectively addresses both direct and indirect factor relationships while revealing essential driving elements, capabilities exceeding those of single-method applications.
The third phase develops an impact mechanism model that elucidates intrinsic mechanisms affecting health information quality, identifies key driving pathways and control nodes for enhancement, and provides theoretical support for improving health information quality in social media environments, thus addressing RQ3.The overall research framework is shown in Figure 1.

Research framework.
Research methods
Meta-ethnography
Meta-ethnography was proposed by sociologists Noblit and Hare 28 in the 1980s. It uses integrated methods such as “analysis” and “comparison” to construct models based on intersubjective meanings, effectively “translating” one study into another to form new, synthesized research outcomes. Rather than simply aggregating prior findings, this methodology adopts a systematic approach to critically compare, evaluate, and synthesize heterogeneous studies on related themes through structured protocols. By iteratively translating conceptual frameworks and extracting core constructs, relationships, and contextual patterns across studies, it enables the development of robust theoretical models or frameworks with enhanced explanatory power. 29 Accordingly, this research implements meta-ethnography to analyze, interpret, and integrate seminal publications addressing health information quality in social media. This synthesis identifies pivotal determinants of information quality, establishing an empirical basis for subsequent validation of key influencing factors.
DEMATEL-ISM
The fuzzy DEMATEL-ISM methodology adopted in this study constitutes an integrated methodological framework that synergistically combines the DEMATEL and ISM approaches. This hybrid system simultaneously addresses the identification of influential factor roles and the hierarchical structuring of factor relationships.
DEMATEL operates as a graph-theoretical technique that translates interdependent relationships into causal diagrams via matrix operations, enabling systematic identification of dominant influencing factors through centrality and causality indices. 30 By contrast, ISM serves as a systems engineering methodology designed to deconstruct complex systems through pairwise relationship analyses. It systematically converts unstructured knowledge into hierarchical models through structured analytical procedures, demonstrating particular efficacy in systems characterized by multivariate interactions, nonlinear dependencies, and structural ambiguities. 31
These complementary methodologies exhibit distinct analytical strengths in factor investigation: DEMATEL excels in causal relationship visualization and critical factor prioritization, while ISM provides robust hierarchical configuration and system modularization. Their synergistic integration mitigates individual limitations, notably enhancing analytical rigor in modeling complex socio-technical systems where interdependencies and structural opacity coexist. 32 To address these complexities, our research synthesizes DEMATEL-ISM to systematically identify critical determinants of health information quality within social media ecosystems, leveraging DEMATEL's strength in causal influence mapping and ISM's capability in multi-level system decomposition.
However, since both the DEMATEL and ISM methods rely on expert subjective evaluations, this study employs fuzzy set theory to fuzzify expert ratings in order to reduce subjectivity and enhance objectivity in the results. The specific implementation steps are illustrated in Figure 2.

Implementation steps of the DEMATEL-ISM method.
Research process
Extraction of health information quality determinants
Identifying and defining the synthesis theme
The main task of this stage is to determine the theme and research object through the collection and collation of relevant materials. Since this paper focuses on the factors influencing the quality of health information in the social media environment, the theme and search direction of the literature will be determined as studies related to social media, health information quality, and influencing factors.
Acquiring and reading original studies
Relevant literature related to the research theme is downloaded from the WOS and CNKI databases. Additionally, methods such as citation tracking and reference snowballing are used to further improve the search results. The search queries for Chinese and English literature are respectively set as follows:
- For Chinese literature: SU = “社交媒体 (Social Media)” OR SU = “在线健康平台 (Online Health Platforms)”) AND SU = “健康信息 (Health Information)” OR SU = “信息质量 (Information Quality)” OR SU = “影响因素 (Influencing Factors)” OR SU = “健康信息质量 (Health Information Quality)” - For English literature: TI = (health information quality OR health literacy OR health misinformation) AND TI = (social media OR social network OR infodemic OR fake news).
Preliminary literature research by the project team found that studies related to social media and health information quality have increased significantly since 2018. This trend has been especially pronounced after the outbreak of the COVID-19 pandemic, which has highlighted the role of social media in the dissemination of health information and spurred further research (see Figure 3). Therefore, the search period is limited to the five years between January 2018 and December 2022.A total of 129 papers have been acquired (67 English-language articles from WOS and 62 Chinese-language articles from CNKI). These papers are then screened according to the CASP 33 evaluation criteria, ultimately retaining 32 papers for inclusion in the study (see Appendix 1). The specific screening process is illustrated in Figure 4.

Trend in annual publications on social media health information quality.

Literature selection flowchart.
Inter-translation among studies
Through repeated reading and extraction, the main metaphors, phrases, ideas, or concepts used in the analysis, discussion, and results of each study were listed. 34 The translation of fundamental concepts enables the comparison of different studies; however, it is essential to keep in mind the connections between the original concepts in the original research. When translating verbatim or extracting concepts, the value of the original text must be preserved. 35 After a preliminary review of 32 original studies, this research found that the majority of scholars primarily focused their studies around three dimensions: “Information,” “Information Environment,” and “Information Person.” Therefore, the dimensions that influence the quality of health information can be identified as Information Resources (R), Information Environment (E), and Informational Actors (A), which are represented by the letters R, E, and P during the translation process.
