
Abstract
Objective
Youth mental health is a global challenge often compounded by fragmented services limiting access. In Canada, Integrated Youth Services (IYS) provide centralized access to youth health services, with youth engagement playing a key role during development and implementation. This study aims to identify key factors influencing youth engagement in mobile health (mHealth) development within an IYS setting.
Methods
We conducted 23 semi-structured interviews with youth, clinical service providers, and non-clinical staff involved in mHealth services at Foundry. The Consolidated Framework for Implementation Research guided deductive thematic analysis.
Results
We identified key facilitators and barriers across five domains: Recognizing core value of engagement, improving external coordination, addressing internal organizational challenges, mitigating power imbalances, and tailoring implementation strategies.
Conclusion
The findings highlight the need for inclusive approaches, regulatory frameworks, and strategies to engage underrepresented youth. Future efforts should prioritize iterative learning systems and safe, supportive spaces for meaningful youth engagement.
Keywords
Introduction
Youth mental health has emerged as a critical global health issue, with increasing recognition of its impact on individuals and communities.1,2 Traditional mental health services struggle to provide care to youth aged 12–24 due to barriers like accessibility, stigma, and inequality,3,4 leading to many calls for developmentally appropriate solutions. In Canada, the mental health system has faced longstanding criticism for its fragmentation, inadequate resources, lack of responsiveness, and inefficiency in addressing the diverse needs of youth across provinces and territories. 5 Integrated Youth Services (IYS) have become a key Canadian solution by offering a single access point to various health and wellness services, including mental health and substance use care, physical and sexual health services, peer support, and social services. 6 Alongside the establishment of IYS, the COVID-19 pandemic was a catalyst to transform IYS by introducing mobile health (mHealth) services. 7 Since 2020, mHealth has become an alternative modality to IYS in-person service access and provision. 8 Early evidence showed integrating mHealth within an IYS setting addressed an unmet need by offering accessible, scalable, and flexible support options such as virtual counseling, peer support, physical and sexual health services, support with obtaining employment, access to groups and workshops, and a library of tools and resources. 8 These tools were designed to be culturally and developmentally appropriate, particularly for youth who face barriers to traditional in-person care. 9
Despite its potential, the sustainability of youth mHealth applications and interventions remains a significant concern for many IYS developers, health providers, and policy makers. 10 Current mHealth tools in youth mental health sectors are highly unregulated and vary significantly in terms of evidence level, measurement, delivery modalities, and evaluation standards. 8 The user retention rate of mHealth apps is also concerning, particularly given the substantial resources invested in their development, raising fears that these services may disappear shortly after their launch.11,12 A previous study from our team gathered perspectives from mHealth stakeholders regarding what contributed to the sustainability of mHealth services. 13 Regular meaningful engagement was identified as a crucial element, with stakeholders emphasizing its importance for understanding the desired features of a successful mHealth service and integrating these insights to better accommodate the needs of youth.
Youth engagement, in this context, can be defined as the intentional, ongoing process of working collaboratively with youth to ensure that their voices, ideas, and lived experiences are meaningfully integrated into the decision-making, design, implementation, and evaluation of programs and services that affect them. It emphasizes youth as equal partners rather than passive participants, fostering empowerment, accountability, and relevance in health service development.14–16 However, youth are often consulted too late or too superficially in the design and delivery of mHealth tools, resulting in services that do not reflect their lived experiences or evolving needs.17,18 In other IYS service streams such as substance use and peer support, true engagement goes beyond consultation. 19 It requires shared decision-making, trust-building, and long-term collaboration with youth throughout every stage of the mHealth development process. 20 Supporting youth as co-creators in mHealth innovation is not only ethically important, but also essential for developing interventions that are usable, relevant, and sustainable. 13
At this time, the concept of “engagement” in mHealth development is unclear in the literature. 8 In some research studies, participant engagement was defined in terms of factors reflecting service utilization, such as the total number of accesses to the intervention, total time spent using the service, frequency of use, and depth of content accessed.21–23 The concept of engagement in other studies is frequently linked to user retention, and researchers assess engagement levels to determine how to maintain users to stay connected with mHealth services. 24 An alternate interpretation of participant engagement in the literature valued and described a civic engagement perspective: The way in which individuals or communities participate and contribute to the development of interventions or processes in their societies. 25
As IYS moves towards mHealth being a core component of the service model, it is critical to have a strong definition of what engagement means from the perspectives of diverse stakeholders who develop and use mHealth IYS. In the context of mHealth development for youth mental health and IYS, this study explores the concept of engagement, emphasizing the importance of involving youth as active, informed, and responsible actors in the development and scaling of mHealth interventions to support their health and wellness.
For this study, the overarching goal is to understand what constitutes successful youth engagement implementation in an IYS setting to support mHealth service sustainability and benefit all stakeholders involved. Specifically, the research questions are (1) What factors influence youth engagement within an IYS setting to support mHealth technology and service development; and (2) What actions are needed to ensure meaningful youth engagement in mHealth development and sustainability planning over time?
