
Abstract
Introduction
Gaps in the health system make it difficult for older adults to have their communication needs and wants heard for that necessary communication to happen. In this study, we investigate attitudes of community-based healthcare professionals (HCPs) regarding the potential utility of a digital technology platform. This platform was designed to enable older adults receiving HCP services in a community setting to provide qualitative narrative impressions and evaluations of their needs and how these needs were addressed by the services. MyHealthMyRecord (MHMR) technology is being designed to provide a digital video-scrapbook for recording and sharing healthcare-related information, observation, and qualitative narratives.
Methods
HCPs were recruited in collaboration with SE Health, a large community-care provider based in Toronto, Canada. Using a user-centered and inclusive design approach, HCPs in community care were asked to comment on the use of the MHMR platform by their patients and to examine a platform prototype. Each session, which lasted approximately 60 min, involved a 40-min semistructured face-to-face interview, followed by a demonstration of the system. Data were analyzed using the Consensual Qualitative Research analysis.
Results
A convenience sample of 7 HCPs, all comfortable with digital technology, participated in the study. The analysis identified 11 themes, with all participants recognizing the value of the MHMR platform in enhancing their capacity to provide services, particularly in tracking to relevant events between patients’ visits.
Conclusions
The HCPs appreciated how the MHMR platform could be used to enhance community health service delivery through valid, reliable, and responsive Person/Patient-Reported Outcomes. It was appreciated that such data could be useful in improving community care experiences while also being useful at a system-wide learning level.
Introduction
Regular access to a known healthcare professional (HCP) is important for effective delivery of preventative health care and the long-term management of ongoing medical conditions. 1 Healthcare professionals are defined as health workers, with whom the person interacts when that person requires care or advice about their health. 2 This can include a family doctor or general practitioner, medical specialist, nurse, and personal support worker (PSW). For this project, we will focus on PSWs and registered nurses/registered practical nurses who provide hands-on continuity of care assistance to older adults and/or persons with complex care needs in a variety of long-term care and community settings. Research has shown that these professionals play a critical role in delivering hands-on care and support across healthcare settings. 3 All people involved in an older adult's health care, coordinate, communicate, and work with each other to set goals, including the person receiving the care.
Continuity-of-care is of particular concern for older adults and their circle of care. This concern will only be amplified in coming years, as older adults are a growing population that relies heavily on healthcare services for chronic or complex health conditions. 4 Currently, the population of Canadians over 85 represents 2.5% of the Canadian population. That percentage is projected to triple over the next 25 years. 5 Each older adult in community care experiences a unique journey, best coordinated through person-centered care (PCC) which by definition involves engagement and participation of the person at the center of the care in healthcare decision-making and is respectful of their autonomy. 6
Currently, tracking of the older adults’ community care journey occurs mainly when an HCP is present to hear, integrate, and record that input. Barriers that limit clinical information gathering are: time pressures; the older adults’/caregivers’ ability to express relevant information during a healthcare encounter; consolidating, and interpreting data during that encounter; and the reliance on the HCP's ability to summarize older adults’/caregivers’ input into their patient chart or electronic health record. 7 In addition, not all recorded information is available to each HCP equally. Retrospectively, this means that patients’ reported qualifying thoughts, concerns, questions, and negative/positive experiences while accessing health services may be lost and may not be available for the types of evaluations and assessments that are necessary for PCC. Furthermore, it is difficult to track changes in the older adult's life and well-being between HCP visits, and then account for the impact of these changes on service delivery effectiveness and outcomes. 8
Patient/person/personal reported outcomes (PROs) incorporated into healthcare records are becoming recognized as important for guiding care management and adaptation. 9 Reports have emphasized the need for such PROs to be fit-for-purpose. There are calls for real-world evidence, including PROs, to be incorporated into evaluations of the safety and effectiveness of medical interventions and innovations. 10 However, those PROs typically require that the older adult fill out standardized questionnaires, which are designed to capture their perspectives and experiences, though there may be variability in patient involvement in the development of these measures. Clinician-driven measures, such as entering quantitative data or journaling, have a high rate of abandonment. 11 The specific challenge of PCC then is to register older adults’ voices within the healthcare system. 12
Clinicians agree that PCC is useful, however, there is no definite consensus around implementation or integration methodology. 13 As a result, patients in Canada are provided with access to their institutional health record items and/or lab results through an institutional portal, yet have no means to interpret data or to provide their subjective input. Given these barriers and systemic challenges, current aspirations for implementing PCC are unlikely to be implemented successfully.
As highlighted in the literature, there is a large quantity of information and accumulated data about chronic illnesses and their reporting. healthcare professionals are under constant time pressure due to the amount and complexity of patient cases they manage.14,15 Additional challenges include, gathering a body of relevant data information and knowledge, interpreting it, and deciding next steps for a patient must be done as quickly as possible but, when data are in many different forms, and lack the patient's input. 13 As a result, HCPs rely on their own professional clinical knowledge and reasoning for deciding the next steps for patients. That pragmatic response presents challenges for respecting a patient's relational autonomy. 16
Patients’ voices, beyond the brief reporting that may occur during an HCP visit, are currently difficult to meaningfully and practically affect health and well-being as specified for PCC practices. 17 There is a need for technologies, training protocols, and efficient, effective, health practices that support PCC and promote new and innovative person-centered health policies. Using a set of technological innovations and methods, we have been engaged in developing and evaluating an inclusive system focused on allowing patients to create, analyze, and share subjective narrative records about their health conditions as they learn to cope with those conditions through accessing healthcare services.
A video-scrapbook technology has been adapted into an early Android-based prototype, called MyHealthMyRecord (MHMR), to explore and demonstrate possible utility of self-directed organization of short duration personally recorded and annotated personal healthcare and well-being-related videos. 18 Patients record personal health and well-being-related events, through short audio-video commentary and narratives, and then optionally add text or graphical annotations to those videos.
