
Abstract
Background
Half of US adults have ≥1 cardiovascular disease (CVD) risk factors. Exercise is the first-line lifestyle therapy to prevent and treat CVD. We developed the Prioritize Personalize Prescribe Exercise algorithm (P3-EX), an evidence-based tool that clinicians can use to prescribe exercise for patients with CVD risk factors.
Purpose
To conduct a feasibility survey study of user satisfaction and usability of P3-EX as an exercise prescription (ExRx) tool among healthcare providers.
Methods
Healthcare providers enter information on the patient's medical history and CVD risk factors into P3-EX. Prioritize Personalize Prescribe Exercise algorithm then scores and prioritizes CVD risk factors and produces an ExRx for the prioritized CVD risk factor. We recruited physicians (N = 39), nurses (N = 63), and allied health professionals (N = 231) who recommend exercise to patients through professional society meetings, presentations, newsletters, and investigators’ networks. Participants completed a timed case study of a patient with CVD risk factors using P3-EX on a templated website. They then completed an adapted version of the Mobile Application Rating Scale, with responses ranging from 5 (completely agree) to 1 (completely disagree) to evaluate the ease of use, system information arrangement, and usefulness of P3-EX. Descriptive statistics determined the % response, time spent using P3-EX, and ExRx produced.
Results
Of the 844 recruited participants, 309 completed the feasibility survey study (healthcare provider N = 143, people with other professional affiliates N = 166). Of these, 86.9% agreed using P3-EX will make their patients healthier; 86.6% agreed feedback is immediate and understandable; 81.4% agreed P3-EX is intuitive, producing high-quality, evidenced-based, individualized ExRx; 83.5% are generally satisfied with P3-EX; 81.3% would recommend P3-EX to colleagues; and 79.2% agreed ExRx produced by P3-EX is safe. However, 34.4% agreed fault tolerance could be improved. Most participants (88.8%) produced an ExRx for the same prioritized CVD risk factor. The average time spent using P3-EX was 4.6 min.
Conclusion
We found healthcare providers are satisfied with P3-EX and agreed that it is a usable ExRx tool for patients with CVD risk factors. Our results are promising because healthcare providers lack the time, knowledge, confidence, and guidance to recommend exercise to patients. Prioritize Personalize Prescribe Exercise algorithm appears to be a potential solution to this problem.
Keywords
Introduction
Cardiovascular disease (CVD) is the leading cause of death in the United States (US) and the world. One in five deaths in the US resulted from CVD in 2021, while one in three deaths worldwide resulted from CVD in 2019.1,2 Approximately half of Americans (47%) have at least one of the five major CVD risk factors: hypertension, diabetes mellitus, dyslipidemia, obesity, and physical inactivity.3,4 The prevalence of these CVD risk factors is 46%, 15%, 11%, 42%, and 25% in the US,5–13 with similar prevalence trends of 31%, 8%, 39%, 13%, and 29% worldwide, respectively.