Methods
Study design
This study used a qualitative, deductive approach guided by the Consolidated Framework for Implementation Research (CFIR) to explore the implementation of youth engagement in mHealth service development within an IYS setting. We used semi-structured, in-depth interviews with three priority participant groups within an IYS initiative. This included: (i) Youth who received care; (ii) clinical service providers who delivered care; and (iii) non-clinical staff who are involved in the system of mHealth delivery. Our team felt that a qualitative approach was particularly well-suited for this study because it allowed for a deeper exploration of the complex, nuanced experiences and perspectives of participants involved in youth engagement within mHealth development and implementation. Unlike surveys, which tend to provide more structured and quantitative data, semi-structured, in-depth interviews were chosen to allow our team to capture rich, detailed insights into participants’ motivations, challenges, and context-specific experiences. We recruited participants from an IYS initiative in British Columbia (BC) called Foundry. After providing information about the study, we obtained written consent from all subjects to participate in the interviews. Ethical approval was received from the University of British Columbia Office of Research Ethics Behavioural Research Ethics Board (#H22-03454).
The Consolidated Framework for Implementation Research
The CFIR is a widely utilized framework that provides a comprehensive structure for evaluating implementation processes across various settings. 26 The constructs of CFIR are organized into five domains: intervention characteristics, outer setting, inner setting, characteristics of individuals, and the process of implementation. 27 By categorizing these elements, CFIR facilitates the systematic assessment of potential barriers and facilitators impacting the uptake and sustainability of an intervention.
Study setting: Foundry
Over the past nine years, a province-wide IYS initiative, Foundry, was developed, implemented, and scaled to maximize healthcare reach for youth living in BC, Canada. Foundry launched its provincial virtual service in April 2020, including the Foundry BC app, allowing youth to access online health resources, schedule appointments with service providers, and communicate with service providers using chat, audio, or video calls. Participants for this research were recruited within the Foundry initiative. We chose to focus first on Foundry because it is the most established IYS initiative in Canada to date. At the time of this study, Foundry had 17 centers open, 18 in development, and a fully operational mHealth service. As well, Foundry has a central backbone administration office (>130 staff) that supports all centers and the virtual service to deliver evidence-based services to youth and families/caregivers. This provides an ideal opportunity to explore the concept of engagement within a new service (mHealth) and a growing system (the Foundry initiative).
Study sample
We recruited three groups of mHealth stakeholders. See Table 1 for the description of each group and how they were recruited.
Description of the three groups of mHealth stakeholders recruited for this study.

Data collection
Qualitative data were collected through 23 one-on-one semi-structured with researchers (XD, SB) online interviews until saturation. The open-ended questions were supported by previous research, 13 guided by previous research on implementation using the CFIR framework, 26 and constructed based on how participants think of engagement and their past youth engagement experiences (See examples in Appendix).28–30 All interviews were recorded and transcribed using Zoom. Notes were taken during the interviews to provide additional reference for later data cleaning processes. All participants were given an alias throughout to protect privacy. Additionally, two participants were provided with a summary of the preliminary findings and invited to give feedback, ensuring that their perspectives were accurately represented and enhancing the credibility of the research.
Data analysis
This study used the CFIR to guide our qualitative data analysis, ensuring a thorough examination of contextual factors influencing the implementation of youth engagement in an IYS setting. Deductive thematic analysis 31 was conducted using the domains and constructs outlined in the CFIR. 26 The lead (XD) and senior (SB) authors created a coding scheme that mapped back to the CFIR constructs, predefining the codes so that we could deductively identify relevant patterns in our data and systematically categorize the data according to the CFIR framework. The research team employed a trustworthiness strategy during data analysis. 32 Before coding the data, the coders (XD, SB) reviewed and discussed CFIR constructs definition thoroughly, coming to a collective understanding of the codes. We recognize the data analysis was informed by the positionality of the authors, acknowledging their distinct perspectives and experiences. Author XD, a young health researcher with experiences in lower-resourced setting, brought a research focus on improving health care access, particularly for youth navigating barriers to mental health services for equity-deserving population. Author SB is an occupational therapist and clinician with extensive experience in youth mental health, offering a practice-based perspective on the integration of mHealth interventions.
Several strategies were employed throughout the analysis to ensure the trustworthiness of the findings, COREQ checklist can be found in the supplemental file. 33 We applied triangulation by involving multiple researchers (XD and SB) who independently and collaboratively coded and reviewed data from different stakeholder groups. Regular peer debriefing sessions were held during weekly research meetings with co-authors to reflect on emerging interpretations and challenge underlying assumptions. We also made space to examine deviant or negative cases (e.g., qualitative data that may contradict the existing CFIR constructs) to ensure a comprehensive and balanced analysis. Data saturation in deductive analysis was determined when all framework categories were fully represented, and no additional subthemes emerged from each group. Once the data were coded, we verified key themes and patterns by reviewing the coded data under each CFIR domain to look for commonalities and draw connections between the constructs. We took notes on how existing CFIR constructs explained our data and identified gaps in the frameworks’ application to the IYS mHealth context.