Synthesis and translation
During the translation process, this study found that while the majority of core concepts could be translated, some meanings from the original works were not accurately conveyed. To address this, this study conducted a secondary interpretation based on inter-translation among studies, analyzing seemingly opposing core concepts to achieve an understanding and explanation of these conflicting ideas, and optimizing the previously identified influencing factors from the initial phase of information gathering.
Presentation of integrated results
To facilitate understanding and dissemination among other researchers, the final stage of meta-ethnography involves presenting integrated findings in various forms such as text, images, and videos. This study concludes that the factors influencing the quality of health information in a social media environment primarily include three dimensions: Information, Information Environment, and Information Person.
Identification of key influencing factors based on the DEMATEL-ISM method
Expert consultation and data collection protocol
In alignment with the fuzzy DEMATEL-ISM methodology, this study engaged 15 qualified experts (holding doctoral degrees or associate professor-level positions with ≥5 years of research experience in healthcare, information management, or public health) to evaluate health information quality determinants derived from meta-ethnography. The three-stage data collection protocol comprised: (1) administering anonymous online questionnaires for pairwise factor relationship assessments using a 0–4 scale (0 = no influence; 4 = extreme influence), with annotations for cross-dimensional or asymmetric interactions; (2) aggregating initial responses to generate feedback reports highlighting influence rankings and divergent ratings, prompting expert revisions; and (3) convening a consensus meeting to validate the finalized hierarchical factor model. A double-blind protocol ensured expert anonymity, complemented by encrypted data transmission and three automated reminders per evaluation round to enforce a two-week completion timeline. Post-study, experts received personalized reports detailing their analytical contributions and the practical implications of the validated model.
Construction of the comprehensive influence matrix
First, following the principles of triangular fuzzy numbers, the ratings from 15 experts were standardized and converted into triangular fuzzy numbers, yielding a triangular fuzzy evaluation matrix. Second, the triangular fuzzy evaluation table was converted into a direct influence matrix using Formula (1) (see Appendix 2). Third, the resulting direct influence matrix was standardized to construct a normalized direct influence matrix. Finally, the comprehensive influence matrix was constructed using Formula (2) (see Appendix 2).
Calculation of centrality and causality of factors
Using Formula (3) to Formula (6) (see Appendix 2), the following metrics were calculated: influence degree (Di), being influenced degree (Ri), centrality (Mi), and causality (Ei).
Centrality reflects the size of the factor's role and its importance within the indicator system. When the causality (Ei) is greater than 0, the factor is considered a causal element, indicating that it has a significant influence on other factors. Conversely, when the causality is less than 0, the factor is regarded as a result element, suggesting that it is mainly influenced by other factors.
Drawing the causal relationship diagram
A causal relationship diagram is created with centrality on the x-axis and causality on the y-axis. In this diagram, the positions of each influencing factor are marked. When the causality is negative, the factor is positioned below the horizontal axis, indicating it is a result factor. Conversely, when the causality is positive, the factor is placed above the horizontal axis, indicating it is a causal factor. The causal relationship diagram clearly differentiates between causal elements and result elements, allowing for a more intuitive assessment of each factor's importance within the overall indicator system.
Construction of the hierarchical model
To construct the hierarchical model, the unit matrix I is added to the comprehensive influence matrix (see Appendix 2 Formula (7)). A threshold λ is then set to obtain the reachability matrix (see Appendix 2 Formula (8)). Based on previous research experience 36 and expert recommendations, the threshold λ is finalized at 0.21.
If the set of all elements equal to 1 in the i-th row of the reachability matrix is defined as R i and the set of all elements equal to 1 in the i-th column is defined as S i , and if R i = R i ∩S i holds true, then the influencing factor a i is defined as a high-level influencing factor. Consequently, the i-th row and column are removed. This process is repeated until all factors are eliminated, resulting in the construction of a hierarchical model for the influencing factors of health information quality.
Results
Translation of influencing factors integration results
Through comparative analysis of the original research, a total of 18 influencing factors related to health information quality have been identified and categorized into three dimensions: Information Resources (content and source), Information Environment (social context and platform context), and Information Actors (creators and users), as shown in Figure 5.
