
Abstract
Background
The UK healthcare system faces challenges due to an ageing population and chronic bed shortages. An acute hospital-at-home (HaH) model of care can offer an alternative for acutely ill patients requiring hospital admission. However, monitoring thesepatients at home presents its own challenges. We used the National Early Warning Score (NEWS) for patients admitted to a HaH to identify deteriorating patients and ensure safe and timely transfer back to hospital when needed.
Design
Retrospective observational cohort study of patients with selected medical conditions admitted to acute HaH, from an NHS district hospital, between 2014 and 2017.
Results
Of the 502 patients admitted to HaH, 443 (88.2%) were successfully treated and discharged, 1 patient died at HaH (an expected death), and 58 (11.5%) required transfer back to hospital and no fatalities reported after transfer. The AUC for total NEWS was significantly lower for non-transferred patients (14.06) compared to transferred patients (24.71) (p < 0.001). 95% of patients treated at HaH rated their care as excellent or good, and 98% were likely to recommend the service
Conclusion
The study confirms the safe and effective use of the NEWS to identify deteriorating patients in an acute HaH setting, enabling timely transfer back and demonstrating that HaH care can be extended to acutely ill patients. This service could serve as an alternative healthcare system for clinically selected patients. It optimizes resource utilization, reduces the burden on acute medicine departments, and enhances patient experience.
Introduction
Healthcare systems worldwide face challenges due to an ageing population, growing healthcare demands, costs, and shortages of hospital beds and personnel. 1 The Royal College of Emergency Medicine estimates that an additional 13,000 hospital beds are required across the National Health Service (NHS) to drive meaningful change and improvement in patient care. 2 However, this has proven difficult due to chronic bed shortages. The COVID-19 pandemic highlighted challenges in hospitals, including increased patient numbers, resource shortages, and staffing issues, emphasising the need for adaptable strategies to maintain effective healthcare delivery. 3 In response, there was a surge in home-based care models, such as telemedicine and HaH services. 4 The recent Darzi Independent Investigation of the NHS in England emphasised the need for innovation, including a significant shift to community-based care and increased use of digital technology, thus reinforcing the benefits of HaH models of care. 5
HaH is a care service that brings hospital-level staff, equipment, and treatments to patients in their homes for conditions that usually require inpatient care. Studies show that this care model reduces mortality, readmission rates, and costs, while increasing patient and carer satisfaction compared to in-hospital care.6,7 HaH services are to become a key component of the NHS strategy, with the UK government planning to treat up to 50,000 patients a month in virtual wards to alleviate pressure on hospital services, reduce waiting times, and improve care for patients. 8 These services are primarily used by NHS trusts to continue the treatment of clinically stable patients, enabling them to complete their care at home. However, they are not designed for acutely ill patients requiring hospital admission. The care of acutely ill patients at home is quite challenging due to the need for close monitoring and regular assessments. Nevertheless, advancements in technology, such as telemedicine, e-patient records, remote monitoring, and tools like NEWS to identify patients at risk of deterioration,9,10 alongside a dedicated clinical team visiting the patient at home, make this achievable.
In this manuscript, we present our experience with a HaH service for acutely ill patients who require hospital admission. This contrasts with existing HaH models that primarily focus on post-discharge care continuity. The service was operated by ORLA, a private healthcare provider contracted by Bristol Royal Infirmary NHS Trust and Princess Alexandra Hospital NHS Trust, from 15th April 2014 to 15th July 2017. It provided hospital-level care at home for selected patients with acute medical conditions that required hospital admission. To monitor these patients, the NEWS system was used, and the aim of the study was to demonstrate that NEWS can be reliably recorded within a HaH setting and used as a track-and-trigger mechanism to identify deteriorating patients and facilitate timely transfer back to the hospital.
Methods
Study design
We conducted a retrospective observational service evaluation of adult patients admitted to the ORLA acute HaH service. The ORLA Healthcare Institutional Review Board granted the study as a service evaluation; hence, ethical approval and written informed consent were waived (Waiver No. 2017-001), and the study was conducted using fully anonymised data. Over this period, the ORLA HaH team provided 24/7 care for 3000 patients. We analysed 502 patient records, randomly selected by the electronic patient record system used by HaH (Crosscare). We recorded changes in NEWS during the admission period, and compared between patients who were successfully discharged from the HaH service, and those who required transfer back to hospital. All patients admitted under the HaH team were requested to complete a patient satisfaction questionnaire. The questionnaire was developed by the HaH service and was not validated prior to its implementation. It aimed to evaluate the quality of care provided by the service, doctors, and nurses. It also included a Friends and Family Test, asking patients how likely they were to recommend the service to others (Supplementary).