Results
A total of 23 mHealth stakeholders participated in this study, with 12 youth who have used the Foundry BC App during the past year, six service providers, and five non-clinical staff who were deeply involved in the development of the mHealth services across the IYS initiative. Half of the youth in the study reported having strong engagement experience including volunteering for engagement programs, participating in focus groups, or participating on local or provincial youth advisory committees. Table 2 summarizes the demographic characteristics reported by the participants.
Summary of demographic description of three groups.

Through one-on-one interviews, participants discussed their understanding of the implementation of meaningful youth engagement to support the development of mobile youth mental health services. Figure 1 presents an overarching framework for youth engagement implementation research, adapted from CFIR and informed by our qualitative data analysis results. Each domain will be explained in detail and participants perspectives will be summarized along with highlight quotes.
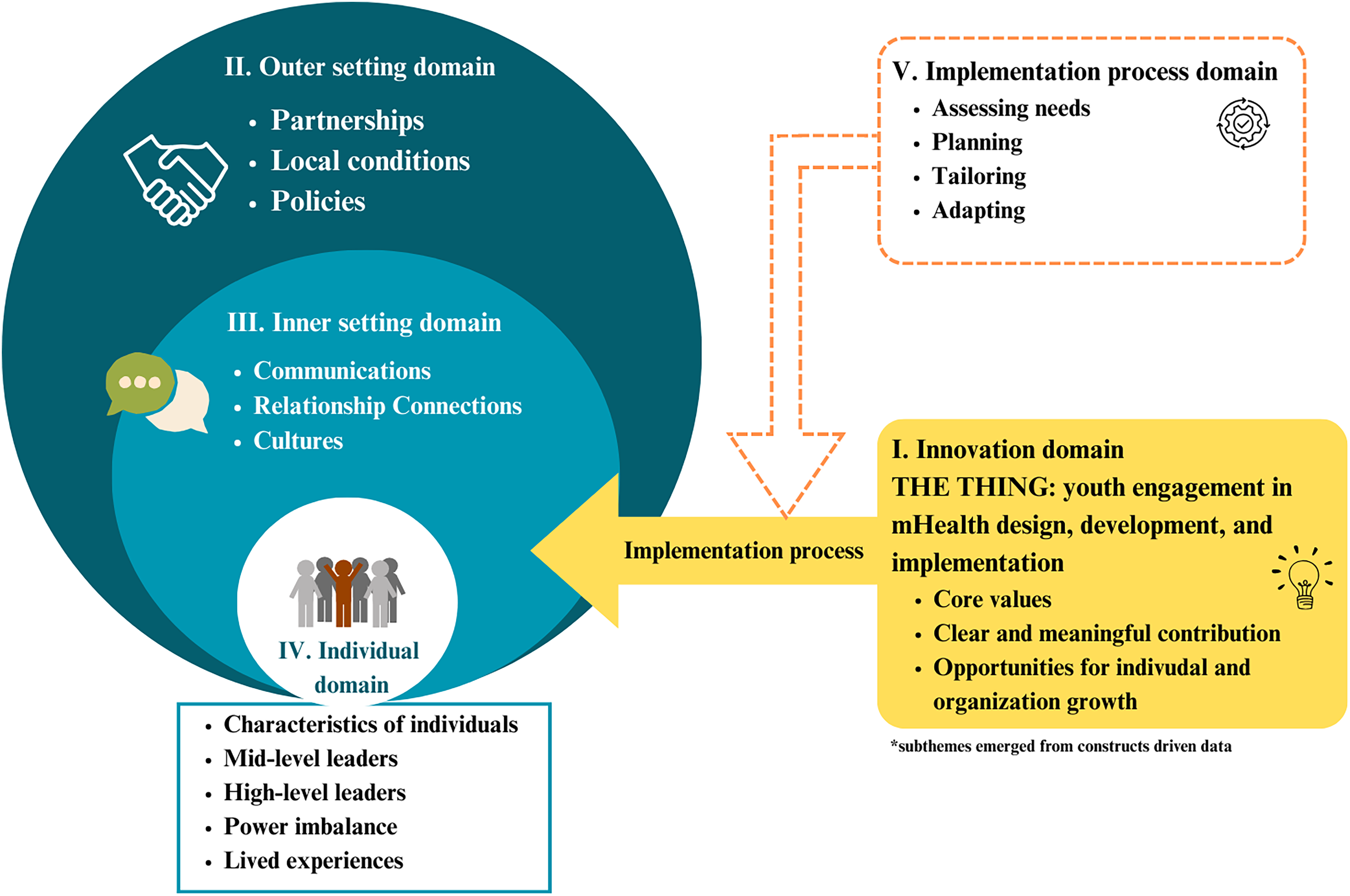
Consolidated Framework for Implementation Research (CFIR) informed by study results. Adapted from the updated CFIR based on user feedback. 26
Innovation domain
The CFIR defines innovation as “the thing” being implemented, and, in this study, 26 refers to the youth engagement plan in mHealth. This section examines participants’ understanding of the concept and core value of “engagement,” setting the foundation for discussions regarding how an engagement plan should be implemented. Participants emphasized that when engagement is effectively executed in mHealth, it involves clear communication of the project's core vision, with well-defined roles that allow both youth and the organization to make meaningful contributions. Additionally, it provides opportunities for continuous learning and growth for both youth and organizations, extending beyond the immediate tasks of the project.
