
Abstract
Background
In-hospital stay of acutely ill elderlies could be reduced by increasing the availability of community-based hospitalizations. The feasibility of remotely managing these patients by specialized internists, without leaving their nursing homes should be sought. In the current pivotal study, we aimed to evaluate the aforementioned model.
Methods
This was a prospective, open-label study at a tertiary medical center and a nursing home. The study aimed at comparing clinical outcomes of patients hospitalized in each location.
Results
Over a period of 5.5 months, we recruited 18 patients designated for hospitalization, meeting our inclusion criteria to either in-hospital stay or staying in their nursing home and treated by means of telemedicine from our tertiary medical center. The mean age was 85.3 years. Out of 114 hospitalization days, 44 days (48%) were at the nursing home. No significant difference was noted in terms of age, gender, and length of stay between the patients who were hospitalized in either location. In almost all cases, diagnosis changed during hospitalization. Three patients died during the study, all included in the in-hospital group. No safety breaching events happened in the nursing home-hospitalization group.
Conclusions
Remote, telemedicine-based hospitalization of nursing home-dwelling elderlies is safe and feasible, potentially reducing the length of in-hospital stay by almost 50%. Larger studies in this realm are warranted.
Background
The challenge: Avoiding in-hospital stay of nursing home-dwelling elderlies
Nursing home-dwelling elderlies are at high risk for hospitalization not only due to their advanced age but also due to the fact that they are bearing other risk factors for hospitalization: Chang et al. 1 have found, in a cohort of 258,759 veterans, the following risk factors for hospitalization: urban residence, chronic medical comorbidities, auditory and visual impairment, chronic pain, any cancer diagnosis, and social instability—all are frequently shared by residents of nursing homes. Furthermore, these patients are also at a high risk for further deterioration during their hospital stay. Chinnappa-Quinn et al. summarized several observational studies showing that acute hospitalizations, for any reason, increase the risk of cognitive decline among elderlies. 2 Furthermore, in-hospital stay increases the risk of falling, and as Toye and co. demonstrated, this risk increases with “every bed moves”. 3 Hospital stay is also detrimental to elderlies prone to insomnia, 4 elderlies suffering from dementia 5 and malnutrition, 6 and harbors a high risk of further functional decline. 7 Also, staying in the nursing home preserve the continuity for care by the nursing and medical staff with whom patients are already well acquainted. The need, therefore, for diminishing unnecessary in-hospital stay of nursing home-dwelling elderlies is well established.
The feasibility: Recent developments in the realm of telemedicine
One possible way to reduce in-hospital stay of the aforementioned population of patients is treating them via telemedicine technologies, without getting them out of their own bed, at their nursing home. A recent pilot study successfully evaluated the feasibility of applying remote, telerehabilitation for elderlies at home, aimed at their need for congestive-heart-failure treatment. 8 Other authors published successful experiences in remote telerehabilitation programs for elderly patients: for sarcopenia therapy, 9 in the post-stroke setting 10 for chronic obstructive pulmonary disease (COPD) patients 11 and more. Levine and co. evaluated hospital-level care at home settings for acutely ill patients and found it reduced cost and service utilization while improving physical activity and was associated with better experience, with no significant differences in quality and safety compared to brick-and-mortar hospitalization.12,13
During the COVID-19 pandemic telemedicine, historically defined by the NIH 14 as “the use of electronic information and communications technologies to provide and support health care when distance separates the participants”, gained much appreciation and numerous publications spread a wealth of experience applying remote-hospitalization methodologies in variable patients’ populations.15,16 Nevertheless, we did not find previous publications addressing the optional remote, tele-based hospitalization by specialists in internal medicine while patients stay at home, that is, in their familiar surroundings at their nursing home facility.
The challenge of the current study was to establish, as a proof-of-concept trial, the application of remote, telemedicine-based hospitalization in a group of a nursing home-dwelling elderly. Our hypothesis was that telemedicine-based hospitalization would not be inferior to in-hospital admissions of this population of nursing home-dwelling elderlies. This was a collaborative effort of BEYOND, the virtual hospitalization arm of the Chaim Sheba Medical Center, a tertiary hospital in Israel and Amal Holdings, a network of nursing homes in their facility based in Raanana, Israel. This facility is one of the largest nursing homes in Israel with over 500 residents. The current collaboration focused on several nursing departments having an experienced nursing staff, with intravenous drug delivery permits. The physicians in this nursing home were either specialized geriatrics or general practitioners. The collaboration was executed as part of these two organizations’ quest for innovative hospitalization methods intended to improve patients’ outcomes while not breaching the Israeli Ministry of Health regulations requiring daily physical visits by a physician and a nurse in home hospitalization programs. Both Sheba BEYOND and AMAL Holdings foresee great significance in a achieving a preliminary proof of concept in establishing a safe and efficient, tele-medicine based, remote hospitalization as executed in the current study. Future implications of our results will be presented hereof in the discussion below.