Statistical analysis
Data were analysed using R (version 4.4.1; R Project for Statistical Computing) software. NEWS was considered a continuous variable and was plotted against time for both groups (transferred and non-transferred). The area under the curve (AUC) of total NEWS over time was calculated for both transferred and non transferred patients. We preferred AUC over alternative methods, such as repeated measures ANOVA or summary statistics (e.g., mean or peak), due to the limited data and the advantage of using all available data rather than replacing them with summary measures. To compare AUCs between the two groups, the Mann-Whitney U test was applied. A p-value < 0.05 was considered statistically significant.
Procedure
Patients presenting to the hospital A&E department were initially assessed and referred by A&E physicians or acute physicians to the HaH team. HaH team evaluated the patients to determine their suitability for admission to HaH.
Patients were eligible for HaH admission if they met the following inclusion criteria: were 18 years or older who required hospital admission for one of the seven diagnoses listed in Table 1, had a baseline NEWS (Table 2) of less than 5 and were acutely unwell but clinically stable enough to be managed in a HaH setting (based on clinical judgement). Additionally, patients had to have a home environment suitable for HaH care, reside within an agreed proximity to the hospital, and pass a satisfactory social care assessment by the HaH team.
Care pathways for HaH admissions (CAP, Community-Acquired Pneumonia; HCAP, Healthcare-Associated Pneumonia; COPD, Chronic Obstructive Pulmonary Disease; NIV, Non-Invasive Ventilation).

NEWS system, CVPU: confusion, voice, pain, unresponsive.
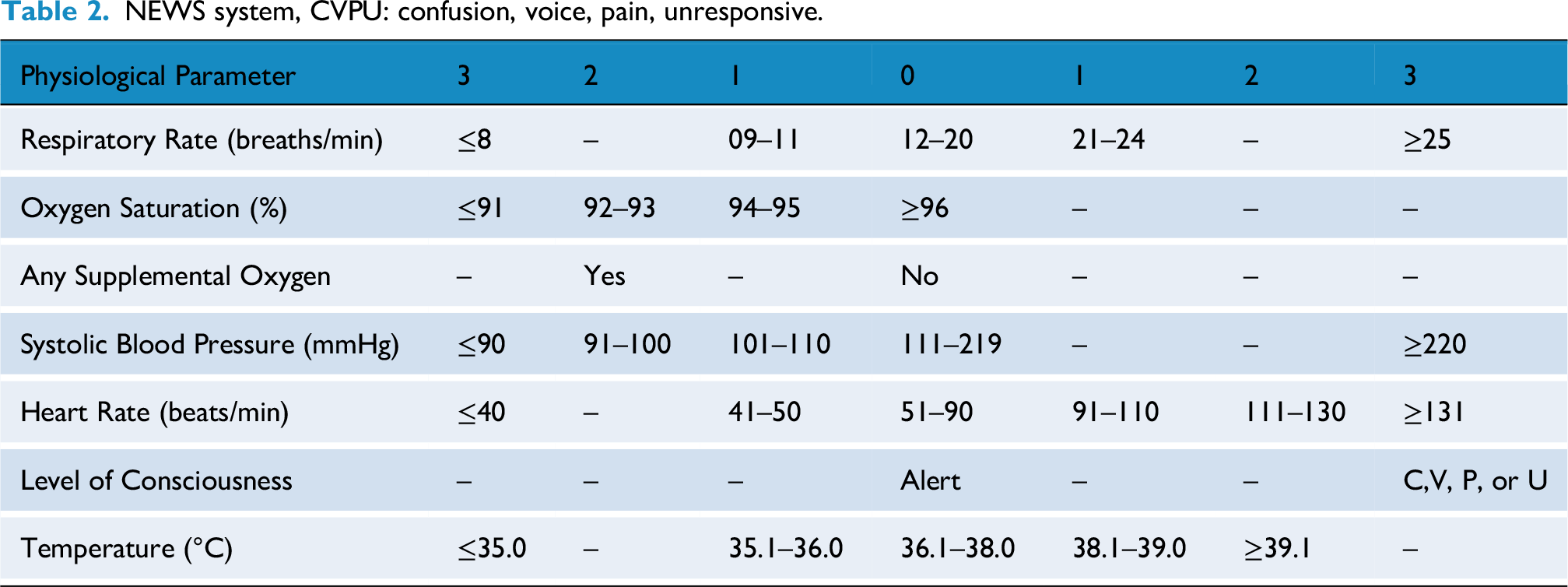
Exclusion criteria included patients with a NEWS score of 5 or higher, as well as those requiring advanced inpatient care, multidisciplinary input, or social services support. The NEWS cut-off of 5 was used, as scores at or above this threshold indicate moderate and high clinical risk and the need for more intensive monitoring and intervention. 11 Patients provided consent prior to admission under HaH. The HaH service utilised a fully developed protocol for conditions admitted under HaH.