Recognizing the many health benefits of physical activity, professional organizations such as the American Heart Association (AHA), American College of Cardiology, American College of Sports Medicine (ACSM), and World Health Organization recommend exercise as the most efficient, cost-effective, and accessible “polypill” to prevent and treat CVD and its risk factors.14–21 Despite these strong endorsements of exercise for heart health, only 30% of primary care physicians recommend exercise to their patients although such recommendations are a strong incentive for patients to exercise.22–28 Recent studies identified the three primary barriers for physicians and other healthcare providers to prescribe exercise to be due to lack of tools, training, and time.22,23,29,30 Indeed, fewer than half of the physicians in the US who finished training before 2013 received formal education in physical activity and/or exercise. 22
An ExRx is the process whereby an individualized physical activity program is structured by Frequency (How Often?), Intensity (How Hard?), Time (How Long?), and Type (What Kind?) principle of exercise or FITT. Personalized ExRxs are preferred over generic approaches to ExRx such as telling patients to walk to optimize health outcomes.29,31–33 Indeed, the ACSM recommends different FITT ExRxs for 26 clinical chronic diseases and health conditions including the major CVD risk factors of hypertension, diabetes mellitus, dyslipidemia, and obesity.21,34–36 Clinical decision support systems are rapidly growing tools in health care because they guide healthcare providers to streamline information, produce evidence-based diagnostics and prescriptions, recommend next steps of treatments, maintain long-term health management plans, and save time.37–40 A well-developed clinical decision support system has the potential to overcome the barriers for clinicians to prescribe personalized ExRx for their patients. 41 Accordingly, we performed a comprehensive systematic review of commercially available digital applications to determine if evidenced-based, time-efficient ExRx clinical decision support tools existed on the market. 42 We found no such ExRx tool existed that addressed the primary barriers physicians face in prescribing exercise to their patients and that focused on CVD risk factors. 43
To address this unmet clinical need for an evidenced-based, time-efficient ExRx clinical decision support system, we integrated: 1) the ACSM exercise preparticipation health screening recommendations 21 ; 2) an adapted AHA Life's Essential 8 cardiovascular health scoring system for untreated and treated CVD risk factors to determine the CVD risk factor posing the greatest heart health risk43,44; 3) the ACSM strategies for designing an ExRx for healthy people with multiple CVD risk factors 21 ; and 4) the ACSM FITT principle of ExRx, into a clinical decision support system, named Prioritize Personalize Prescribe Exercise algorithm (P3-EX), that Prioritizes Personalize Prescribes EXercise for individuals with multiple CVD risk factors. The purpose of this study is to test the usability and feasibility of P3-EX with a validated survey as an ExRx algorithm for clinicians to use among healthy adults with CVD risk factors.
Methods
The University of Connecticut Institutional Review Board declared this study exempt under category 45 CFR 46.104 (d) (2) as research that only included survey procedures that obtain information recorded by the investigator such that the identity of the human subjects cannot readily be ascertained, directly or through identifiers linked to the subjects. Specifically, because the study was exempted, the University of Connecticut Institutional Review Board approved subjects to provide informed consent through the study website as written informed consent was waived. From March 22, 2022 to January 30, 2023, we recruited as many healthcare providers (including physicians, nurses, physician assistants, exercise physiologists, and nutritionists who worked in hospitals) and other professionals working in healthcare-related fields (including biotechnology/pharmaceutical industry, health insurance, corporate/medical wellness, concierge medicine, clinical research, medical health education, and sports medicine) as needed to complete 300 study participants. All the recruitment was completed online. We posted study recruitment information in newsletters from professional organizations worldwide and at professional meetings and presentations. We also emailed study invitations to potential participants within the investigators’ professional networks. In addition, being employed in the professional disciplines above, study participants qualified if they had experience and/or an interest in recommending exercise to patients or clients. The inclusion criteria were: 1) is currently employed or past employed in the healthcare-related professional disciplines described above; and 2) experienced in and/or have an interest in recommending exercise to patients or clients.
During recruitment, we emailed the study invitation to participants, through which participants directly visited the study website. Once on the website, participants read detailed information about the study, provided informed consent, and completed the study within about 25 min. Participants completed the study using the web-based P3-EX algorithm containing a case study constructed by study investigators of a patient who was healthy other than having CVD risk factors that were posted on the study website. The case study included the following information: age, gender, smoking and exercise habits, CVD risk factors, medications, presence of signs and symptoms of CVD, diabetes mellitus, or renal disease, family history of chronic disease and health conditions, and the patient's exercise goals (see Supplement 1 for the case study). After reading the case study, the participants entered information on age, gender, and the presence of signs and symptoms of CVD, metabolic disease, and renal disease, and the desired exercise intensity. From the information entered, the web-based P3-EX algorithm determined if medical clearance was necessary before exercise participation based on the guidance of the ACSM. 1
Then, participants entered information on the CVD risk factors, including BMI, waist circumference, blood pressure, blood glucose, blood lipids–lipoproteins, and medications taken for any CVD risk factor, if any, into the web-based P3-EX algorithm. The web-based P3-EX algorithm then scored the CVD risk factors using the cardiovascular health risk scoring system adapted from the AHA's Life's Essential 8 that the investigators modified based upon the CVD risk factor being treated or not treated with medications.43,44 Study participants then applied the ACSM's ExRx strategies for people with multiple CVD risk factors 21 to prioritize the CVD risk factor posing the greatest cardiovascular health risk. Last, the web-based P3-EX algorithm produced a personalized FITT ExRx for that prioritized CVD risk factor. See Figure 1 and Figure 2 for the workflow of the P3-EX algorithm. Further details on the algorithm have been published elsewhere. 44 The time spent from participants first entering information from the case study into the web-based P3-EX algorithm to producing the personalized FITT ExRx was automatically recorded.