Recently, an automated machine-learning (ML) system has been incorporated to help patients analyze and display their data in various graphical and text-based formats, such as bar graphs and textual notes. This new feature of MHMR is designed to convert patient-recorded videos into informative summaries by analyzing audio-video commentary and textual annotations. The ML system extracts key themes, sentiments, and relevant data points, synthesizing them into formats like word clouds and bar graphs (see Tanvir et al., 2021 for details on preferred visualizations for MHMR). 19 We anticipate that this capability will enable HCP to quickly understand the patient's priorities, needs, and overall health status based on their self-recorded inputs.
To drive user-centered design of such functionality, it is critical to understand the needs of potential users, both HCPs and patients. Often the literature focuses on improving patient perspectives and experiences of PCC and less on HCP's needs or what is required in their practice to enable PCC, particularly for chronic conditions. For example, Jaensch et al. 20 distilled 15 academic peer-reviewed publications for contemporaneous agreement using the Santana PCC framework in a systematic review. They found that there was considerable agreement and evidence from patients and HCP on the PCC framework elements, although patients had complaints about the lack of PCC for some elements. However, while patients and HCP agreed on the elements of the framework, e.g., communication is important and the perceived power imbalance between patients and HCP should be reduced, there is little about actionable methods of achieving the framework goals, particularly for HCP. In this paper, we are not only examining HCP needs but also how those needs could be realized with MHMR.
In collaboration with a health-care partner (SE Health, www.sehc.org), we recruited HCPs to participate in a study of how a MHMR platform could guide case management and community care service delivery with those HCPs. This project focused on the HCP interfaces of the system, specifically HCPs providing community-care for older adults. The research objective was to explore the needs and potential utilization by HCPs of patient-generated qualitative data through the MHMR platform in planning, allocating, delivering care, and ensuring care continuity.
Research questions:
What input (concerns, questions, and negative and positive experiences) from older adults are desired by community HCPs? In which format should older adults’ input be provided to be useful and usable by HCPs?
Methods
Study design
The design was a cross-sectional, predominantly qualitative study aimed at collecting data on HCPs’ perspectives regarding the MHMR application, as well as understanding older adults’ needs for tracking their own data and reactions to the prototype interfaces. The main goal of the overall project was to develop and evaluate a platform for older adults to create, record, curate, and share qualitative narrative data content about their health and living/life situations that can be used for improving communication and health management between older adults and their formal caregivers. Data were collected through face-to-face interviews with HCPs from SE Health providing care to older adults living in the community. This study was approved by Toronto Metropolitan University (formerly, Ryerson University) human research ethics board (REB protocol # 2019–297). We used an early MHMR prototype to engage individuals from a range of sectors within the health system, particularly HCPs, in identifying next steps for transforming the prototype into a practical solution. To gather insights on their needs and guide feedback on the functionality of the MHMR interface for communicating patient narratives, we developed visual interfaces that had limited functionality to change between screens and select some on-screen elements such as to change the timeline from days to weeks on the line graph (see, e.g., Figure 1) to share with HCPs.

Example of the MHMR application interface to represent input from HCPs, such as nurses and personal support workers.
Recruitment
We recruited potential participants from community-care HCPs working with SE Health using an information flyer. The flyer was posted at SE health sites, available for 12 months, and included contact details such as the email address/phone number of the Principal Investigator and research team for potential participants to inquire and participate. The initial outreach was conducted through convenience sampling via the flier, followed by purposive sampling to reach potential participants who met the inclusion criteria for this study: participants had to be HCPs working with SE Health, and possess sufficient English language skills, as self-reported by the participants through the recruitment flyer, to engage in discussions. We employed purposive sampling of these HCPs as a strategic approach to enhance the relevance, depth, and efficiency of our qualitative research. Participants were asked to take part in an interview session in person, at a convenient time and location for them. Prior to participation, they read and signed a consent form, which detailed the study's objectives, procedures, potential risks, and benefits, in accordance with the ethical standards set by the Canadian Tri-Council Policy Statement: Ethical Conduct of Research Involving Humans. Participants received incentives upon completion of the survey and interview to acknowledge their time and contribution. After signing the consent form, and agreeing on a meeting time, participants completed a prestudy questionnaire upon arrival. The project was then explained, and the prototype was demonstrated during the interview. Following this, participants engaged in a face-to-face interview. The whole session lasted approximately 60 min and was audio-video recorded.
MyHealthMyRecord system design and demonstration of prototype
The MHMR platform was developed to support the collection and assessment of qualitative data generated by individuals. Older adults share their experiences and feedback about their health with HCPs or family members. In principle, this information can guide decisions regarding their health management and treatment. As a first step in the system design, we recruited a codesigner participant to assist in developing a usable platform. They played a pivotal role in shaping the MHMR design through active participation in the development process. This encompassed contributions to brainstorming, ongoing feedback, validation of design choices, user-interface problem-solving, and direct involvement in usability testing, all of which enriched the project. The details of the system design in our previous published paper.21–23 While the patient perspectives on the system were reported in this earlier research, HCP perspectives were outstanding. Hence, this paper is specifically focused on HCP needs and concerns for, and reactions to the presentation and use of patient-generated qualitative data through MHMR.
The MHMR login page was the first screen that participants viewed. Standard input fields asking for login credentials were present on this page. It was included in the prototype to offer HCPs an idea of the various aspects of the platform design, even though the HCPs would not interact with this part of the actual application because the patient would create the account. The prototype had “Record,” “View Summaries,” “View Patient Videos,” and “Share data” available from the homepage. Because only patients, not HCPs, would use the Record and Share their data functions, they were not functional for this study. The aim was to provide insight into how HCP patients could use the platform.