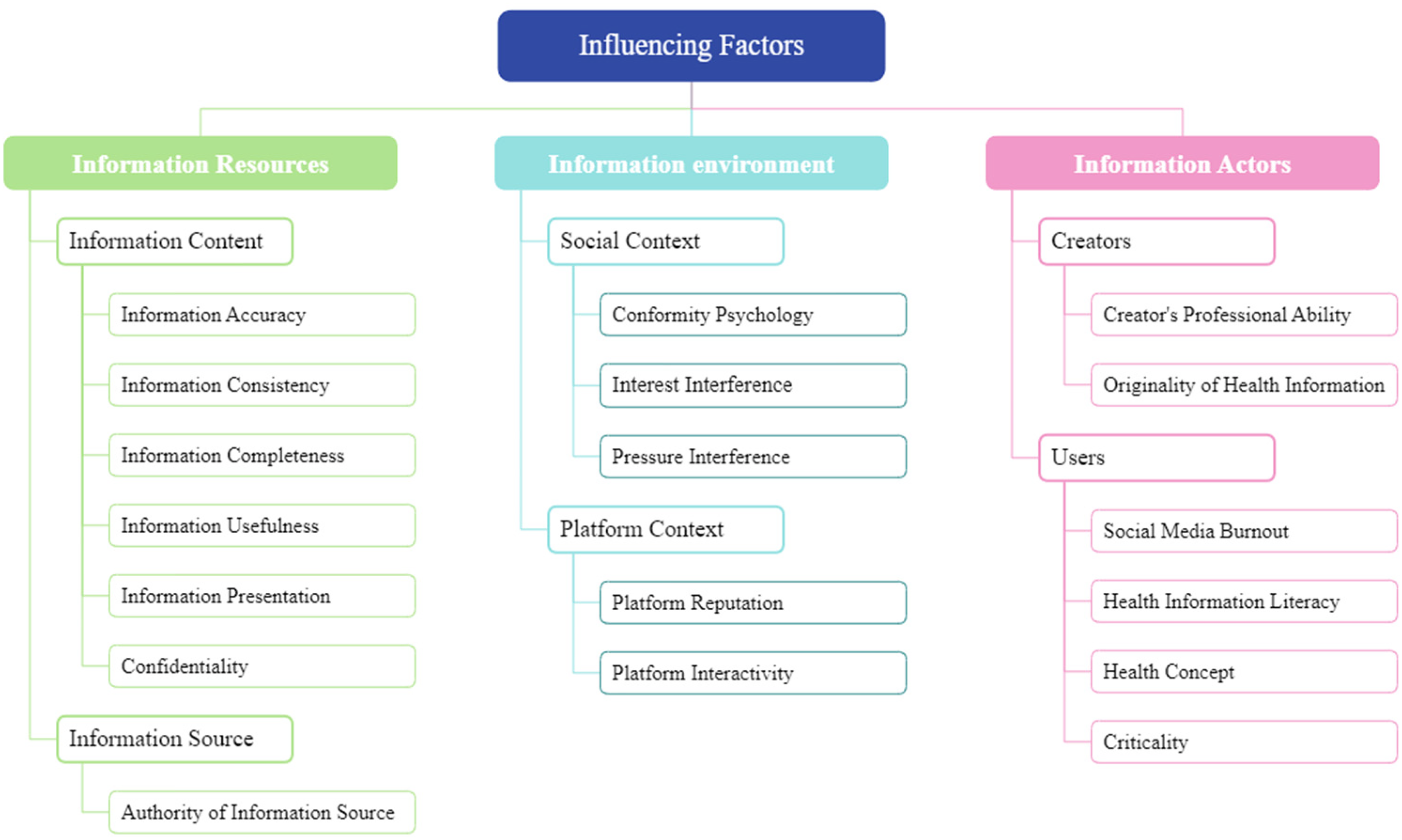
Influencing factors and classification.
Comprehensive impact matrix results
This paper establishes a comprehensive impact matrix according to Formula (2), as shown in Appendix 3. This matrix reflects the direct and indirect impact degrees and relationships among various factors.
Impact index calculation results
Based on Formulas (3) to (6), this paper calculates the influence degree, influenced degree, centrality, and causality of the 18 influencing factors, as well as their ranking results, as shown in Appendix 4.
Causal relationship quadrant diagram
According to the calculation results shown in Appendix 2, we used Python software programming for visualization to draw the causal relationship diagram, as shown in Figure 6. From the diagram, it can be seen that the causal relationship diagram is divided into four quadrants. Seven factors are located in the first quadrant: Information accuracy (F1), information usefulness (F4), authority of information source (F7), creator's professional ability (F13), criticality (F18), health concept (F17), and health information literacy (F16). Three factors are located in the second quadrant: information consistency (F2), information completeness (F3), and confidentiality (F6). Five factors are located in the third quadrant: interest interference (F9), pressure interference (F10), information presentation (F5), social media burnout (F15), and platform interactivity (F12). Three factors are located in the fourth quadrant: conformity psychology (F8), originality of health information (F14), and platform reputation (F11).

Causal relationship diagram.
Centrality analysis
Generally, the higher the centrality value, the more important the influencing factor is, and the more likely it is to be identified as a key influencing factor. Thus, from Figure 6, it can be observed that the 10 influencing factors located in the first and fourth quadrants are key influencing factors with high centrality. In the information dimension, the centrality ranking of information accuracy is the highest, indicating that the accuracy of health information is the most important factor affecting the quality of health information. The centrality rankings of information usefulness (F4) and authority of information source (F7) are also high, making them important influencing factors second only to information accuracy. In the information environment dimension, platform reputation (F11) ranks third overall in centrality, highlighting the importance of reputation for social media platforms. Social media platforms with better reputations are more likely to gain users’ trust. In the information people dimension, criticality (F18), creator's professional ability (F13), and health information literacy (F16) are top-ranking influencing factors. This indicates that the production of high-quality health information relies on creators and users with high health information literacy (good health and medical knowledge and information technology skills).