Steps in the workflow of the web-based Prioritize Personalize Prescribe Exercise (P3-EX) algorithm.
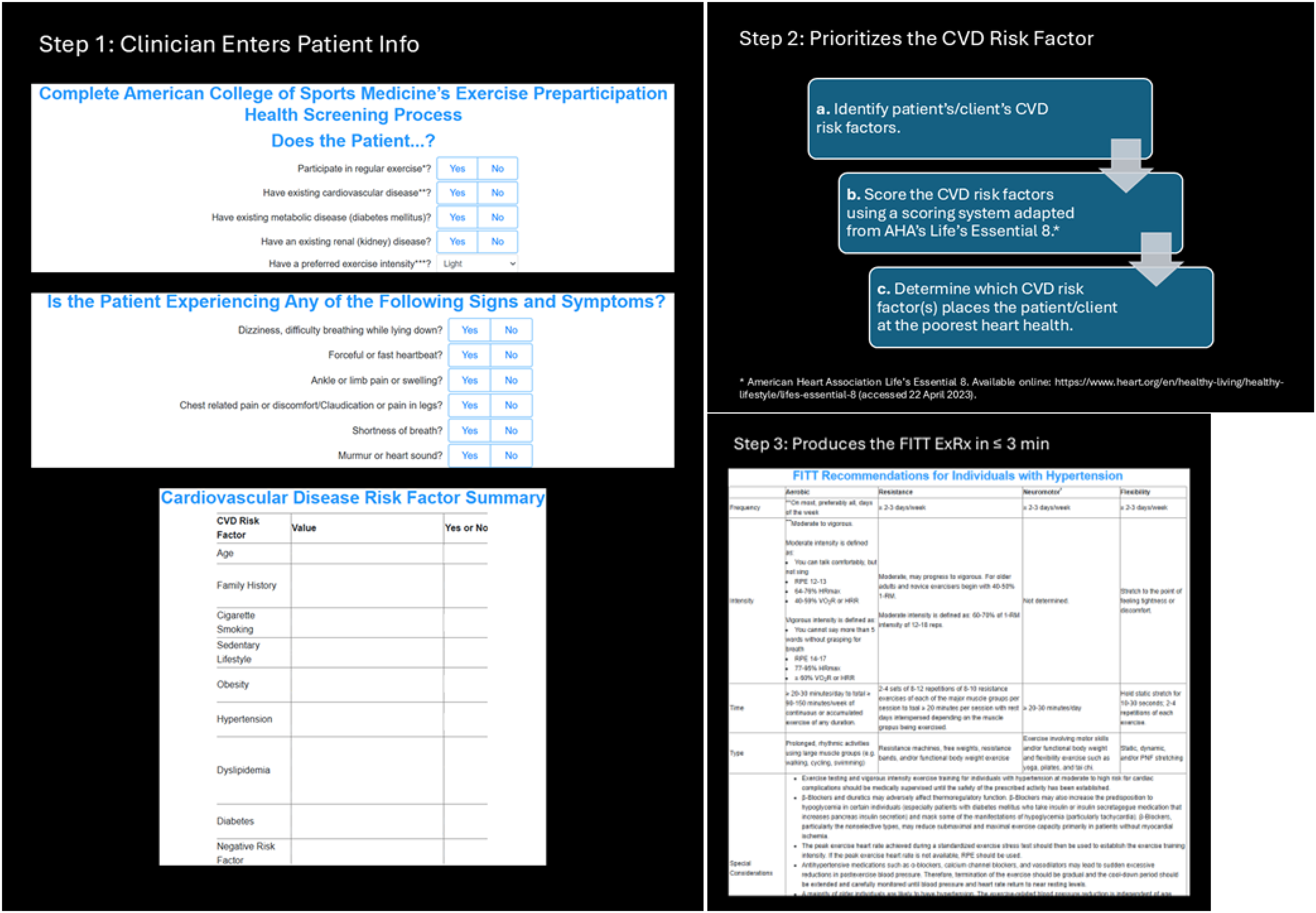
Screenshots of the steps in the workflow of the web-based Prioritize Personalize Prescribe Exercise (P3-EX) algorithm.