Data collection: prestudy questionnaire, and interview
The data collection process was organized into two main components: the prestudy questionnaire and the semistructured interview. The prestudy questionnaire gathered general (demographics) information about participants, and their experience with technology. There were two questions on types of computing devices and applications commonly used, and there were two 7-point Likert style questions measuring participants’ opinions on learning new technologies and their comfort with them. The prestudy questionnaire took about 10 min to complete (Appendix 1). Participants were then shown a 10-min demonstration of the prototype, followed by a 40-min semistructured interview. The prestudy questionnaire and interview were conducted by a senior postdoctoral researcher. The interview questions gathered information about how older adults could record their experiences, health information, health services interaction, and how those individuals’ HCPs could benefit from those records (Appendix 2). The preinterview questionnaire used in this study was adapted from an existing validated technology utility tool. This tool is publicly available and does not require copyright permission. To ensure the clarity and relevance of the prestudy questionnaire and the semistructured interview guide, these instruments were pilot-tested with a graduate nursing student who was part of the research team. Feedback from this pilot-testing informed minor revisions to the tools to improve their clarity and focus. The preinterview questionnaire was delivered in English and consisted of two parts: Part I focused on HCP opinions on how likely it might be that older adult's would use the technology, how it could be made more accessible for older adults to document, register, and reflect upon their experience with healthcare services, and their preferences for sharing; Part II explored how the technology and the narratives captured from older adults through MHMR could be helpful to HCPs for assessing and managing their older adult patients. In addition, questions were asked about the features and feedback of the prototype.
Participants
A convenience sample of seven community-care HCPs working with SE Health (1 male, 6 female) were recruited. Six participants were aged 35 to 64, and one was aged 25–34 years old. The years of experience in the current discipline for six participants ranged from 6 to 20 years, and one participant ranged from 1 to 5 years. All participants had used a computer, tablets, and a smartphone/cell on a daily basis. Five participants used medical equipment (such as Digital Monitor, Digital Medication Pumps, Mobile Technology Carts) several times a week to a few times a week. Two participants had never used medical equipment. In addition, six participants never used smartwatches or other types of personal health devices. The majority of participants (6 of 7) used web browsers, office applications, electronic medical records (EMRs), scheduling software, emails, and text/voice messaging applications on an everyday basis. Telemedicine and Internet-based Video Conferencing (e.g., Skype, FaceTime) were used by 5 of 7 participants; however, this study timeline is prepandemic. All participants strongly agreed that they enjoyed learning about new technologies and were comfortable using them.
Data analysis
A Consensual Qualitative Research (CQR) methodology was selected to analyze the qualitative data using multiple researchers to better understand complex data and reduce biases that can result from a single researcher. 24 Consensual Qualitative Research was a common methodology in qualitative research for dependability in exploratory thematic analysis. 24 Team members were able to discuss disagreements respectfully while coming to a consensus on the themes that best captured the meaning of the data. The data analysis process followed a systematic approach. Initially, we conducted open coding on the raw data generated from the HCP interviews, identifying relevant and recurring themes. The coded data were then presented in a frequency distribution table for comparison between themes. 24 Coding was carried out on the raw video data using the Noldus Observer video analysis tool to ensure that nonspeech information could be used as necessary. To enhance the rigor of our study and analysis, we employed a method of counting statements to quantify the prevalence of themes across participant responses. 25 This quantitative approach complements our qualitative analysis by providing a systematic method to identify and prioritize themes that are more frequently discussed or emphasized by participants. By quantifying the prevalence of themes, we aim to uncover patterns and areas of particular significance within our qualitative data. The combination of qualitative thematic analysis and quantitative theme frequency counts strengthened the reliability and validity of our findings.
Method of consensus coding
The first step in the analysis was to formulate domains and themes. Three reviewers reviewed all interview videos. To limit the potentially distorting effects of group decision-making processes and to work cooperatively, a group atmosphere was created in which each individual's opinion was valued. We engaged in an open exchange of ideas in which we sought to understand each other's perspectives.
After the initial “hearing” of each other's views, commonalities and differences were identified. Differences were examined in a spirit of compromise, with the team first agreeing on content and then agreeing on specific wording for each domain and theme. When there was no consensus among the three reviewers, the raw data was reevaluated; the reviewers listened to a recording of the interview and considered the context of the case to help them determine whether the interpretation of the data was correctly identified.