Methods
Study design
This was a prospective, open-label, interventional, comparative study. As a preliminary, pilot study, the cohort size was determined by the ethics committee (to be 20) and the study was terminated at 18 patients due to the COVID-19 constraints within the nursing home.
Eligibility criteria
Potentially eligible Amal residents followed the patients’ flow as shown in Figure 1. Inclusion criteria: The residents or their guardians were offered to sign in advance an informed consent to participate in the study in case they develop one of the following complications requiring hospitalization: urinary tract infection, respiratory tract infection, lower limb cellulitis, and other cause of deterioration not included in the exclusion criteria. These disease states were chosen according to the list of disease states that are listed in the current national guidelines as eligible for home, remote care telemedicine. 17 Candidates were sent by ambulance to Sheba's emergency room (ER) and underwent an initial work-up. Following ER physician's decision to admit the patient, the study's physician, a senior internal medicine specialist, and director of an internal medicine ward examined him/her in the ER. In case patients met one of the exclusion criteria, based on the ABCNO criteria for deterioration, 18 they would not be recruited and would be hospitalized in the ward: pending airway obstruction; respiratory distress; respiratory rate of more than 30/min or less than 8/min; oxygen saturation < 90% while receiving supplementary oxygen; systolic blood pressure of less than 80 mmHg or more than 200 mmHg; peripheral pulse rate of less than 40/min or more than 130/min; deteriorating level of consciousness (Glasgow Coma Scale of less than 10); convulsions; deterioration during ER stay; or any clinical consideration of treating staff or study physician.
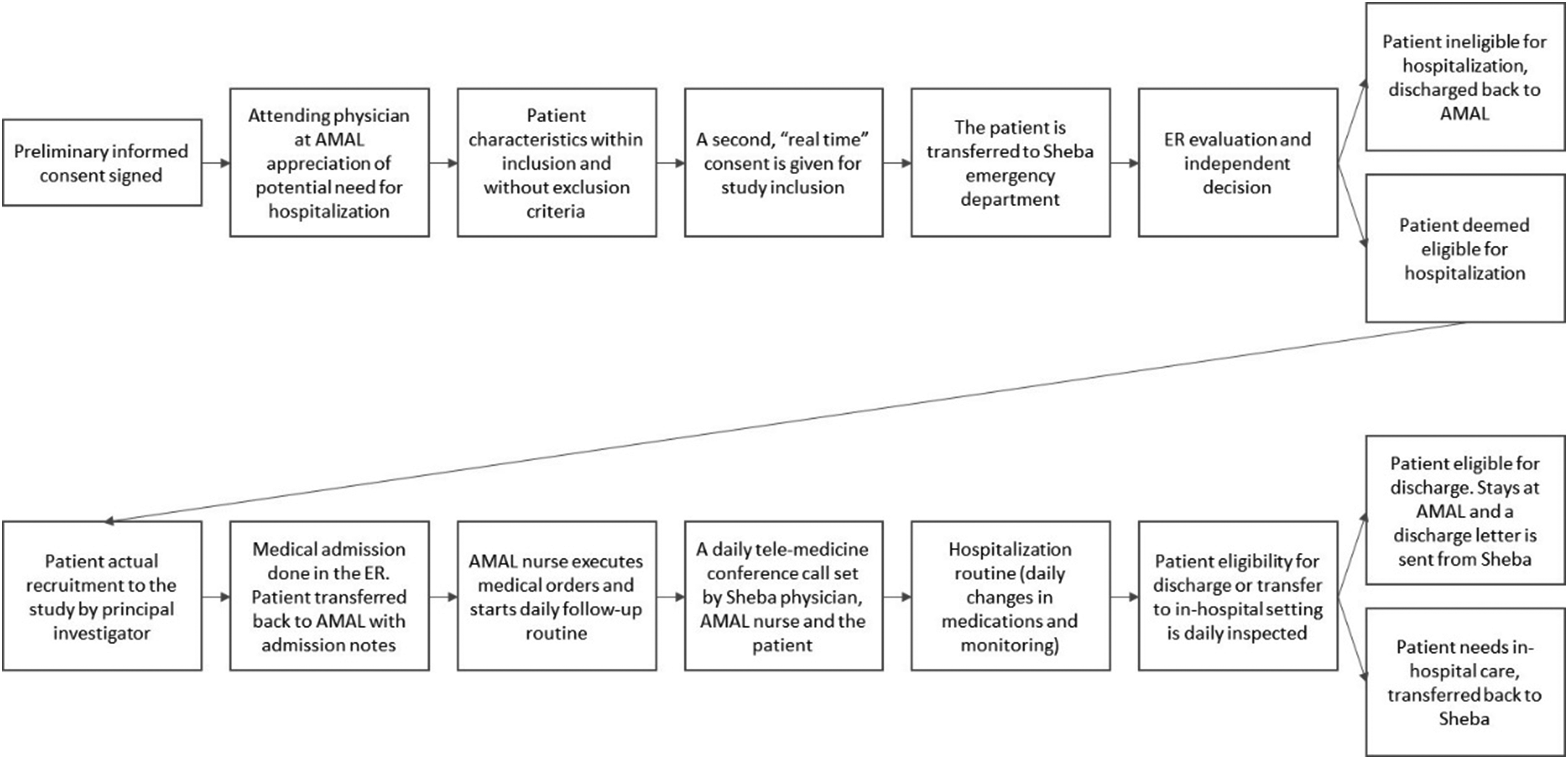
Patient flow diagram.
Study procedures
Eligible patients received a treatment plan and, after coordination with the nursing home staff, were sent back by ambulance to be hospitalized in their own bed. An informed consent was signed by the patients or their guardians during the first 24 hours of home hospitalization. All patients’ data were transferred between the nursing home and hospital staff using a safe box-based email communication.
The home's nursing staffs (sometimes joined by a general practicing physician who is also part of the nursing home staff) executed the medical orders including vital signs measurement, admission of supplemental oxygen, wound treatment, intravenous treatment, and all other nursing care required. The home's staff was in contact with the study physician (a specialist in internal medicine, serving as director of one of Sheba Medical Center’s internal medicine departments) 24/7 as needed. At least once daily, in the morning hours, a remote visit was conducted in presence of the patient and the home's nursing staff with