Cause degree analysis
The cause degree indicates the impact of a factor on other factors. When the cause degree is greater than 0, it means that the factor will affect other factors. From Figure 6, it can be seen that the influencing factors located in the first and second quadrants have high cause degrees and are causal factors. The six factors of information accuracy (F1), information usefulness (F4), authority of information source (F7), information consistency (F2), information completeness (F3), and confidentiality (F6) belong to the Information Resources dimension. Among them, information accuracy (F1) and information usefulness (F4) have both high cause degrees and high centrality, indicating that they are key factors among all influencing factors. Creator's professional ability (F13), health concept (F17), health information literacy (F16), and criticality (F18) belong to the information people dimension. Among these, creator's professional ability (F13) and health concept (F17) have the highest cause degrees in the information people dimension, indicating that these two factors easily influence the quality of health information indirectly through their effects on other factors. There are no causal factors in the information environment dimension, suggesting that the information environment is most susceptible to influence by other factors but does not easily affect other factors.
Hierarchical model
First, this paper constructs the interaction relationships among the influencing factors based on the classification results of hierarchical factors and revises the interaction relationships of some factors according to expert opinions. Then, a multi-level hierarchical structure model of factors affecting the quality of health information in the social media environment is constructed, as shown in Figure 7. From Figure 7, it can be seen that there are six levels of influencing factors affecting the quality of health information in the social media environment. Arrows represent the influence relationships between lower-level factors and upper-level factors, and the direction of the arrows determines whether there is an influence relationship between certain factors. Based on the degree of influence of each factor on the quality of health information, these six levels are categorized into direct influence, indirect influence, and essential influence. The first level is the direct influence layer, including nine factors: information consistency (F2), information completeness (F3), information presentation (F5), conformity psychology (F8), interest interference (F9), pressure interference (F10), platform reputation (F11), Platform Interactivity (F12), social media burnout (F15). The second to fourth levels are the indirect influence layers, including seven factors: confidentiality (F6), originality of health information (F14), information accuracy (F1), criticality (F18), authority of information source (F7), information usefulness (F4), creator's professional ability (F13). The fifth and sixth levels are the essential layers, including two factors: health information literacy (F16) and health concept (F17).

Hierarchical model of influencing factors on health information quality in the social media environment.
Direct impact analysis
Factors in the direct impact layer directly affect the quality of health information in the social media environment. Analysis of this layer reveals that information consistency and comprehensiveness pertain to the informational Content perspective, indicating that high-quality health information requires completeness, consistency, and comprehensiveness. Information presentation and platform interactivity emphasize user experience, meaning that optimizing the interface design and providing convenient interactive features can enhance the quality of health information. Herd mentality, platform reputation, and social media fatigue are considered from the user's psychological perspective, where the reputation of a social media platform is a crucial criterion for users to judge the quality of health information. Due to herd mentality, users tend to seek health information from highly reputable social media platforms. However, social media fatigue can significantly hinder the dissemination of health information; repetitive and low-quality health information, if not properly managed, will increase the user's burden, thus affecting their judgment of the quality of health information.
Indirect impact analysis
Factors from the second to fourth layers indirectly influence the quality of health information on social media through interactions with other factors. Analysis of the relationships among these factors reveals that confidentiality and originality of health information influence platform reputation, thereby indirectly affecting the quality of health information on social media. Information accuracy influences confidentiality and originality, which in turn affects platform reputation and ultimately impacts the quality of health information. Accurate information reflects the truth and remains consistent across time and location, and only accurate information can comprehensively reflect the full picture. Users’ critical thinking impacts the originality of health information, thus affecting platform reputation and indirectly influencing the quality of health information. The authority of information sources affects information consistency, thereby indirectly affecting the quality of health information. Information accuracy, critical thinking, and the authority of sources are interrelated; authoritative information tends to be more accurate, and when individuals are willing to question authority, it leads to stricter supervision of information, thereby improving accuracy. The usefulness of information and the professional ability of creators directly affect individual critical thinking, which in turn influences the originality of health information and platform reputation, ultimately impacting the quality of health information. Additionally, the usefulness of health information and the professional ability of creators are strongly interconnected, indicating that the professional level of creators directly affects the quality of health information. High user evaluations of health information demonstrate the creators’ professional capabilities, forming a bidirectional interactive relationship.
Fundamental impact analysis
Health information literacy and health concepts located in the fifth and sixth layers are foundational and core factors influencing the quality of health information on social media. Personal health information literacy directly impacts critical thinking and, through the pathway of health information originality and platform reputation, indirectly affects the quality of health information. Simultaneously, health information literacy directly influences whether individuals exhibit herd mentality and their evaluation of platform reputation, ultimately indirectly affecting the quality of health information. Health concepts directly influence personal health information literacy, which then follows the pathway of health literacy to ultimately impact users’ judgment of health information quality. Health concepts can also indirectly impact the quality of health information through direct effects on platform reputation and herd mentality.
Impact mechanism
The above analyses clarify the interactions among influencing factors and their effects on the quality of health information in the social media environment. Based on this, a model of the impact mechanism of health information quality in the social media environment is constructed (as shown in Figure 7). This model reveals key links affecting health information quality and provides theoretical support for improving health information quality in social media environments.