The three reviewers, one postdoc and two nursing graduate students with working experience in clinical settings, worked together on the primary coding, discussing each decision until a consensus was reached. Two senior researchers served as auditors, providing checks at each stage of the domain and theme development process, particularly when there was a lack of consensus or guidance required. They offered feedback to the primary team, which then revised decisions based on this input through an additional consensus process.
This consensus process was central to the credibility and trustworthiness of the data analysis as it allows for triangulation of different researchers’ understanding of the data. An agreement on an interpretation by multiple people gave us more confidence than a single person's interpretation of the data.26,27 The final key feature of the consensual process was ensuring that the data were grounded in the participants’ words, when researchers disagreed on data evaluation.
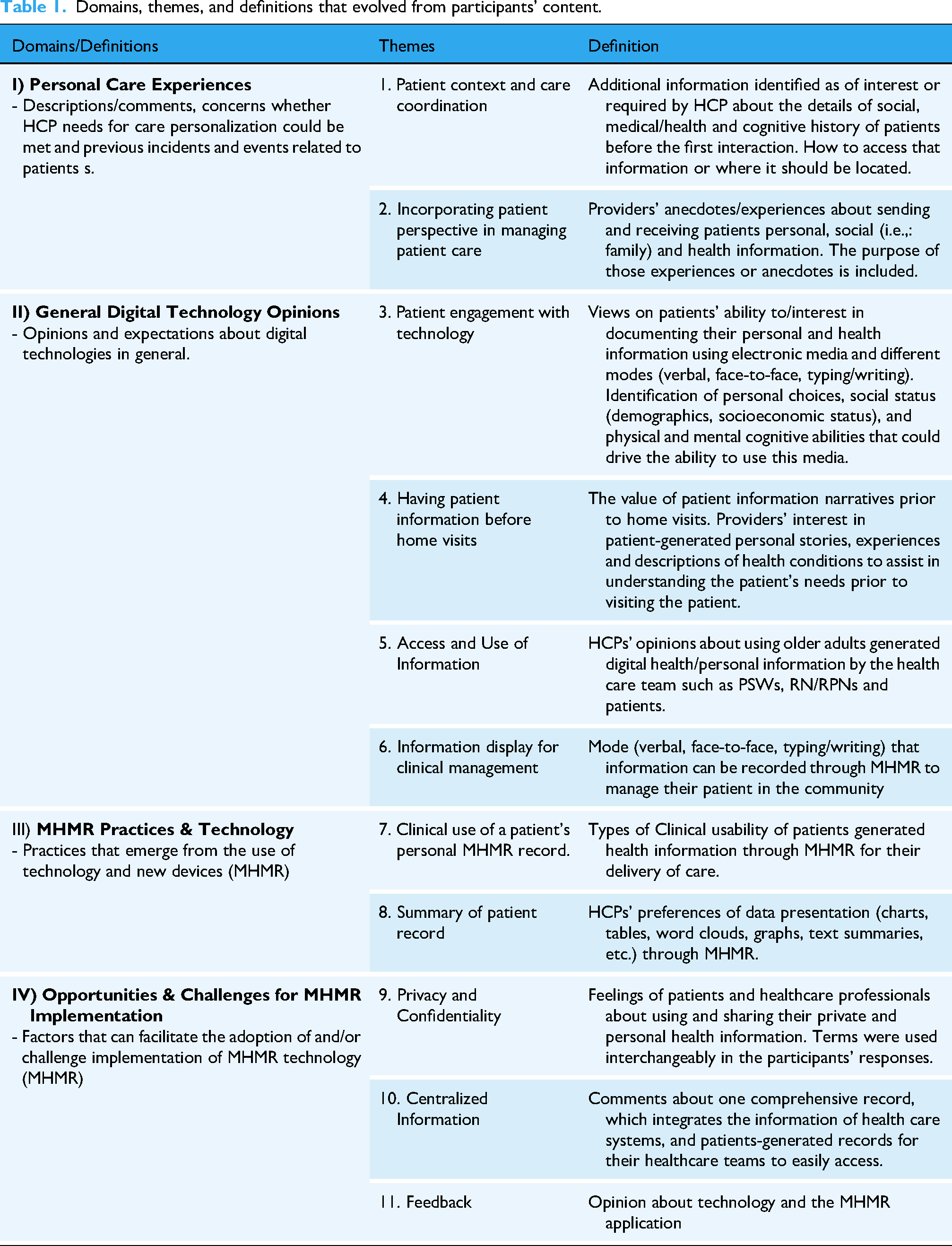
A set of 11 themes was identified and defined (see Table 1). The themes were then organized into four higher-level domains: I) Personal Care Experiences II) General Digital Technology Opinion l, III) MHMR Practices & Technology
Domains, themes, and definitions that evolved from participants’ content.
Themes, modifiers, and quotes that evolved from HCP interviews.

Validity and reliability of the CQR process
Several quality criteria were used to ensure the validity of the coding process and the data interpretation. During the consensus process, initially, a postdoc and two graduate students of the team performed an independent review of the data. One of the senior authors was not only familiar with the topic but also an expert researcher. Her training as a qualitative researcher and older adults enabled her to develop competencies in interviewing skills and an understanding of group dynamics. The consensus process was central to the credibility or trustworthiness of the data analysis because it allowed us to triangulate different researchers’ understanding of the data. When multiple individuals agree on an interpretation, there was greater confidence that others would concur with that interpretation, 26 than if only one person analyzed and interpreted the data. 27 A key feature of this consensual process was returning to the raw data to ensure that the emerging understanding of the data was grounded in the participants’ words. When disagreements arose among researchers regarding data interpretation, they reread the participants’ responses, listened to recordings of the interviews, and considered the context of each case to determine whether their interpretations were informed by the data or influenced by their own biases and expectations.
Results
All seven (n = 7) participants made a total of 126 coded statements; the frequency of coded statements per theme can be found in Table 3. The total number of coded statements per domain was: Personal Care Experiences (31, 26%), Technology in General (43, 34%), Practices/Technology in MHMR (29, 23%), and Facilitators/challenges Related to MHMR (23, 18%).
The details of the number of coded statements, stated by participants per the theme.

* Not all participants made comments on each theme.
In this section, we report how the themes that emerged as important among PSW and Nurses can highlight common understanding and components useful in planning, allocating, and delivering care, and ensuring care continuity. Then, we summarize how these themes were used to inform the MHMR prototype development. In this study, HCPs used “clients” and “patients” interchangeably, therefore, we have preserved the term ‘clients’ only when it appears verbatim in participant responses.
Domain I: personal care experience
1. Context of care coordination
To achieve optimal health or wellness, participants addressed potential gaps in meeting patients’ medical, social, and financial needs.
Participant P1, a PSW with 6–10 years of experience, stated: “We need equipment, towels, pens they (clients) do not have it…….make sure about the client's abilities, walking turns or even going to the washroom.” “……..we don't get medication lists, we don't get the surgeon's numbers, we don't have emergency contacts…”
Except for one, all participants identified that fragmentation of systems and communication among HCPs make coordinating care extremely challenging. Participants identified the lack of approaches to medical and community-service-related components that include broad-based multidisciplinary and diversified programs. In order to accomplish necessary levels of coordination during transitions among health care entities, there is a need for higher levels of effort required on the HCPs’ part. “A lot of times in the community, we don't have access to the doctor right away…………. I don’t know what to do with this, can we try this, and make suggestions that way. They (Doctors or medical facilities) get back to us either through e-mail or fax. But what I find is, clients are getting a disservice because not all nurses, PSWS – not everybody works the same, everyone has their own way of thinking…..and a patient doesn't get looked after properly.” (P4)
Participants specifically expressed challenges to care coordination due to difficulties in meeting the diverse needs of patients including language barriers and safety. “Language barriers……it's hard to get information from patients because I can’t understand them.” (P2)
Based on these findings, we interpret that a digital platform could assist in reducing some of these barriers by allowing patients to provide access to their personal data and analysis to community care workers and services. Healthcare professional do not need to rely solely on accessing patient information in these fragmented systems.