Some participants viewed engagement as a valuable means of treating youth as active mHealth product users, ensuring their ongoing connection to virtual services through consistent outreach. Participants also highlighted engagement as a learning opportunity, focusing less on the mere measure of participant involvement and more on it as a mutual, iterative process of learning.
Collectively, participants acknowledged that engaging youth in mHealth design and development provides organizations with valuable insights into current youth trends, preferences, and the dynamics of online platforms. They emphasized the significance of engagement to enhance service effectiveness and accessibility—especially for reaching underserved populations and transform their lived experiences to meaningful contributions. The whole point of engagement is to access like that one youth. It takes that one youth who [is] in their shell and is hiding because no one is that no one is reaching out to them, and they feel like they're alone. Rachel, youth. The only reason the Foundry BC platform has been successful at all is because we designed it with young people at the beginning. Most of the technology, you see, fail because they were kind of designed with only service providers and nobody else. And they realize, after implementing it is that they left out the voices of the only people they don't pay to use the platform. Allison, tech implementation manager.
Outer setting domain
The outer setting refers to the wider external system and context that can impact youth engagement to support mHealth IYS design, development, and implementation.
Partnerships
External connections and partnerships with schools, community centers, and other healthcare facilities were identified as key factors in facilitating youth engagement to support the development and sustainability of mHealth services. The partnerships described included collaborative educational activities, such as in-person presentations, workshops, curricula, and conferences, aimed at raising awareness and creating opportunities for youth involvement in mHealth development.
Participants highlighted the value of identifying “champions” within schools and communities—individuals who can advocate for and promote the concept of youth engagement at Foundry to support mHealth innovations and growth. Participants emphasized that these champions play a crucial role in increasing local support for both the development of services and the integration of mHealth initiatives with other community-specific initiatives.
Some youth participants shared that their engagement with Foundry often led to new partnerships and opportunities for professional growth. For instance, one youth participant described how their involvement with Foundry resulted in an international collaboration on a global health project. This project focused on engaging youth from lower-resourced areas to co-design mHealth services tailored to their specific living conditions, demonstrating the broader impact of youth engagement in the development of mHealth solutions. Right now we're trying to combine both of the Youth Advisory Committees [here and in Vietnam]. Since youth in Vietnam doesn't have anything like Foundry, so what we're doing with the Vietnamese youth right now is that we're trying to co-design an app for them, to give ideas to help and just be a general support system for the youth, because I know in Vietnam there may be a lot more stigma around youth mental health. Sisi, youth.
Local conditions
Participants identified environmental and political conditions as barriers impacting the implementation of youth engagement in mHealth development and sustainability planning. Some youth reported that they did not feel like participating in such opportunities because of stigma surrounding mental health in their communities or within their own families. Some youth noted that their schools and parents could “get territorial” knowing their youth have been asked to talk about potentially sensitive health information. Participants stressed the importance of understanding local context before asking youth to engage in novel opportunities such as mHealth technology and service development. For example, participants who had experiences working with Indigenous communities reported some local centers used traditional healing power as a part of their therapy sessions, which was not usually compatible with integrated mHealth tools. Participants also identified practical factors such as understanding of the available resources (e.g., local Wi-Fi connectivity, how to pay youth for their time) and what support was needed from the community (e.g., from teachers, parents, Elders) to allow youth to engage in such opportunities. We don't have all the context of what that community or within the school looks like. We don't have context of their Wi-Fi, what their policies are on using phones. We need to work with them and know how [engagement] integrates within their setting. Alex, product adoption lead.
Policies
A major barrier to implementing meaningful youth engagement in mHealth development was the lack of legislation, regulations, professional guidelines, or standards that mandate youth involvement in all processes related to mHealth development and sustainability. Participants stressed the need for regulations to ensure that youth are consistently engaged in the creation of technology and services intended for them. Participants noted that these regulations should also ensure that youth feel supported throughout the entire process and have access to all the necessary information to participate, including the freedom to disengage if they choose.
Participants noted that establishing policies and regulations around youth engagement could be highly beneficial in defining clear roles and responsibilities before the implementation phase begins. They pointed out the complexities within communities that influence who can provide support to youth and who cannot. Building strong infrastructure within the organization was seen as crucial for creating the systems and processes needed to onboard youth, support them during the project, and follow up afterward for ongoing work or professional development. The next section elaborates on this theme in greater detail. Probably there are concerns around credentialing. How do you verify that the person who's providing a service over an app is in a position to be providing mental health care? If I had a teenager, I would want to know that they're connecting with someone in a regulated health profession or with an organization that has some reputability. Lulu, service providers.
Inner setting domain
In this study, the inner setting refers to the Foundry IYS backbone organization, where youth engagement planning and execution often takes place. The backbone organization includes service providers delivering care both in-person at Foundry centers and virtually via the Foundry BC app, as well as non-clinical staff working on program development and implementation. This includes youth and family/caregiver engagement, evaluation, and communications specialists.