Suitable patients were admitted to the HaH service by a senior nurse and a General Internal Medicine-accredited consultant, who also performed the admission clerking. The patients were then transferred home by an ambulance, and the first clinical team visit took place within an hour, at patient's home. Monitoring and telemedicine equipments were installed to record and transmit physiological parameters, observe clinical progress, and calculate NEWS. Patient observations, including respiratory rate, oxygen saturation, temperature, blood pressure, heart rate, and consciousness level, were recorded in the HaH electronic patient records system (EPR) by the visiting nurse and were accessible to all HaH staff via customised tablets and hospital personal computers.
Patients received up to six visits per day by a nurse, along with daily phone calls from a physician, coordinated with the visiting nurse, to assess the patient's clinical status. The number of nursing visits was determined by the admitting team based on their initial assessment and was adjusted as the patient progressed towards discharge. Daily updates on patients’ progress were documented by the clinical team. Physician visits occurred every two to three days or more frequently, depending on clinical needs. Drug charts were left at the patient's home, and any new medications were screened by a pharmacist from the HaH team.
In the event of a patient's clinical deterioration; a two-point increase in the NEWS above baseline prompted a review by a HaH nurse, and then a physician visit if required, and If the NEWS increased by three or more points, an urgent physician review was conducted at the patient's home within an hour to assess whether transfer back to hospital was required.
Results
A total of 502 patients admitted to the HaH service were analysed. Among these patients, 443 (88.2%) were successfully treated and subsequently discharged from the service. One patient (0.2%) passed away (expected death) while under HaH care, and 58 patients (11.5%) necessitated transfer back to the hospital for escalation of treatment. There was no mortality in this group, through that admission period. Charactristics of studied population are given in Table 3.
Characteristics of the studied population

Comparison of NEWS between transferred and non-transferred (discharged) patients from HaH
Mean NEWS (±standard deviation) for patients who remained in HaH versus those transferred back to hospital from Day 0 (D0) to Day 10 (D10) is compared in Table 4. The data indicate that patients transferred back to the hospital had a higher mean NEWS. The AUC for NEWS was 14.06 for non-transferred patients and 24.71 for the transferred group, with the difference being highly significant (p < 0.001; Figure 1). For day-to-day changes in NEWS, the AUC was 3.60 for non-transferred patients and 6.74 for transferred patients, also demonstrating a statistically significant difference (p = 0.01; Figure 2).