2. Personal perspective in managing patient care
Participants reiterated that they take the time to get to know their patients’ challenges thus providing services that better address the needs of patients and improve their quality of care. It is important to provide high-quality care, providers must understand and respect their patient's needs, attitudes, and concerns. “Our team is very good at interacting with each other to get the job done because the ultimate job is to get the client looked after.” (P4)
Participants were asked about the information they needed before arriving at patients’ homes and sharing information with other providers. Healthcare professionals shared experiences about the challenges of receiving the health information of patients and communicating with other providers, and they suggested using a central electronic system to combat these issues. “Making phone calls and leaving voice messages we find isn’t the best way to communicate, especially if it's a different agency (organization). For example, if the PSW is coming in the next day (from another agency) and (if I) need to inform them (about something), and I have left a voicemail, …..can we guarantee they will actually receive the voicemail before they reach the patient's house. I’d like it (info) to be shared electronically. If there's a way that we can communicate with other agencies electronically, this would be more beneficial and the way forward to the future.” (P3)
Participants expressed that HCP training and experience in the community also plays a role in understanding how and when to intervene to ensure appropriate outcomes, along with the patients’ information. In response to day-to-day challenges, community nurses require increased skills in the system-and community-level interventions. “… Nowadays, it takes (up to) three days for supplies to get to the patient's home from the Toronto Central LHIN
1
(P), …….We get to the patient's home and the hospital has not sent supplies because they don’t remember or think about that side of it. We….. (don’t have supplies), so what do you do? Well, am I going to leave the patient with nothing? No, so usually I have a big purse, it has an excess number of little dressings I can apply until the supplies come in, and we go from there.” (P4)
Domain II: general digital technology opinions
3. Patient engagement with technology
Some participants suspect that it is difficult to engage patients, especially older adults, with the technology. “The old age (adults) they never use it (technology), only the phone. They even have a cell phone and don’t answer.” (P1)
However, other participants indicated that if an electronic media with an audio/video interface was introduced to organize their personal and health information, the patients will happily adopt it. “I think it (audio/video) would be the easiest way if they could have somebody to just press a button (on the tablet) and just talk. The easier, the better.” (P2)
Participants highlighted the potential of technology to improve patient engagement, enhance care continuity, and support better management of health conditions. For instance, one participant noted how technology could help patients track health data, manage appointments, and maintain personal health records. This illustrates how HCP views technology as supporting patient autonomy and communication with HCPs, streamlining care coordination, and improving healthcare delivery. “I think most of them, it would be (clients recording) their feelings, how they feel, if they are capable, they could do their blood pressures and vital signs. … even if they have pain, and sometimes they get very confused (to express). Sometimes I have patients who have so many HCPs that they forget who's who, so maybe they could have their own notes for themselves. Maybe ……..they could take pictures of their HCPs because sometimes they literally forget who's who. … so I could have access too.” (P2)
4. Having patient information before home visits
All HCP discussed the importance and need of obtaining patients’ information before visiting patients’ homes. They emphasized that specific medical conditions, social dynamics, and personal information are vital in assisting these patients. Timely access to detailed medical information containing the clinician's diagnosis, previous history of the patient and current conditions are essential for clinical management in the community. “For example, I have a client who was diagnosed with cancer last year, but because it was so traumatic, she does not remember her meeting with the doctor – how she was diagnosed, treatment, lab work, etc. I can go back, or the patient can go back to review the information to get a better picture of where we are now based on the treatment she is getting.” (P5)
Some HCP also revealed that sometimes patients are unable to retain important information regarding their treatment when speaking with their care team so there is a need for a tool that allows these HCPs to assist these patients. “Audio/video recording would be beneficial for patients who have a hard time remembering their personal and health information and status.” (P5)
In addition, HCP safety concerns with respect to clutter, pets, allergies, etc. are of considerable importance before visiting these patients’ homes. In our study, all HCPs reported feeling obligated to work, despite concerns for their safety. Integration of data and the flow of critical information between participants is highly recommended. “Safety, sometimes when we are going to their homes it's a big unknown, is it is safe for us, we would like to know if there is too much clutter, if they have pets, those are things we need to know beforehand.” (P6)
5. Access and use of information
There is a widely recognized need for a common standard for recording and transmitting clinical information and solutions. In our study, HCPs expressed a desire to access patients’ generated data through digital technologies that allow sharing across care teams. “I think it (technology) would be very useful because it's relevant subjective data coming from the patient. P3.
P3 and P7 emphasized the need for access to recorded data on patients’ health and psychosocial information to make decisions about how to treat the patient. “Sometimes you see the client crying or very moody, sometimes anxious… you don’t know why the client is acting out like this. If I knew why this happened … maybe, they didn’t sleep or have supper or had some pain. You……. need to have the information so you can deal with it.” (P7)
Participants thought remote access to healthcare services might increase participation for those who are medically or socially vulnerable, or who do not have ready access to providers. “I think it (technology) could be really helpful, especially for those who cannot get out of their house, not just because of personal reasons but also their health issues, or they just don't want to see their doctor. I think this would be very helpful to have that virtual visit.” (P6)
6. Information displays for clinical management
When participants were asked about their idea of visualizations for summarizing patient-generated data from MHMR, they expressed the need for a clinical information system, which can extract, display, and process text or graph-oriented data information appropriate to therapeutic needs. “If I could just grab the tablet (any device), click on name and I could find the (health) information. Probably in the text (format) … and it could have headings (of clinical information) for each area and you could click and then document.” (P2)
The preferable mode for the majority of participants was text summary. “…….in a document form, or an e-mail …. documentation (readable statements) …You can summarize it. P4”…“A graph, voice, is not enough, I want word description (notes)…….1 page (summary is enough).” (P1). As expected, it resembles the type of information provided in clinical notes with which participants were familiar as documentation contained in medical records and patient charts tends to be text dominant.