Next the participants completed a survey to evaluate the usability and feasibility of the web-based P3-EX algorithm. The study adapted a previously validated survey, named the Mobile Application Rating Scale,45,46 that contained a scale to determine the usability of mobile apps for diabetes management which is a CVD risk factor, and a scale to evaluate the quality of mobile health apps across four dimensions: engagement, functionality, aesthetics, and information quality. We modified the survey by removing questions: 1) about aspects of an app not related to usability and feasibility (e.g., if the app is entertaining); and 2) not applicable to the functions of the web-based P3-EX algorithm. In addition, diabetes-specific contents of the Mobile Application Rating Scale45,46 was replaced with CVD risk factor and ExRx specific contents. Participants responded to each survey question with a number range from 5 (completely agree) to 1 (completely disagree). Participants were not asked to provide reasons for their choice of number. In addition, participants’ demographic information was also collected by the adapted survey (see Supplement 2 for the adapted survey). Of note, the journal the survey was published in is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium. In addition, we have obtained the permission from the copyright holder to use this questionnaire in this study (see Supplement 2 and Supplement 3 for more detail).
Statistical analysis
We used descriptive statistics to calculate the % range of response for each survey question, time spent using the web-based P3-EX algorithm, and the FITT ExRx produced. We then performed a series of chi-square tests to test the associations among participants responses to each of survey questions and their gender, professional background (i.e., healthcare provider vs. other healthcare-related profession), and if the participant met the physical activity guidelines, recommended exercise to their patients, and worked directly with patients. We also performed chi-square tests to test if there were differences between the ACSM ExRx strategy used to prioritize the CVD risk factor and final ExRx FITT produced. In addition, we performed a logistic regression with no covariates to investigate the association between actual time spent to prioritize the CVD risk factor using the web based P3-EX algorithm and the level of participant agreement that using the web-based P3-EX algorithm would save time then when recommending exercise to their patients. All statistical analyses were done using IBM SPSS Statistics (28.0.0.0).
We also performed a post hoc power analysis to compute the achieved power of this study with 309 participants. We used G*Power (3.1.9.4), 47 with the following inputs: statistical test = means: difference from constant (one sample case); tails = 2; effect size d = 8; α error prob = 0.05; and total sample size = 309. The calculated critical t is 1.97 and the power of this study is 1.00.
Results
We sent recruitment email invitations to 844 potential participants. Of these, 309 (36.6%) agreed to participate and all completed the study. Of these, 143 (46.3%) were healthcare providers (see Table 1 for the breakdown of healthcare provider professions), while the remainder were working in the fields of: 1) biotechnology or the pharmaceutical industry (N = 28, 9.1%); 2) health insurance (N = 20, 6.5%); 3) corporate/medical wellness (N = 23, 7.4%); 4) concierge medicine (N = 21, 6.8%); 5) clinical research (N = 24, 7.8%); 6) medical health education (N = 30, 9.7%); or 7) sports medicine (N = 20, 6.5%). The participants were mostly middle-aged (41.0 ± 13.0 years), white (70.2%) females (60.4%) who worked in the US (86.7%) and met the physical activity guidelines for Americans from the U.S. Department of Health and Human Services (92.5%) (Table 1).
The participant demographic information.