the study physician. During this visit, a remote physical examination was performed using TytoCare®. The TytoCare® system is a digital platform designed for remote physical examination including a stethoscope for heart and lungs' auscultation, a digital otoscope for visualization of the tympanic membrane, a digital thermometer, and a tongue depressor enabling visual examination of the pharynx. The device is equipped with an algorithm that guides the patients (or their assistants) through the process of the physical examination. Data and visuals were recorded and transmitted through the internet to the physician and a video conference was performed. In case a specialist consultation was required, the study physician consulted one of Sheba's consultants. Each daily visit was recorded in the patient's electronic medical record. The visit's summary included orders for blood tests, oxygen supplementation, medication orders, respiratory physiotherapy, and a recommendation to send the patient back to the hospital in case of deterioration or to discharge him/her in case of improvement.
During the entire nursing-home hospitalization period, in case of deterioration, the patient would be returned immediately to the hospital's ward after coordination with the study physician. When the patient was ready for discharge, a letter of discharge was sent to the nursing home's staff and continued treatment plan was transferred to the staff by phone as well to allow optimal continuity of care. The study physician was available for further consultation regarding the patient's care for another week after discharge.
Data recording
Data recorded included demographic (age, gender) and clinical information (e.g. baseline medical status, referral diagnosis, working diagnosis, and prescribed medications), days of in-hospital and nursing home hospitalization, outcomes and complications (falls, acquired infections, new stress ulcers, and delirium).
Statistical analysis
Categorical variables (patients’ gender and initial allocation) are described in proportions and percentage. Continuous variables (age and length of hospitalization) were analyzed for normal distribution and described as mean and SD in case of normal distribution and median and Inter-Quartile Range (IQR) in any other case. Comparison of continuous variables was performed using the ANOVA test. All statistical analyses were double-sided and a p < 0.05 was considered statistically significant.
Ethical declaration
Prior to initiation, this study was approved by Sheba's local ethics committee (approval # SMC-6807-20).
Results
During a period of 5.5 months (August 2020 through January 2021), 18 patients were included in this study. Patients were recruited only after they or their guardians gave a preliminary informed consent to join the study and a second written consent signed upon index hospitalization (either in-hospital or at-nursing home). Figure 1 describes the detailed patient flow in this study.