Communications (information and technology infrastructure)
Providing multiple ways for youth to submit feedback and communicate was recognized as a crucial aspect of meaningful youth engagement in mHealth, particularly for those who are less vocal and prefer more discreet methods to express their opinions. Participants highlighted that the current fragmented communication system forces them to manually collect and organize information from various channels, such as phone calls, texts, websites, and apps. This lack of integration was reported by participants to be especially problematic in engagement efforts involving multiple stakeholders, as it leads to inefficiencies, increases the potential for errors, and disrupts the timely coordination of responses. As a result, participants noted that quite often the quality and effectiveness of youth engagement are diminished. There's no way to look at a youth's contact information unless we go to the schedule in another old system, and that's only if they book with us on the phone before [when there was no app]. It's annoying that if we have multiple modes of communication let's say if we have all 4 types for an appointment time you can’t edit those times in the same templates or same email schedule. Serene, service provider.
Relationship connections
The involvement of all stakeholders was identified as the primary facilitator for meaningful youth engagement, requiring different parties and departments across the organization to sit at the same table with youth to facilitate engagement experiences. This collaborative approach ensures that diverse perspectives are integrated, and more importantly, youth can feel heard and valued by “people running the place.” At the same time, participants, especially non-clinical staff identified “change management” as a barrier within the organization to the successful implementation of youth engagement in mHealth work. In an effort to include diverse perspectives, introducing new voices from different disciplines can sometimes disrupt existing rapport and engagement processes. For youth who are already involved, it is essential to continuously create opportunities to build relationships with new members and understand their different priorities and work styles. When this is not effectively managed, participants noted that it can result in inconsistencies in goal setting and undermine the trust that youth have built, leading to a loss of sustained engagement. It would only help to be able to engage with the other participants, other groups, the doctors, or of people running it as well. It can be difficult… but if you're just meeting once every month, or once every 2 weeks to have updates on thing, and meet online too. It is really important to have that network going. Rice, youth.
Culture
Participants reported that the implementation of youth engagement requires fostering a culture that is youth-centered, non-judgmental, open-minded, and deeply respectful of diversity which is essential for creating meaningful and effective solutions. Participants proposed that when such culture help services to better meet the specific needs of youth, building trust, promoting a sense of safety, and encouraging participation while fostering innovative perspectives. They also summarized that respect for diversity must guide youth engagement in mHealth settings. This approach supports inclusivity and equity for all youth, including those whose barriers were shaped by their unique community and context.
A key message emphasized by all participants, particularly youth, was the importance of recognizing lived experience from each youth as unique and not easily categorized. This finding highlight youth engagement must occur within a culture that genuinely values the individual experiences of youth, rather than relying on categorization that risks overlooking those who do not speak dominant or mainstream languages. Participants reinforced repeatedly that every lived experience matters, and that youth engagement is essential because it provides a meaningful process through which diverse and often marginalized voices can be genuinely heard and integrated. I think what makes lived experience stand out is that it provides context to what is currently happening in the world and what is currently impacting youth. And it provides diversity perspective and contact. I think especially with the emphasis on intersectionality, there's a lot of things we can't categorize. I find in the academia world we tend to categorize certain things to better digest the information. But lived experience could be really unique to each person. And I think that's what makes it important that young people are talking about what they experience to give the world more insight, what they're actually struggling in real time. Kate, youth.
Individual domain
This domain describes factors contributing to mHealth youth engagement that are relevant to the roles and characteristics of individuals. 26
Mid-level leaders
In this study, individuals with a moderate level of authority to make decisions are referred to as mid-level leaders. This may include patient engagement leaders and those who are hired to support engagement efforts across the IYS organization. Participants emphasized that the key facilitator for youth engagement in mHealth is ensuring that both leaders and youth fully understand their roles and how they can contribute. In our IYS setting, mid-level leaders play a crucial role to help with the communication between youth and decision makers because they understand the needs and desires of both parties. For example, some youth noted that they need adequate time and information to feel prepared for meetings and they identified that mid-level leaders have the capacity to offer such coaching. Mid-level leaders are often overlooked but play an indispensable role, to involve youth in discussions with high-level leaders and decision makers to shape effective engagement for developing mHealth planning and implementation strategies. I think the main thing is (for the engagement specialist) to select people who have an intention to be there and have an intention to make a difference in the health and wellness world. I think that's something that I'm exploring as well is, how do we engage more youth to participate in a Youth Action Council? So maybe they should provide posters with the information that there is a Youth Action Council, and communicate more about training and the benefits. Rice, youth.