*At least 150 min of moderate intensity physical activity or 75 min of vigorous intensity physical activity per week cumulatively. 48
The first series of questions on the survey inquired about the participants’ general satisfaction using the web-based P3-EX algorithm (Table 2, question 1–3). Most participants (80.4%) were satisfied with using the web-based P3-EX algorithm and would use it with their patients (73.3%) and recommend it to their colleagues (92.6%) when it becomes an app.
The survey questions by percent of participants’ (n) answers for each of the five possible responses.

Note: Participants who answered N/A or did not answer were not included in percentage calculations.
P3-EX: Prioritize Personalize Prescribe Exercise.
The second series of questions on the survey asked for the participants’ perceived ease of use of the web-based P3-EX algorithm (Table 2, question 4–9). Most participants (85.4%) agreed the web-based P3-EX algorithm was intuitive and the logic of it was easy to follow (83.4%) (Table 2, questions 4 and 5). In addition, the wording (87.0%), images and tables (79.7%), and click sensitive areas (89.2%) were all perceived as easy to recognize and understood by most of the participants. Last, when asked if the feedback provided by P3-EX was instant and understandable, 86.8% of the participants agreed (Table 2, question 9).
The third series of questions on the survey asked about the participants’ perceived ease to the eye of the web-based P3-EX algorithm (Table 2, question 10–11). Most of the participants felt the color contrast was easy on eyes (79.8%), and the size of the screen and input fields were large enough (90.2%).
The fourth series of questions on the survey asked about the practicality of the web-based P3-EX algorithm (Table 2, questions 12–14). Most of the participants agreed that the fault tolerance of P3-EX was high enough (68.2%), 73.9% agreed P3-EX could save them time when prescribing exercise to their patients, and 79.8% agreed the risk of using P3-EX to patients was minimal. The average time spent using P3-EX to produce the personalized FITT ExRx was 4.6 + 1.8 min.
We performed a series of chi-square tests to examine the associations among participants’ characteristics and their responses to each of the 14 questions. The responses did not differ by gender, if the participants directly worked with their patients or not, and if they regularly recommended exercise to patients or not (all ps > 0.5). The frequency by which participants agreed that they would recommend the web-based P3-EX algorithm to their colleagues differed by profession (p = 0.029) such that 75.9% (N = 82) of healthcare providers agreed, whereas 87.2% (N = 102) of participants working in other professions agreed. Last, we performed a logistic regression to investigate the association between time spent in P3-EX and whether using P3-EX would save time (Table 2, question 13). The participants who spent more time using the web-based P3-EX algorithm to produce the personalized FITT ExRx were more likely to disagree that it saved them time (p < 0.01).
Figure 3 displays the percentage of participants that selected the ACSM's exercise prescription strategies to prioritize the CVD risk factor to focus the FITT ExRx. Over half (54.0%, N = 167) of the participants chose ACSM Strategy C, which was the ExRx that encompasses most of the FITT ExRx for the other CVD risk factors; 12.0% chose ACSM Strategy B, which was the most conservative ExRx regarding intensity and/or volume; and 34.0% chose ACSM Strategy A, which was the ExRx that focused on the CVD risk factor that is the most limiting regarding activities of daily living and/or quality of life. Of the CVD risk factors that the patient had, independent of the ACSM Strategy used, hypertension was prioritized by most of the participants (77.9%) followed by dyslipidemia 12.9%, and obesity 7.1%. However, depending on the ACSM ExRx strategy chosen, the frequency of the CVD risk factor prioritized to focus the ExRx differed (p < 0.001). When using ACSM Strategy A, hypertension was prioritized by most of the participants (83.8%) followed by obesity (13.3%) and dyslipidemia (2.9%). When using ACSM Strategy B dyslipidemia was prioritized by most of the participants (78.4%) followed by obesity (13.5%) and hypertension (8.1%). When choosing ACSM Strategy C, hypertension was prioritized by most of the participants (93.4%) followed by dyslipidemia (4.8%) and obesity (4.8%).

The percentage of participants (n) that selected the ACSM's exercise prescription strategies to prioritize the cardiovascular disease risk factor to focus the FITT ExR.