The mean age of our patients was 85.3 years. The Overall number of hospitalization days was 114, of which, 44 days (48%) were at the nursing home. There were no significant differences in patients' age, gender proportion, and length of hospitalization between patients who spent their hospitalization time in either location. Table 1 details relevant patients' characteristics according to their hospitalization site allocation. Table 2 describes both the gender, group of allocation, age, referral diagnosis, discharge diagnosis, and special remarks. Three fatalities occurred, related to severe sepsis, all during the in-hospital stay. No safety breaching events happened in the AMAL tele-hospitalization group. The overall satisfaction was very high among patients and staff alike.
Patient characteristics according to their main hospitalization site allocation.

Patient initial referral, initial diagnoses, and final discharge diagnoses.
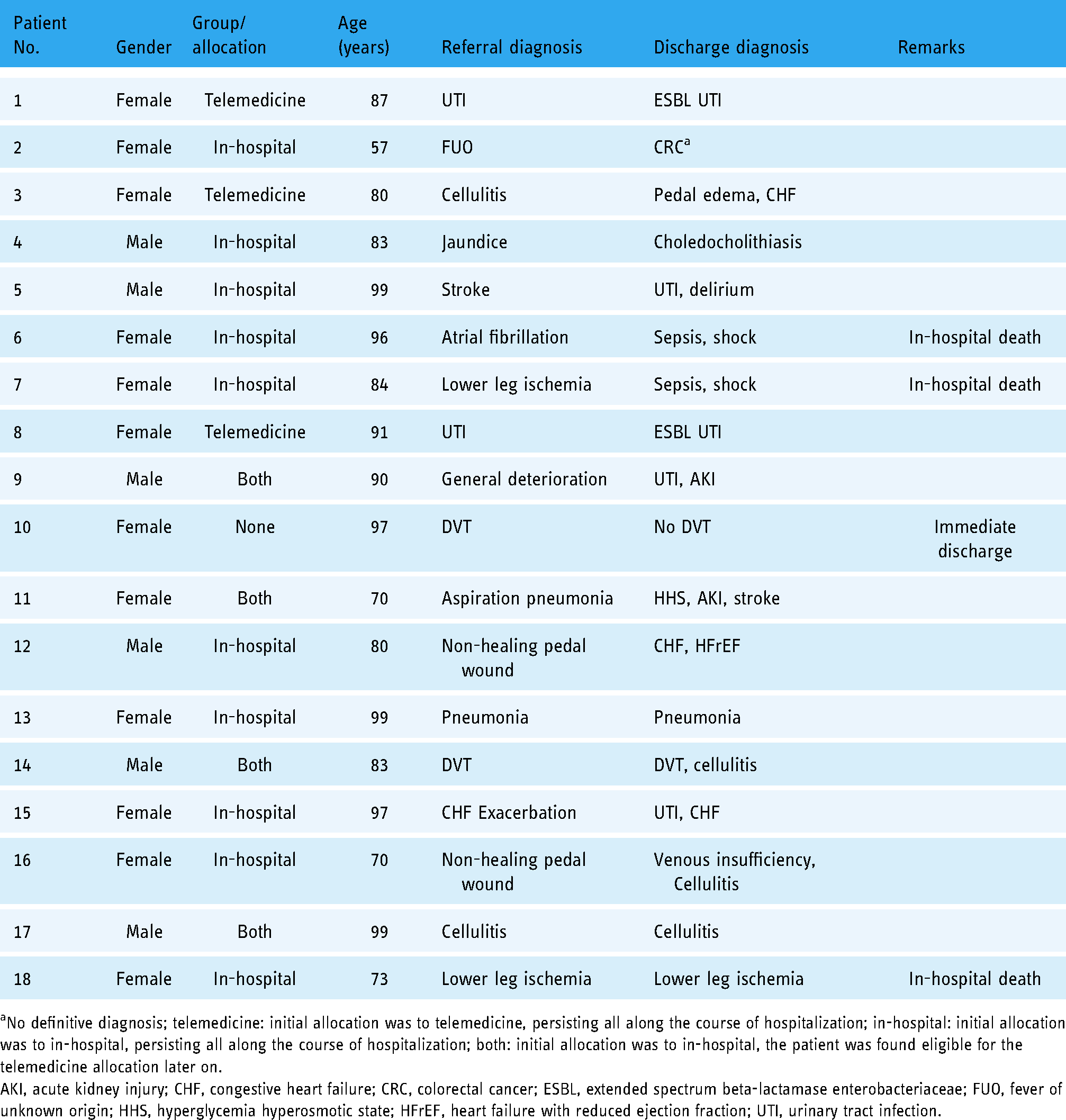
No definitive diagnosis; telemedicine: initial allocation was to telemedicine, persisting all along the course of hospitalization; in-hospital: initial allocation was to in-hospital, persisting all along the course of hospitalization; both: initial allocation was to in-hospital, the patient was found eligible for the telemedicine allocation later on.