High-level leaders
Participants highlighted the essential role of senior leadership in championing youth engagement within mHealth service delivery. These leaders were particularly valued for their ability to set clear, cohesive goals across stakeholder groups and address change management challenges, as discussed in the previous domain. The importance of strong leadership was also emphasized in the context of training new staff, ensuring they understand the value of youth engagement both within the organization and specifically in mHealth initiatives. Additionally, leaders were seen as pivotal in fostering connections across organizations and communities, promoting the work, and articulating the role of youth in all aspects of mHealth, including community-specific initiatives. Retaining well-trained staff throughout the mHealth process was identified as a key strategy to maintain the quality of discussions around youth engagement and to ensure that processes are consistently in place to facilitate meaningful engagement whenever and wherever needed. It's really important to have someone who can effectively facilitate the youth council, someone whose leadership is respected by others in the organization, who has the authority to make decisions, to say no, and to stop things that aren’t working. That person also needs to be someone the young people trust, someone they feel safe around and who won’t compromise their care. Sometimes, organizations impose unnecessary barriers, like requiring youth to be ‘well’ for a year before they can join the council. But in my experience, those barriers aren’t helpful. I’ve worked with youth council members who’ve gone in and out of the hospital, and they’ve been some of the most valuable contributors I’ve ever worked with. So … yeah, you need someone who can make those timely, adaptive, and responsive decisions. Allison, tech implementation manager.
Other implementation facilitators
Recognizing and finding strategies for the youth-staff-organization power imbalance was identified as a rising concern when implementing young engagement into mHealth service design and execution. In youth engagement in mHealth spaces, participants noted that the power difference is often rooted in traditional perceptions of adult versus youth roles, where adult-staff hold formal authority and decision-making power, while youth are often seen as participants rather than partners. Participants reported that staff are typically perceived by youth as more experienced and knowledgeable, which can overshadow the unique perspectives of youth to design a service that is fit for purpose for them. Youth participants discussed how communication dynamics can play a critical role during engagement processes and often reflect imbalances, with staff leading discussions and youth having fewer opportunities to voice their opinions. Participants emphasized the importance of involving youth in decision-making and leadership roles. They advocated for providing training and resources, allowing youth to take lead in mHealth planning and execution, and ensuring transparent processes for equitable participation. Youth felt that open communication empowers them and their peers to engage actively, fostering a sense of ownership and ensuring their voices are truly reflected in the development and implementation of mHealth services. All participants strongly emphasized that incorporating considerations of power dynamics into the implementation process can address traditionally embedded hierarchies and authority structures, mitigate negative feedback from youth, and help close systemic equity gaps across different stakeholder groups. I think youth engagement … there is a power imbalance. There are probably young people getting services from you right now who would like to be on your youth council, and that then creates some struggles in terms of if that same person's service provider is facilitating the council, how do you manage that power, how do you create the safe space for that young person to tell them your idea is terrible, so I think that's where it gets complicated. There has been structural stigma for people to not listen to their ideas.” Allison, tech implementation manager.
Participants emphasized that it is essential to recognize that untrained youth (who have not participated in any health-related field training) have the capacity to engage meaningfully and deliver achievable insights and changes. Youth identified that they are experts in their own lived experience and bring rich experience when it comes to mHealth design and implementation. Youth participants identified that they are the target audience and “consumers,” and they have a better understanding of what a successful mHealth service for youth looks like. In addition to their lived experience, they reported that they felt that they bring deeper insights from their user experience with other online platforms they use for psychoeducation purposes, such as Snapchat and TikTok. We're not really trying to give professional advice here, we're just here to share a perspective and really try to make these services more accessible to youth, you wouldn't need healthcare perspective for that. It doesn't matter even if you have an education or not. All you're doing is just providing your perspective and hopefully making the services more usable for youth. Camile, youth.
Implementation process domain
This section outlines strategies and activities designed to ensure that youth engagement in IYS mHealth is systematic, well-supported, and continuously improving. These efforts aim to enhance the successful adoption and sustainability of mHealth services within an IYS context.
Assessing needs
Participants, particularly those with experience in youth engagement, underscored the necessity of expanding efforts to not only understand the requirements for mHealth services, but also to assess the diverse needs of youth participating in engagement opportunities. Youth participants cited a range of motivations for joining these opportunities, including incentives, volunteer hours, career development in the health field, sharing challenges encountered during their personal use of mHealth services, and a desire to make a positive impact in their communities. Each youth participant emphasized the importance of staff being attuned to their individual needs and personal circumstances when implementing youth engagement initiatives. It depends on their interactive styles. Are they hands on? Are they verbal? Are they more interested in literacy stuff? What do they want out of it? And it really depends on individual differences, how they perceive social cues as well cuz they could have a learning disability or a lot of mental challenges where they don't understand those certain social cues in social environment. Emily, youth.
Planning
All participants emphasized the importance of having a well-defined youth engagement implementation plan before initiating any youth engagement processes in mHealth development or project implementation. They noted that, ideally, this plan should be co-designed by youth engagement experts—not necessarily from the mHealth field, but individuals who understand the best practices for engaging youth in virtual environments. Both youth and non-youth staff stressed the significance of clearly defining when, how, and where to engage youth in the design, development, and implementation of mHealth services.
Participants suggested that youth should be involved from the planning phase and throughout every stage of the mHealth process. They emphasized that youth engagement should be ongoing and sustained over the long term to ensure their input is consistently integrated and valued during the iterative mHealth design process.