Discussion
This study tested the feasibility of P3-EX, particularly user satisfaction and usability, as an ExRx tool for healthcare professionals to use for patients with CVD risk factors. The results demonstrated P3-EX had consistently high and favorable participant responses regarding their satisfaction with and usability of P3-EX as an ExRx tool for patients with CVD risk factors. Indeed, 80–90% of the 309 respondents agreed that P3-EX was intuitive, producing high-quality, evidenced-based, individualized ExRx; using P3-EX would make their patients healthier; feedback was immediate and understandable; and they would recommend P3-EX to their colleagues and were satisfied with P3-EX. In addition, over 70% of the respondents agreed P3-EX was safe, would save them time when prescribing exercise, and they would use P3-EX with their patients.
The average time it took the respondents to produce the personalized ExRx using P3-EX was 4 min and 32 s with a standard deviation of 1 min and 45 s. However, when considering only the health care providers, the time for completion was a minute less than that of the overall sample. The average time of a doctor's visit in the US is 17.4 min. 49 Thus, at present, using P3-EX would take 20–25% of the time when the doctor is visiting with the patient. Although there are no data on how much time doctors can allocate to a new task during standard of care, P3-EX should be further streamlined to reduce usage time when developing the minimum viable product for go-to-market testing. Another feature of P3-EX that could be improved is fault tolerance which is the ability of P3-EX to run without interruption. 50 Fault tolerance has a profound impact on the success of an mHealth app by directly affecting: 1) the average time to complete a task, 2) the accuracy of the app, and 3) user satisfaction in general.51,52 Therefore, P3-EX should also consider improving fault tolerance of P3-EX when developing the minimum viable product for go-to-market testing to also improve the time to completion.
The final product of P3-EX is an individualized, comprehensive FITT ExRx that focuses on a prioritized chronic disease or health condition. 42 In our feasibility survey study, participants were given the same case study that had the following CVD risk factors: obesity, hypertension, and dyslipidemia (Supplement 1). Although respondents selected different ACSM ExRx strategies to focus the FITT ExRx, 80% selected hypertension to focus the FITT ExRx followed by 13% selecting dyslipidemia and 7% obesity. Using the ACSM strategies to focus the FITT ExRx on a given chronic disease or health condition is a matter of clinical decision making. 44 Nonetheless, choosing hypertension to be the health condition/ CVD risk factor to focus the FITT ExRx was remarkedly consistent among our sample.
Despite our systematic review of the literature, we were unable to find an established cutoff value to rate inter-user consistency for mHealth apps.42,53 Therefore, we compared the results of our feasibility survey study to a similar study by Marinus et al. 51 In their study, 47 physiotherapists were provided with three of the same case studies and prescribed a FITT ExRx for each. The investigators found a very wide inter-user variability in all elements of the FITT ExRx prescribed and low levels of agreement with the professional guidelines for patients with CVD. 54 For example, the prescribed frequency of exercise ranged from two to seven times per week and time per session ranged from 20 to 120 min. 55 Foccardi et al. provided 26 general practitioners with a standardized clinical case to evaluate their ExRx skills. When the researchers compared the general practitioners’ prescribed ExRx to the professional guidelines, exercise frequency and intensity were under-dosed, and there was significant heterogeneity in the prescription of exercise type with resistance exercise generally not prescribed. Specifically, the prescribed frequency ranged from one to seven times per week; time per session ranged from 20 to 60 min; and 8% of the general practitioners prescribed vigorous exercise, 42% prescribed moderate, and 46% prescribed light intensity. 54 Of note, the general practitioners in this study rated their ExRx skills as insufficient, and they would welcome a guidelines-based digital decision support tool to use in their practice such as P3-EX to improve patient outcomes.29,54
Our findings indicate there are important considerations as the P3-EX minimum viable product is developed for future testing. One is the diversity of the participants in terms of race/ethnicity and place of work. In our study ∼30% of respondents belonged to minor ethnicity and racial groups, while 70% were white (Table 2). Moreover, 87% of respondents worked in the US, while only 13% worked in countries outside of the US (Table 2). To generate a deeper and wider understanding of the feasibility of P3-EX, future work should involve participants from underrepresented ethnicity and racial groups nationally and internationally. Most of the respondents in our study met or exceeded the amount of physical activity recommended in the Physical Activity Guidelines for Americans (Table 2). 48 Because physically active health care providers are more likely to recommend exercise to patients, 24 having an overall physically active sample may limit the generalizability of our findings. To avoid similar limitations, future work should include a less physically active sample.