As shown in Figure 8, 18 influencing factors are categorized into three dimensions: Information Resources, information people, and information environment. There are mutual influences between Information Resources and information people, and they also affect the information environment in different ways. Information people can have direct, indirect, and fundamental impacts on health information quality. Factors in the information people dimension are divided into three levels: social media fatigue is at the top level, directly impacting health information quality; users’ critical thinking and creators’ professional ability are at the intermediate level, indirectly affecting health information quality; health information literacy and health concepts are at the bottom level, fundamentally impacting health information quality. Information Resources itself can have direct and indirect impacts on health information quality. The Information Resources dimension is divided into two levels: information consistency, comprehensiveness, and presentation are at the top level, directly affecting health information quality; information confidentiality, accuracy, source authority, and usefulness are at the lower level, indirectly affecting health information quality through other influencing factors. The information environment only has a direct impact on health information quality, with all factors in the information environment dimension directly affecting health information quality.
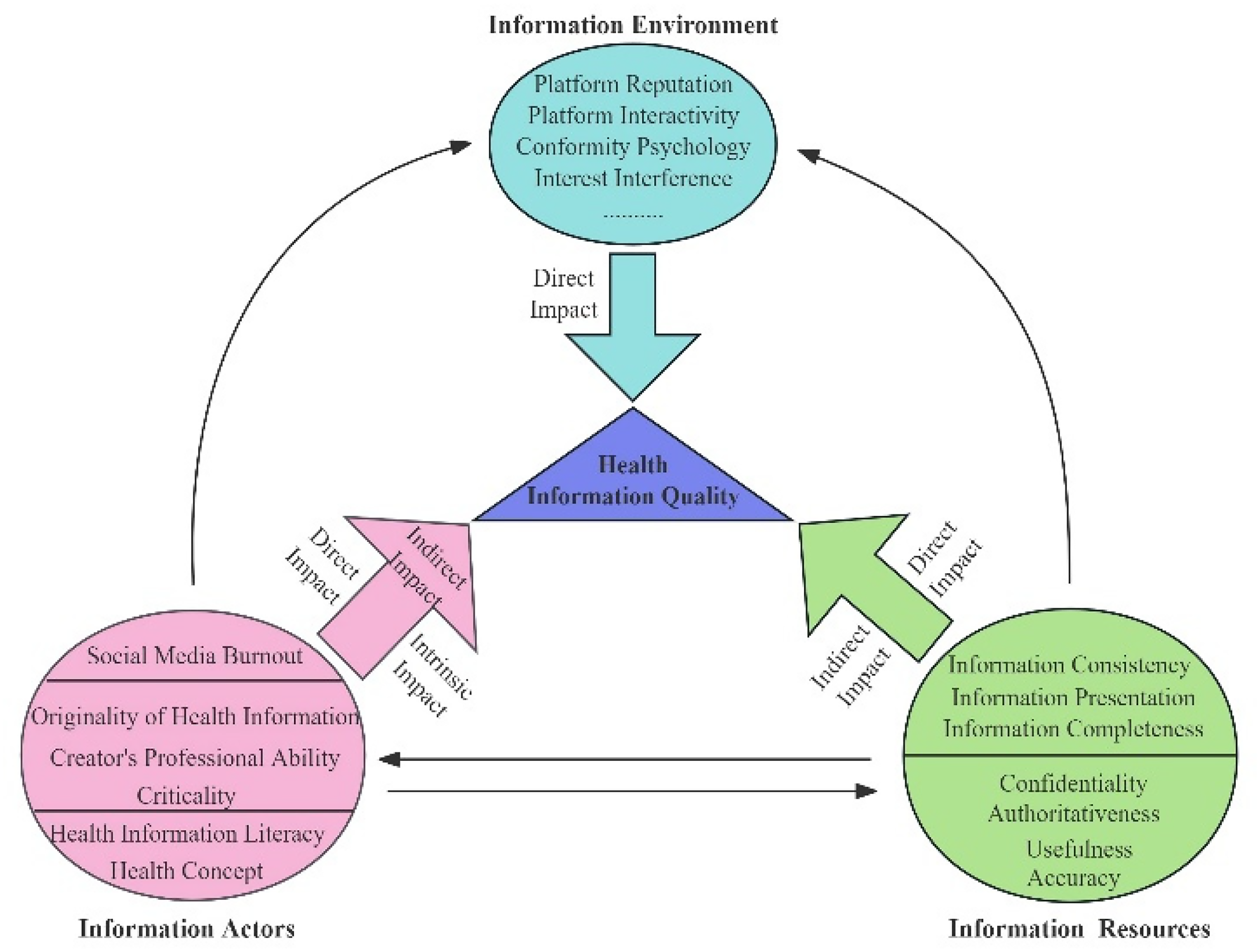
Impact mechanism model of health information quality.
Discussion
Research implications
Based on the results of this study, the author believes that the quality of health information in the social media environment can be improved from the following aspects.