Various methods of engagement were proposed, including online surveys, social activities at schools or in communities, focus groups, and youth advisory committees. Additionally, participants suggested numerous venues for youth engagement, such as academic institutions (e.g., high schools, universities), community spaces (e.g., churches, community centers, libraries), social support organizations (e.g., not-for-profit agencies), healthcare facilities (e.g., physician offices, parenting spaces), and online platforms (e.g., social media, virtual forums).
Some participants also proposed paid team roles for youth, which would involve more hands-on mHealth engagement, such as attending team meetings, participating in governance councils, and contributing directly to the development of technology. Overall, participants acknowledged the complexity of youth engagement within the mHealth space and the need for it to evolve alongside the technology and services. While the intrinsic value of youth engagement in mHealth was widely recognized, participants highlighted that adequate planning, resources, and infrastructure are essential to ensure its sustainability and effective integration across the IYS organization.
Tailoring and adapting
Participants also noted that youth engagement for mHealth involves iteratively implementing a variety of strategies to attract and encourage active participation in processes, such as technology development, service planning, and the evaluation of impact. Participants stated that ideal engagement includes an ongoing process of training youth so that they are ready for upcoming needs, rather than reacting to every situation as it arises. Participants noted that it is essential to support continuous recruitment and training efforts, along with offering competitive compensation, to help sustain youth in their roles and attract new youth to the work. Participants noted that, when compared to in-person services, mHealth design and service delivery are constantly changing. Participants suggested that IYS and other youth mental health organizations need to adapt to the ever-changing needs of youth and communities, technology requirements, and outcomes. Although the online “context” is perceived as one community, participants emphasized that it is indeed many more communities and youth coming to access mHealth services. Continuously planning for how to engage different youth in mHealth processes was critical to support all quality improvement efforts and staying ahead of possible innovations and challenges. In summary, participants emphasized that not only must mHealth technology adapt and evolve over time, but also the methods used by Foundry to engage diverse youth.
Discussion
This is the first study to investigate what influences the implementation of youth engagement to support the development of mHealth services in an IYS setting. We used CFIR as a guiding tool to analyze qualitative data collected from 23 semi-structured interviews on stakeholders’ responses on youth engagement in mHealth development and sustainability. Using CFIR provides a systematic way to identify barriers and facilitators across multiple domains, ensuring a comprehensive understanding of implementation processes. It also supports the development of context-sensitive, evidence-based strategies to improve outcomes, particularly in complex settings like youth mHealth services. 26 We identified the following domains and main needs following CFIR: (1) Innovation domain: The need to understand the core value of engagement; (2) outer setting domain: The need to coordinate external partners and policy; (3) inner setting domain: The need to resolve change of management challenge within different teams within organizations; (4) individual characteristics domain: The need to identify youth and staff roles during engagement and recognize the power imbalance; and (5) implementation process domain: The need to assess unique needs, plan ahead and make tailored and adapted coping strategy.
Our results support the existing literature which emphasizes the critical role of engagement in the integration of mHealth services within IYS, particularly because of the diverse needs of youth who come from various personal and cultural backgrounds. 13 Individuals from these groups perceive both facilitators and barriers to mHealth services in different ways, highlighting the importance of involving youth at all stages of the planning, designing, developing, and implementing phases of mHealth initiatives. While CFIR has been used to explore factors influencing mHealth implementation, it has not been applied to studying youth engagement specifically, exposing a significant gap in the research. 34 Previous studies on the engagement of people with lived experience also point to substantial gaps in both understanding and effectively implementing engagement strategies.17,35 The findings of this study contribute to addressing some of these identified research gaps, providing valuable insights into fostering meaningful youth engagement in mHealth services.
In this study, as shown in Figure 1, the innovation domain identified a critical challenge of the lack of clarity among youths and their caregivers regarding the concept and fundamental value of engagement. This study pinpoints youth, in particular, may question the authenticity of engagement efforts, fearing that their input will not be genuinely considered. To address this concern, our study suggested it is crucial to establish regulatory frameworks prior to implementation that ensure compliance with legal and ethical standards while maintaining flexibility to respect the lived experiences of youth, especially in contexts where professional health training is not involved. The outer setting results drew attention to the unique connections to nature and traditional healing practices in remote and Indigenous communities, advocating for a more inclusive and culturally sensitive approach to engagement that incorporates local perspectives, even when working with technology and innovation such as mHealth. Additionally, the individual domain underscores how traditional healthcare hierarchies can create barriers to engagement, with structural stigma often disempowering youth from openly sharing their experiences (see Figure 1). An emerging literature exists about power dynamics in youth mental health, but more research is needed to understand the challenges and barriers in the mHealth context.36–38 These challenges include structural and perceptual barriers, such as stigma, low mental health literacy, and privacy concerns, especially in lower-resourced and equity-deserving communities.39,40 Power imbalances between youth and adults, including clinicians who provide care, engagement specialists who guide the implementation process, and parents who provide consent to engagement activities, can all influence the design, development, and implementation of youth engagement in mHealth interventions. Understanding and addressing these intersecting barriers is critical to developing equitable, accessible, and youth-centered mHealth services.8,40–42
This study highlights a crucial objective of youth engagement: reaching out to those youth who feel isolated and left out. While engaging passionate and empathetic youth for feedback is important, as their motivation and understanding of how they can contribute often lead to significant impact, it is equally important to consider the perspectives of those who are less inclined to participate in mHealth processes. 36 This includes youth who may be less vocal or whose participation is influenced by their wellness status. Strategies to engage these equity-deserving populations include reducing participation barriers, maximizing the benefits of involvement, providing regular feedback, and adopting youth-centered approaches that prioritize equity.43–45 Addressing these gaps and empowering youth to share their lived experiences is essential for driving meaningful healthcare changes and transforming youth-centered health systems. 46 The study also underscores the importance of local “champions” in coordinating and supporting health initiatives. Our data suggest that appointing school and community champions could serve as vital bridges for communication, helping to amplify the voices of underrepresented youth and develop strategies to overcome engagement barriers.