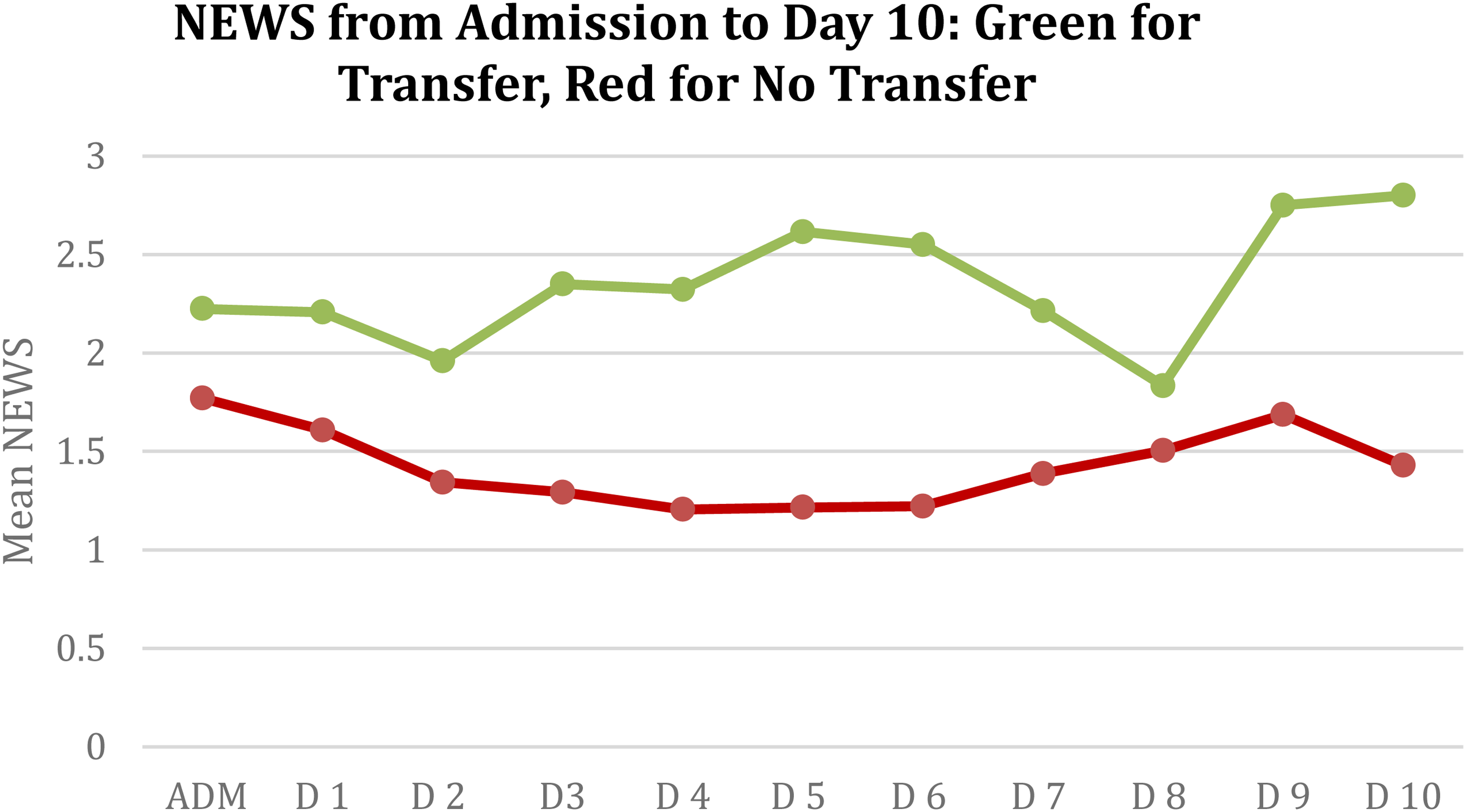
Mean NEWS by day for all HaH patients.

Change in NEWS (Δ), calculated by deducting NEWS on the day from the previous day.
Mean NEWS (±SD) of patients admitted to HaH

Patient experience
A total of 604 participants completed the patient satisfaction questionnaire developed by the HaH service, with 98% of patients indicating they were highly likely or likely to recommend the HaH service to their friends and family. 95% of patients rated their doctors’ and nursing care as excellent or good with regard to communication, explaining their condition, treatment risks within the HaH model, and involving them in decision-making. High satisfaction levels (96%) were also noted for other aspects of the service, including the effective organization, transfers, information provision, and discharge.
Discussion
Our data showed that incorporating the NEWS track-and-trigger mechanism in a HaH setting for acutely ill patients could effectively predict clinical deterioration and ensure timely transfer back to the hospital. We demonstrated that approximately 90% of these patients were safely treated at home, with only 10% requiring transfer, and no fatalities among those transferred back. Additionally, we observed statistically significant differences in total NEWS between patients successfully managed at home and those requiring transfer.
To the best of our knowledge, this is the first study on acute HaH services in the UK. The literature on acute HaH services is limited, with most studies focusing on outpatient infusion therapies and early discharges, rather than on acute care within the HaH setting. 12 Few studies, however, have explored the management of acute conditions at home.13–15 Leff et al. demonstrated that conditions like pneumonia, heart failure, COPD, and cellulitis can be safely managed at home. 13 A randomized controlled trial also confirmed that HaH is safe for certain acute conditions and is associated with reduced costs, fewer readmissions, and higher patient satisfaction compared to inpatient care. 14 For COPD exacerbations, a systematic review showed that HaH significantly reduces readmissions and lowers mortality rates. 15 While previous studies of HaH models have shown promising results, the absence of a standardized mechanism for detecting patient deterioration remains a significant gap. Our study addresses this gap by incorporating the NEWS, offering a systematic approach to patient monitoring.