Some participants expressed interest in accessing the summary in multiple ways to better understand the patient's situation. “I want to see the patient's face (interest in raw video data). It gives me their viewpoint from their perspective at the moment when their pain is the worst. Video and point summaries (is more meaningful). P4 “…… nurses prefer both a flow sheet and a narrative summary……. this allows us to have a greater picture.” (P5)
Domain III: MHMR practices & technology
Participants showed a positive attitude and suggested that patients’ information generated through MHMR would be very useful for their delivery of care. “Yes, this (technology MHMR) will be helpful for my assessment, as it provides information about their needs.” (P1)
Participants found MHMR technology's functionality could assist in identifying key issues of the patients and their perspectives about the delivery of care. “They would be documenting their pain, their mental health status, they could even document their mobility, “I had trouble getting up today or their medication compliance like, “I was having nausea and wasn’t able to take my meds today……. can express how they feel, they can also express … how they would like to go about receiving the care in their care plan.” (P3)
Participants emphasized that the patients’ important health information – such as falls, pain, and screening dates, in electronic form makes it easy for participants to manage their care. An electronic data platform (Health informatics) can provide a mechanism for patients to provide their clinician(s), and stakeholders with critical information. ……..instead of walking in and going through every single assessment (pain, falls), you are here to focus on a certain area.” (P4)
Summary of patient record
When participants were asked about their preferences for the data presentation, a majority preferred a text summary as the most likable mode, followed by graph (word cloud and line graph). “I’d like it (the technical summary) at least two pages long.” (P3) A few of these participants were not familiar with graphs and charts and therefore preferred text summary only. “…… not sure how a word cloud works, …a text summary would be nice. P6
In addition, two (n = 2) participants suggested having access to information in more than one presentation format. “I would like to see a word cloud, a graph…..with a little summary. I would like two ways to access the information, visual and written.” (P2)
Privacy and confidentiality
All participants were highly concerned about the patient information staying secure so unauthorized individuals would not gain access to the information. P3 stated “…… can this information be hacked? What happens if the client loses the tablet and is still logged in?”
HCPs questioned the MHMR security and confidentiality because they considered the information patient's would collect to be important and critical health information, which a patient may not like to share. Generally, patient confidentiality is often a fundamental rule among institutions and HCPs. “… what protection do you have there? What privacy, and what security measures do you put on? It's health information that's private and should never be shared.” (P4)
However, none of these participants was worried about sharing a patient's critical information with other HCPs, as they suggested signed consent from the patient would be sufficient. One participant stated “I don’t think they (HCPs) would be concerned about it (privacy) if they got consent at the beginning that all HCPs would be informed anyway.” (P3) Effective communication and sharing of information among providers are key components of PCC.
In terms of patients’ perspectives on privacy and confidentiality, all participants said that patients may be apprehensive about sharing their health and social information with others or even with their close circle of care. However, patients need to be asked directly, which was not part of this study. “From a mental health perspective, patients can be skeptical or apprehensive when two doctors discuss and view their personal information or video. This is a concern for patients because they are not aware of who is viewing or sharing their information. Patients may feel that the doctors (outside of their circle of care) are talking negatively about them.” (P5)
Domain IV: opportunities & challenges for MHMR implementation
Centralized information
All participants support the idea of centralized information in the healthcare system to provide better and more comprehensive care to patients. Participants 5 and 7 emphasized the need for a patient-centered approach and institutional commitment to centralized information. “A centred platform where we (HCPs) can all have access too. And then access for the nurses where we can see the care plans. On this platform, we can also show the patient, so they can pick and choose what is important to them (i.e., lab work).” (P5) Also, participants feel, if the system were centralized then it would be more client-centred care “I think it (centralized information) would be good client-centred care.” (P7)
All participants were inclined towards a system where patient data were accessible to all stakeholders. “It would be nice if all the disciplines – hospital, community, LHIN coordinators and the hospital putting all this information together – it would be better if everyone had access to the same information.” (P2)
However, one participant was doubtful about the mode of transition, yet hopeful “I think the integration (MHMR integration) would be a slow transition, but I could see it (centralization) happening.” (P3)
Most participants agreed that electronic health information is likely to play an increasingly important role in the future. They also felt that shared electronic clinical data would contribute to improved quality of care. “I can foresee I would get help especially if they are being transferred into the hospital. In the community we do not have traditional transfer notes, so we don't have checklists that say this this and this. Now if we can make this video, we can refer to… they can see it and understand what is really happening. For example, a wound that is stage 4, all that information will be transferred over, is only that the wound is stage 4 and how it progressed to stage 4 and how it looks like and the diagnosis and plan of treatment immediately.” (P6)
Feedback
Before the interview ended, the researcher asked for feedback on the prototype of the MHMR application; a majority of the participants were satisfied with the prototype MHMR application. “Your app is something that could help build up that information behind the scenes once the patient leaves the hospital, you’ve got an app we’re looking forward to doing……your app fills in the gap.” (P4)
However, few drew attention to patients’ limited knowledge of technology and their financial situations that may hinder the usability of MHMR routinely. “My only concern is technology-wise, they are so slow. … and who pays for these (devices/technology)?” (P2)
In addition, HCPs felt certain patient groups (e.g., older adults) may not find the MHMR application useful as they don't like change and adapting to technology, hence, would not use the MHMR application. “The technology itself is a challenge, if we’re referring to older adults, they don’t adapt to change well. So they suggested that the application can be a stepping stone and used it as a motivator for change. “You have to train them (older adult clients using the application), but that's a simple one-finger task for them to be able to get the same data.” (P4)
In terms of feedback on data visualization, one participant suggested adding more filters in the word cloud to view different aspects of patients’ conditions. “ ……..word cloud would be very interesting if there was a way we could click on the different words to access the statement or the feature related to the word, and have it be a shortcut. For instance, if I click on ‘prolonged’, what was prolonged? ‘Difficult’? What was difficult? If the words in the word cloud could be linked – for example, Was it prolonged confusion? Or prolonged weakness?” (P5)
Given that word clouds are used for searching, browsing, impression forming and recognizing or matching, it was anticipated that participants would find them useful in finding patterns for matching specific health conditions.
Discussion
This study evaluated community-care-based HCPs’ perspectives on how MHMR could be used for planning, allocating resources, delivering care, and ensuring care continuity in the community. Four domains and eleven themes emerged from the perspectives of the HCPs regarding their views on HCPs’ needs while working in the community for older adults. Results from this study with seven participants (PSWs and Nurses) showed that the MHMR application prototype could potentially support care coordination, managing patient care, retrieving information before visits and summary of patient records, while acknowledging areas requiring further exploration. The qualitative findings assisted in reasoning the participant's preferences and needs directing future design choices to improve the prototype. The qualitative data frequency distribution systematically categorized and quantified themes derived from HCP narratives, offering clarity on prevalent patterns and areas of importance in our dataset. This quantitative dimension complemented our qualitative analysis by adding rigor and systematicity enhancing the reliability and validity of our findings. The purposive sampling method targeted diverse HCPs across disciplines relevant to MHMR so that we could ensure that there were balanced perspectives adding to the credibility of the findings.