Enhancing the usefulness, accuracy, and authoritativeness of health information
First, value user evaluations of health information utility and enhance its usefulness. This study's results indicate that the usefulness of information is a key factor influencing the quality of health information in social media environments. Whether the disseminated health information is useful to users significantly impacts their judgment of its quality. Therefore, a comprehensive user feedback mechanism should be established to regularly collect user feedback on health information usage. Based on this feedback, adjustments should be made to the Information Resources and dissemination methods to ensure users can easily access useful information. Second, establish effective guidelines for publishing health information to improve its accuracy. The study's results show that the centrality and causality of information accuracy rank highest, forming the foundation and core of enhancing health information quality. Therefore, a stringent gatekeeping mechanism should be reinforced, with strict review and publication standards covering ethics, content, and privacy protection. Third, establish cooperation with official media platforms and authoritative expert teams to ensure the authoritativeness of information sources. The study results indicate that the authoritativeness of information sources is a crucial factor, second only to information accuracy, indirectly affecting the quality of health information. In social media, every user can become an information publisher, including authoritative experts and media, as well as “pseudo-experts” seeking popularity. Thus, platforms should collaborate with official and authoritative experts to ensure the authoritativeness of information sources.
Strengthening user privacy protection, creating a positive health information environment, and building brand effect
First, enhance user privacy protection and regularly update valuable health information. The study results indicate that the confidentiality of information indirectly affects the quality of health information on social media platforms by influencing the platform's reputation. Therefore, by strengthening the protection of users’ personal information, social media platforms can enhance user trust and recognition. Second, increase communication channels with information recipients. The study results show that enhancing platform interactivity can improve the quality of health information. As a typical feature of interactive social media, platforms can establish good interactive relationships with users through methods such as reply comments and regular Q&A sessions. Interaction can improve users’ experience with health information. Third, encourage the publication of more diversified and visualized health Information Resources. Diverse and visualized health content, such as images, videos, and animations, can more easily attract users’ attention. By publishing vivid and interesting content, platforms can attract more users, enhancing their experience and improving their evaluation of health information quality.
Enhancing the professional competence of health information publishers and improving users’ health information literacy
First, establish a professional certification function for information publishers and improve the certification mechanism for their professional levels. From the perspective of information providers, the professional competence of creators is a prominent influencing factor. Compared to general information, health information has stronger professionalism and higher creation thresholds. Therefore, a review mechanism for the professional competence of health information publishers must be established, examining their medical education background and professional qualifications. Publishers lacking relevant qualifications should not be allowed to publish health information or must undergo stricter reviews to ensure the accuracy and authoritativeness of the published information. Second, encourage the creation and dissemination of valuable original information. The study results indicate that the originality of health information indirectly affects its quality. Therefore, social media platforms should provide certain rewards for excellent original information published by creators. This can encourage publishers to create more high-quality original information rather than simply copying or forwarding information from other platforms. High-quality original information will attract more users to the social media platform, forming a positive cycle. Third, improve users’ health concepts and health literacy through publicity and training. The study results indicate that users’ health information literacy is a fundamental factor affecting the quality of health information in social media environments. Government management departments and social media platforms should regularly provide public lectures on health knowledge and methods for healthily obtaining and identifying false health information in social media environments. This will improve users’ health information literacy, enabling them to filter and apply health information effectively in social media.
Research prospects
This study combines ethnographic methods, DEMATEL, and ISM methods to explore the quality of health information in social media environments, including the extraction of influencing factors, identification of key influencing factors, and analysis of relationships among these factors. These three parts form a comprehensive analysis system for influencing factors, leveraging the strengths of each method while overcoming the limitations of individual methods. The study of influencing factors is not only a hot topic in the fields of social media and health information but also in other management domains, such as information system service quality, user intention for digital reading services, and user adoption of AI-generated content. Therefore, this study suggests that the proposed analysis system can effectively address the quality issues of health information and be applied to the study of influencing factors in the aforementioned domains. Future work will apply this method system to more fields to verify its universality.
Conclusion
To improve the quality of health information in the social media context, this study employs a combination of meta-ethnography, fuzzy DEMATEL, and ISM methods to investigate the influencing factors of health information quality and the interrelationship mechanisms among these factors. The study reveals key links that contribute to the enhancement of health information quality in the social media environment.
A total of 18 factors affecting health information quality have been identified, with each factor closely linked and exhibiting cross-level relationships. The key influencing factors include information accuracy, authority orientation, platform reputation, creator expertise, information usefulness, health information literacy, originality of health information, authority of information sources, and health concepts, categorized into three dimensions: information, users, and environment. By controlling these nine key influencing factors, the quality of health information in the social media environment can be significantly improved.
While this study provides an in-depth analysis of the mechanisms influencing health information quality in social media environments, several limitations should be acknowledged. Firstly, the literature selection was restricted to the CNKI and WOS databases, and the search keyword strategy may require further optimization, resulting in a limited pool of retrieved articles. Secondly, the evaluation of inter-factor relationships relied on expert subjective judgments. Although fuzzy set theory was introduced to mitigate subjectivity in expert scoring, residual biases inherent in expert-driven assessments cannot be fully eliminated. Therefore, future work will expand literature sources (e.g. incorporating Scopus and PubMed) and refine search algorithms to identify additional domain-relevant studies, enabling more comprehensive factor extraction. Furthermore, a hybrid qualitative-quantitative approach will be adopted to enhance the objectivity of relationship evaluations among influencing factors.
Footnotes
Acknowledgments
The authors would like to thank the 15 experts in the fields of healthcare and information management who scored the relationships between the influencing factors. In addition, they would like to thank Xi Wang for his support in touching up and editing the article and Xinyu Zhu provided assistance in data collection for the paper.