The use of NEWS as a predictive tool for patient deterioration has been extensively studied and validated in multiple settings. Studies have demonstrated that the NEWS is a reliable predictor of prehospital and in-hospital clinical deterioration, ICU admissions, and mortality across various patient groups.16–20 It is more reliable than other monitoring systems in predicting cardiac arrest, ICU admissions, and mortality. 21 Our data demonstrated that NEWS could be accurately recorded in a HaH setting and could detect patients at risk of deterioration, hence, enabling timely transfer back to hospital. Integrating NEWS into a HaH service helped develop a care model that enabled selected acutely unwell patients to be treated safely at home, thereby reducing pressure on hospital resources and allowing acute hospitals to focus on critically ill patients.
Our data revealed high levels of patient satisfaction with the HaH care model, consistent with previous studies showing high satisfaction with these services.22, 23 Our patients were satisfied with both clinical care and service provision. However, potential biases may exist, as patients who chose HaH care may naturally prefer this model, and those with positive experiences may be more likely to respond and provide favourable feedback. Patient satisfaction is a widely recognized metric for assessing quality in healthcare. Furthermore, high levels of patient satisfaction are linked to reduced emergency attendance, lower healthcare expenditures, and decreased mortality rates. 24
Our service evaluation had several limitations. The retrospective design may have introduced selection bias, which limited the generalizability of the findings and reduced control over potential confounding factors. The lack of a control group and comparison with in-hospital care limited the ability to assess relative effectiveness or safety. We assessed total NEWS rather than individual NEWS components, which made it difficult to correlate deterioration in specific organ systems. We did not collect data on patients following their transfer back to hospital, which limited our ability to assess the longer-term safety of this model. However, there was no mortality, as no mortality root cause analysis was conducted. Finally, the patient feedback tool used in this study was not pilot-tested, and the results may be influenced by response and selection bias.
Conclusion
Our data demonstrate that selected acutely ill patients can be safely treated in a HaH setting. NEWS can be reliably measured in acute HaH and effectively used as a track-and-trigger mechanism to identify patient deterioration. Given the increasing pressure on acute hospitals, HaH has the potential to become an integral part of future healthcare systems for selected patients. Future studies should focus on comparing HaH with traditional in-hospital care and assess long-term outcomes, cost-effectiveness, and patient outcomes in those who deteriorate and are subsequently readmitted to the hospital. Additionally, we recommend using standardised questionnaire tools for assessment of patient satisfaction in future research.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251351374 - Supplemental material for Utilising national early warning score as a track and trigger mechanism in hospital-at-home care for acutely ill patients
Supplemental material, sj-docx-1-dhj-10.1177_20552076251351374 for Utilising national early warning score as a track and trigger mechanism in hospital-at-home care for acutely ill patients by Younes R Younes, Nicholas Cron, Benjamin CT Field, Virginia Yuk-Chun Lam, Ashwin Delmonte Sen, Vidhu Nayyar, James Clark, Sunil Zachariah, Kavitha Lakshmipathy, Lisa Yang, Daniel Johnston, Jackie Row, David Harrop and Julian Emmanuel in DIGITAL HEALTH
Footnotes
Acknowledgements
We acknowledge the support of ORLA Healthcare, which provided acute HaH care for a selected group of patients as described in this manuscript. Additionally, we acknowledge the financial support from Bridges Ventures, a private equity fund, which supported and funded ORLA Healthcare.
Contributionship
YRY: Writing, review & editing. NC: Formal analysis. BCTF: Writing, review & editing. VYCL: Original draft, writing, review & editing, methodology, conceptualization. ADS: Original draft, writing, review & editing, methodology, conceptualization. VN: Writing, review & editing. JC: Writing, review & editing. SZ: Writing, review & editing. KL: Writing, review & editing. LY: Original draft, writing, review & editing, methodology, conceptualization. DJ: Original draft, writing, review & editing, methodology, conceptualization. JR: Original draft, writing, review & editing, methodology, conceptualization. DH: Original draft, writing, review & editing, methodology, conceptualization. JE: Original draft, writing, review & editing, methodology, conceptualization, data curation, supervision.
Conflict of interest
JE, AS, DH, JR, VL, YL, DJ were employed by ORLA healthcare. The authors declare that this did not influence the study's design, analysis or interpretation
Ethical approval statement
Ethical approval was waived by The ORLA Healthcare Institutional Review Board (Waiver No. 2017-001) as the study was granted service evaluation and all procedures performed were part of routine care.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.