Despite our positive findings, we plan to continue to improve the functionality of P3-EX in the following ways. First, is to improve the design of graphs and tables because the respondents rated them the most unfavorably, that is, “strongly disagree”, among all questions in the survey (Table 2). Second, is to test the feasibility of the algorithm under specific real-world test settings with patients. Third, is to enhance the scalability of P3-EX so that its function will include services targeting clinical populations with other chronic diseases and health conditions, other lifestyle behaviors such as diet, behavioral prompts, real-time monitoring with wearables such as electrocardiographic monitoring for patients in cardiac rehabilitation.
Our study has several strengths. The first is its ability to collect and analyze data from a large sample of 309 respondents. Although we did not perform a priori sample size power calculation, our post-hoc power calculation indicated the study was more than adequately powered. Furthermore, the large sample size of this study is generally uncommon among health care app evaluation survey studies that typically have samples ranging in size from 45 to 115 participants. 55 In addition, as far as we are aware, we are the first study design to purposefully include participants from eight different types of professionals working in healthcare and healthcare related fields 56 enabling us to capture a wide range of perspectives on the feasibility of P3-EX. Last, based on our recently published systematic review of publicly available digital exercise applications, no app on the market covered the evidence-based functions and P3-EX does.42,56
Conclusion
We found that healthcare professionals and professionals working in healthcare related fields consistently rated P3-EX favorably regarding usability and user satisfaction, being well received as a digital ExRx tool to be used in clinical practice. P3-EX meets an unmet clinical need; nonetheless, fault tolerance and the time to completion can be improved when developing the minimum viable product for future market testing.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251360884 - Supplemental material for An exercise prescription algorithm for clinicians to use with their patients with cardiovascular disease risk factors
Supplemental material, sj-docx-1-dhj-10.1177_20552076251360884 for An exercise prescription algorithm for clinicians to use with their patients with cardiovascular disease risk factors by Shiqi Chen, Yin Wu, Justin Kennedy, Gregory Panza, Margaux Zwierko Guidry, Linda S Pescatello and in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251360884 - Supplemental material for An exercise prescription algorithm for clinicians to use with their patients with cardiovascular disease risk factors
Supplemental material, sj-docx-2-dhj-10.1177_20552076251360884 for An exercise prescription algorithm for clinicians to use with their patients with cardiovascular disease risk factors by Shiqi Chen, Yin Wu, Justin Kennedy, Gregory Panza, Margaux Zwierko Guidry, Linda S Pescatello and in DIGITAL HEALTH
Footnotes
Ethical considerations
This study is determined to qualify for exemption, and thus approved by the University of Connecticut Institutional Review Board on February 18, 2021. The referral number is X21-000.
Author contributions
Shiqi Chen contributed in the following ways: 1) concept, design, and data interpretation; 2) recruitment; 3) drafting of the manuscript; 4) coding of P3-EX algorithm; and 5) final approval. Yin Wu, and Linda Pescatello contributed to this systematic review in the following ways: 1) concept, design, and data interpretation; 2) recruitment; 3) drafting of the manuscript; and 4) final approval. Justin Kennedy contributed in the following ways: 1) coding of P3-EX algorithm. Gregory Panza and Margaux Guidry contributed in the following ways: 1) concept, design, and data interpretation; and 2) recruitment.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Linda Pescatello is the owner of P3-EX LLC, a software company that prioritizes, prescribes, and personalizes exercise (P3-EX) for individuals with cardiovascular disease (CVD) risk factors, and inventor of the intellectual property (IP) of P3-EX which could benefit from this research.
Guarantor
LSP.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.