Ethical approval
We would like to clarify that the study is a research analysis based on previously published, public, and available scientific literature. It did not involve any direct interaction with human or animal subjects, nor did it involve the collection of any new primary data (including patient data, surveys, interviews, or biological samples). As the study is secondary data analysis and is taken from freely accessible database, hence, ethical approval is not applicable.
Informed consent
This paper focuses on the key factors influencing the quality of health information in the social media environment and their hierarchical logical relationships, and the research data are health information-related literature data, which is a secondary study of the published literature and does not involve human or animal studies; therefore, informed consent from subjects is not applicable.
Contributorship
XZ and QXW proposed research ideas, designed the study, data collection and processing, and drafting of thesis. YQN assisted in data collection and revised article content and formatting. AQH assisted in data processing. RFL designed the study and supervised the research methodology and statistics, and was involved in touching up and editing the article as well as revising article. All authors revised it critically for intellectual content and have approved the final version of this protocol. 21
Funding
This article is one of the research outcomes of the project funded by the Basic Scientific Research Business Fee of Beijing University of Chinese Medicine (Project No.: 2023-JYB-JBZD-068).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
XZ and RFL.
Appendix 1. The literature included in the study consists of 32 articles
Appendix 2. Formulas used in this paper
Appendix 3. Comprehensive impact matrix

| F1 | F2 | F3 | F4 | F5 | F6 | F7 | F8 | F9 | F10 | F11 | F12 | F13 | F14 | F15 | F16 | F17 | F18 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F1 | 0.20 | 0.24 | 0.24 | 0.25 | 0.23 | 0.22 | 0.24 | 0.27 | 0.22 | 0.24 | 0.28 | 0.22 | 0.25 | 0.26 | 0.25 | 0.25 | 0.22 | 0.26 |
| F2 | 0.18 | 0.14 | 0.17 | 0.18 | 0.18 | 0.17 | 0.18 | 0.20 | 0.18 | 0.18 | 0.20 | 0.18 | 0.18 | 0.19 | 0.18 | 0.18 | 0.18 | 0.19 |
| F3 | 0.18 | 0.17 | 0.14 | 0.18 | 0.18 | 0.17 | 0.18 | 0.20 | 0.18 | 0.18 | 0.20 | 0.18 | 0.18 | 0.19 | 0.18 | 0.18 | 0.18 | 0.19 |
| F4 | 0.21 | 0.19 | 0.19 | 0.17 | 0.20 | 0.19 | 0.20 | 0.24 | 0.20 | 0.20 | 0.25 | 0.20 | 0.22 | 0.21 | 0.20 | 0.22 | 0.22 | 0.21 |
| F5 | 0.15 | 0.14 | 0.16 | 0.17 | 0.13 | 0.16 | 0.14 | 0.18 | 0.16 | 0.16 | 0.19 | 0.16 | 0.17 | 0.17 | 0.17 | 0.17 | 0.16 | 0.18 |
| F6 | 0.18 | 0.17 | 0.17 | 0.18 | 0.18 | 0.14 | 0.18 | 0.19 | 0.18 | 0.18 | 0.22 | 0.18 | 0.18 | 0.19 | 0.18 | 0.18 | 0.16 | 0.19 |
| F7 | 0.22 | 0.19 | 0.19 | 0.19 | 0.19 | 0.19 | 0.16 | 0.21 | 0.19 | 0.19 | 0.24 | 0.19 | 0.19 | 0.20 | 0.19 | 0.20 | 0.19 | 0.23 |
| F8 | 0.18 | 0.15 | 0.15 | 0.17 | 0.17 | 0.17 | 0.17 | 0.15 | 0.17 | 0.17 | 0.19 | 0.17 | 0.17 | 0.18 | 0.17 | 0.18 | 0.17 | 0.18 |
| F9 | 0.18 | 0.16 | 0.16 | 0.15 | 0.17 | 0.16 | 0.17 | 0.19 | 0.13 | 0.17 | 0.19 | 0.17 | 0.15 | 0.18 | 0.17 | 0.18 | 0.17 | 0.18 |
| F10 | 0.18 | 0.16 | 0.16 | 0.17 | 0.17 | 0.17 | 0.17 | 0.19 | 0.17 | 0.13 | 0.19 | 0.17 | 0.17 | 0.18 | 0.17 | 0.16 | 0.15 | 0.18 |
| F11 | 0.21 | 0.18 | 0.18 | 0.19 | 0.18 | 0.18 | 0.18 | 0.20 | 0.18 | 0.18 | 0.17 | 0.18 | 0.19 | 0.19 | 0.19 | 0.19 | 0.18 | 0.20 |
| F12 | 0.14 | 0.15 | 0.13 | 0.14 | 0.18 | 0.13 | 0.14 | 0.17 | 0.16 | 0.14 | 0.18 | 0.12 | 0.16 | 0.17 | 0.16 | 0.16 | 0.16 | 0.17 |