Specifically, all participants mentioned that there was a current lack of information sharing and access to medical record information among community care health workers that not only puts them at a disadvantage in providing individual care efficiently and effectively, but also potentially compromised their safety. They viewed MHMR as a way of gaining access to patient-generated data that they believed patients would be willing to share with them as long as patients were comfortable and confident in using the MHMR technology. Studies have shown that supplemental electronic communication emphasizing physicians’ collaboration and improves patients’ outcomes with chronic diseases.28–31 This may also be transferable to other HCP but may be a difficult implementation given the quantity and variety of HCP with varying communication needs involved. Inadequate patient information left PSWs unprepared to be sensitive to patient needs, as seen in previous literature.32,33 They highlighted the need for more documentation about health services used in-between visits, interactions with HCPs in a circle of care, concerns, previous medical history, missing medical information, and the care plan. Strengthening the public health system and improving population health depends upon expertise in community engagement and partnership development. 34 They viewed MHMR as a tool that could provide some of this information. However, they also commented on the need for presenting summaries of the MHMR video data in a way that they could understand and use. Specifically, they wanted short readable reports along with graphs and charts.
Although patient medical records have traditionally been kept on paper, EMRs are becoming more popular because they can reduce medical errors brought on by illegible handwriting, and give access to large quantities of data. 35 It is important for health professionals to understand older adults’ apprehensions, opinions, and experiences in order to assess their real needs and offer tailor-made services. Patient-generated data are a more contemporary technique for collecting medical record data. This approach requires the patient or their caregivers to collect health information but there are few accessible and trusted tools for this purpose. 12 While EMRs may address the issues of illegible handwriting in paper systems, EMRs may also contain potential errors from data entry, which in turn presents new management challenges posed by extensive datasets, prompting the need for further research into user-friendliness and data security in healthcare.
Technology is pivotal in healthcare, enhancing access to services, decentralizing care, and empowering patients to manage their conditions, thus improving quality of life.36,37
Patient-generated data are often collected using specialized, publicly available wearable technology (e.g., FitBit™). This is pertinent to our study as it reflects a growing trend in healthcare where individuals contribute to their health records through personal devices. However, due to systemic constraints in validating the authenticity of patient-generated data, concerns remain about its reliability. Additionally, some data generated by patient-owned platform technologies are not available directly to either patients or their HCPs in a raw format because of platform business models.38,39 The platform's terms of service typically do not recognize patient ownership of their data. Instead, the data are usually stored and owned by the organization selling the technology and its proprietary data collection and analysis software, neither of which is shareable. Typically, if an individual discontinues their payments, all their data are inaccessible to them, and effectively “lost.” 40 The significant risks involved in this scenario are, first, the individual does not have access to the personal data they collected in a specific period which could be useful for multipurpose, and second, if personal data fall into the wrong hands, people could be harmed. Depending on the situation, they could become victims of identity theft, discrimination, or even physical harm. These challenges underscore the importance of considering not only the technical capabilities of platform technologies such as wearable technologies but also the broader implications for patient empowerment, data security, and privacy in the public/private healthcare settings where HCP-provided care protocols are delivered.
In this study, participants stated that their first choice for data visualization would be a Text Summary that would consist of no more than “one page” summary of the main clinically relevant information. This preference aligns with previous research showing that HCPs often prioritize narrative clinical notes, and the text summary in MHMR was seen as comparable to this format.14,41 While text-based summaries were strongly favored, participants also recognized the potential value of visual tools, particularly word clouds. Prior research has shown that although text-based notes were preferred they were not necessarily that useful for understanding patient data. Tanvir et al. 19 found that text summaries were used by HCP to gain an overview of a patient's situation but that other visualization such as word clouds, and line and bar graphs were used to understand patterns and specific details about a patient's health. The presentation of patient data affects a healthcare provider's ability to understand and interpret important data. 42 Several studies have shown that summaries of the text, rather than graphs, are more effective in decision-making. For example, Gatt et al. 43 found that users (doctors and nurses) made better decisions after reviewing manually generated text summaries compared to graphical data alone. Similarly, Sultanum et al. 44 emphasized the need to integrate textual summaries to get an overview of clinical documentation instead of relying on graphical representations. Other studies have shown that while graphical visualizations can aid in teaching and learning, they are often more effective when used in conjunction with text.11,45 To meet diverse users need, MHMR should offer multiple visualization formats, allowing providers to select the most appropriate method for their clinical context. Additionally, some participants expressed interest in accessing patient-recorded videos for more nuanced insight into specific health concerns. Ensuring easy access to relevant video content alongside visualizations could further support informed clinical decision-making.
All HCPs had concerns and offered suggestions about the need for advanced levels of technology literacy to use MHMR by their patients. They discussed age, language, and limited technology literacy as key factors that could hinder the adoption and successful use of the technology by older adults they serve. While it is important to ensure that interfaces are easy to learn and use by target populations, it is also crucial that the users themselves are part of the design and development work. 46 The next stage of MHMR development will not only use best practices for designing the user interface and experience, such as those recommended by the W3C (World Wide Web Consortium), patient researchers will be engaged throughout the process. 47
Participants expressed concerns about privacy, data security, and how those would affect sharing. Vo et al. 39 also found that patients were reluctant to share information with their HCPs due to worries about data security. Cybersecurity and data privacy are neither unique to this application nor are they resolved for most Internet-based applications. While blockchain and advanced encryption technology may eventually offer efficient and effective solutions, currently they do not. Essentially, any data that are shared or contained on the Internet is vulnerable. 48 One of the opportunities that MHMR offers is that data are stored locally on patient's devices. Individuals can choose to electronically share some or all of their data, or just the summary visualizations with others. In the end, all the participants recognized the opportunity of the MHMR technology for enhancing HCPs’ support for managing older adults in the community, and for accessing the patient's personal data as appropriate and trusted HCPs who could assist patients better than they do now.