Our study outlines how future efforts to engage youth in mHealth development and design should prioritize developing tailored strategies that address the unique needs of different youth, particularly before implementation, to foster long-term collaboration and meaningful outcomes. It is also crucial to ensure that youth are reimbursed for their time and expertise that reflects the value of their contributions, also acknowledging the potential barriers to participation, such as financial constraints or lack of time. Creating a safe and supportive environment for youth is crucial to avoid tokenism, where youth participation becomes merely symbolic and their influence is limited or nonexistent. It is particularly important to consider the specific needs of equity-deserving groups, including providing accessible avenues for participation, such as informal or flexible methods (e.g., online focus groups, peer support groups, or using creative platforms like art or storytelling) for those who may feel uncomfortable in more formal settings. Additionally, to ensure youth feel safe in participating, it is critical to establish clear guidelines and support systems that promote trust, transparency, and respect throughout the engagement process. A holistic framework, combining thoughtful planning and regulation before engagement, should be established to address both practical and structural barriers specific to mHealth, laying the foundation for effective and sustained youth involvement in mHealth service development. Furthermore, to enhance coordination and facilitate youth engagement both within and outside the organization, it is essential to develop an integrated system that connects various engagement partners, coordinates resources, offers guidance, and encourages continuous learning and knowledge sharing. This is especially important in mHealth development, as it often requires collaboration with external technology teams not traditionally involved in healthcare systems, necessitating additional efforts for knowledge mobilization and alignment across sectors.
Study limitations
This study has several limitations. First, we interviewed three groups of mHealth stakeholders within a single IYS initiative, excluding external community partners and policymakers who often have significant influence in mHealth decision-making. As a result, our sample may not fully represent the broader mHealth stakeholder demographics. Second, although some youth participants were involved in advisory committees and other engagement activities, our recruitment strategy did not specifically prioritize youth with extensive engagement experience. Future research should aim to include a broader range of external partners and policymakers to capture diverse perspectives and to better understand the factors influencing successful youth engagement in IYS settings.
Conclusion
The future of youth mental health care is one “where technology wraps around the problem, not problem around technology.” This work lays the foundation for an evolving system where youth are empowered, their voices are heard, and solutions are not only accessible but tailored to youths’ unique and evolving needs. This study used semi-structured interviews to explore the key factors influencing youth engagement in the development of mHealth services within an IYS initiative. We identified critical facilitators and barriers across domains that highlight the potential of youth engagement to enhance the effectiveness and sustainability of mHealth services while empowering youth voice in youths’ healthcare journey. At the same time, we have identified the need for pre-implementation considerations, the creation of safe environments for youth, the development of an iterative learning health system, and strategies to reach the unreachable youth are future endeavors aiming to optimize youth engagement implementation with the goal to improve stakeholder experiences and health outcomes.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251355345 - Supplemental material for “You can’t categorize lived experiences”: Understanding youth engagement in mobile health in an integrated youth services setting
Supplemental material, sj-docx-1-dhj-10.1177_20552076251355345 for “You can’t categorize lived experiences”: Understanding youth engagement in mobile health in an integrated youth services setting by Xiaoxu Ding, Liisa Holsti, Julia Schmidt, Natalie Parde, Brodie Sakakibara and Skye Barbic in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251355345 - Supplemental material for “You can’t categorize lived experiences”: Understanding youth engagement in mobile health in an integrated youth services setting
Supplemental material, sj-docx-2-dhj-10.1177_20552076251355345 for “You can’t categorize lived experiences”: Understanding youth engagement in mobile health in an integrated youth services setting by Xiaoxu Ding, Liisa Holsti, Julia Schmidt, Natalie Parde, Brodie Sakakibara and Skye Barbic in DIGITAL HEALTH
Footnotes
Ethical considerations
Ethical approval was received from the University of British Columbia Office of Research Ethics Behavioural Research Ethics Board (#H22-03454).
Author contributions
XD: Conceptualization, methodology, data collection, analysis, writing—original draft. LH: Methodology, writing—review & editing. JS: Methodology, writing—review & editing. NP: Writing—review & editing. BS: Writing—review & editing. SB: Conceptualization, writing—review & editing, supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Appendix
Sample Interview Questions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.