AKI, acute kidney injury; CHF, congestive heart failure; CRC, colorectal cancer; ESBL, extended spectrum beta-lactamase enterobacteriaceae; FUO, fever of unknown origin; HHS, hyperglycemia hyperosmotic state; HFrEF, heart failure with reduced ejection fraction; UTI, urinary tract infection.
Discussion
Increasing relevance of hospital-at-home programs
In their November 2020 announcement, the Centers for Medicare & Medicaid Services (CMS) declared that “broad regulatory flexibility” should be employed regarding applications of “Hospital Without Walls” initiatives. 19 This can be regarded as a climax for ongoing changes in terms of hospital and hospitalization care, in variable patients’ settings: In the field of end-of-life-hospitalizations, a recent Cochrane review concluded that hospital at home (HAH) in this setting is feasible and is supported by solid evidence. 17 Kaymaz et al. found out that HAH is both safe, effective, and should be advocated in times of increasing pressure on inpatients' beds requirements for patients with stable COPD. 18 Liong, Lim, and Lai summarized the findings of 10 systematic reviews regarding several paramount parameters of HAH versus conventional in-hospital stay. They concluded that clinical outcomes are comparable or even superior in the case of HAH programs. Also, they showed that in terms of length-of-stay and cost outcomes, HAH programs (both hospitalization avoidance of early discharge models) warrant further attention in times of rising costs and shrinking resources. 19 The current study showed that a HAH program can be based also in a nursing-home, aided by the local professional staff and managed by a specialized, hospital-based, internal medicine physician. In the current study, we proved the feasibility of a HAH model, combining a hospital-based internal medicine department and a community-based nursing home, a model that was not previously sought. This new model, unprecedented in our state previously, should serve as a proof of concept for regulatory authorities when innovative solutions for overcrowded hospitals are contemplated.
Advancements relating to digital remote monitoring and treatment modalities
The current COVID-19 pandemic has accelerated the rate and ease of remote monitoring and treatment technologies as part of telemedicine-based HAH programs. 20 The current study demonstrates the feasibility of using several selected telemedicine platforms in order to monitor elderly patients.
The results of this small, pioneering group of patients showed that careful patient's selection can assure that acute, but stable patients can benefit from staying in their nursing home and still receive tertiary medical services. Triage for patients may be conducted in nursing homes/onsite without transferring them to the hospital/emergency department in future studies. The fact that several referral diagnoses were, eventually replaced by other, discharge diagnoses, further strengthens the rationale of telemanagement of these patients by a specialized physician from a tertiary hospital throughout their stay in their nursing home.
Conclusions
Our study supplied a proof of concept: remote, telemedicine-based hospitalization of nursing home-dwelling elderlies is feasible. Our preliminary findings enforce our initial hypothesis that telemedicine-based hospitalization is not inferior to in-hospital admissions of this population of nursing home-dwelling elderlies. The non-inferiority was demonstrated in the fact that none of the patients that were tele-hospitalized was jeopardized by his/her remote telemanagement. We offer a model that is also scalable and can be applied by “twinning” neighboring hospitals and nursing homes. Further, larger scale studies should implement such models, and also, address financial, reimbursement issues.
Limitations
This was a small, open-label study, serving as a proof-of-concept preliminary research. The encouraging outcomes should serve only as a basis for further, large-scale studies. Also, our findings should be related mainly to the special constellation of cooperative group of hospitalists and personnel of a high-standards nursing home.
Footnotes
Acknowledgments
The authors would like to thank the nursing and medical staff of AMAL Holdings for their compliance and willingness to innovate, for the best interests of their residents. Also, we thank the technical and secretarial faculty of BEYOND, our new virtual hospital at Sheba.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contriburship
All authors had significant contributions for this study.
Ethical approval
This study was approved by the Chaim Sheba Medical Center ethics committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
Guarantor
No guarantees were given regarding this study.