Finally, HCPs endorsed the notion of integrating patient-generated data from the MHMR application into electronic health records as it expands the capacity to monitor patients remotely, and HCPs can address the clinical issues efficiently. Healthcare professionals and all stakeholders such as health information technology vendors, wearable devices and mobile health vendors, data visualization designers, and data scientists should work together to develop and improve the frictionless user experience.49,50 Overall, experts believe that significant benefits to patients and society can be realized when centralized information systems are widely adopted and used in a “meaningful” way. 51 However, this ideal remains difficult to achieve despite the many attempts to standardize data-sharing models in the healthcare industry due to the diversity of data types, stakeholders, and competing interests. Integrated MHMR data into electronic health records must follow these moving standards. One unique feature (and perhaps advantage) of MHMR in this regard is that the data are owned and controlled by the patient, who determines what to share, with whom, when, and how.
Limitations and strengths of the study
There were several limitations of this study. One of the main limitations was the sample size and participant demographics. The current study included a relatively small sample size, predominantly comprising PSWs and nurses. This homogeneity within the participant demographics may have influenced the diversity of opinions and preferences observed. Future research on MHMR should aim to incorporate a larger and more diverse sample, encompassing various healthcare disciplines and experience levels. This approach would provide a more comprehensive understanding of how different HCPs perceive and use digital health tools in patient care. Moreover, the majority of participants in this study were from similar gender and professional backgrounds, potentially limiting the transferability of the findings across broader healthcare contexts. Different healthcare professions and genders may have distinct training regimens, patient interaction expectations, and technological proficiency, which could significantly affect their attitudes towards and utilization of MHMR technologies. 52 Therefore, future studies, should strive to include a more heterogeneous participant pool to capture a broader spectrum of perspectives and experiences. In addressing these limitations, we recognize the need for a more inclusive and representative sample in future research efforts. By doing so, we can enhance the robustness and transferability of findings related to MHMR technology adoption and implementation within diverse healthcare settings.
Another limitation of the study was the number of visualizations presented. While the prototype included a line graph and other visual elements, it did not include a word cloud or final data visualizations for review. The word cloud, as shown in Figure 1, was part of an initial concept presented to participants. It was depicted as a wireframe in a separate static prototype rather than being integrated into the application, as was intended for future stages of the project. Participants were asked to imagine different possibilities for data visualizations and consider their preferences. Future studies should include concrete examples of data visualizations and assess how various graphical features contribute to the understanding of the data. A technical limitation was that the MHMR prototype was presented as a series of prototype screens with limited functionality enabled. While the prototype provided a visual representation of the interface design and layout, their static nature prevented participants from interacting with the prototype in a realistic manner. This lack of functionality limited our ability to gather authentic user feedback on usability, user experience, and the practicality of the MHMR tool in real-world scenarios. In addition, there were some technical difficulties with the tablet display during the prototype demonstration, which may have affected the participant's view of the MHMR prototype as some information may have been missed or not clearly visible on the demonstration screen. Future iterations of MHMR research will incorporate a fully functional prototype that allows HCPs to interact with the system as intended. This would enable more accurate assessments of system performance, workflow integration, and user satisfaction. However, the initial reactions, suggestions, and opinions of HCP as one of the user groups of MHMR were valuable and insightful for the next stage of development. As recommended by user-centered design methods, user evaluations on early prototypes are crucial in ensuring the user perspectives are included and potential issues are identified as early as possible so they can be avoided. 53
One limitation of this study is that the preinterview questionnaire and semistructured interview only had internal validity and not external validity, which may affect the reliability of the data collected. However, the preinterview questionnaire was adapted from an existing validated instrument. 54 While pilot testing was conducted, the lack of external validation may still limit the generalizability of the findings. Future research could benefit from using fully validated instruments to enhance the robustness and generalizability of the results.
A final limitation reflects limited examples of real multiway sharing of patients owned and generated data with HCPs reflecting development of a partnership with the patient in goal-oriented care, where goals are generated by patients. Future work will involve specifically developing complex care management scenarios where such patient partnerships have been shown to generate better results, 55 describe the need to incorporate context into healthcare quality evaluation frameworks dependent on complex care interventions. It is self-evident that the perspective of the person receiving care is an essential element of such evaluations. 21
This study offers several strengths. It makes significant scientific contributions to understanding how HCP could use patient-generated qualitative data via digital platforms for planning, allocating, and delivering care, as well as ensuring care continuity. By employing CQR, the study rigorously analyzes and visualizes complex qualitative data, offering insightful interpretations that enhance comprehension. The emphasis on user-centered data generation approaches advances methodologies for effectively communicating qualitative insights. Additionally, the study contributes valuable advancements to human factors research in healthcare and beyond. The novelty of this project lies in its innovative exploration of qualitative patient-generated data using digital technology from an HCP perspective, paving the way for new frontiers in digital healthcare data utilization and visualization.
Conclusion
In collaboration with SE Health, a large community care provider, this study demonstrates how the MHMR platform could guide case management and community-care service delivery. The study found a growing interest among HCPs in the use of digital technologies including MHMR for delivering health services to older adults in the community. Optimizing the integration of digital health technology for older adults in the community requires collaboration among HCPs and institutions. This opens areas for future research, given the increasing uptake of technology among older adults globally, who are seeking to play a greater role in aligning systemic care goals with their self-perceived complex-care needs and interests.
Footnotes
Acknowledgments
The authors like to thank the participants for providing their time and considerable insight. The authors would like to thank Daltash Dhaliwal for her assistance during the data collection and analyses. In addition, the authors are thankful to Dr Patrick Neumann for his advice and support throughout the historical study.
Ethical considerations
The study was reviewed and approved by the Toronto Metropolitan University, previously known as Ryerson University Human Ethics Research Committee (Protocol# REB 2019–297). All older adults freely given, informed consent to participate in the study. Informed consent statement was included in the method section.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author contributions
All authors contributed to the design and implementation of the research, to the analysis of the results and to the writing of the manuscript.
Funding
This research was supported by the AGE-WELL Network of Centres of Excellence through the Core Research Program 2020 (CRP Catalyst 2019) and was funded under grant number AWCAT-2019–131. We gratefully acknowledge AGE-WELL for their support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data will not be available in a public repository due to the older adults privacy and confidentiality issue.
Guarantor
SFL and DF.