| F13 | 0.23 | 0.19 | 0.19 | 0.22 | 0.20 | 0.19 | 0.22 | 0.22 | 0.20 | 0.20 | 0.25 | 0.20 | 0.17 | 0.23 | 0.20 | 0.21 | 0.20 | 0.21 |
| F14 | 0.19 | 0.18 | 0.18 | 0.18 | 0.18 | 0.18 | 0.18 | 0.20 | 0.18 | 0.18 | 0.23 | 0.18 | 0.18 | 0.16 | 0.18 | 0.19 | 0.18 | 0.20 |
| F15 | 0.18 | 0.17 | 0.17 | 0.18 | 0.18 | 0.17 | 0.15 | 0.19 | 0.17 | 0.17 | 0.20 | 0.17 | 0.18 | 0.18 | 0.14 | 0.18 | 0.17 | 0.19 |
| F16 | 0.20 | 0.18 | 0.18 | 0.19 | 0.19 | 0.18 | 0.19 | 0.23 | 0.19 | 0.19 | 0.22 | 0.19 | 0.19 | 0.20 | 0.19 | 0.16 | 0.21 | 0.22 |
| F17 | 0.20 | 0.18 | 0.18 | 0.19 | 0.19 | 0.18 | 0.19 | 0.23 | 0.19 | 0.19 | 0.22 | 0.19 | 0.19 | 0.20 | 0.19 | 0.22 | 0.15 | 0.22 |
| F18 | 0.23 | 0.20 | 0.20 | 0.23 | 0.20 | 0.20 | 0.22 | 0.24 | 0.20 | 0.20 | 0.25 | 0.20 | 0.21 | 0.23 | 0.20 | 0.21 | 0.20 | 0.18 |
Note: F1: Information Accuracy; F2:Information Consistency; F3: Information Completeness; F4: Information usefulness; F5: Information presentation; F6: Confidentiality; F7: Authority of information source; F8: Conformity Psychology; F9: Interest Interference; F10: Pressure interference; F11: Platform Reputation; F12: Platform Interactivity; F13: Creator's Professional Ability; F14: Originality of Health Information; F15: Social Media Burnout; F16: Health Information Literacy; F17: Health Concept; F18: Criticality.
Appendix 4. Indicator system of influencing factors and impact index

| Impact factors | Di | Ci | Mi | Ri | Factor attributes | ||||
|---|---|---|---|---|---|---|---|---|---|
| Value | Ranking | Value | Ranking | Value | Ranking | Value | Ranking | ||
| F1 | 4.33063668 | 1 | 3.43144595 | 5 | 7.76208263 | 1 | 0.89919073 | 1 | C |
| F2 | 3.23389754 | 10 | 3.13841185 | 18 | 6.37230939 | 14 | 0.09548569 | 8 | C |
| F3 | 3.23389754 | 10 | 3.14024948 | 17 | 6.37414701 | 13 | 0.09364806 | 9 | C |
| F4 | 3.69525769 | 4 | 3.33571006 | 7 | 7.03096775 | 5 | 0.35954763 | 3 | C |
| F5 | 2.94014636 | 17 | 3.32210373 | 10 | 6.26225009 | 17 | −0.38195738 | 15 | R |
| F6 | 3.2304072 | 12 | 3.14569134 | 16 | 6.37609853 | 12 | 0.08471586 | 10 | C |
| F7 | 3.53552238 | 5 | 3.24374286 | 11 | 6.77926524 | 8 | 0.29177952 | 4 | C |
| F8 | 3.05748514 | 14 | 3.69265512 | 2 | 6.75014025 | 10 | −0.63516998 | 18 | R |
| F9 | 3.03779066 | 16 | 3.23389754 | 14 | 6.2716882 | 16 | −0.19610687 | 14 | R |
| F10 | 3.04587717 | 15 | 3.23801313 | 13 | 6.2838903 | 15 | −0.19213596 | 13 | R |
| F11 | 3.34495247 | 8 | 3.87123218 | 1 | 7.21618464 | 3 | −0.52627971 | 17 | R |
| F12 | 2.75199228 | 18 | 3.23389754 | 14 | 5.98588981 | 18 | −0.48190526 | 16 | R |
| F13 | 3.71787226 | 3 | 3.32834042 | 8 | 7.04621268 | 4 | 0.38953184 | 2 | C |
| F14 | 3.32441738 | 9 | 3.51212245 | 4 | 6.83653983 | 7 | −0.18770508 | 12 | R |
| F15 | 3.13940749 | 13 | 3.32621933 | 9 | 6.46562681 | 11 | −0.18681184 | 11 | R |
| F16 | 3.51248872 | 6 | 3.41662087 | 6 | 6.9291096 | 6 | 0.09586785 | 7 | C |
| F17 | 3.51248872 | 6 | 3.24157725 | 12 | 6.75406598 | 9 | 0.27091147 | 5 | C |
| F18 | 3.8024032 | 2 | 3.59500976 | 3 | 7.39741296 | 2 | 0.20739343 | 6 | C |
Note: F1: Information Accuracy; F2: Information Consistency; F3: Information Completeness; F4: Information usefulness; F5: Information presentation; F6: Confidentiality; F7: Authority of information source; F8: Conformity Psychology; F9: Interest Interference; F10: Pressure interference; F11: Platform Reputation; F12: Platform Interactivity; F13: Creator's Professional Ability; F14: Originality of Health Information; F15: Social Media Burnout; F16: Health Information Literacy; F17: Health Concept; F18: Criticality; C: causal factors; R: resulting factors.